
Supporting Preschoolers’ Mental Health and Academic Learning through the PROMEHS Program: A Training Study

 ,
,  ,
,  , , , and
, , , and
Abstract
1. Introduction
1.1. SEL Competencies and Mental Health
1.2. Children’s Mental Health and Early Learning Outcomes
1.3. School-Based Interventions in Preschool Settings and the PROMEHS Program
1.4. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Research Design and Procedure
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Main Features of the PROMEHS Program
| Whole-school approach. PROMEHS acknowledges the importance of collaborative work between students, teachers, families, school leaders, community stakeholders, and policymakers. |
| Universal. The implementation involves the entire school community and does not target only clinical or at-risk populations. |
| Multiple initiatives. The program includes training courses and supervision for teachers; meetings with school leaders, parents, and policymakers; guidelines and manualized activities to be carried out at school and at home; dissemination events for stakeholders. |
| Manualized and multi-year handbooks and glossaries. PROMEHS consists of seven handbooks that offer multi-year programming for students from 3 up to 18 years, their teachers, and parents. Two handbooks include guided activities that students and teachers can carry out at school, as part of the mainstream curriculum (one for kindergarten and primary school, and the other for lower and upper secondary school); two handbooks include guided activities that students can carry out at home, with their parents’ help and contribute. All the activities have been developed according to the S.A.F.E. approach [10]. The other three volumes—addressed to teachers, parents, and school leaders/policymakers—offer guidelines and recommendations for promoting mental health. Furthermore, two glossaries (one for kindergarten and primary school teachers, and one for lower and upper secondary teachers) are provided to support teachers’ mental health literacy. All the materials are available in seven languages (Croatian, English, Greek, Italian, Latvian, Portuguese, and Romanian). |
| Professional teachers’ training. The implementation includes the delivery of high-quality training composed of initial training and ongoing supervision to ensure robust and reliable implementation. Teachers are required to deliver the PROMEHS activities on a weekly basis during the regular school day. |
| Themes. The curriculum comprises three themes: the promotion of SEL; the promotion of resilience; the prevention of social, emotional, and behavioral problems. |
| Evidence-based approach. The program was evaluated by comparing the experimental and waiting list control groups at two-time points and analyzing any significant effects on teachers’ and students’ outcomes. The evaluation was conducted using a sample size that met the ESSA (Every Student Succeeds Act) criterion for offering large enough power to capture the program’s effects [84]. |
| Independent evaluation. The independent evaluators, who were not involved in the program’s development and implementation, reviewed the handbooks to reduce potential bias and ensure the reliability of the evaluation procedures and findings. |
| Quality of implementation. The program’s fidelity, dosage, quality, responsiveness, and adaptation are assessed [88]. |
| Multi-informant assessments. Multiple informants (students, teachers, and parents) were used to assess the program’s impact on students’ and teachers’ mental health. |
| Developmental perspective. The PROMEHS curriculum acknowledges that students’ and teachers’ mental health encompasses dynamic and multifaceted knowledge, skills, practices, and attitudes that may change over time. |
| Active family engagement. Student and parent handbooks are designed to reinforce the acquisition of skills and behaviors learned at school by applying them at home. |
| Sustainability. The PROMEHS program was developed through collaborative work with local, regional, national, and international policymakers to maximize the impact and sustainability of the results over time. |
References
- Meriem, C.; Khaoula, M.; Ghizlane, C.; Asmaa, M.A.; Ahmed, A.O.T. Early childhood development (0–6 years old) from healthy to pathologic: A review of the literature. Open J. Med. Psychol. 2020, 9, 100–122. [Google Scholar] [CrossRef]
- Bølstad, E.; Havighurst, S.S.; Tamnes, C.K.; Nygaard, E.; Bjørk, R.F.; Stavrinou, M.; Espeseth, T. A pilot study of a parent emotion socialization intervention: Impact on parent behavior, child self-regulation, and adjustment. Front. Psychol. 2021, 12, 730278. [Google Scholar] [CrossRef]
- McMahon, C.A.; Bernier, A. Twenty years of research on parental mind-mindedness: Empirical findings, theoretical and methodological challenges, and new directions. Dev. Rev. 2017, 46, 54–80. [Google Scholar] [CrossRef]
- Eurostat—Childcare Arrangements in the EU. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20220504-2 (accessed on 14 April 2023).
- European Parliamentary Research Service—Participation in Early Education and Care. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2021/696210/EPRS_BRI(2021)696210_EN.pdf (accessed on 14 April 2023).
