
Multivariable Projections of Caries-Free Prevalence and the Associated Factors from 2019 to 2030 among Schoolchildren Aged 6, 12 and 16-Year-Old in Malaysia


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants, Data Source and Description
2.2. Data Analysis
3. Results
3.1. Selection of Potential Associated Factors of Caries-Free for MLR
3.2. Multiple Linear Regression of Caries-Free Prevalence and Associated Factors among Schoolchildren
3.3. Multiple Linear Regression with Arma Errors for 12 Years Old Schoolchildren
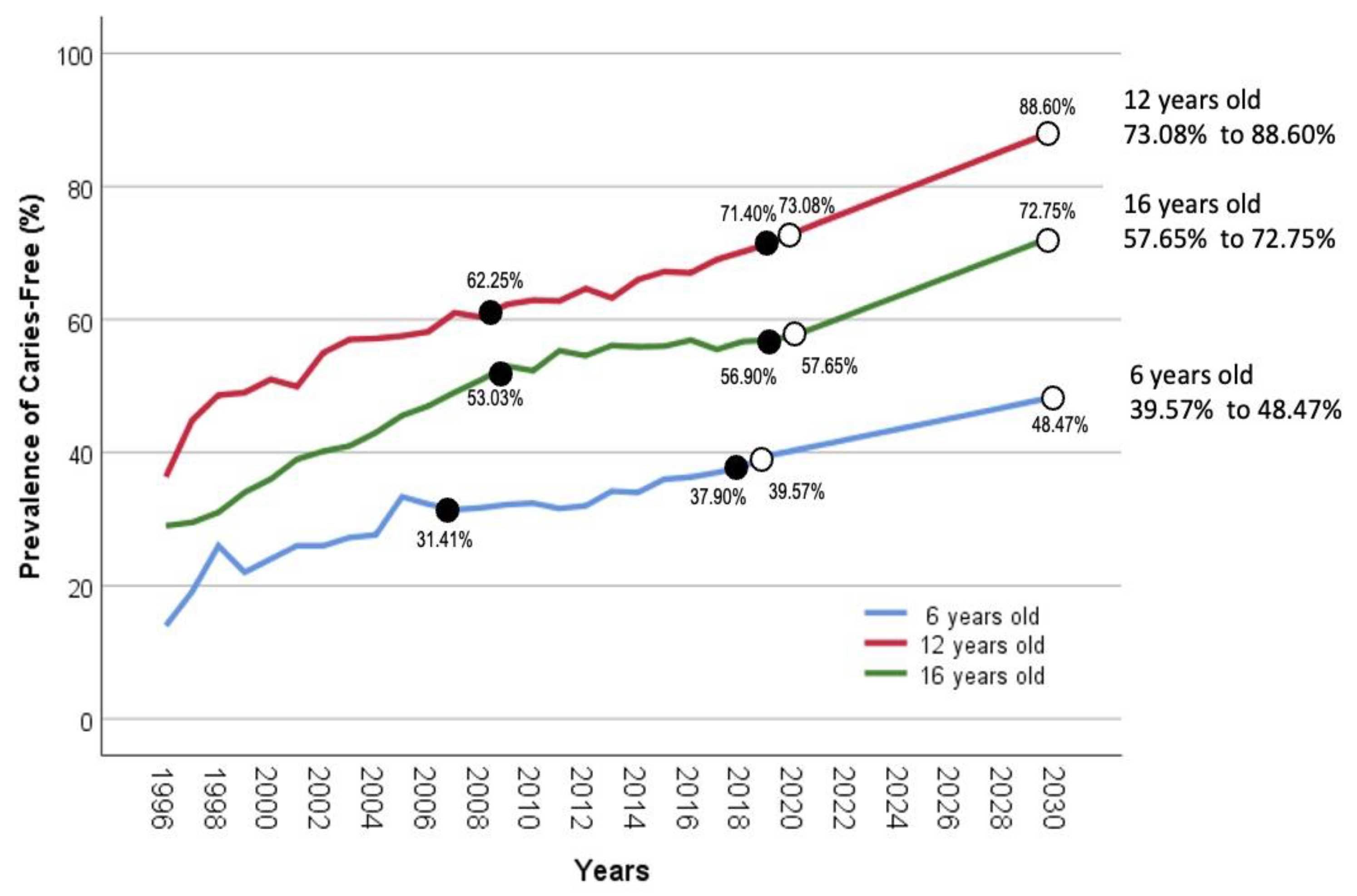
3.4. Projection of Caries-Free Prevalence among Schoolchildren
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sudhanthar, S.; Lapinski, J.; Turner, J.; Gold, J.; Sigal, Y.; Thakur, K.; Napolova, O.; Stiffler, M. Improving oral health through dental fluoride varnish application in a primary care paediatric practice. BMJ Open Qual. 2019, 8, e000589. [Google Scholar] [CrossRef] [PubMed]
- Quock, R.L. Dental caries: A current understanding and implications. J. Nat. Sci. 2015, 1, 27. [Google Scholar]
- Philip, N.; Suneja, B.; Walsh, L. Beyond Streptococcus mutans: Clinical implications of the evolving dental caries aetiological paradigms and its associated microbiome. Br. Dent. J. 2018, 224, 219–225. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sugars and Dental Caries; WHO: Geneva, Switzerland, 2017.
- Mendes, F.M.; Braga, M.M. Caries detection in primary teeth is less challenging than in permanent teeth. Dent. Hypotheses 2013, 4, 17. [Google Scholar] [CrossRef]
- Basheer, A.; Jaidka, S. Prevalence of dental caries in school children aged 5 to 16 years. J. Adv. Med. Dent. Sci. Res. 2019, 7, 24–26. [Google Scholar]
- Pitts, N.; Mayne, C. A Global Consensus for Achieving a Dental Cavity-Free Future 2021; King’s College London: London, UK, 2021; pp. 1–36. [Google Scholar]
- Swarna Nantha, Y. Addiction to sugar and its link to health morbidity: A primer for newer primary care and public health initiatives in Malaysia. J. Prim. Care Community Health 2014, 5, 263–270. [Google Scholar] [CrossRef]
- Goh, E.V.; Azam-Ali, S.; McCullough, F.; Roy Mitra, S. The nutrition transition in Malaysia; key drivers and recommendations for improved health outcomes. BMC Nutr. 2020, 6, 32. [Google Scholar] [CrossRef]
- Zahara, A.; Fashihah, M.; Nurul, A. Relationship between frequency of sugary food and drink consumption with occurrence of dental caries among preschool children in Titiwangsa, Kuala Lumpur. Malays. J. Nutr. 2010, 16, 83–90. [Google Scholar]
- Amarra, M.S.V.; Khor, G.L.; Chan, P. Intake of added sugar in Malaysia: A review. Asia Pac. J. Clin. Nutr. 2016, 25, 227–240. [Google Scholar]
- Sheiham, A.; James, W. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- Weeratunga, P.; Jayasinghe, S.; Perera, Y.; Jayasena, G.; Jayasinghe, S. Per capita sugar consumption and prevalence of diabetes mellitus–global and regional associations. BMC Public Health 2014, 14, 186. [Google Scholar] [CrossRef]
- Edney, L.; Afzali, H.H.A.; Cheng, T.; Karnon, J. Mortality reductions from marginal increases in public spending on health. Health Policy 2018, 122, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Bjørndal, L.; Simon, S.; Tomson, P.; Duncan, H. Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 949–973. [Google Scholar] [CrossRef]
- Moysés, S.J. Inequalities in oral health and oral health promotion. Braz. Oral Res. 2012, 26, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health; WHO: Geneva, Switzerland, 2022.
- Safiri, S.; Kelishadi, R.; Heshmat, R.; Rahimi, A.; Djalalinia, S.; Ghasemian, A.; Sheidaei, A.; Motlagh, M.E.; Ardalan, G.; Mansourian, M. Socioeconomic inequality in oral health behavior in Iranian children and adolescents by the Oaxaca-Blinder decomposition method: The CASPIAN-IV study. Int. J. Equity Health 2016, 15, 143. [Google Scholar] [CrossRef]
- Mullane, D.O.; Baez, R.; Jones, S.; Lennon, M.; Petersen, P.; Rugg-Gunn, A.; Whelton, H.; Whitford, G.M. Fluoride and oral health. Community Dent. Health 2016, 33, 69–99. [Google Scholar]
- Do, L.; Ha, D.; Roberts-Thomson, K.; Jamieson, L.; Peres, M.; Spencer, A. Race-and income-related inequalities in oral health in Australian children by fluoridation status. JDR Clin. Transl. Res. 2018, 3, 170–179. [Google Scholar] [CrossRef]
- Glick, M.; Williams, D.M.; Yahya, I.B.; Bondioni, E.; Cheung, W.W.; Clark, P.; Jagait, C.K.; Listl, S.; Mathur, M.R.; Mossey, P. Vision 2030: Delivering Optimal Oral Health for All; FDI World Dental Federation: Geneva, Switzerland, 2021; Available online: https://www.fdiworlddental.org/vision2030 (accessed on 10 December 2021).
- Hyndman, R.; Athanasopoulos, G. Forecasting: Principles and Practice, 2nd ed.; OTexts: Melbourne, Australia, 2018. [Google Scholar]
- Ministry of Health. Annual Report 2018; Ministry of Health Malaysia: Putrajaya, Malaysia, 2018. Available online: https://hq.moh.gov.my/ohd/images/pdf/annual_rpt/annual_rpt18.pdf (accessed on 8 December 2022).
- Department of Statistics Malaysia, Official Portal. 2023. Available online: https://www.dosm.gov.my/portal-main/article/background-role-function/ (accessed on 15 January 2023).
- Food and Agriculture Organization. Food and Agriculture Data 2019; FAO: Rome, Italy, 2019. [Google Scholar]
- Machiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A. Terminology of dental caries and dental caries management: Consensus report of a workshop organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef]
- Twumasi-Ankrah, S.; Odoi, B.; Adoma Pels, W.; Gyamfi, E.H. Efficiency of Imputation Techniques in Univariate Time Series. Int. J. Sci. Environ. Technol. 2019, 8, 430–453. [Google Scholar]
- Majid, G.; Bakhshandeh, S.; Shirvani, A.; Emadi, N.; Samadzadeh, H.; Fatemi, N.M.; Ghasemian, A. Dental caries experience and socio-economic status among Iranian children: A multilevel analysis. BMC Public Health 2019, 19, 1569. [Google Scholar]
- Van den Bos Verma, M.; de Vreede, L.; Achterbosch, T.; Rutten, M.M. Consumers discard a lot more food than widely believed: Estimates of global food waste using an energy gap approach and affluence elasticity of food waste. PLoS ONE 2020, 15, e0228369. [Google Scholar]
- Masood, M.; Yusof, N.; Hassan, M.I.A.; Jaafar, N. Assessment of dental caries predictors in 6-year-old school children-results from 5-year retrospective cohort study. BMC Public Health 2012, 12, 989. [Google Scholar] [CrossRef]
- Baldwin, K.; Schmidhuber, J.; Prakash, A.; Browning, J.; Kao, M.; Fabi, C. Guidelines for the Compilation of Food Balance Sheets; Global Strategy: Rome, Italy, 2017. [Google Scholar]
- Zhang, Z. Model building strategy for logistic regression: Purposeful selection. Ann. Transl. Med. 2016, 4, 111. [Google Scholar] [CrossRef]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013; Volume 398. [Google Scholar]
- Gogtay, N.J.; Thatte, U.M. Principles of correlation analysis. J. Assoc. Physicians India 2017, 65, 78–81. [Google Scholar] [PubMed]
- Akinwande, M.O.; Dikko, H.G.; Samson, A. Variance inflation factor: As a condition for the inclusion of suppressor variable(s) in regression analysis. Open J. Stat. 2015, 5, 754. [Google Scholar] [CrossRef]
- Appiah, S.T.; Buabeng, A.; Dumakor-Dupey, N. Multivariate Analysis of the Effect of Climate Conditions on Gold Production in Ghana. Ghana Min. J. 2018, 18, 72–77. [Google Scholar] [CrossRef]
- Ministry of Education. Malaysia Educational Statistics; Ministry of Education Malaysia: Putrajaya, Malaysia, 2019; pp. 1–51. Available online: https://www.moe.gov.my/menumedia/media-cetak/penerbitan/quick-facts/2722-quick-facts-2019/file (accessed on 19 January 2023).
- Ruhaya, H.; Jaafar, N.; Jamaluddin, M.; Ismail, A.R.; Ismail, N.M.; Badariah, T.C.; Mat, A.; Mohamed, S.Z. Nutritional status and early childhood caries among preschool children in Pasir Mas, Kelantan, Malaysia. Arch. Orofac. Sci. 2012, 7, 56–62. [Google Scholar]
- Van Loveren, C. Sugar restriction for caries prevention: Amount and frequency. Which is more important? Caries Res. 2019, 53, 168–175. [Google Scholar] [CrossRef]
- Skafida, V.; Chambers, S. Positive association between sugar consumption and dental decay prevalence independent of oral hygiene in pre-school children: A longitudinal prospective study. J. Public Health 2018, 40, e275–e283. [Google Scholar] [CrossRef]
- Qian, D.; Fu, M.; Zhou, Y.; Cao, Y.; Guo, T.; Zhou, Z.; Li, M.; Peng, X.; Zheng, X.; Li, Y. Sucrose promotes caries progression by disrupting the microecological balance in oral biofilms: An in vitro study. Sci. Rep. 2020, 10, 2961. [Google Scholar]
- Wang, J.; Jin, G.; Gu, K.; Sun, J.; Zhang, R.; Jiang, X. Association between milk and dairy product intake and the risk of dental caries in children and adolescents: NHANES 2011–2016. Asia Pac. J. Clin. Nutr. 2021, 30, 283–290. [Google Scholar]
- Bohari, N.F.M.; Kruger, E.; John, J.; Tennant, M. Analysis of dental services distribution in Malaysia: A geographic information systems–based approach. Int. Dent. J. 2019, 69, 223–229. [Google Scholar] [CrossRef]
- Nguyen, D.H.; Martin, J.T. Common dental infections in the primary care setting. Am. Fam. Physician 2008, 77, 797–802. [Google Scholar]
- Goldberg, M. Deciduous tooth and dental caries. Ann. Pediatr. Child Health 2017, 5, 1120. [Google Scholar]
- Ministry of Health. National Oral Health Survey of School Children 2017. Vol. II: Oral Health Status 12-Year-Old School Children; Ministry of Health Malaysia: Putrajaya, Malaysia, 2017. Available online: https://hq.moh.gov.my/ohd/images/pdf/research/NHMS%202017%20NOHSS%202017%20Vol%20II%20Oral%20Health%20Status%20of%2012%20yr%20olds.pdf (accessed on 12 December 2022).
- Ministry of Health. Garis Panduan Perkhidmatan Kesihatan Pergigian Sekolah; Ministry of Health Malaysia: Putrajaya, Malaysia, 2022. Available online: https://hq.moh.gov.my/ohd/images/pdf/xtvtnsop/gp_perkhidmatan_sekolah.pdf (accessed on 5 January 2023).
- Ministry of Health. Annual Report 2020; Oral Health Division, Ministry of Health Malaysia: Putrajaya, Malaysia, 2020. Available online: https://hq.moh.gov.my/ohd/images/pdf/annual_rpt/annual_%20rpt20.pdf (accessed on 10 January 2023).
- Anwar, N.H.; Nor, N.A.M.; Yusof, Z.Y.M. Effect of the SIMS program on oral hygiene levels of 5–6-year-old children in the Kampar District, Malaysia: A cluster-randomized controlled trial. Makara J. Health Res. 2020, 24, 9. [Google Scholar]
- Zemaitiene, M.; Grigalauskiene, R.; Andruskeviciene, V.; Matulaitiene, Z.K.; Zubiene, J.; Narbutaite, J.; Slabsinskiene, E. Dental caries risk indicators in early childhood and their association with caries polarization in adolescence: A cross-sectional study. BMC Oral Health 2017, 17, 2. [Google Scholar] [CrossRef]
- Alotaibi, W.M.; Habbal, N.H.; Alghamdi, S.A.; Alanazi, M.O.; Alblowi, S.S.; Aljohani, A.M.; Aljohani, R.M. Dental Caries in Relation to Obesity in Children: A Systematic Review and Meta-analysis. Ann. Med. Health Sci. Res. 2020, 10, 1029–1033. [Google Scholar]
- Williams, S.; Wei, L.; Griffin, S.O.; Thornton-Evans, G. Untreated caries among US working-aged adults and association with reporting need for oral health care. J. Am. Dent. Assoc. 2021, 152, 55–64. [Google Scholar] [CrossRef]
- Gazzaz, A.Z. Family Socioeconomic Status, Psychosocial Factors, and Oral Health in Children and Adolescents; University of British Columbia: Vancouver, BC, Canada, 2022. [Google Scholar]
- Zaman, S.B.; Hossain, N.; Mehta, V.; Sharmin, S.; Mahmood, S.A.I. An association of total health expenditure with GDP and life expectancy. J. Med. Res. Innov. 2017, 1, AU7–AU12. [Google Scholar] [CrossRef]
- Siami-Namini, S. Healthcare Expenditure, Economic Growth, and Inflation in the G7 Countries: A Panel Cointegration Approach. Res. J. Econ. 2018, 8, 2. [Google Scholar]
- Zhang, X.; Zhang, L.; Zhang, Y.; Liao, Z.; Song, J. Predicting trend of early childhood caries in mainland China: A combined meta-analytic and mathematical modelling approach based on epidemiological surveys. Sci. Rep. 2017, 7, 6507. [Google Scholar] [CrossRef] [PubMed]
- Aoun, A.; Darwiche, F.; Al Hayek, S.; Doumit, J. The fluoride debate: The pros and cons of fluoridation. Prev. Nutr. Food Sci. 2018, 23, 171. [Google Scholar] [CrossRef] [PubMed]
- Pollick, H. The role of fluoride in the prevention of tooth decay. Pediatr. Clin. 2018, 65, 923–940. [Google Scholar] [CrossRef]
- Maharani, D.A.; Zhang, S.; Gao, S.S.; Chu, C.-H.; Rahardjo, A. Dental caries and the erosive tooth wear status of 12-year-old children in Jakarta, Indonesia. Int. J. Environ. Res. Public Health 2019, 16, 2994. [Google Scholar] [CrossRef]
- Sitthisettapong, T.; Tasanarong, P.; Phantumvanit, P. Strategic Management of Early Childhood Caries in Thailand: A Critical Overview. Front. Public Health 2021, 9, 664541. [Google Scholar] [CrossRef]
- Wang, K.; Pang, L.; Fan, C.; Cui, T.; Yu, L.; Lin, H. Enamel and dentin caries risk factors of adolescents in the context of the international caries detection and assessment system (ICDAS): A longitudinal study. Front. Pediatr. 2020, 8, 419. [Google Scholar] [CrossRef]
- Mahfouz, M.; Abu Esaid, A. Dental caries prevalence among 12–15 year old Palestinian children. Int. Sch. Res. Not. 2014, 2014, 785404. [Google Scholar] [CrossRef]
- Obregón-Rodríguez, N.; Fernández-Riveiro, P.; Piñeiro-Lamas, M.; Smyth-Chamosa, E.; Montes-Martínez, A.; Suárez-Cunqueiro, M.M. Prevalence and caries-related risk factors in schoolchildren of 12-and 15-year-old: A cross-sectional study. BMC Oral Health 2019, 19, 120. [Google Scholar] [CrossRef]


{kind=link}
| Age Group | Correlation Pair | Correlation Coefficient (r) | p-Value * |
|---|---|---|---|
| 6 years old | GDP vs. caries-free | 0.841 | <0.001 |
| CPI vs. caries-free | 0.901 | <0.001 | |
| Household income vs. caries-free | 0.819 | <0.001 | |
| Relative poverty vs. caries-free | −0.693 | <0.001 | |
| Sugar consumption vs. caries-free | −0.505 | 0.014 | |
| Fluoridated water vs. caries-free | 0.790 | <0.001 | |
| 12 years old | GDP vs. caries-free | 0.893 | <0.001 |
| CPI vs. caries-free | 0.943 | <0.001 | |
| Household income vs. caries-free | 0.869 | <0.001 | |
| Relative poverty vs. caries-free | −0.698 | <0.001 | |
| Sugar consumption vs. caries-free | −0.391 | 0.050 | |
| Fluoridated water vs. caries-free | 0.771 | 0.001 | |
| 16 years old | GDP vs. caries-free | 0.881 | <0.001 |
| CPI vs. caries-free | 0.936 | <0.001 | |
| Household income vs. caries-free | 0.840 | <0.001 | |
| Relative Poverty vs. caries-free | −0.686 | <0.001 | |
| Sugar consumption vs. caries-free | −0.340 | 0.104 | |
| Fluoridated water vs. caries-free | 0.867 | <0.001 |
| Age | Associated Factors | Coefficient (95% CI) | Standard Error | p-Value * | VIF | R2 |
|---|---|---|---|---|---|---|
| 6 | Household Income | 2.6 × 10−3 (0.002, 0.003) | 3.6 × 10−4 | <0.001 | 2.13 | 0.945 |
| Sugar consumption | −0.06 (−0.08, −0.05) | 0.007 | <0.001 | 1.03 | ||
| Water fluoridation | 0.34 (0.16, 0.53) | 0.089 | 0.001 | 2.17 | ||
| 12 | GDP | 1 × 10−3 (8 × 10−4, 1.4 × 10−3) | 1.3 × 10−4 | <0.001 | 2.16 | 0.931 |
| Sugar consumption | −0.07 (−0.09, −0.04) | 0.012 | <0.001 | 1.02 | ||
| Water fluoridation | 0.31 (0.01, 0.61) | 0.144 | 0.044 | 2.20 | ||
| 16 | GDP | 9.0 × 10−4 (0.001, 0.002) | 1.2 × 10−4 | <0.001 | 2.16 | 0.949 |
| Sugar consumption | −0.06 (−0.08, −0.03) | 0.011 | <0.001 | 1.02 | ||
| Water fluoridation | 0.78 (0.49, 1.07) | 0.138 | <0.001 | 2.20 |
| Model | Age Group | Variables | Coefficients | SE | p-Value | Ljung Box Test (p-Value) |
|---|---|---|---|---|---|---|
| Regression with ARMA (0,0,1) Errors | 12 years old | GDP Water fluoridation | 0.0012 0.215 | 0.0002 0.177 | <0.001 <0.044 | 0.113 |
| Sugar & sweetener | −0.063 | 0.013 | 0.044 |
| Age Group | Forecasted Years | Significant Associated Factors | Prevalence of Caries-Free (%) | ||
|---|---|---|---|---|---|
| Household Income (MYR) (Brown Linear) | Sugar Consumption (kcal/Capita/Day) (Damped Trend) | Water Fluoridation (%) (ARIMA 0,1,0) | |||
| 6 years old | 2019 | 5873.00 | 413.59 | 74.62 | 39.57 |
| 2020 | 6088.00 | 414.02 | 75.15 | 40.37 | |
| 2021 | 6303.00 | 414.39 | 75.67 | 41.17 | |
| 2022 | 6518.00 | 414.70 | 76.19 | 41.97 | |
| 2023 | 6733.00 | 414.98 | 76.71 | 42.78 | |
| 2024 | 6948.00 | 415.21 | 77.24 | 43.59 | |
| 2025 | 7163.00 | 415.42 | 77.76 | 44.40 | |
| 2026 | 7378.00 | 415.59 | 78.28 | 45.21 | |
| 2027 | 7593.00 | 415.74 | 78.80 | 46.02 | |
| 2028 | 7808.00 | 415.87 | 79.33 | 46.84 | |
| 2029 | 8023.00 | 415.98 | 79.85 | 47.66 | |
| 2030 | 8238.00 | 416.08 | 80.37 | 48.47 | |
| GDP (Million MYR) (Brown Linear) | Sugar consumption (kcal/capita/day) (Damped trend) | Water Fluoridation (%) (Damped trend) | |||
| 12 years old | 2020 | 40,439.16 | 413.37 | 73.35 | 73.08 |
| 2021 | 41,685.26 | 413.82 | 73.80 | 74.69 | |
| 2022 | 42,931.36 | 414.20 | 74.24 | 76.22 | |
| 2023 | 44,177.45 | 414.53 | 74.69 | 77.76 | |
| 2024 | 45,423.55 | 414.82 | 75.14 | 79.30 | |
| 2025 | 46,669.65 | 415.06 | 75.59 | 80.85 | |
| 2026 | 47,915.75 | 415.27 | 76.03 | 82.39 | |
| 2027 | 49,161.85 | 415.45 | 76.48 | 83.94 | |
| 2028 | 50,407.95 | 415.61 | 76.93 | 85.49 | |
| 2029 | 51,654.05 | 415.75 | 77.38 | 87.04 | |
| 2030 | 52,900.15 | 415.86 | 77.83 | 88.60 | |
| GDP (Million MYR) (Brown Linear) | Sugar consumption (kcal/capita/day) (Damped trend) | Water Fluoridation (%) (Damped trend) | |||
| 16 years old | 2020 | 40,439.16 | 57.65 | 73.35 | 57.65 |
| 2021 | 41,685.26 | 59.15 | 73.80 | 59.15 | |
| 2022 | 42,931.36 | 60.65 | 74.24 | 60.65 | |
| 2023 | 44,177.45 | 62.16 | 74.69 | 62.16 | |
| 2024 | 45,423.55 | 63.66 | 75.14 | 63.66 | |
| 2025 | 46,669.65 | 65.18 | 75.59 | 65.18 | |
| 2026 | 47,915.75 | 66.68 | 76.03 | 66.68 | |
| 2027 | 49,161.85 | 68.20 | 76.48 | 68.20 | |
| 2028 | 50,407.95 | 69.71 | 76.93 | 69.71 | |
| 2029 | 51,654.05 | 71.23 | 77.38 | 71.23 | |
| 2030 | 52,900.15 | 72.75 | 77.83 | 72.75 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najihah, L.; Wan Husin, W.Z.; Marhazlinda, J. Multivariable Projections of Caries-Free Prevalence and the Associated Factors from 2019 to 2030 among Schoolchildren Aged 6, 12 and 16-Year-Old in Malaysia. Children 2023, 10, 1125. https://doi.org/10.3390/children10071125
Najihah L, Wan Husin WZ, Marhazlinda J. Multivariable Projections of Caries-Free Prevalence and the Associated Factors from 2019 to 2030 among Schoolchildren Aged 6, 12 and 16-Year-Old in Malaysia. Children. 2023; 10(7):1125. https://doi.org/10.3390/children10071125
Chicago/Turabian StyleNajihah, Lokman, Wan Zakiyatussariroh Wan Husin, and Jamaludin Marhazlinda. 2023. "Multivariable Projections of Caries-Free Prevalence and the Associated Factors from 2019 to 2030 among Schoolchildren Aged 6, 12 and 16-Year-Old in Malaysia" Children 10, no. 7: 1125. https://doi.org/10.3390/children10071125
APA StyleNajihah, L., Wan Husin, W. Z., & Marhazlinda, J. (2023). Multivariable Projections of Caries-Free Prevalence and the Associated Factors from 2019 to 2030 among Schoolchildren Aged 6, 12 and 16-Year-Old in Malaysia. Children, 10(7), 1125. https://doi.org/10.3390/children10071125