
Association between Weight Status and Mental Health among Korean Adolescents: A Nationwide Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Body Weight Status
2.2.2. Health Condition
2.2.3. Socio-Demographic Variables
2.3. Statistical Analyses
2.4. Ethics Statements
3. Results
3.1. General Characteristics of the Study Population
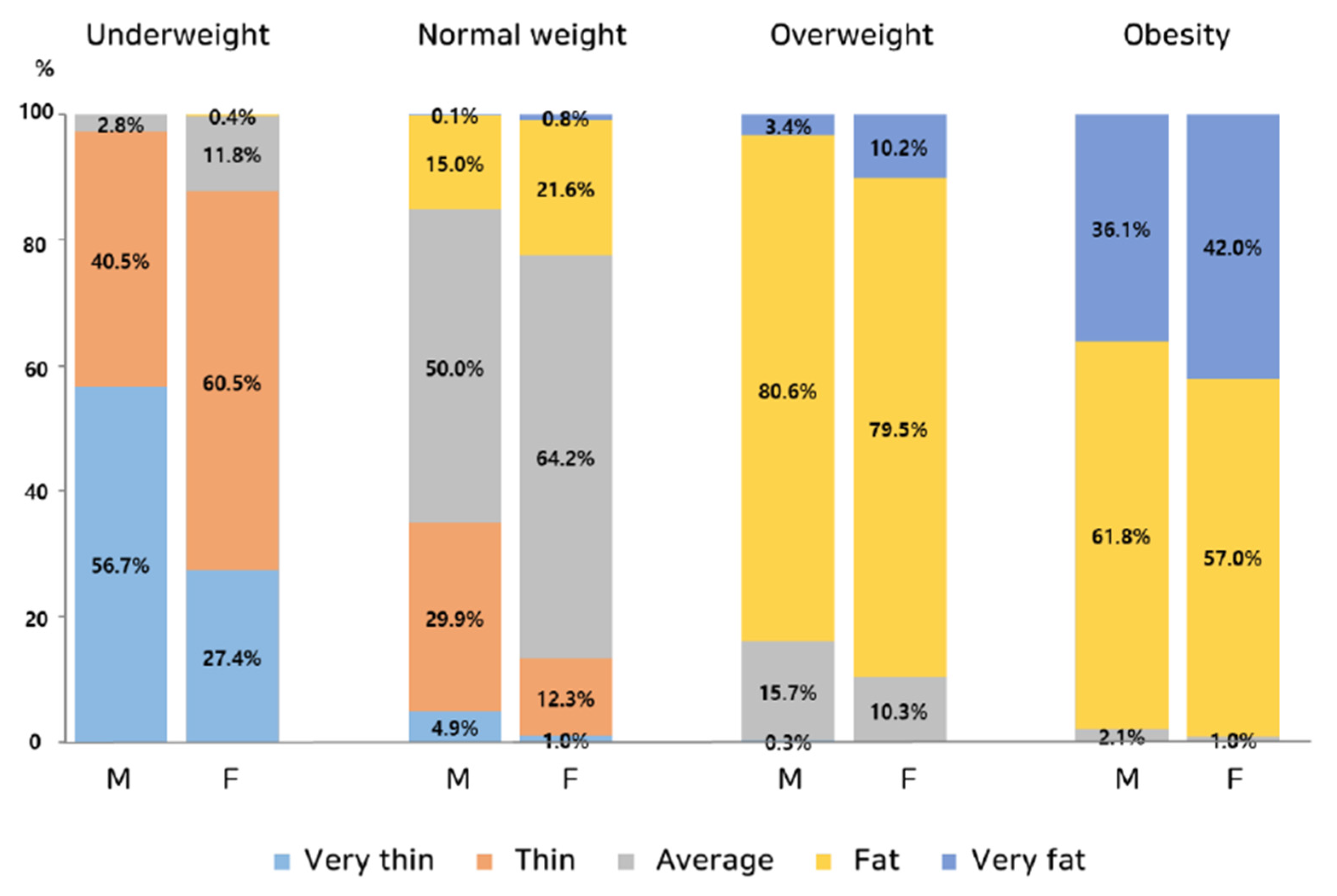
3.2. Body Weight Status of the Study Population According to Sex
3.3. Health Condition of the Study Population
3.4. Association between Body Weight Status and Mental Health Conditions
3.5. Subgroup Analysis of the Characteristics Associated with Mental Health Conditions among Obese Adolescents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blakemore, S.J. Adolescence and mental health. Lancet 2019, 393, 20301. [Google Scholar] [CrossRef] [PubMed]
- Assopardi, P. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar]
- Borelli, J.L.; Prinstein, M.J. Reciprocal, Longitudinal Associations Among Adolescents’ Negative Feedback-Seeking, Depressive Symptoms, and Peer Relations. J. Abnorm. Child Psychol. 2006, 34, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Graber, J.A. Pubertal timing and the development of psychopathology in adolescence and beyond. Horm. Behav. 2013, 64, 262–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adolescent Mental Health; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 17 November 2020).