- Ashdown, D.M.; Bernard, M.E. Can explicit instruction in social and emotional learning skills benefit the social-emotional development, well-being, and academic achievement of young children? Early Child. Educ. J. 2012, 39, 397–405. [Google Scholar] [CrossRef]
- Domitrovich, C.E.; Durlak, J.A.; Staley, K.C.; Weissberg, R.P. Social-emotional competence: An essential factor for promoting positive adjustment and reducing risk in school children. Child Dev. 2017, 88, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Schindler, H.S.; Kholoptseva, J.; Oh, S.S.; Yoshikawa, H.; Duncan, G.J.; Magnuson, K.A.; Shonkoff, J.P. Maximizing the potential of early childhood education to prevent externalizing behavior problems: A meta-analysis. J. Sch. Psychol. 2015, 53, 243–263. [Google Scholar] [CrossRef]
- Cavioni, V.; Grazzani, I.; Ornaghi, V.; Agliati, A.; Pepe, A. Adolescents’ mental health at school: The mediating role of life satisfaction. Front. Psychol. 2021, 12, 720628. [Google Scholar] [CrossRef]
- Learning Policy Institute—Evidence for Social and Emotional Learning in Schools. Available online: https://learningpolicyinstitute.org/product/evidence-social-emotional-learning-schools-report (accessed on 14 April 2023).
- Mahoney, J.L.; Weissberg, R.P.; Greenberg, M.T.; Dusenbury, L.; Jagers, R.J.; Niemi, K.; Schlinger, M.; Schlund, J.; Shriver, T.P.; VanAusdal, K.; et al. Systemic social and emotional learning: Promoting educational success for all preschool to high school students. Am. Psychol. 2021, 76, 1128–1142. [Google Scholar] [CrossRef]
- Collaborative for Academic, Social, and Emotional Learning—Keeping SEL Developmental: The Importance of a Developmental Lens for Fostering and Assessing SEL Competencies. Available online: https://casel.org/casel-resources-keeping-sel-developmental/ (accessed on 14 April 2023).
- Brownell, C.A.; Zerwas, S.; Ramani, G.B. ‘‘So big’’: The development of body self-awareness in toddlers. Child Dev. 2007, 78, 1426–1440. [Google Scholar] [CrossRef]
- Taumoepeau, M.; Reese, E. Understanding the self through siblings: Self-awareness mediates the sibling effect on social understanding. Soc. Dev. 2014, 23, 1–18. [Google Scholar] [CrossRef]
- Cavioni, V.; Grazzani, I.; Ornaghi, V.; Pepe, A.; Pons, F. Assessing the factor structure and measurement invariance of the Test of Emotion Comprehension (TEC): A large cross-sectional study with children aged 3-10 years. J. Cogn. Dev. 2020, 21, 406–424. [Google Scholar] [CrossRef]
- Conte, E.; Ornaghi, V.; Grazzani, I.; Pepe, A.; Cavioni, V. Emotion knowledge, theory of mind, and language in young children: Testing a comprehensive conceptual model. Front. Psychol. 2019, 10, 2144. [Google Scholar] [CrossRef]
- Grazzani, I.; Ornaghi, V.; Conte, E.; Pepe, A.; Caprin, C. The relation between emotion understanding and theory of mind in children aged 3 to 8: The key role of language. Front. Psychol. 2018, 9, 724. [Google Scholar] [CrossRef] [PubMed]
- Calkins, S.D.; Leerkes, E.M. Early attachment processes and the development of emotional self-regulation. In Handbook of Self-Regulation. Research, Theory, and Applications, 2nd ed.; Vohs, K.D., Baumeister, R.F., Eds.; The Guilford Press: New York, NY, USA, 2011; pp. 355–373. [Google Scholar]
- Kurki, K.; Järvenoja, H.; Järvelä, S.; Mykkänen, A. Young children’s use of emotion and behaviour regulation strategies in socio-emotionally challenging day-care situations. Early Child. Res. Q. 2017, 41, 50–62. [Google Scholar] [CrossRef]
- Silkenbeumer, J.R.; Schiller, E.; Kartner, J. Co- and self-regulation of emotions in the preschool setting. Early Child. Res. Q. 2018, 44, 72–81. [Google Scholar] [CrossRef]
- Gockeritz, S.; Schmidt, M.F.H.; Tomasello, M. Young children’s creation and transmission of social norms. Cogn. Dev. 2014, 30, 81–95. [Google Scholar] [CrossRef]
- Rakoczy, H.; Schmidt, M.F.H. The early ontogeny of social norms. Child Dev. Perspect. 2013, 7, 17–21. [Google Scholar] [CrossRef]
- Rossano, F.; Rakoczy, H.; Tomasello, M. Young children’s understanding of violations of property rights. Cognition 2011, 121, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.F.H.; Tomasello, M. Young children enforce social norms. Curr. Dir. Psychol. Sci. 2012, 21, 232–236. [Google Scholar] [CrossRef]
- Killen, M.; Mulvey, L.K.; Richardson, C.; Jampol, N.; Woodward, A. The accidental transgressor: Morally-relevant theory of mind. Cognition 2011, 119, 197–215. [Google Scholar] [CrossRef]
