

Clinical Patterns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study


 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
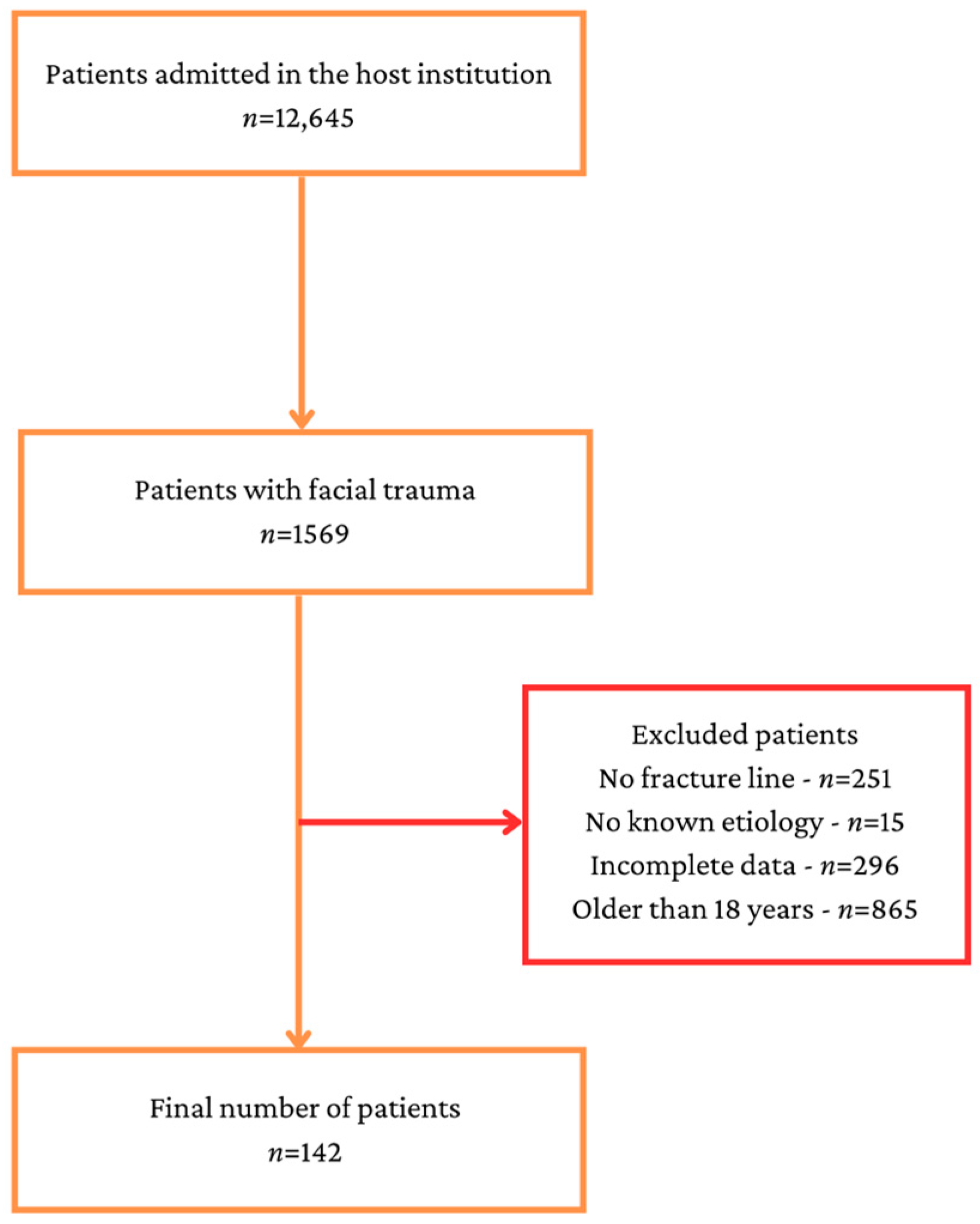
2.2. Participants and Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gómez Roselló, E.; Quiles Granado, A.M.; Artajona Garcia, M.; Juanpere Martí, S.; Laguillo Sala, G.; Beltrán Mármol, B.; Pedraza Gutiérrez, S. Facial fractures: Classification and highlights for a useful report. Insights Imaging 2020, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Lalloo, R.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; Roberts, N.L.S.; Sylte, D.O.; et al. Epidemiology of facial fractures: Incidence, prevalence and years lived with disability estimates from the Global Burden of Disease 2017 study. Inj. Prev. 2020, 26 (Suppl. S1), i27–i35. [Google Scholar] [CrossRef]
- Juncar, M.; Tent, P.A.; Juncar, R.I.; Harangus, A.; Mircea, R. An epidemiological analysis of maxillofacial fractures: A 10-year cross-sectional cohort retrospective study of 1007 patients. BMC Oral Health 2021, 21, 128. [Google Scholar] [CrossRef] [PubMed]
- Cole, P.; Kaufman, Y.; Hollier, L.H., Jr. Managing the pediatric facial fracture. Craniomaxillofac. Trauma Reconstr. 2009, 2, 77–83. [Google Scholar] [CrossRef]
- Braun, T.L.; Xue, A.S.; Maricevich, R.S. Differences in the Management of Pediatric Facial Trauma. Semin. Plast. Surg. 2017, 31, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Imahara, S.D.; Hopper, R.A.; Wang, J.; Rivara, F.P.; Klein, M.B. Patterns and outcomes of pediatric facial fractures in the United States: A survey of the National Trauma Data Bank. J. Am. Coll. Surg. 2008, 207, 710–716. [Google Scholar] [CrossRef]
