
Partial Pulpotomy in Young Permanent Teeth: A Systematic Review and Meta-Analysis


 ,
,  , and
, and 
Abstract
:1. Introduction
Rationale of Study and Objective
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
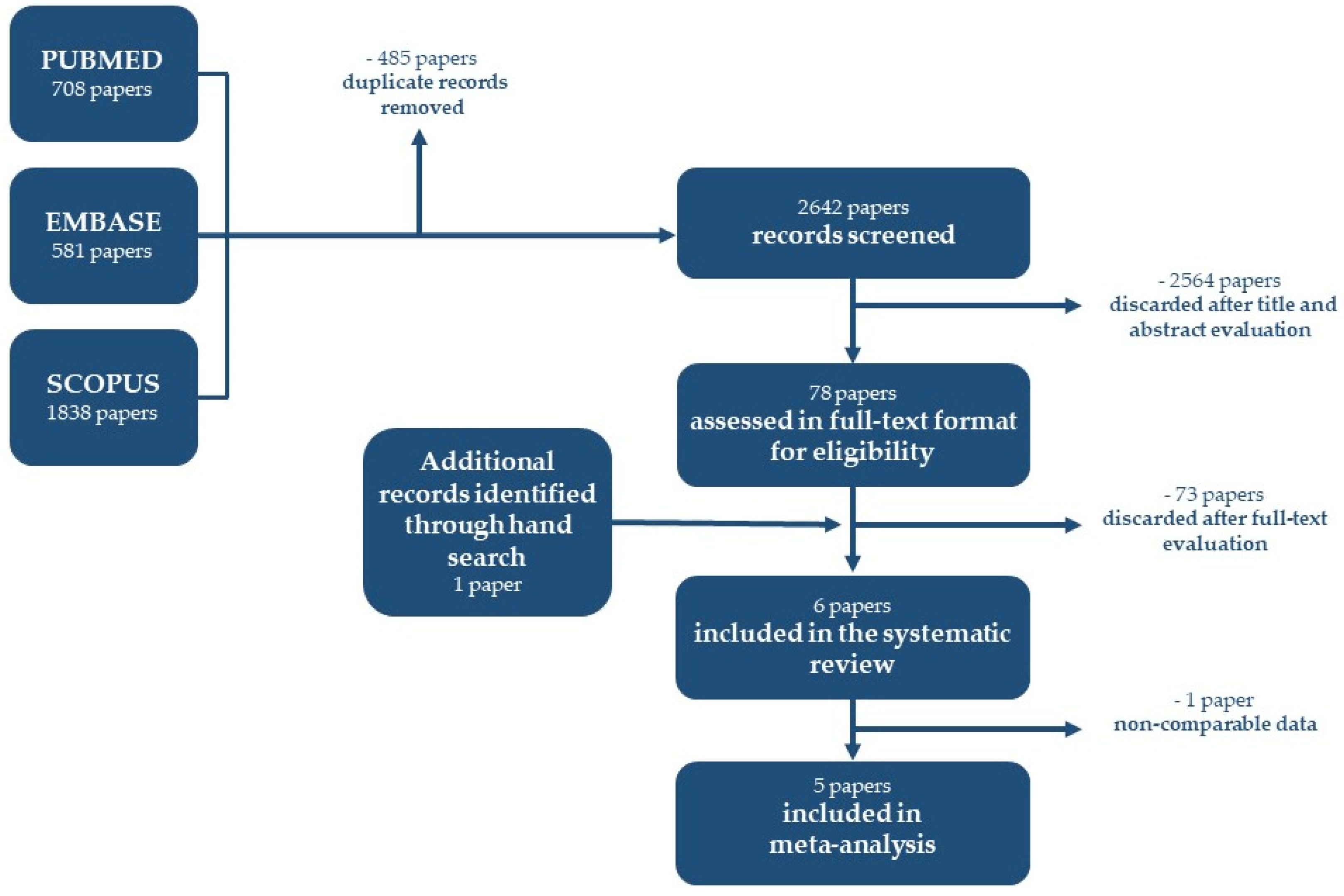
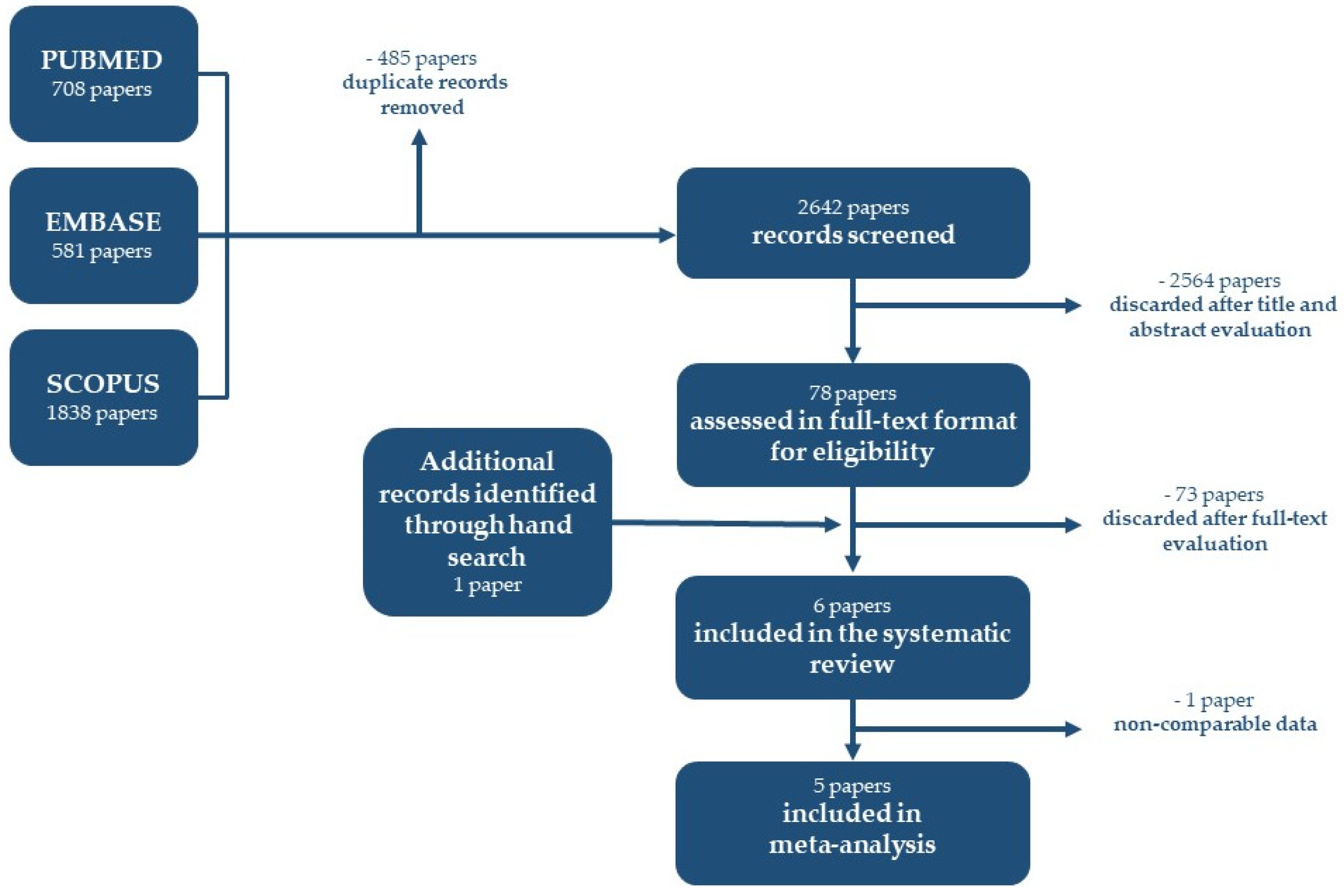
2.4. Study Selection and Data Extraction
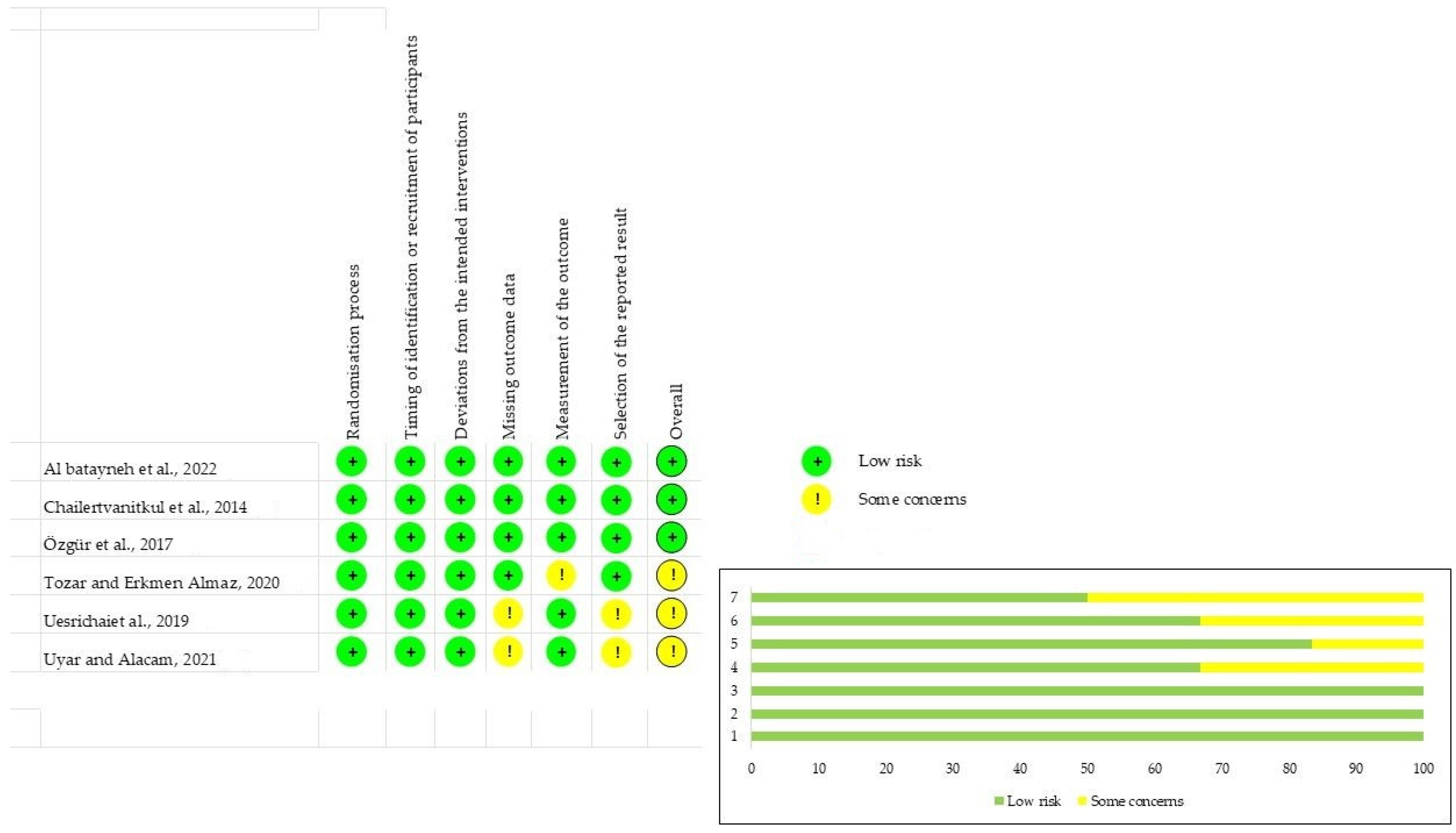
2.5. Risk of Bias and Quality Evaluation of Included Studies
2.6. Outcome Measures
2.7. Heterogeneity
2.8. Synthesis of the Results
3. Results
3.1. Reliability and Validity
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Qualitative Synthesis
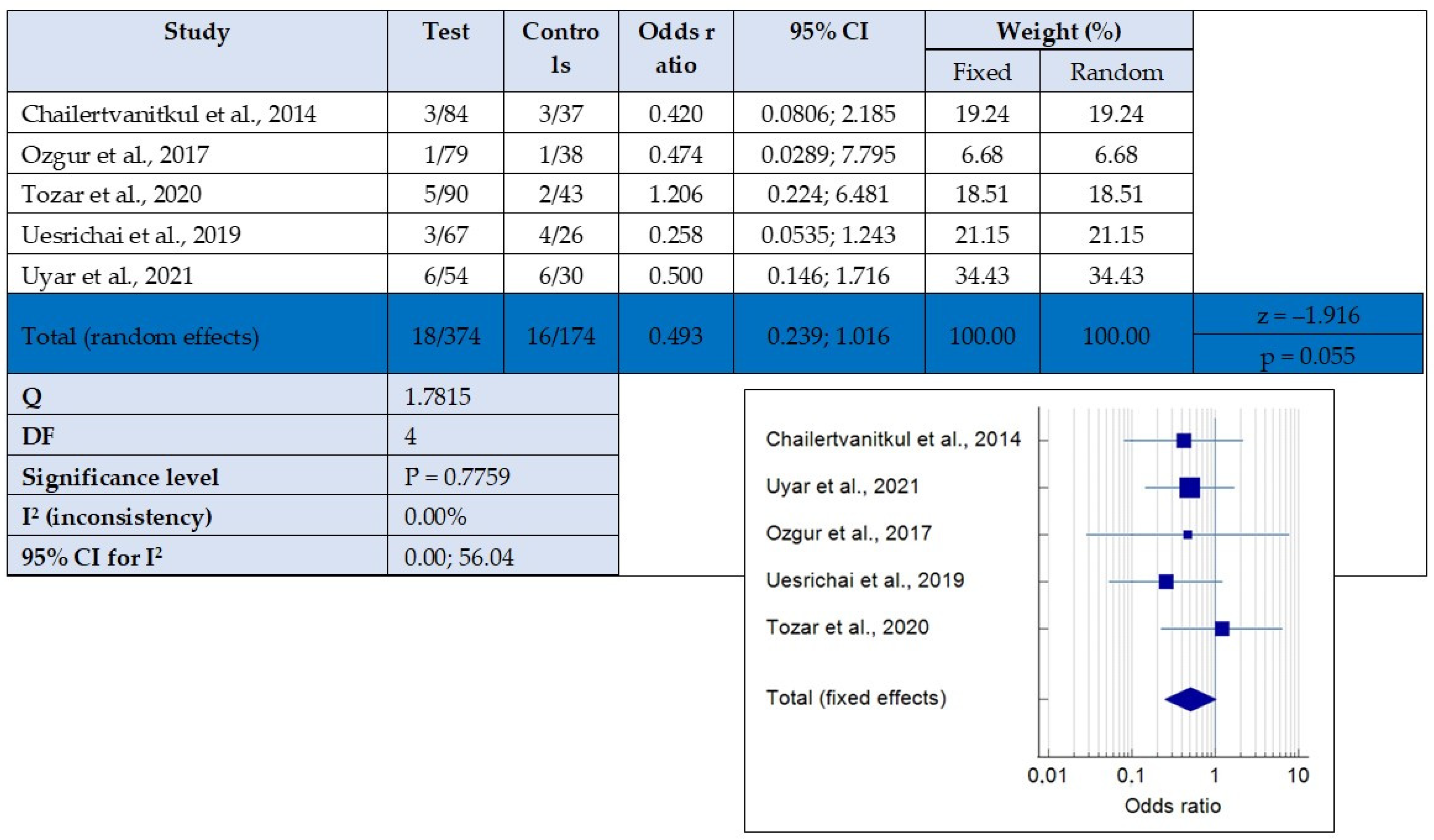
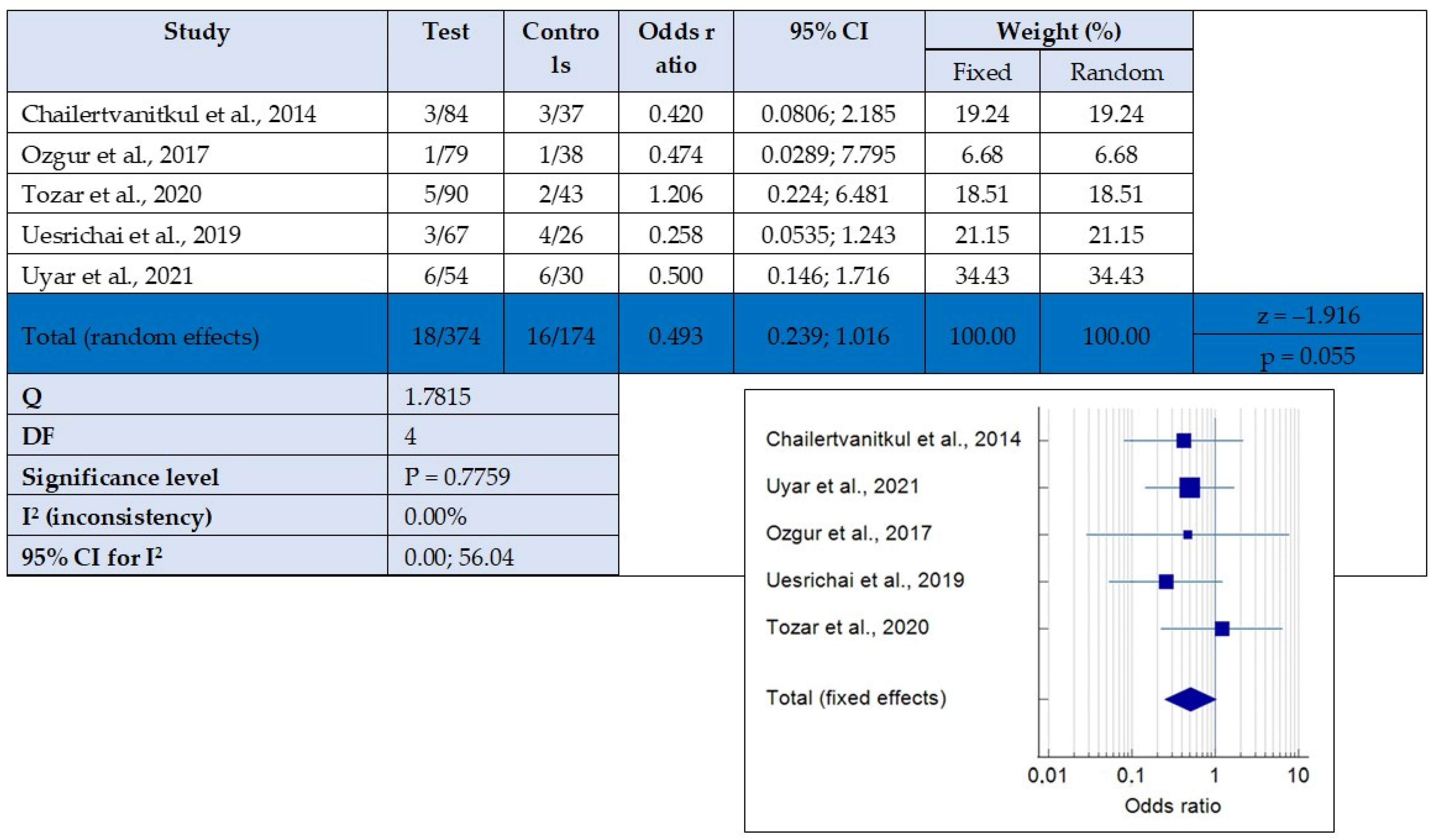
3.5. Quantitative Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Uribe, S.E.; Innes, N.; Maldupa, I. The global prevalence of early childhood caries: A systematic review with meta-analysis using the WHO diagnostic criteria. Int. J. Paediatr. Dent. 2021, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Dong, B.; Yu, D.; Ren, Q.; Sun, Y. The prevalence of molar incisor hypomineralization: Evidence from 70 studies. Int. J. Paediatr. Dent. 2018, 28, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Chailertvanitkul, P.; Paphangkorakit, J.; Sooksantisakoonchai, N.; Pumas, N.; Pairojamornyoot, W.; Leela-Apiradee, N.; Abbott, P.V. Randomized control trial comparing calcium hydroxide and mineral trioxide aggregate for partial pulpotomies in cariously exposed pulps of permanent molars. Int. Endod. J. 2014, 47, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Pujar, P.; Subbareddy, V.V. Evaluation of the tooth brushing skills in children aged 6–12 years. Eur. Arch. Paediatr. Dent. 2013, 14, 213–219. [Google Scholar] [CrossRef]