- Patel, V.; Flisher, A.J.; Hetrick, S.; McGorry, P. Mental health of young people: A global public-health challenge. Lancet 2007, 369, 1302–1313. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Gu, X.; Zhang, T.; Lee, J. Adolescents’ physical activity and depressive symptoms: A psychosocial mechanism. Int. J. Environ. Res. Public Health 2022, 19, 1276. [Google Scholar] [CrossRef] [PubMed]
- Pulgarón, E.R. Childhood Obesity: A Review of Increased Risk for Physical and Psychological Comorbidities. Clin. Ther. 2013, 35, A18–A32. [Google Scholar] [CrossRef]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of Australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolesc. Health Med. Ther. 2016, 7, 125–146. [Google Scholar] [CrossRef]
- Yi, D.Y.; Kim, S.C.; Lee, J.H.; Lee, E.H.; Kim, J.Y.; Kim, Y.J.; Kang, K.S.; Hong, J.; Shim, J.O.; Lee, Y.; et al. Clinical practice guideline for the diagnosis and treatment of pediatric obesity: Recommendations from the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology Hepatology and Nutrition. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 1111312. [Google Scholar] [CrossRef]
- Sanderson, K.; Patton, G.C.; McKercher, C.; Dwyer, T.; Venn, A.J. Overweight and Obesity in Childhood and Risk of Mental Disorder: A 20-Year Cohort Study. Aust. N. Z. J. Psychiatry 2011, 45, 384–392. [Google Scholar] [CrossRef]
- Quek, Y.-H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Sun, Q.; Zhai, L.; Bai, Y.; Wei, W.; Jia, L. The Prevalence of Depression and Anxiety Symptoms among Overweight/Obese and Non-Overweight/Non-Obese Children/Adolescents in China: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 340. [Google Scholar] [CrossRef]
- Jung, S.J.; Woo, H.-T.; Cho, S.; Park, K.; Jeong, S.; Lee, Y.J.; Kang, D.; Shin, A. Association between body size, weight change and depression: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 211, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Herbozo, S.; Thompson, J.K. Obesity in Youth: Causes, Consequences, and Cures; American Psychological Association: Washington, DC, USA, 2009; pp. 99–114. [Google Scholar]
- Gaskin, J.L.; Pulver, A.J.; Branch, K.; Kabore, A.; James, T.; Zhang, J. Perception or reality of body weight: Which matters to the depressive symptoms. J. Affect. Disord. 2013, 150, 350–355. [Google Scholar] [CrossRef]
- Mingoia, J.; Hutchinson, A.D.; Wilson, C.; Gleaves, D.H. The relationship between social networking site use and the internalization of a thin ideal in females: A meta-analytic review. Front. Psychol. 2017, 8, 1351. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Xu, Y.; Guo, X.; Zhang, J.; Wang, H.; Lou, X.; Liang, J.; Tao, F. Body image as risk factor for emotional and behavioral problems among Chinese adolescents. BMC Public Health 2018, 18, 1179. [Google Scholar] [CrossRef]
- Paxton, S. Body image dissatisfaction, extreme weight loss behaviours: Suitable targets for public health concerns? Health Promot. J. Austr. 2000, 10, 15–19. [Google Scholar]
- Dion, J.; Hains, J.; Vachon, P.; Plouffe, J.; Laberge, L.; Perron, M.; McDuff, P.; Kalinova, E.; Leone, M. Correlates of body dissatis-faction in children. J. Pediatrics. 2016, 171, 202–207. [Google Scholar] [CrossRef]
- Brunet, J.; Sabiston, C.M.; Dorsch, K.D.; McCreary, D.R. Exploring a model linking social physique anxiety, drive for muscularity, drive for thinness and self-esteem among adolescent boys and girls. Body Image 2010, 7, 137–142. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yun, S.; Hwang, S.-S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135–149. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Mental Health Promotive and Preventive Interventions for Adolescents: Helping Adolescents Thrive; World Health Organization: Geneva, Switzerland; Available online: https://www.who.int/publications/i/item/9789240011854 (accessed on 28 September 2020).