- Vyas, R.M.; Dickinson, B.P.; Wasson, K.L.; Roostaeian, J.; Bradley, J.P. Pediatric facial fractures: Current national incidence, distribution, and health care resource use. J. Craniofac. Surg. 2008, 19, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Dobitsch, A.A.; Oleck, N.C.; Liu, F.C.; Halsey, J.N.; Hoppe, I.C.; Lee, E.S.; Granick, M.S. Sports-Related Pediatric Facial Trauma: Analysis of Facial Fracture Pattern and Concomitant Injuries. Surg. J. 2019, 5, e146–e149. [Google Scholar] [CrossRef]
- Montovani, J.C.; de Campos, L.M.; Gomes, M.A.; de Moraes, V.R.; Ferreira, F.D.; Nogueira, E.A. Etiology and incidence facial fractures in children and adults. Braz. J. Otorhinolaryngol. 2006, 72, 235–241. [Google Scholar] [CrossRef]
- Gassner, R.; Tuli, T.; Hächl, O.; Moreira, R.; Ulmer, H. Craniomaxillofacial trauma in children: A review of 3385 cases with 6060 injuries in 10 years. J. Oral Maxillofac. Surg. 2004, 62, 399–407. [Google Scholar] [CrossRef]
- Andrew, T.W.; Morbia, R.; Lorenz, H.P. Pediatric Facial Trauma. Clin. Plast. Surg. 2019, 46, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Grunwaldt, L.; Smith, D.M.; Zuckerbraun, N.S.; Naran, S.; Rottgers, S.A.; Bykowski, M.; Kinsella, C.; Cray, J.; Vecchione, L.; Saladino, R.A.; et al. Pediatric facial fractures: Demographics, injury patterns, and associated injuries in 772 consecutive patients. Plast. Reconstr. Surg. 2011, 128, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Totonchi, A.; Sweeney, W.M.; Gosain, A.K. Distinguishing anatomic features of pediatric facial trauma. J. Craniofac. Surg. 2012, 23, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Adibelli, Z.H.; Songu, M.; Adibelli, H. Paranasal sinus development in children: A magnetic resonance imaging analysis. Am. J. Rhinol. Allergy. 2011, 25, 30–35. [Google Scholar] [CrossRef]