- Boustedt, K.; Dahlgren, J.; Twetman, S.; Roswall, J. Tooth brushing habits and prevalence of early childhood caries: A prospective cohort study. Eur. Arch. Paediatr. Dent. 2020, 21, 155–159. [Google Scholar] [CrossRef]
- Al-Batayneh, O.B.; Abdelghani, I.M. Outcome of vital pulp therapy in deeply carious molars affected with molar incisor hypomineralisation (MIH) defects: A randomized clinical trial. Eur. Arch. Paediatr. Dent. 2022, 23, 587–599. [Google Scholar] [CrossRef]
- Ghanim, A.M.; Manton, D.J.; Morgan, M.V.; Marino, R.J.; Bailey, D.L. Trends of oral health care and dental treatment needs in relation to molar incisor hypomineralisation defects: A study amongst a group of Iraqi schoolchildren. Eur. Arch. Paediatr. Dent. 2012, 13, 171–178. [Google Scholar] [CrossRef]
- Leong, D.J.X.; Yap, A.U. Vital pulp therapy in carious pulp-exposed permanent teeth: An umbrella review. Clin. Oral Investig. 2021, 25, 6743–6756. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F., Jr.; Li, Y.; Tay, F.R. Vital pulp therapy: Histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J. Dent. 2019, 86, 41–52. [Google Scholar] [CrossRef]
- Lin, L.M.; Ricucci, D.; Saoud, T.M.; Sigurdsson, A.; Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust. Endod. J. 2020, 46, 154–166. [Google Scholar] [CrossRef]
- Alqaderi, H.E.; Al-Mutawa, S.A.; Qudeimat, M.A. MTA pulpotomy as an alternative to root canal treatment in children’s permanent teeth in a dental public health setting. J. Dent. 2014, 42, 1390–1395. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.J.; Seremidi, K.; Stratigaki, E.; Kloukos, D.; Duggal, M.; Gizani, S. Deep dentine caries management of immature permanent posterior teeth with vital pulp: A systematic review and meta-analysis. J. Dent. 2022, 124, 104214. [Google Scholar] [CrossRef] [PubMed]
- Ghoddusi, J.; Forghani, M.; Parisay, I. New approaches in vital pulp therapy in permanent teeth. Iran. Endod. J. 2014, 9, 15–22. [Google Scholar]