- Mojtabai, R.; Olfson, M.; Han, B. National Trends in the Prevalence and Treatment of Depression in Adolescents and Young Adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef]
- Kim, K.M. What makes adolescents psychologically distressed? Life events as risk factors for depression and suicide. Eur. Child Adolesc. Psychiatry 2021, 30, 359–367. [Google Scholar] [CrossRef]
- Webb, H.J.; Zimmer-Gembeck, M.J. The role of friends and peers in adolescent body dissatisfaction: A review and critique of 15 years of research. J. Res. Adolesc. 2014, 24, 564–590. [Google Scholar] [CrossRef]
- Luppino, F.S.; De Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and de-pression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- McCrea, R.L.; Berger, Y.G.; King, M.B. Body mass index and common mental disorders: Exploring the shape of the association and its moderation by age, gender and education. Int. J. Obes. 2011, 36, 414–421. [Google Scholar] [CrossRef] [PubMed]
- de Wit, L.M.; van Straten, A.; van Herten, M.; Penninx, B.W.; Cuijpers, P. Depression and body mass index, a u-shaped association. BMC Public Health 2009, 9, 14. [Google Scholar] [CrossRef]
- Hong, S.M.; Hur, Y.I. Relationship between obesity and depression in Korean adults: Korea National Health and Nutrition Examination Survey 2014. Medicine 2017, 96, e9478. [Google Scholar] [CrossRef]
- Lee, J.-H.; Park, S.K.; Ryoo, J.-H.; Oh, C.-M.; Choi, J.-M.; McIntyre, R.S.; Mansur, R.B.; Kim, H.; Hales, S.; Jung, J.Y. U-shaped relationship between depression and body mass index in the Korean adults. Eur. Psychiatry 2017, 45, 72–80. [Google Scholar] [CrossRef]
- Brewis, A.A.; Han, S.Y.; SturtzSreetharan, C.L. Weight, gender, and depressive symptoms in South Korea. Am. J. Hum. Biol. 2017, 29, e22972. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.W.; Hong, S.M. Relationships among Body Mass Index, Body Image, and Depression in Korean Adults: Korea National Health and Nutrition Examination Survey 2014 and 2016. J. Obes. Metab. Syndr. 2019, 28, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Darimont, T.; Karavasiloglou, N.; Hysaj, O.; Richard, A.; Rohrmann, S. Body weight and self-perception are associated with depression: Results from the National Health and Nutrition Examination Survey (NHANES) 2005–2016. J. Affect. Disord. 2020, 274, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Choi, Y.; Han, K.-T.; Cheon, S.-Y.; Kim, J.-H.; Lee, S.G.; Park, E.-C. The Combined Effect of Subjective Body Image and Body Mass Index (Distorted Body Weight Perception) on Suicidal Ideation. J. Prev. Med. Public Health 2015, 48, 94–104. [Google Scholar] [CrossRef]
- Choi, Y.; Choi, E.; Shin, D.; Park, S.M.; Lee, K. The Association between Body Weight Misperception and Psychosocial Factors in Korean Adult Women Less than 65 Years Old with Normal Weight. J. Korean Med. Sci. 2015, 30, 1558–1566. [Google Scholar] [CrossRef]