- Shah, R.K.; Dhingra, J.K.; Carter, B.L.; Rebeiz, E.E. Paranasal sinus development: A radiographic study. Laryngoscope 2003, 113, 205–209. [Google Scholar] [CrossRef]
- Alcalá-Galiano, A.; Arribas-García, I.J.; Martín-Pérez, M.A.; Romance, A.; Montalvo-Moreno, J.J.; Juncos, J.M. Pediatric facial fractures: Children are not just small adults. Radiographics 2008, 28, 441–461. [Google Scholar] [CrossRef]
- Ryu, J.; Yun, S.J.; Lee, S.H.; Choi, Y.H. Screening of pediatric facial fractures by brain computed tomography: Diagnostic performance comparison with facial computed tomography. Pediatr. Emerg. Care 2020, 36, 1259. [Google Scholar] [CrossRef]
- Goldwasser, T.; Bressan, S.; Oakley, E.; Arpone, M.; Babl, F.E. Use of sedation in children receiving computed tomography after head injuries. Eur. J. Emerg. Med. 2015, 22, 413–418. [Google Scholar] [CrossRef]
- Nguyen, B.N.; Edwards, M.J.; Srivatsa, S.; Wakeman, D.; Claderon, T.; Lamoshi, A.; Wallenstein, K.; Fabiano, T.; Cantor, B.; Bass, K.; et al. Clinical and radiographic predictors of the need for facial CT in pediatric blunt trauma: A multi-institutional study. Trauma Surg. Acute Care Open 2022, 7, e000899. [Google Scholar] [CrossRef]
- Siy, R.W.; Brown, R.H.; Koshy, J.C.; Stal, S.; Hollier, L.H., Jr. General management considerations in pediatric facial fractures. J. Craniofac. Surg. 2011, 22, 1190–1195. [Google Scholar] [CrossRef]