- Islam, R.; Islam, M.R.R.; Tanaka, T.; Alam, M.K.; Ahmed, H.M.A.; Sano, H. Direct pulp capping procedures—Evidence and practice. Jpn. Dent. Sci. Rev. 2023, 59, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Singh, H.; Dhillon, J.S.; Batra, M.; Saini, M. MTA versus Biodentine: Review of Literature with a Comparative Analysis. J. Clin. Diagn. Res. 2017, 11, ZG01–ZG05. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Yu, Y.H.; Karabucak, B. Endodontic treatments on permanent teeth in pediatric patients aged 6–12 years old. J. Dent. Sci. 2023, 18, 1109–1115. [Google Scholar] [CrossRef]
- Koc Vural, U.; Kiremitci, A.; Gokalp, S. Which is the most effective biomaterial in indirect pulp capping? 4- year comparative randomized clinical trial. Eur. Oral Res. 2022, 56, 35–41. [Google Scholar] [CrossRef]
- Drouri, S.; El Merini, H.; Sy, A.; Jabri, M. Evaluation of Direct and Indirect Pulp Capping with Biodentine in Vital Permanent Teeth with Deep Caries Lesions. Cureus 2023, 15, e39374. [Google Scholar] [CrossRef]
- Palczewska-Komsa, M.; Kaczor-Wiankowska, K.; Nowicka, A. New Bioactive Calcium Silicate Cement Mineral Trioxide Aggregate Repair High Plasticity (MTA HP)-A Systematic Review. Materials 2021, 14, 4573. [Google Scholar] [CrossRef]
- Pedano, M.S.; Li, X.; Yoshihara, K.; Landuyt, K.V.; Van Meerbeek, B. Cytotoxicity and Bioactivity of Dental Pulp-Capping Agents towards Human Tooth-Pulp Cells: A Systematic Review of In-Vitro Studies and Meta-Analysis of Randomized and Controlled Clinical Trials. Materials 2020, 13, 2670. [Google Scholar] [CrossRef]
- Aeinehchi, M.; Eslami, B.; Ghanbariha, M.; Saffar, A.S. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: A preliminary report. Int. Endod. J. 2003, 36, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317. [Google Scholar] [CrossRef] [PubMed]