- Poulin-Dubois, D. Theory of mind development: State of the science and future directions. In New Perspectives on Early Social-Cognitive Development, 1st ed.; Hunnius, S., Meyer, M., Eds.; Elsevier: North Andover, MA, USA, 2020; Volume 254, pp. 141–166. [Google Scholar] [CrossRef]
- Cigala, A.; Mori, A.; Fangareggi, F. Learning others’ point of view: Perspective taking and prosocial behaviour in preschoolers. Early Child Dev. Care 2015, 185, 1199–1215. [Google Scholar] [CrossRef]
- Sette, S.; Baumgartner, E.; MacKinnon, D.P. Assessing social competence and behavior problems in a sample of Italian preschoolers using the Social Competence and Behavior Evaluation Scale. Early Educ. Dev. 2015, 26, 46–65. [Google Scholar] [CrossRef]
- Aslan, D.; Köksal Akyol, A. Impact of an empathy training program on children’s perspective-taking abilities. Psychol. Rep. 2020, 123, 2394–2409. [Google Scholar] [CrossRef] [PubMed]
- Mori, A.; Cigala, A. ‘Putting oneself in someone else’s shoes during childhood: How to learn it’ Training for preschool age children. Br. J. Educ. Psychol. 2019, 89, 750–766. [Google Scholar] [CrossRef]
- Ornaghi, V.; Grazzani, I.; Cherubin, E.; Conte, E.; Piralli, F. ‘Let’s talk about emotions!’. The effect of conversational training on preschoolers’ emotion comprehension and prosocial orientation. Soc. Dev. 2015, 24, 166–183. [Google Scholar] [CrossRef]
- January, A.M.; Casey, R.J.; Paulson, D. A meta-analysis of classroom-wide interventions to build social skills: Do they work? School Psychol. Rev. 2011, 40, 242–256. [Google Scholar] [CrossRef]
- Taylor, R.; Oberle, E.; Durlak, J.A.; Weissberg, R.P. Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef]
- Cavioni, V.; Grazzani, I.; Ornaghi, V. Mental health promotion in schools: A comprehensive theoretical framework. Int. J. Emot. Educ. 2020, 12, 65–82. [Google Scholar]
- Kristjánsson, K. Positive psychology and positive education: Old wine in new bottles? Educ. Psychol. 2012, 47, 86–105. [Google Scholar] [CrossRef]
- Conte, E.; Grazzani, I.; Pepe, A. Social cognition, language, and prosocial behaviors: A multitrait mixed-methods study in early childhood. Early Educ. Dev. 2018, 29, 814–830. [Google Scholar] [CrossRef]
- Farina, E.; Belacchi, C. Being visible or being liked? Social status and emotional skills in bullying among young children. Eur. J. Dev. Psychol. 2022, 19, 267–282. [Google Scholar] [CrossRef]
- Imuta, K.; Henry, J.D.; Slaughter, V.; Selcuk, B.; Ruffman, T. Theory of mind and prosocial behavior in childhood: A meta-analytic review. Dev. Psychol. 2016, 52, 1192–1205. [Google Scholar] [CrossRef] [PubMed]
- Sette, S.; Spinrad, T.L.; Baumgartner, E. The relations of preschool children’s emotion knowledge and socially appropriate behaviors to peer likability. Int. J. Behav. Dev. 2017, 41, 532–541. [Google Scholar] [CrossRef]
- Laible, D.; Carlo, G.; Murphy, T.; Augustine, M.; Roesch, S. Predicting children’s prosocial and co-operative behavior from their temperamental profiles: A person-centered approach. Soc. Dev. 2014, 23, 734–752. [Google Scholar] [CrossRef]
- Williams, K.E.; Berthelsen, D. The development of prosocial behaviour in early childhood: Contributions of early parenting and self- regulation. Int. J. Early Child. 2017, 49, 73–94. [Google Scholar] [CrossRef]
- Clark, R.; Menna, R.; McAndrew, A.J.; Johnson, E.M. Language, aggression, and self-regulation in young children. J. Emot. Behav. Disord. 2021, 29, 135–147. [Google Scholar] [CrossRef]
- Trentacosta, C.J.; Fine, S.E. Emotion knowledge, social competence, and behavior problems in childhood and adolescence: A meta-analytic review. Soc. Dev. 2010, 19, 1–29. [Google Scholar] [CrossRef]
- Willoughby, M.; Kupersmidt, J.; Voegler-Lee, M.; Bryant, D. Contributions of hot and cool self-regulation to preschool disruptive behavior and academic achievement. Dev. Neuropsychol. 2011, 36, 162–180. [Google Scholar] [CrossRef]
- Maguire, L.K.; Niens, U.; McCann, M.; Connolly, P. Emotional development among early school-age children: Gender differences in the role of problem behaviours. Educ. Psychol. 2016, 36, 1408–1428. [Google Scholar] [CrossRef]
- Martinsone, B.; Supe, I.; Stokenberga, I.; Damberga, I.; Cefai, C.; Camilleri, L.; Bartolo, P.; O’Riordan, M.R.; Grazzani, I. Social emotional competence, learning outcomes, emotional and behavioral difficulties of preschool children: Parent and teacher evaluations. Front. Psychol. 2022, 12, 760782. [Google Scholar] [CrossRef]