- Ferreira, P.; Marques, M.; Pinho, C.; Rodrigues, J.; Reis, J.; Amarante, J. Midfacial fractures in children and adolescents: A review of 492 cases. Br. J. Oral Maxillofac. Surg. 2004, 42, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C.E.; Troulis, M.J.; Kaban, L.B. Pediatric facial fractures: Recent advances in prevention, diagnosis and management. Int. J. Oral Maxillofac. Surg. 2006, 35, 2–13. [Google Scholar] [CrossRef]
- Segura-Palleres, I.; Sobrero, F.; Roccia, F.; de Oliveira Gorla, L.F.; Pereira-Filho, V.A.; Gallafassi, D.; Faverani, L.P.; Romeo, I.; Bojino, A.; Copelli, C. Characteristics and age-related injury patterns of maxillofacial fractures in children and adolescents: A multicentric and prospective study. Dent. Traumatol. 2022, 38, 213–222. [Google Scholar] [CrossRef]
- Chao, M.T.; Losee, J.E. Complications in pediatric facial fractures. Craniomaxillofac. Trauma Reconstr. 2009, 2, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Burgueño Torres, L.; Mourelle Martínez, M.R.; de Nova García, J.M. A study on the chronology and sequence of eruption of primary teeth in Spanish children. Eur. J. Paediatr. Dent. 2015, 16, 301–304. [Google Scholar] [PubMed]
- Lynch, R.J. The primary and mixed dentition, post-eruptive enamel maturation and dental caries: A review. Int. Dent. J. 2013, 63 (Suppl. S2), 3–13. [Google Scholar] [CrossRef]
- Ferreira, P.C.; Barbosa, J.; Braga, J.M.; Rodrigues, A.; Silva, Á.C.; Amarante, J.M. Pediatric Facial Fractures: A Review of 2071 Fractures. Ann. Plast. Surg. 2016, 77, 54–60. [Google Scholar] [CrossRef]
- Hoppe, I.C.; Kordahi, A.M.; Paik, A.M.; Lee, E.S.; Granick, M.S. Age and sex-related differences in 431 pediatric facial fractures at a level 1 trauma center. J. Craniomaxillofac. Surg. 2014, 42, 1408–1411. [Google Scholar] [CrossRef]