- Sen, H.G.; Helvacioglu-Yigit, D.; Yilmaz, A. Radiopacity evaluation of calcium silicate cements. BMC Oral Health 2023, 23, 491. [Google Scholar] [CrossRef] [PubMed]
- Katge, F.A.; Patil, D.P. Comparative Analysis of 2 Calcium Silicate-based Cements (Biodentine and Mineral Trioxide Aggregate) as Direct Pulp-capping Agent in Young Permanent Molars: A Split Mouth Study. J. Endod. 2017, 43, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Slaboseviciute, M.; Vasiliauskaite, N.; Drukteinis, S.; Martens, L.; Rajasekharan, S. Discoloration Potential of Biodentine: A Systematic Review. Materials 2021, 14, 6861. [Google Scholar] [CrossRef]
- Al-Hiyasat, A.S.; Ahmad, D.M.; Khader, Y.S. The effect of different calcium silicate-based pulp capping materials on tooth discoloration: An in vitro study. BMC Oral Health 2021, 21, 330. [Google Scholar] [CrossRef]
- Mathur, V.P.; Dhillon, J.K.; Kalra, G. A new approach to facilitate apexogenesis using soft tissue diode laser. Contemp. Clin. Dent. 2014, 5, 106–109. [Google Scholar] [CrossRef]
- Aslantas, E.E.; Buzoglu, H.D.; Karapinar, S.P.; Cehreli, Z.C.; Muftuoglu, S.; Atilla, P.; Aksoy, Y. Age-related Changes in the Alkaline Phosphatase Activity of Healthy and Inflamed Human Dental Pulp. J. Endod. 2016, 42, 131–134. [Google Scholar] [CrossRef]
- Aslantas, E.E.; Buzoglu, H.D.; Muftuoglu, S.F.; Atilla, P.; Karapinar, S.P.; Aksoy, Y. Effects of aging and inflammation on catalase activity in human dental pulp. Arch. Oral Biol. 2022, 141, 105482. [Google Scholar] [CrossRef]
- WHO. Youth and health risks. In Sixty-Fourth World Health Assembly; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Uyar, D.S.; Alacam, A. Evaluation of partial pulpotomy treatment in cariously exposed immature permanent molars: Randomized controlled trial. Niger. J. Clin. Pract. 