- Ostrov, J.M.; Massetti, G.M.; Stauffacher, K.; Godleski, S.A.; Hart, K.C.; Karch, K.M.; Mullins, A.D.; Ries, E.E. An intervention for relational and physical aggression in early childhood: A preliminary study. Early Child. Res. Q. 2009, 24, 15–28. [Google Scholar] [CrossRef]
- Luo, L.; Reichow, B.; Snyder, P.; Harrington, J.; Polignano, J. Systematic review and meta-analysis of classroom-wide social–emotional interventions for preschool children. Topics Early Child. Spec. Educ. 2022, 42, 4–19. [Google Scholar] [CrossRef]
- Murano, D.; Sawyer, J.E.; Lipnevich, A.A. A meta-analytic review of preschool social and emotional learning interventions. Rev. Educ. Res. 2020, 90, 227–263. [Google Scholar] [CrossRef]
- Ștefan, C.A.; Dănilă, I.; Cristescu, D. Classroom-wide school interventions for preschoolers’ social-emotional learning: A systematic review of evidence-based programs. Educ. Psychol. Rev. 2022, 34, 2971–3010. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef]
- Agnafors, S.; Barmark, M.; Sydsjö, G. Mental health and academic performance: A study on selection and causation effects from childhood to early adulthood. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 857–866. [Google Scholar] [CrossRef]
- Birch, S.H.; Ladd, G.W. The teacher-child relationship and children’s early school adjustment. J. Sch. Psychol. 1997, 35, 61–79. [Google Scholar] [CrossRef]
- Bosman, R.J.; Roorda, D.L.; van der Veen, I.; Koomen, H.M.Y. Teacher-student relationship quality from kindergarten to sixth grade and students’ school adjustment: A person-centered approach. J. Sch. Psychol. 2018, 68, 177–194. [Google Scholar] [CrossRef]
- Denham, S.A.; Bassett, H.H.; Sirotkin, Y.S.; Brown, C.; Morris, C.S. “No-o-o-o peeking”: Preschoolers’ executive control, social competence, and classroom adjustment. J. Res. Child. Educ. 2015, 29, 212–225. [Google Scholar] [CrossRef]
- Ladd, G.W.; Kothenderfer, B.J.; Coleman, C.C. Friendship quality as a predictor of young children’s early school adjustment. Child Dev. 1996, 67, 1103–1118. [Google Scholar] [CrossRef]
- Curby, T.W.; Brown, C.A.; Bassett, H.H.; Denham, S.A. Associations between preschoolers’ social–emotional competence and preliteracy skills. Infant Child Dev. 2015, 24, 549–570. [Google Scholar] [CrossRef]
- Denham, S.A.; Bassett, H.H.; Zinsser, K.; Wyatt, T.M. How preschoolers’ social–emotional learning predicts their early school success: Developing theory-promoting, competency-based assessments. Infant Child Dev. 2014, 23, 426–454. [Google Scholar] [CrossRef]
- Guhn, M.; Gadermann, A.M.; Almas, A.; Schonert-Reichl, K.A.; Hertzman, C. Associations of teacher-rated social, emotional, and cognitive development in kindergarten to self-reported wellbeing, peer relations, and academic test scores in middle childhood. Early Child. Res. Q. 2016, 35, 76–84. [Google Scholar] [CrossRef]
- Denham, S.A.; Bassett, H.H.; Mincic, M.; Kalb, S.; Way, E.; Wyatt, T.; Segal, Y. Social-emotional learning profiles of preschoolers’ early school success: A person-centered approach. Learn. Individ. Differ. 2012, 22, 178–189. [Google Scholar] [CrossRef]
- Raver, C.C.; Knitzer, J. Ready to Enter: What Research Tells Policy Makers about Strategies to Promote Social and Emotional School Readiness among Three and Four-Year-Olds; National Center for Children in Poverty, Columbia University: New York, NY, USA, 2002. [Google Scholar]
- Korucu, I.; Ayturk, E.; Finders, J.K.; Schnur, G.; Bailey, C.S.; Tominey, S.L.; Schmitt, S.A. Self-regulation in preschool: Examining its factor structure and associations with pre-academic skills and social-emotional competence. Front. Psychol. 2022, 12, 717317. [Google Scholar] [CrossRef]
- Esch, P.; Bocquet, V.; Pull, C.; Couffignal, S.; Lehnert, T.; Graas, M.; Fond-Harmant, L.; Ansseau, M. The downward spiral of mental disorders and educational attainment: A systematic review on early school leaving. BMC Psychiatry 2014, 14, 237. [Google Scholar] [CrossRef]
- Hair, E.; Halle, T.; Terry-Humen, E.; Lavelle, B.; Calkins, J. Children’s school readiness in the ECLS-K: Predictions to academic, health, and social outcomes in first grade. Early Child. Res. Q. 2006, 21, 431–454. [Google Scholar] [CrossRef]
- Malecki, C.K.; Elliot, S.N. Children’s social behaviors as predictors of academic achievement: A longitudinal analysis. Sch. Psychol. Q. 2002, 17, 1–23. [Google Scholar] [CrossRef]
- Corcoran, R.P.; Cheung, A.C.; Kim, E.; Xie, C. Effective universal school-based social and emotional learning programs for improving academic achievement: A systematic review and meta-analysis of 50 years of research. Educ. Res. Rev. 2018, 25, 56–72. [Google Scholar] [CrossRef]