- Kim, Y.; Austin, S.B.; Subramanian, S.V.; Kawachi, I. Body weight perception, disordered weight control behaviors, and de-pressive symptoms among Korean adults: The Korea National Health and Nutrition Examination Survey 2014. PLoS ONE. 2018, 13, e0198841. [Google Scholar]
- Roberts, R.E.; Duong, H.T. Perceived weight, not obesity, increases risk for major depression among adolescents. J. Psychiatr. Res. 2013, 47, 1110–1117. [Google Scholar] [CrossRef]
- Seo, D.-C.; Lee, C.G. The effect of perceived body weight on suicidal ideation among a representative sample of US adolescents. J. Behav. Med. 2013, 36, 498–507. [Google Scholar] [CrossRef]
- Huang, L.; Tao, F.-B.; Wan, Y.-H.; Xing, C.; Hao, J.; Su, P.-Y.; Xing, X.-Y. Self-reported weight status rather than BMI may be closely related to psychopathological symptoms among Mainland Chinese adolescents. J. Trop. Pediatr. 2011, 57, 307–311. [Google Scholar] [CrossRef]
- Frisco, M.L.; Houle, J.N.; Martin, M.A. The image in the mirror and the number on the scale: Weight, weight perceptions, and adolescent depressive symptoms. J. Health. Soc. Behav. 2010, 51, 215–228. [Google Scholar] [CrossRef]
- Chai, L.; Xue, J. Weight, weight perceptions, and health and well-being among Canadian adolescents: Evidence from the 2017–2018 Canadian Community Health Survey. Am. J. Health. Promot. 2022, 36, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Rao, W.-W.; Zong, Q.-Q.; Zhang, J.-W.; An, F.-R.; Jackson, T.; Ungvari, G.S.; Xiang, Y.; Su, Y.-Y.; D’Arcy, C.; Xiang, Y.-T. Obesity increases the risk of depression in children and adolescents: Results from a systematic review and meta-analysis. J. Affect. Disord. 2020, 267, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Mannan, M.; Mamun, A.; Doi, S.; Clavarino, A. Is there a bi-directional relationship between depression and obesity among adult men and women? Systematic review and bias-adjusted meta analysis. Asian J. Psychiatry 2016, 21, 51–66. [Google Scholar] [CrossRef]
- Thurston, I.B.; Sonneville, K.R.; Milliren, C.E.; Kamody, R.C.; Gooding, H.C.; Richmond, T.K. Cross-sectional and Prospective Examination of Weight Misperception and Depressive Symptoms Among Youth with Overweight and Obesity. Prev. Sci. 2017, 18, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Haynes, A.; Sutin, A.; Daly, M. Self-perception of overweight and obesity: A review of mental and physical health outcomes. Obes. Sci. Pract. 2020, 6, 552–561. [Google Scholar] [CrossRef]
- Byeon, H. Association between Weight Misperception Patterns and Depressive Symptoms in Korean Young Adolescents: National Cross-Sectional Study. PLoS ONE 2015, 10, e0131322. [Google Scholar] [CrossRef]
- Lim, Y.; Kim, B. Body Mass Index, Body Weight Perception, and Depressed Mood in Korean Adolescents. J. Korean Acad. Child Adolesc. Psychiatry 2017, 28, 31–37. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 5683) | Male (n = 3013) | Female (n = 2670) | p Value | Overweight & Obese (n = 1186) | p Value * |