- Marek, A.P.; Nygaard, R.M.; Cohen, E.M.; Polites, S.F.; Sirany, A.E.; Wildenberg, S.E.; Elsbernd, T.A.; Murphy, S.; Dean Potter, D.; Zielinski, M.D.; et al. Rural versus urban pediatric non-accidental trauma: Different patients, similar outcomes. BMC Res. Notes 2018, 11, 519. [Google Scholar] [CrossRef]
- Hedström, E.M.; Waernbaum, I. Incidence of fractures among children and adolescents in rural and urban communities—Analysis based on 9965 fracture events. Inj. Epidemiol. 2014, 1, 14. [Google Scholar] [CrossRef]
- Pittman, S.K.; Farrell, A.D. Patterns of community violence exposure among urban adolescents and their associations with adjustment. Am. J. Community Psychol. 2022, 70, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Iida, S.; Matsuya, T. Paediatric maxillofacial fractures: Their aetiological characters and fracture patterns. J. Craniomaxillofac. Surg. 2002, 30, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S. A retrospective study of mandibular fractures in children. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 269–274. [Google Scholar] [CrossRef]
- Panesar, K.; Susarla, S.M. Mandibular Fractures: Diagnosis and Management. Semin. Plast. Surg. 2021, 35, 238–249. [Google Scholar] [CrossRef]
- Gadicherla, S.; Sasikumar, P.; Gill, S.S.; Bhagania, M.; Kamath, A.T.; Pentapati, K.C. Mandibular Fractures and Associated Factors at a Tertiary Care Hospital. Arch. Trauma Res. 2016, 5, e30574. [Google Scholar] [CrossRef] [PubMed]
- Pickrell, B.B.; Serebrakian, A.T.; Maricevich, R.S. Mandible Fractures. Semin. Plast. Surg. 2017, 31, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Niazi, K.T.; Raja, D.K.; Prakash, R.; Balaji, V.R.; Manikandan, D.; Ulaganathan, G.; Yoganandha, R. Massive expanding hematoma of the chin following blunt trauma. J. Pharm. Bioallied Sci. 2016, 8 (Suppl. S1), S182–S184. [Google Scholar] [CrossRef]