- Simões, C.; Santos, A.C.; Lebre, P.; Daniel, J.R.; Branquinho, C.; Gaspar, T.; de Matos, M.G. Assessing the impact of the European resilience curriculum in preschool, early and late primary school children. Sch. Psychol. Int. 2021, 42, 539–566. [Google Scholar] [CrossRef]
- Browne, G.; Gafni, A.; Roberts, J.; Byrne, C.; Majumdar, B. Effective/efficient mental health programs for school-age children: A synthesis of reviews. Soc. Sci. Med. 2004, 58, 1367–1384. [Google Scholar] [CrossRef] [PubMed]
- The Conduct Problems Prevention Research Group. The implementation of the Fast Track Program: An example of a large-scale prevention science efficacy trial. J. Abnorm. Child Psychol. 2002, 30, 1–17. [Google Scholar] [CrossRef]
- Weare, K.; Nind, M. Mental health promotion and problem prevention in schools: What does the evidence say? Health Promot. Int. 2011, 26, i29–i69. [Google Scholar] [CrossRef] [PubMed]
- Cavioni, V.; Zanetti, M.A. Social-emotional learning and students’ transition from kindergarten to primary school in Italy. In Transforming the Future of Learning with Educational Research; Askell-Williams, H., Ed.; IGI Global: Hershey, PA, USA, 2015; pp. 241–258. [Google Scholar]
- Ungar, M. Multisystemic Resilience: Adaptation and Transformation in Contexts of Change; Oxford University Press: New York, NY, USA, 2021. [Google Scholar]
- Blewitt, C.; Fuller-Tyszkiewicz, M.; Nolan, A.; Bergmeier, H.; Vicary, D.; Huang, T.; McCabe, P.; McKay, T.; Skouteris, H. Social and emotional learning associated with universal curriculum-based interventions in early childhood education and care centers: A systematic review and meta-analysis. JAMA Netw. Open 2018, 1, e185727. [Google Scholar] [CrossRef]
- Losel, F.; Stemmler, M.; Bender, D. Long-term evaluation of a bimodal universal prevention program: Effects on antisocial development from kindergarten to adolescence. J. Exp. Criminol. 2013, 9, 429–449. [Google Scholar] [CrossRef]
- Ștefan, C.A.; Dănilă, I.; Cristescu, D. Assessing the effectiveness and the mechanisms of the Social-Emotional Prevention Program for Preschoolers: Findings from a universal school-based intervention. J. Sch. Psychol. 2023, 98, 206–223. [Google Scholar] [CrossRef] [PubMed]
- Ștefan, C.A.; Miclea, M. Effects of a multifocused prevention program on preschool children’s competencies and behavior problems. Psychol. Sch. 2013, 50, 382–402. [Google Scholar] [CrossRef]
- Lester, L.; Cefai, C.; Cavioni, V.; Barnes, A.; Cross, D. A whole-school approach to promoting staff wellbeing. Aust. J. Teach. Educ. 2020, 45, 1–22. [Google Scholar] [CrossRef]
- Cefai, C.; Arlove, A.; Duca, M.; Galea, N.; Muscat, M.; Cavioni, V. RESCUR Surfing the Waves: An evaluation of a resilience programme in the early years. Pastor. Care Educ. 2018, 36, 189–204. [Google Scholar] [CrossRef]
- Cavioni, C.; Grazzani, I.; Ornaghi, V.; Agliati, A.; Gandellini, S.; Cefai, C.; Camilleri, L.; Bartolo, P.; Tatalovic Vorkapic, S.; Golob, L.; et al. A multi-component curriculum to promote teachers’ mental health: Findings from the PROMEHS program. Int. J. Emot. Educ. 2023, 15, 34–52. [Google Scholar] [CrossRef]
- Cefai, C.; Camilleri, L.; Bartolo, P.; Grazzani, I.; Cavioni, V.; Conte, E.; Ornaghi, V.; Agliati, A.; Gandellini, S.; Tatalovic Vorkapic, S.; et al. The effectiveness of a school-based, universal mental health programme in six European countries. Front. Psychol. 2022, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Poulou, M.S.; Grazzani, I.; Cavioni, V.; Ornaghi, V.; Conte, E.; Cefai, C.; Camilleri, L.; Bartolo, P. Changes in students’ social and emotional competences following the implementation of a school-based intervention program. Am. J. Appl. Psychol. 2022, 11, 122–132. [Google Scholar]
- dos Santos, M.F.; Simões, C.; Santos, A.C.; Lebre, P.; Grazzani, I. Does online implementation make a difference in the effects of a mental health curriculum at schools? Int. J. Environ. Res. Public Health 2022, 19, 16990. [Google Scholar] [CrossRef]
- Colomeischi, A.A.; Duca, D.S.; Bujor, L.; Rusu, P.P.; Grazzani, I.; Cavioni, V. Impact of a school mental health program on children’s and adolescents’ socio-emotional skills and psychosocial difficulties. Children 2022, 9, 1661. [Google Scholar] [CrossRef] [PubMed]
- CASEL—Evidence-Based Social and Emotional Learning Programs: CASEL Criteria Updates and Rationale. Available online: https://casel.org/wp-content/uploads/2021/01/11_CASEL-Program-Criteria-Rationale.pdf (accessed on 14 April 2023).
- Brackett, M.A.; Bailey, C.S.; Hoffmann, J.D.; Simmons, D.N. RULER: A theory-driven, systemic approach to social, emotional, and academic learning. Educ. Psychol. 2019, 54, 144–161. [Google Scholar] [CrossRef]
- Smith, T.E.; Sheridan, S.M.; Kim, E.M.; Park, S.; Beretvas, S.N. The effects of family-school partnership interventions on academic and social-emotional functioning: A meta-analysis exploring what works for whom. Educ. Psychol. Rev. 2020, 32, 511–544. [Google Scholar] [CrossRef]
- Djamnezhad, D.; Koltcheva, N.; Dizdarevic, A.; Mujezinovic, A.; Peixoto, C.; Coelho, V.; Achten, M.; Kolumbán, E.; Machado, F.; Hofvander, B. Social and emotional learning in preschool settings: A systematic map of systematic reviews. Front. Educ. 2021, 6, 691670. [Google Scholar] [CrossRef]
- Martinsone, B.; Stokenberga, I.; Grazzani, I. Monitoring system of implementation of the Promoting Mental Health at Schools (PROMEHS) program. Front. Psychol. 2022, 13, 1043001. [Google Scholar] [CrossRef]
- Grazzani, I.; Agliati, A.; Conte, E.; Cavioni, V.; Gandellini, S.; Ornaghi, V.; Rossi, F.M.; Tatalović Vorkapić, S.; Tambolaš, A.C.; Lisjak, K.; et al. PROMEHS. The Curriculum to Promote Mental Health at School. Activities Handbook for Teachers, Kindergarten and Primary School (Ages 3–10); Mimesis Edizioni: Milan, Italy, 2022. [Google Scholar]
- Grazzani, I.; Agliati, A.; Conte, E.; Cavioni, V.; Gandellini, S.; Ornaghi, V.; Rossi, F.M.; Tatalović Vorkapić, S.; Tambolaš, A.C.; Lisjak, K.; et al. PROMEHS. The Curriculum to Promote Mental Health at School. Activities Handbook for Students, Kindergarten and Primary School (Ages 3–10); Mimesis Edizioni: Milan, Italy, 2022. [Google Scholar]
- Elliott, S.N.; DiPerna, J.C.; Anthony, C.J.; Lei, P.; Gresham, F.M. Social Skills Improvement System, Social Emotional Learning (SSIS-SEL) Brief Scales; SAIL CoLab: Scottsdale, AZ, USA, 2020. [Google Scholar]
- Anthony, C.J.; Elliott, S.N.; DiPerna, J.C.; Lei, P. The SSIS SEL brief scales-student form: Initial development and validation. Sch. Psychol. 2020, 35, 277–283. [Google Scholar] [CrossRef]
- Anthony, C.J.; Elliott, S.N.; Yost, M.; Lei, P.-W.; DiPerna, J.C.; Cefai, C.; Camilleri, L.; Bartolo, P.A.; Grazzani, I.; Ornaghi, V.; et al. Multi-informant validity evidence for the SSIS SEL Brief Scales across six European countries. Front. Psychol. 2022, 13, 928189. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.; Lamping, D.L.; Ploubidis, G.B. When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers and children. J. Abnorm. Child Psychol. 2010, 38, 1179–1191. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2014. [Google Scholar]
- Jennings, P.A.; Greenberg, M.T. The prosocial classroom: Teacher social and emotional competence in relation to student and classroom outcomes. Rev. Educ. Res. 2009, 79, 491–525. [Google Scholar] [CrossRef]
- Cowie, H.; Myers, C.-A. The impact of the COVID-19 pandemic on the mental health and well-being of children and young people. Child. Soc. 2021, 35, 62–74. [Google Scholar] [CrossRef]
- Cusinato, M.; Iannattone, S.; Spoto, A.; Poli, M.; Moretti, C.; Gatta, M.; Miscioscia, M. Stress, resilience, and well-being in Italian children and their parents during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8297. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Belfield, C.; Bowden, A.; Klapp, A.; Levin, H.; Shand, R.; Zander, S. The economic value of social and emotional learning. J. Benefit-Cost Anal. 2015, 6, 508–544. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Test | Post-Test | |||
|---|---|---|---|---|
| Experimental | Waiting List | Experimental | Waiting List | |
| Self-awareness | 11.59 (2.33) | 11.06 (2.23) | 12.62 (2.14) | 11.40 (2.08) |
| Self-management | 11.96 (2.52) | 12.25 (2.43) | 12.44 (2.39) | 12.30 (2.33) |
| Social awareness | 12.42 (2.33) | 11.86 (2.31) | 13.14 (2.25) | 12.13 (2.43) |
| Relationship skills | 12.98 (2.13) | 12.81 (2.13) | 13.46 (2.05) | 13.18 (2.05) |
| Responsible decision-making | 12.85 (2.39) | 12.89 (2.72) | 13.38 (2.21) | 12.98 (2.28) |
| SEL total | 61.78 (10.22) | 60.87 (9.54) | 65.02 (9.67) | 61.99 (9.46) |
| Prosocial behavior | 10.38 (3.13) | 10.49 (3.01) | 11.06 (3.06) | 10.81 (2.99) |
| Internalizing problems | 7.87 (5.09) | 8.97 (5.71) | 7.48 (5.21) | 9.05 (5.23) |
| Externalizing problems | 9.61 (5.23) | 9.83 (5.39) | 9.31 (5.15) | 9.91 (5.26) |
| Academic motivation | 3.90 (0.90) | 3.89 (0.88) | 4.07 (0.89) | 4.04 (0.81) |
| Engagement in learning | 3.87 (0.92) | 3.91 (0.88) | 4.07 (0.94) | 3.94 (0.86) |
| Academic performance | 3.82 (0.93) | 3.83 (0.88) | 4.06 (0.90) | 3.88 (0.87) |
| Academic outcomes total | 11.60 (2.64) | 11.63 (2.51) | 12.20 (2.63) | 11.87 (2.38) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Self-awareness | - | ||||||||||||
| 2. Self-management | 0.53 ** | - | |||||||||||
| 3. Social awareness | 0.70 ** | 0.54 ** | - | ||||||||||
| 4. Relationship skills | 0.67 ** | 0.58 ** | 0.77 ** | - | |||||||||
| 5. Responsible decision-making | 0.70 ** | 0.73 ** | 0.72 ** | 0.79 ** | - | ||||||||
| 6. SEL total | 0.84 ** | 0.79 ** | 0.86 ** | 0.88 ** | 0.92 ** | - | |||||||
| 7. Prosocial behavior | 0.31 ** | 0.42 ** | 0.35 ** | 0.34 ** | 0.45 ** | 0.44 ** | - | ||||||
| 8. Internalizing problems | −0.28 ** | 0.01 | −0.32 ** | −0.35 ** | −0.15 ** | −0.25 ** | 0.51 ** | - | |||||
| 9. Externalizing problems | −0.39 ** | −0.45 ** | −0.45 ** | −0.45 ** | −0.44 ** | −0.51 ** | 0.32 ** | 0.72 ** | - | ||||
| 10. Academic motivation | 0.46 ** | 0.48 ** | 0.44 ** | 0.48 ** | 0.54 ** | 0.56 ** | 0.37 ** | −0.12 * | −0.32 ** | - | |||
| 11. Engagement in learning | 0.46 ** | 0.52 ** | 0.42 ** | 0.47 ** | 0.56 ** | 0.57 ** | 0.38 ** | −0.08 * | −0.30 ** | 0.88 ** | - | ||
| 12. Academic performance | 0.45 ** | 0.50 ** | 0.38 ** | 0.46 ** | 0.55 ** | 0.55 ** | 0.38 ** | −0.06 | −0.28 ** | 0.84 ** | 0.88 ** | - | |
| 13. Academic outcomes total | 0.48 ** | 0.52 ** | 0.43 ** | 0.49 ** | 0.57 ** | 0.58 ** | 0.39 ** | −0.09 * | −0.31 ** | 0.95 ** | 0.96 ** | 0.95 ** | - |
| 14. Gender | −0.14 ** | −0.21 ** | −0.16 ** | −0.11 * | −0.15 ** | −0.18 ** | −0.11 * | 0.02 | 0.18 ** | −0.22 ** | −0.23 ** | −0.19 ** | −0.23 ** |
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| 1. Number of activities | - | ||||
| 2. SEL changes | 0.26 ** | - | |||
| 3. Prosocial changes | 0.02 | 0.59 ** | - | ||
| 4. Internalizing changes | −0.20 ** | −0.37 ** | −0.25 ** | - | |
| 5. Externalizing changes | −0.11 * | −0.53 ** | −0.39 ** | −0.24 ** | - |
| 6. Academic outcomes changes | 0.07 | 0.49 ** | 0.35 ** | −0.20 ** | −0.37 ** |
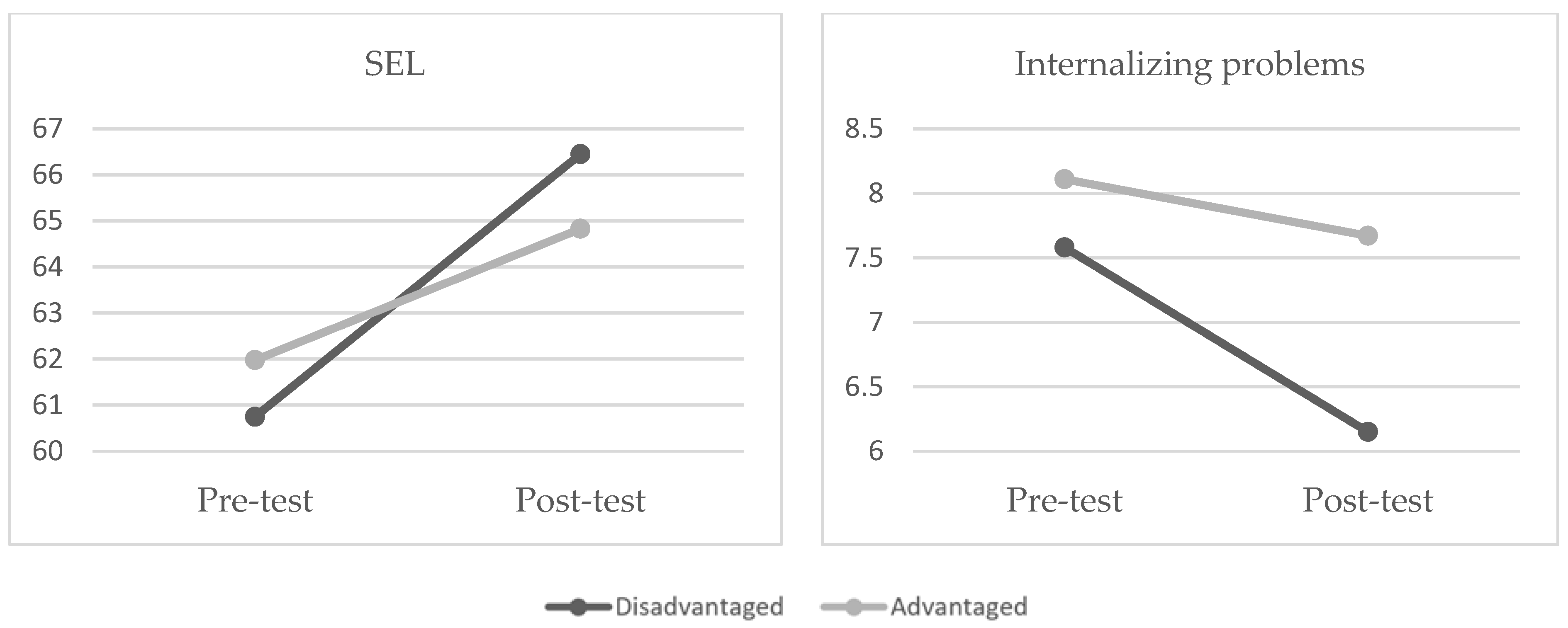
| Pre-Test | Post-Test | |||
|---|---|---|---|---|
| Advantaged | Disadvantaged | Advantaged | Disadvantaged | |
| SEL total | 61.91 (9.45) | 60.75 (13.44) | 64.76 (9.39) | 66.45 (10.98) |
| Prosocial behavior | 10.77 (3.03) | 9.45 (3.52) | 11.25 (3.03) | 10.44 (3.15) |
| Internalizing problems | 8.29 (5.08) | 7.91 (4.71) | 7.86 (5.17) | 6.35 (4.87) |
| Externalizing problems | 9.96 (5.11) | 9.05 (5.76) | 9.55 (5.42) | 8.27 (5.85) |
| Academic outcomes total | 11.84 (2.57) | 10.56 (2.75) | 12.36 (2.52) | 11.44 (2.83) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conte, E.; Cavioni, V.; Ornaghi, V.; Agliati, A.; Gandellini, S.; Santos, M.F.; Santos, A.C.; Simões, C.; Grazzani, I. Supporting Preschoolers’ Mental Health and Academic Learning through the PROMEHS Program: A Training Study. Children 2023, 10, 1070. https://doi.org/10.3390/children10061070
Conte E, Cavioni V, Ornaghi V, Agliati A, Gandellini S, Santos MF, Santos AC, Simões C, Grazzani I. Supporting Preschoolers’ Mental Health and Academic Learning through the PROMEHS Program: A Training Study. Children. 2023; 10(6):1070. https://doi.org/10.3390/children10061070
Chicago/Turabian StyleConte, Elisabetta, Valeria Cavioni, Veronica Ornaghi, Alessia Agliati, Sabina Gandellini, Margarida Frade Santos, Anabela Caetano Santos, Celeste Simões, and Ilaria Grazzani. 2023. "Supporting Preschoolers’ Mental Health and Academic Learning through the PROMEHS Program: A Training Study" Children 10, no. 6: 1070. https://doi.org/10.3390/children10061070
APA StyleConte, E., Cavioni, V., Ornaghi, V., Agliati, A., Gandellini, S., Santos, M. F., Santos, A. C., Simões, C., & Grazzani, I. (2023). Supporting Preschoolers’ Mental Health and Academic Learning through the PROMEHS Program: A Training Study. Children, 10(6), 1070. https://doi.org/10.3390/children10061070