2021, 24, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Özgür, B.; Kargın, S.T.; Ölmez, M.S. Clinical evaluation of giomer- and resin-based fissure sealants on permanent molars affected by molar-incisor hypomineralization: A randomized clinical trial. BMC Oral Health 2022, 22, 275. [Google Scholar] [CrossRef] [PubMed]
- Uesrichai, N.; Nirunsittirat, A.; Chuveera, P.; Srisuwan, T.; Sastraruji, T.; Chompu-inwai, P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: A noninferiority randomized controlled trial. Int. Endod. J. 2019, 52, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Tozar, K.N.; Erkmen Almaz, M. Evaluation of the Efficacy of Erbium, Chromium-doped Yttrium, Scandium, Gallium, and Garnet Laser in Partial Pulpotomy in Permanent Immature Molars: A Randomized Controlled Trial. J. Endod. 2020, 46, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Jha, S.; Bhol, S.; Dash, B.P.; Sarangal, H.; Namdev, R. Molar Incisor Hypomineralization: Clinical Characteristics with Special Emphasis on Etiological Criteria. J. Pharm. Bioallied Sci. 2021, 13, S651–S655. [Google Scholar] [CrossRef]
- Cabral, R.N.; Nyvad, B.; Soviero, V.; Freitas, E.; Leal, S.C. Reliability and validity of a new classification of MIH based on severity. Clin. Oral Investig. 2020, 24, 727–734. [Google Scholar] [CrossRef]
- Alanzi, A.; Faridoun, A.; Kavvadia, K.; Ghanim, A. Dentists’ perception, knowledge, and clinical management of molar-incisor-hypomineralisation in Kuwait: A cross-sectional study. BMC Oral Health 2018, 18, 34. [Google Scholar] [CrossRef]
- Kang, C.M.; Sun, Y.; Song, J.S.; Pang, N.S.; Roh, B.D.; Lee, C.Y.; Shin, Y. A randomized controlled trial of various MTA materials for partial pulpotomy in permanent teeth. J. Dent. 2017, 60, 8–13. [Google Scholar] [CrossRef]
- Albaiti, S.S.; Albishri, R.F.; Alhowig, M.T.; Tayyar, W.I.; Alqurashi, N.F.; Alghamdi, F.T. Partial Pulpotomy as an Applicable Treatment Option for Cariously Exposed Posterior Permanent Teeth: A Systematic Review of Randomized Clinical Trials. Cureus 2022, 14, e26573. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Yew, Y.Q.; Lee, H.Y.; Low, T.; Pillai, M.P.M.; Laer, T.S.; Wafa, S. Is pulpotomy a promising modality in treating permanent teeth? An umbrella review. Odontology 2022, 110, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Loghin, S.; Siqueira, J.F., Jr. Correlation between clinical and histologic pulp diagnoses. J. Endod. 2014, 40, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Muliyar, S.; Shameem, K.A.; Thankachan, R.P.; Francis, P.G.; Jayapalan, C.S.; Hafiz, K.A. Microleakage in endodontics. J. Int. Oral Health 2014, 6, 99–104. [Google Scholar]
- Cho, S.Y.; Seo, D.G.; Lee, S.J.; Lee, J.; Lee, S.J.; Jung, I.Y. Prognostic factors for clinical outcomes according to time after direct pulp capping. J. Endod. 2013, 39, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Delgado, R.M.; Botelho, J.; Machado, V.; Mendes, J.J.; Lopes, L.B. Knowledge, perception, and clinical experiences on molar incisor hypomineralization amongst Portuguese dentists. BMC Oral Health 2022, 22, 250. [Google Scholar] [CrossRef]
- Gamboa, G.C.S.; Lee, G.H.M.; Ekambaram, M.; Yiu, C.K.Y. Knowledge, perceptions, and clinical experiences on molar incisor hypomineralization among dental care providers in Hong Kong. BMC Oral Health 2018, 18, 217. [Google Scholar] [CrossRef]
- European Society of Endodontology; Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar] [CrossRef]
- AAE Position Statement on Vital Pulp Therapy. J. Endod. 2021, 47, 1340–1344. [CrossRef]