|---|---|---|---|---|---|---|
| Estimated population (%) | 4,050,528 (100%) | 2,152,279 (53.1%) | 1,898,250 (46.9%) | 842,414 (20.8%) | ||
| Age (years) | 15.1 ± 0.0 | 15.2 ± 0.0 | 15.1 ± 0.0 | 0.450 | 15.3 ± 0.1 | 0.007 |
| Total calorie intake (kcal/d) | 2204.5 ± 16.5 | 2486.2 ± 24.6 | 1887.4 ± 18.1 | <0.001 | 2129.9 ± 32.5 | 0.006 |
| Body mass index (%tile) | 0.001 | |||||
| Underweight (<5th) | 8.3 (0.5)% | 9.9 (0.7)% | 6.5 (0.5)% | |||
| Normal (5~85th) | 70.8 (0.7)% | 68.6 (1.0)% | 73.3 (1.0)% | |||
| Overweight (85~95th) | 9.1 (0.4)% | 9.2 (0.6)% | 9.1 (0.6)% | |||
| Obesity (>95th) | 11.7 (0.5)% | 12.3 (0.7)% | 11.1 (0.7)% | |||
| Weight perception | <0.001 | <0.001 | ||||
| Very thin | 6.0 (0.4)% | 9.0 (0.7)% | 2.5 (0.3)% | 0.1 (0.1)% | ||
| Thin | 19.1 (0.6)% | 24.6 (0.9)% | 13.0 (0.8)% | 0.0% | ||
| Average | 42.1 (0.8)% | 36.2 (1.0)% | 48.8 (1.2)% | 6.7 (0.8)% | ||
| Fat | 27.2 (0.7)% | 25.3 (0.9)% | 29.3 (1.1)% | 68.6 (1.5)% | ||
| Very fat | 5.5 (0.4)% | 4.8 (0.5)% | 6.3 (0.6)% | 24.6 (1.5)% | ||
| Weight misperception | <0.001 | <0.001 | ||||
| Concordance | 71.1 (0.7)% | 72.3 (1.0)% | 69.8 (1.0)% | 56.8 (1.6)% | ||
| Discordance, underestimated | 10.5 (0.5)% | 12.7 (0.7)% | 8.1 (0.6)% | 40.3 (1.6)% | ||
| Discordance, overestimated | 18.4 (0.6)% | 15.0 (0.8)% | 22.1 (0.9)% | 2.9 (0.5)% | ||
| Intention to control weight | <0.001 | <0.001 | ||||
| No | 33.0 (0.7)% | 40.2 (1.0)% | 24.8 (1.0)% | 13.8 (1.1)% | ||
| Yes | 67.0 (0.7)% | 59.8 (1.0)% | 75.2 (1.0)% | 86.2 (1.1)% | ||
| Perceived health status | 0.009 | <0.001 | ||||
| Good/Very good | 59.1 (0.8)% | 61.4 (1.1)% | 56.6 (1.1)% | 48.2 (1.7)% | ||
| Fair | 35.2 (0.8)% | 33.2 (1.1)% | 37.4 (1.1)% | 43.1 (1.7)% | ||
| Bad/Very bad | 5.7 (0.4)% | 5.4 (0.5)% | 6.1 (0.5)% | 8.6 (1.0)% | ||
| Depressed mood | <0.001 | 0.409 | ||||
| No | 90.9 (0.5)% | 92.6 (0.6)% | 88.9 (0.7)% | 90.2 (1.0)% | ||
| Yes | 9.1 (0.5)% | 7.4 (0.6)% | 11.1 (0.7)% | 9.8 (1.0)% | ||
| Perceived stress | <0.001 | 0.060 | ||||
| None/Mild | 74.3 (0.7)% | 77.6 (0.9)% | 70.5 (1.0)% | 71.9 (1.5)% | ||
| Much/Very much | 25.7 (0.7)% | 22.4 (0.9)% | 29.5 (1.0)% | 28.1 (1.5)% | ||
| Suicidal ideation | <0.001 | 0.360 | ||||
| No | 92.6 (0.4)% | 95.2 (0.5)% | 89.6 (0.7)% | 91.9 (0.9)% | ||
| Yes | 7.4 (0.4)% | 4.8 (0.5)% | 10.4 (0.7)% | 8.1 (0.9)% | ||
| Household income | 0.188 | 0.846 | ||||
| High | 29.4 (1.0)% | 29.7 (1.1)% | 29.1 (1.3)% | 29.7 (1.6)% | ||
| Middle | 57.5 (1.0)% | 58.1 (1.2)% | 56.8 (1.3)% | 56.8 (1.7)% | ||
| Low | 13.1 (0.7)% | 12.2 (0.8)% | 14.1 (0.9)% | 13.5 (1.3)% | ||
| Area of residency | 0.058 | 0.564 | ||||
| Urban area | 84.5 (1.2)% | 85.4 (1.2)% | 83.4 (1.4)% | 85.1 (1.6)% | ||
| Rural area | 15.5 (1.2)% | 14.6 (1.2)% | 16.6 (1.4)% | 14.9 (1.6)% |
| Depressed Mood | Perceived Stress | Suicidal Ideation | ||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Body mass index 1 | ||||||
| