
Use of Pulse Oximetry during Resuscitation of 230 Newborns—A Video Analysis


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Data Collection and Equipment
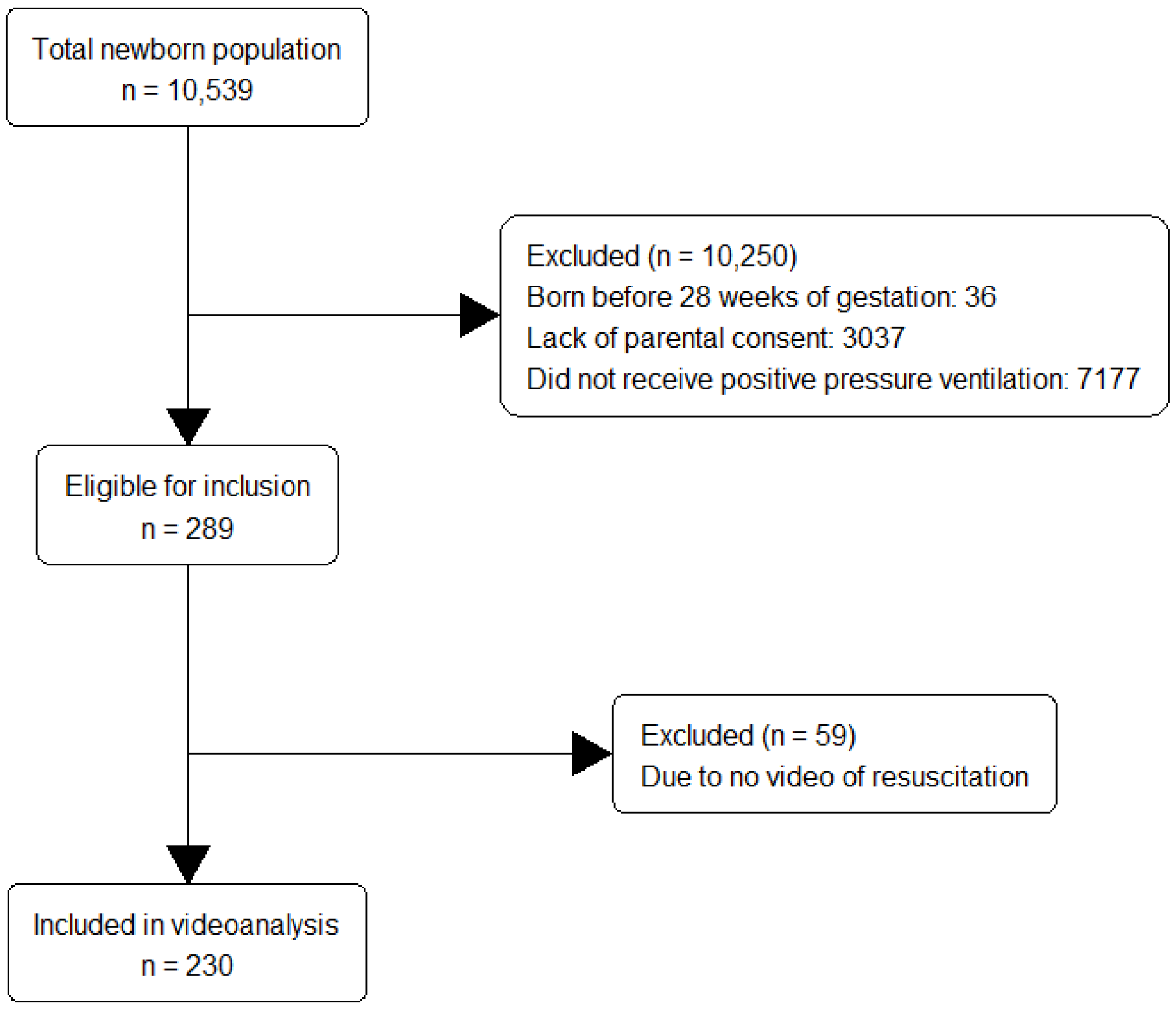
2.3. Inclusion Criteria
2.4. Calculations and Definitions
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Use of Auscultation, ECG and PO Assessment during Resuscitation
3.2. Number of HCPs Involved and Equipment Used for Application and Adjustment of PO
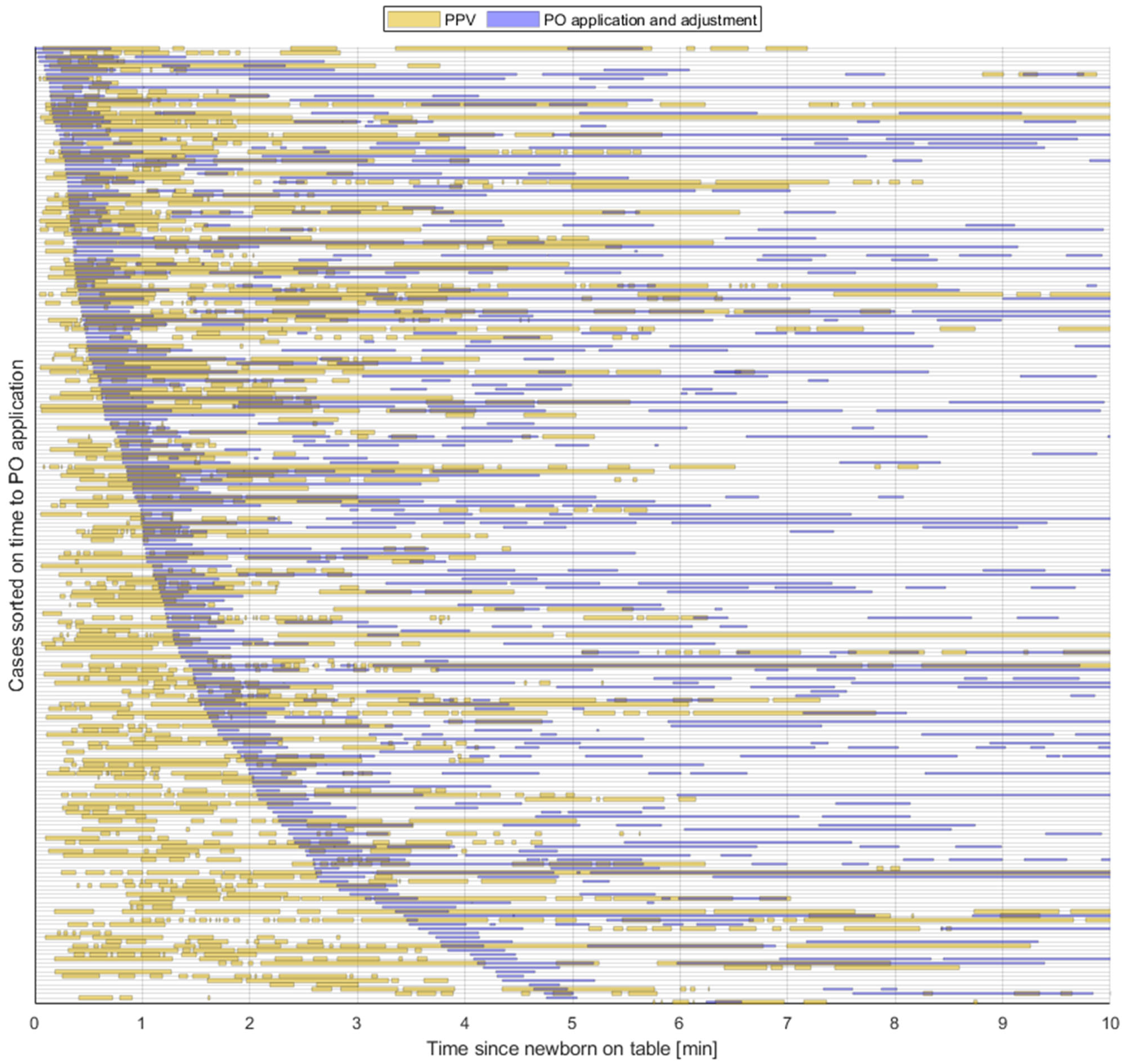
3.3. Time Spent on the Application and Adjustment of PO
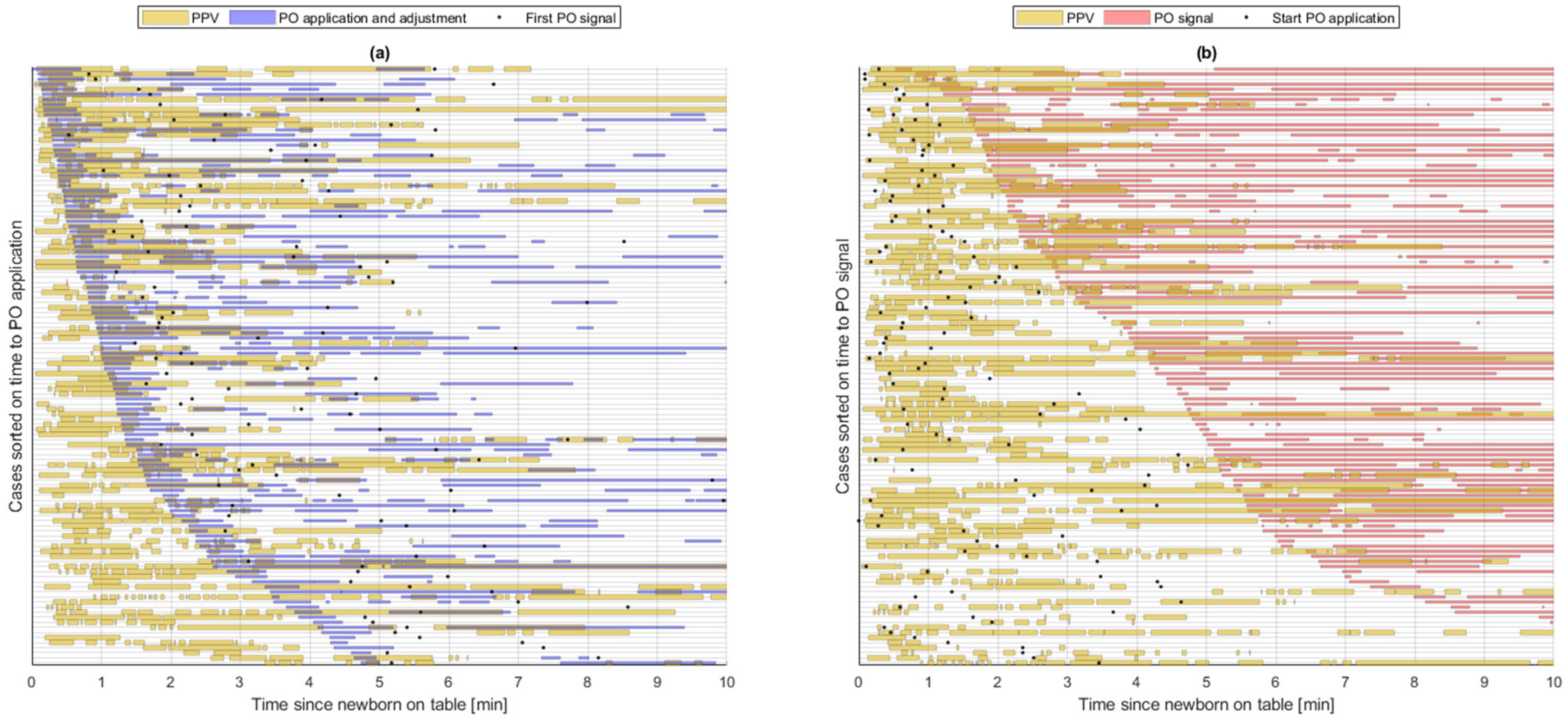
3.4. Feedback on PO Signal
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skare, C.; Kramer-Johansen, J.; Steen, T.; Odegaard, S.; Niles, D.E.; Nakstad, B.; Solevag, A.L.; Nadkarni, V.M.; Olasveengen, T.M. Incidence of Newborn Stabilization and Resuscitation Measures and Guideline Compliance during the First Minutes of Life in Norway. Neonatology 2015, 108, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rudiger, M.; Skare, C.; Szczapa, T.; Te Pas, A.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.W.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation 2020, 156, A156–A187. [Google Scholar] [CrossRef] [PubMed]
- Bjorland, P.A.; Oymar, K.; Ersdal, H.L.; Rettedal, S.I. Incidence of newborn resuscitative interventions at birth and short-term outcomes: A regional population-based study. BMJ Paediatr. Open 2019, 3, e000592. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Greif, R.; Morley, P.T.; Ng, K.C.; Olasveengen, T.M.; Singletary, E.M.; Soar, J.; Cheng, A.; Drennan, I.R.; Liley, H.G.; et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations: Summary from the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation 2022, 146, e483–e557. [Google Scholar] [CrossRef]
- Kamlin, C.O.; O’Donnell, C.P.; Everest, N.J.; Davis, P.G.; Morley, C.J. Accuracy of clinical assessment of infant heart rate in the delivery room. Resuscitation 2006, 71, 319–321. [Google Scholar] [CrossRef]
- Bjorland, P.A.; Ersdal, H.L.; Oymar, K.; Rettedal, S.I. Compliance with guidelines and efficacy of heart rate monitoring during newborn resuscitation: A prospective video study. Neonatology 2020, 117, 175–181. [Google Scholar] [CrossRef]
- Katheria, A.; Rich, W.; Finer, N. Electrocardiogram provides a continuous heart rate faster than oximetry during neonatal resuscitation. Pediatrics 2012, 130, e1177–e1181. [Google Scholar] [CrossRef]
- Iglesias, B.; Rodriguez, M.J.; Aleo, E.; Criado, E.; Herranz, G.; Moro, M.; Martinez Orgado, J.; Arruza, L. Pulse oximetry versus electrocardiogram for heart rate assessment during resuscitation of the preterm infant. Anales Pediatría 2016, 84, 271–277. [Google Scholar] [CrossRef]
- Mizumoto, H.; Tomotaki, S.; Shibata, H.; Ueda, K.; Akashi, R.; Uchio, H.; Hata, D. Electrocardiogram shows reliable heart rates much earlier than pulse oximetry during neonatal resuscitation. Pediatr. Int. 2012, 54, 205–207. [Google Scholar] [CrossRef]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; Kim, H.S.; Liley, H.G.; Mildenhall, L.; Simon, W.M.; et al. Part 7: Neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015, 132 (Suppl. S1), S204–S241. [Google Scholar] [CrossRef]
- van Vonderen, J.J.; Hooper, S.B.; Kroese, J.K.; Roest, A.A.; Narayen, I.C.; van Zwet, E.W.; te Pas, A.B. Pulse oximetry measures a lower heart rate at birth compared with electrocardiography. J. Pediatr. 2015, 166, 49–53. [Google Scholar] [CrossRef]
- Johnson, P.A.; Cheung, P.Y.; Lee, T.F.; O’Reilly, M.; Schmolzer, G.M. Novel technologies for heart rate assessment during neonatal resuscitation at birth—A systematic review. Resuscitation 2019, 143, 196–207. [Google Scholar] [CrossRef]
- Dawson, J.A.; Saraswat, A.; Simionato, L.; Thio, M.; Kamlin, C.O.; Owen, L.S.; Schmölzer, G.M.; Davis, P.G. Comparison of heart rate and oxygen saturation measurements from Masimo and Nellcor pulse oximeters in newly born term infants. Acta Paediatr. 2013, 102, 955–960. [Google Scholar] [CrossRef]
- Rettedal, S.; Eilevstjonn, J.; Kibsgaard, A.; Kvaloy, J.T.; Ersdal, H. Comparison of Heart Rate Feedback from Dry-Electrode ECG, 3-Lead ECG, and Pulse Oximetry during Newborn Resuscitation. Children 2021, 8, 1092. [Google Scholar] [CrossRef]
- Narayen, I.C.; Smit, M.; van Zwet, E.W.; Dawson, J.A.; Blom, N.A.; te Pas, A.B. Low signal quality pulse oximetry measurements in newborn infants are reliable for oxygen saturation but underestimate heart rate. Acta Paediatr. 2015, 104, e158–e163. [Google Scholar] [CrossRef]
- Iglesias, B.; Rodri Guez, M.A.J.; Aleo, E.; Criado, E.; Marti Nez-Orgado, J.; Arruza, L. 3-lead electrocardiogram is more reliable than pulse oximetry to detect bradycardia during stabilisation at birth of very preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F233–F237. [Google Scholar] [CrossRef]
- Dawson, J.A.; Davis, P.G.; O’Donnell, C.P.; Kamlin, C.O.; Morley, C.J. Pulse oximetry for monitoring infants in the delivery room: A review. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F4–F7. [Google Scholar] [CrossRef]
- Reddy, K.S.; Venkataravanappa, S.T.; Gururaja, G. Feasibility of Oxygen Saturation Monitoring During Neonatal Resuscitation in Indian Scenario. Indian Pediatr. 2018, 55, 999. [Google Scholar] [CrossRef]
- Gandhi, B.; Rich, W.; Finer, N. Time to achieve stable pulse oximetry values in VLBW infants in the delivery room. Resuscitation 2013, 84, 970–973. [Google Scholar] [CrossRef]
- Louis, D.; Sundaram, V.; Kumar, P. Pulse oximeter sensor application during neonatal resuscitation: A randomized controlled trial. Pediatrics 2014, 133, 476–482. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.P.; Kamlin, C.O.; Davis, P.G.; Morley, C.J. Obtaining pulse oximetry data in neonates: A randomised crossover study of sensor application techniques. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F84–F85. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, A.; Simionato, L.; Dawson, J.A.; Thio, M.; Kamlin, C.O.; Owen, L.; Schmolzer, G.; Davis, P.G. Determining the best method of Nellcor pulse oximeter sensor application in neonates. Acta Paediatr. 2012, 101, 484–487. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.P.; Kamlin, C.O.; Davis, P.G.; Morley, C.J. Feasibility of and delay in obtaining pulse oximetry during neonatal resuscitation. J. Pediatr. 2005, 147, 698–699. [Google Scholar] [CrossRef]
- Baquero, H.; Alviz, R.; Castillo, A.; Neira, F.; Sola, A. Avoiding hyperoxemia during neonatal resuscitation: Time to response of different SpO2 monitors. Acta Paediatr. 2011, 100, 515–518. [Google Scholar] [CrossRef]
- Boldingh, A.M.; Skare, C.; Nakstad, B.; Solevag, A.L. Suboptimal heart rate assessment and airway management in infants receiving delivery room chest compressions: A quality assurance project. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 545–549. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Newborn Characteristics n = 230 | |
|---|---|
| Variable | |
| Gestational age (weeks) | 40 (38, 40) |
| Very preterm (28 to <32 weeks) | 5 (2.2%) |
| Moderate preterm (32 to <34 weeks) | 7 (3.0%) |
| Late preterm (34 to <37 weeks) | 21 (9.1%) |
| Term (≥37 weeks) | 197 (85.7%) |
| Weight (grams) | 3565 (3042, 3914) |
| Female gender n (%) | 100 (44%) |
| Apgar | |
| 1 min Apgar | 5 (4, 7) |
| 5 min Apgar | 8 (6, 9) |
| 10 min Apgar | 9 (8, 10) |
| Umbilical cord values | |
| Arterial pH (n = 184) | 7.20 (7.11, 7.25) |
| Arterial base excess (n = 176) | 4.34 (1.67, 6.13) |
| Arterial pCO2 (n = 175) | 8.16 (7.14, 9.64) |
| Pulse oximetry n (%) | 222 (97%) |
| Positive pressure ventilation duration (seconds) | 126 (65, 232) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolstad, V.; Pike, H.; Eilevstjønn, J.; Buskov, F.; Ersdal, H.; Rettedal, S. Use of Pulse Oximetry during Resuscitation of 230 Newborns—A Video Analysis. Children 2023, 10, 1124. https://doi.org/10.3390/children10071124
Kolstad V, Pike H, Eilevstjønn J, Buskov F, Ersdal H, Rettedal S. Use of Pulse Oximetry during Resuscitation of 230 Newborns—A Video Analysis. Children. 2023; 10(7):1124. https://doi.org/10.3390/children10071124
Chicago/Turabian StyleKolstad, Vilde, Hanne Pike, Joar Eilevstjønn, Frederikke Buskov, Hege Ersdal, and Siren Rettedal. 2023. "Use of Pulse Oximetry during Resuscitation of 230 Newborns—A Video Analysis" Children 10, no. 7: 1124. https://doi.org/10.3390/children10071124
APA StyleKolstad, V., Pike, H., Eilevstjønn, J., Buskov, F., Ersdal, H., & Rettedal, S. (2023). Use of Pulse Oximetry during Resuscitation of 230 Newborns—A Video Analysis. Children, 10(7), 1124. https://doi.org/10.3390/children10071124