- Chevalier, V.; Le Fur Bonnabesse, A.; Duncan, H.F. Frightened of the pulp? A qualitative analysis of undergraduate student confidence and stress during the management of deep caries and the exposed pulp. Int. Endod. J. 2021, 54, 130–146. [Google Scholar] [CrossRef]
- Duncan, H.F. Present status and future directions-Vital pulp treatment and pulp preservation strategies. Int. Endod. J. 2022, 55 (Suppl. S3), 497–511. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Source | Location | Funding Source |
|---|---|---|---|
| Al-batayneh et al., 2022 [6] | Eur Arch Paed Dent | Jordan | University grant |
| Chailertvanitkul et al., 2014 [3] | Int Endod J | Thailand | Not reported |
| Özgür et al., 2017 [37] | BMC Oral Health | Turkey | University grant |
| Tozar and Erkmen Almaz, 2020 [38] | J Endod | Turkey | University grant |
| Uesrichai et al., 2019 [39] | Int Endod J | Thailand | University grant |
| Uyar and Alacam, 2021 [40] | Niger J Clin Pract | Turkey | None |
| Study | Age (Range or Mean) | Patients (n) | Teeth (n) | Drop-Out of Teeth n (%) | Study Design | Final Restoration | Follow-Up (mo.) | Overall Success Rate at 12 mo. (n/Total) | Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|
| Test | Control | |||||||||
| Al-batayneh et al., 2022 [6] * | 11 ± 3.2 y | 50 | 50 | 3/50 (6.0%) | PP vs. IPC or FP | GIC, SSC | 3, 6, 12, 24 | PP 11/12 | IPC 2/25 | VTP is a valid option in severe carious lesions of permanent first molars with MIH over 24 mo. IPC had a higher success rate (95.8%) than PP or CP (85.7% for both). |
| FP 2/11 | ||||||||||
| Chailertvanitkul et al., 2014 [3] | 7–10 y | 80 | 84 | 8/84 (9.5%) | MTA vs. CH | Amalgam | 3, 6, 12, 24 | MTA 41/44 | CH 37/40 | PP using MTA or CH resulted in favourable treatment outcomes. Unfavorable outcomes increase for pulp exposure >5 mm |
| Özgür et al., 2017 [34] | 6–13 y | 63 | 80 | 4/80 (5.0%) | MTA vs. CH | CR | 6, 12, 18, 24 | MTA/SH 19/20 | CH/SH 19/20 | PP with MTA or CH produces comparable and favorable results in immature permanent teeth. |
| MTA/SS 20/20 | CH/SS 19/19 | |||||||||
| Tozar and Erkmen Almaz, 2020 [36] | 6–15 y | 90 | 90 | 3/90 (3.3%) | MTA vs. MTA + Laser Er, Cr: YSGG | GIC, CR | 1, 3, 6, 12 | MTA 40/45 | MTA + Laser 43/45 | The use of the laser did not contribute to the success rate compared to MTA alone. |
| Uesrichai et al., 2019 [35] | 10 y | 69 | 69 | 2/67 (3.0%) | MTA vs. BD | C, SSC | 32.2 ± 17.9 | MTA 34/37 | BD 26/30 | Permanent teeth with signs and symptoms of irreversible pulpitis were successfully treated with PP using MTA and BD. |
| Uyar and Alacam, 2021 [33] | 7.9 y | 105 | 119 | 0/54 (0.0%) | MTA vs. CH or BD | SSC | 3, 6, 12 | MTA 17/18 | CH 13/18 | PP treatment is a good option and has high success rates at 12 months with CH, MTA, and BD. |
| BD 17/18 | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camoni, N.; Cagetti, M.G.; Cirio, S.; Esteves-Oliveira, M.; Campus, G. Partial Pulpotomy in Young Permanent Teeth: A Systematic Review and Meta-Analysis. Children 2023, 10, 1447. https://doi.org/10.3390/children10091447
Camoni N, Cagetti MG, Cirio S, Esteves-Oliveira M, Campus G. Partial Pulpotomy in Young Permanent Teeth: A Systematic Review and Meta-Analysis. Children. 2023; 10(9):1447. https://doi.org/10.3390/children10091447
Chicago/Turabian StyleCamoni, Nicole, Maria Grazia Cagetti, Silvia Cirio, Marcella Esteves-Oliveira, and Guglielmo Campus. 2023. "Partial Pulpotomy in Young Permanent Teeth: A Systematic Review and Meta-Analysis" Children 10, no. 9: 1447. https://doi.org/10.3390/children10091447
APA StyleCamoni, N., Cagetti, M. G., Cirio, S., Esteves-Oliveira, M., & Campus, G. (2023). Partial Pulpotomy in Young Permanent Teeth: A Systematic Review and Meta-Analysis. Children, 10(9), 1447. https://doi.org/10.3390/children10091447