- Chapman, V.M.; Fenton, L.Z.; Gao, D.; Strain, J.D. Facial fractures in children: Unique patterns of injury observed by computed tomography. J. Comput. Assist. Tomogr. 2009, 33, 70–72. [Google Scholar] [CrossRef]
- Ferreira, P.C.; Barbosa, J.; Amarante, J.M.; Carvalho, J.; Rodrigues, A.G.; Silva, Á.C. Associated injuries in pediatric patients with facial fractures in Portugal: Analysis of 1416 patients. J. Craniomaxillofac. Surg. 2015, 43, 437–443. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, S.H.; Cho, P.D. Analysis of 809 facial bone fractures in a pediatric and adolescent population. Arch. Plast. Surg. 2012, 39, 606–611. [Google Scholar] [CrossRef]
- Mckenzie, J.; Nguyen, E. Minimally Invasive Surgical Management of Complex Pediatric Facial Fractures. Craniomaxillofac. Trauma Reconstr. Open 2021, 6, 24727512211022601. [Google Scholar] [CrossRef]
- Singh, G.; Mohammad, S.; Chak, R.K.; Lepcha, N.; Singh, N.; Malkunje, L.R. Bio-resorbable plates as effective implant in paediatric mandibular fracture. J. Maxillofac. Oral Surg. 2012, 11, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Naik, P. Remodelling in Children’s Fractures and Limits of Acceptability. Indian J. Orthop. 2021, 55, 549–559. [Google Scholar] [CrossRef]
- Țenț, P.A.; Juncar, R.I.; Moca, A.E.; Moca, R.T.; Juncar, M. The Etiology and Epidemiology of Pediatric Facial Fractures in North-Western Romania: A 10-Year Retrospective Study. Children 2022, 9, 932. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
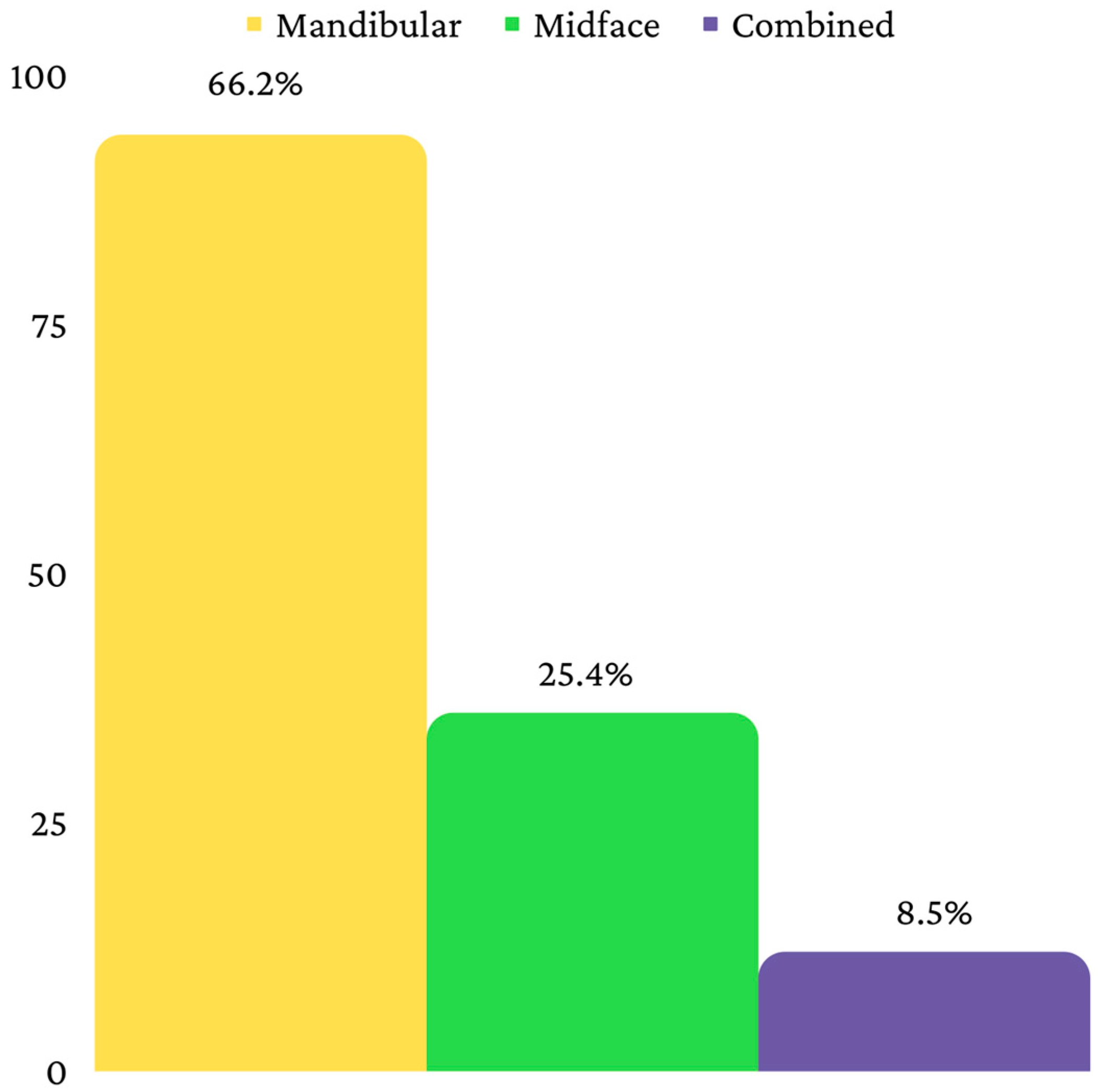
| Fracture (n, %) | Mandibular | Midface | Combined | |
|---|---|---|---|---|
| Age | p * | |||
| Mean ± SD | 15.32 ± 3.63 | 14.02 ± 4.01 | 14.58 ± 3.75 | 0.139 |
| Median (IQR) | 17 (14–18) | 16 (10.25–17) | 16 (10.25)–18 | |
| Age Group | p ** | |||
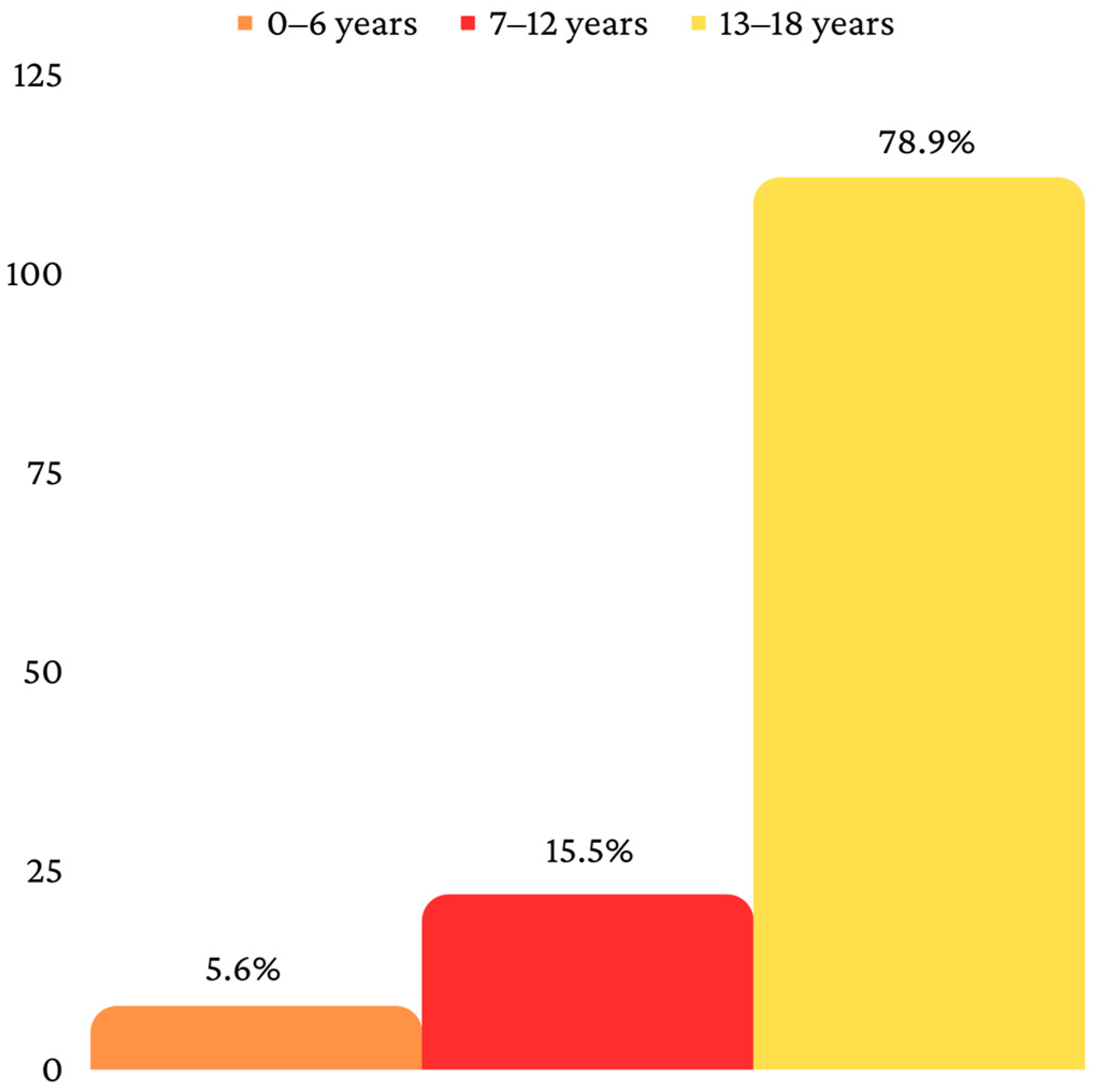
| 0–6 years | 6 (6.4%) | 2 (5.6%) | 0 (0%) | 0.067 |
| 7–12 years | 9 (9.6%) | 9 (25%) | 4 (33.3%) | |
| 13–18 years | 79 (84%) | 25 (69.4%) | 8 (66.7%) | |
| Living environment | p ** | |||
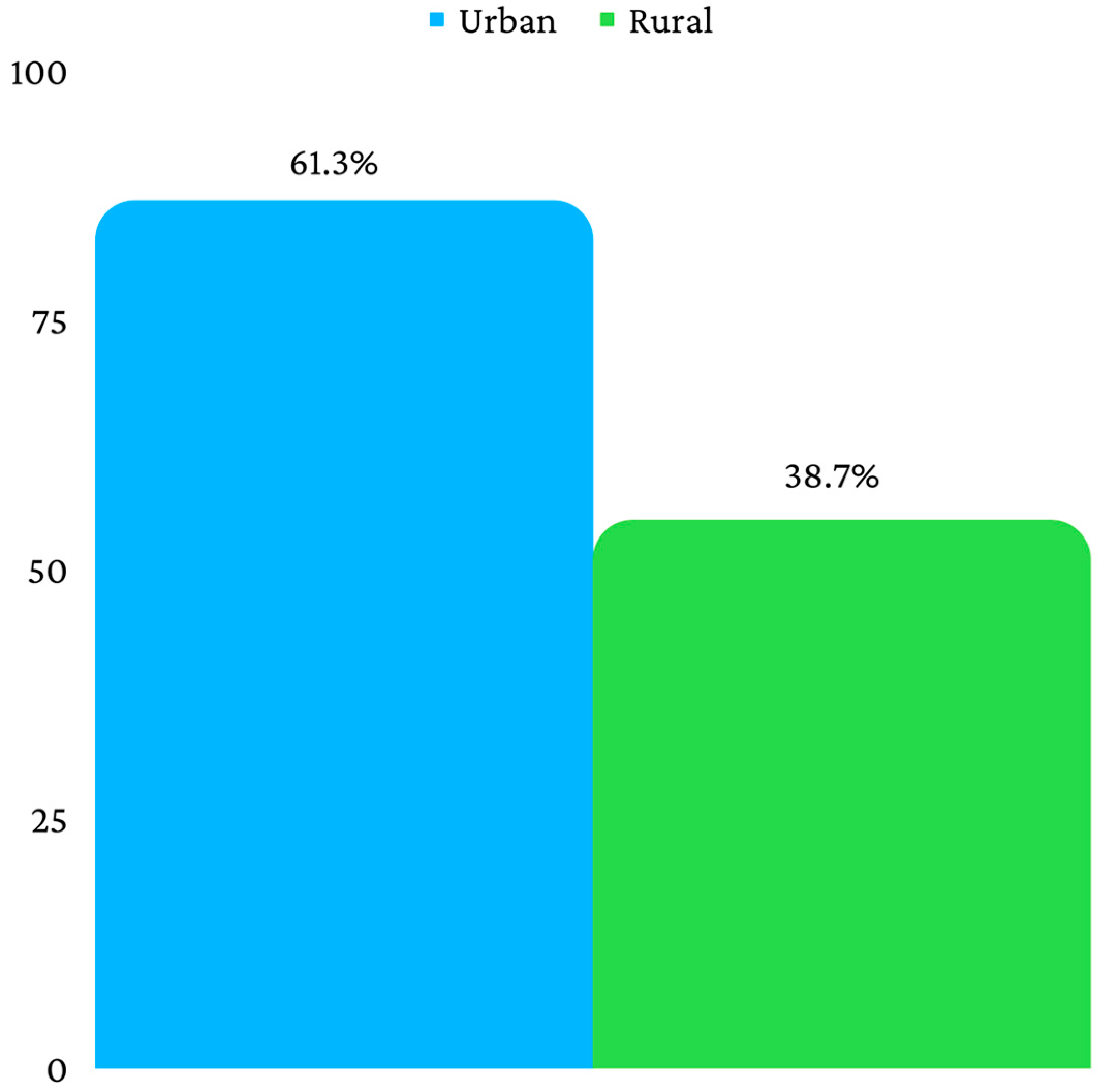
| Rural | 35 (37.2%) | 19 (52.8%) | 1 (8.3%) | 0.017 |
| Urban | 59 (62.8%) | 17 (47.2%) | 11 (91.7%) | |
| Fracture Location | No. | Percentage * |
|---|---|---|
| Mandibular angle | 47 | 50% |
| Lateral | 32 | 34% |
| Subcondylar | 31 | 33% |
| Paramedian | 27 | 28.70% |
| Vertical ramus | 3 | 3.20% |
| Median | 2 | 2.10% |
| Coronoid | 2 | 2.10% |
| Fracture Location | No. | Percentage * |
|---|---|---|
| Disjunction of the malar bone | 17 | 47.2% |
| Alveolar | 11 | 30.6% |
| Nasal | 8 | 22.2% |
| Orbital floor | 5 | 13.9% |
| Le Fort I | 2 | 5.6% |
| Le Fort II | 2 | 5.6% |
| Le Fort III | 2 | 5.6% |
| Malar dysfunction | 17 | 47.2% |
| Fracture (n, %) | Mandibular | Midface | Combined | p * |
|---|---|---|---|---|
| Amplitude | ||||
| Fissure | 1 (1.1%) | 6 (16.7%) | 1 (8.3%) | 0.002 |
| Total | 93 (98.9%) | 30 (83.3%) | 11 (91.7%) | |
| Displacement | ||||
| No | 87 (92.6%) | 29 (80.6%) | 6 (50%) | 0.001 |
| Yes | 7 (7.4%) | 7 (19.4%) | 6 (50%) | |
| Fracture (n, %) | Mandibular | Midface | Combined | p * |
|---|---|---|---|---|
| Hematoma | ||||
| No | 72 (76.6%) | 7 (19.4%) | 1 (8.3%) | <0.001 |
| Yes | 22 (23.4%) | 29 (80.6%) | 11 (91.7%) | |
| Laceration | ||||
| No | 78 (83%) | 19 (52.8%) | 5 (41.7%) | <0.001 |
| Yes | 16 (17%) | 17 (47.2%) | 7 (58.3%) | |
| Abrasion | ||||
| No | 73 (77.7%) | 20 (55.6%) | 2 (16.7%) | <0.001 |
| Yes | 21 (22.3%) | 16 (44.4%) | 10 (83.3%) | |
| Fracture (n, %) | Mandibular | Midface | Combined | p * |
|---|---|---|---|---|
| Treatment | ||||
| Orthopedic | 81 (86.2%) | 33 (91.7%) | 8 (66.7%) | 0.085 |
| Osteosynthesis plates | 1 (1.1%) | 1 (2.8%) | 0 (0%) | |
| Cerclage | 5 (5.3%) | 0 (0%) | 0 (0%) | |
| Combined | 7 (7.4%) | 2 (5.6%) | 4 (33.3%) | |
| Evolution | ||||
| Favorable | 91 (96.8%) | 36 (100%) | 11 (91.7%) | 0.229 |
| Unfavorable | 3 (3.2%) | 0 (0%) | 1 (8.3%) | |
| Complications | ||||
| No complications | 91 (96.8%) | 36 (100%) | 11 (91.7%) | 0.124 |
| Osteitis | 3 (3.2%) | 0 (0%) | 0 (0%) | |
| Vicious consolidation | 0 (0%) | 0 (0%) | 1 (8.3%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juncar, R.I.; Moca, A.E.; Juncar, M.; Moca, R.T.; Țenț, P.A. Clinical Patterns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study. Children 2023, 10, 800. https://doi.org/10.3390/children10050800
Juncar RI, Moca AE, Juncar M, Moca RT, Țenț PA. Clinical Patterns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study. Children. 2023; 10(5):800. https://doi.org/10.3390/children10050800
Chicago/Turabian StyleJuncar, Raluca Iulia, Abel Emanuel Moca, Mihai Juncar, Rahela Tabita Moca, and Paul Andrei Țenț. 2023. "Clinical Patterns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study" Children 10, no. 5: 800. https://doi.org/10.3390/children10050800
APA StyleJuncar, R. I., Moca, A. E., Juncar, M., Moca, R. T., & Țenț, P. A. (2023). Clinical Patterns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study. Children, 10(5), 800. https://doi.org/10.3390/children10050800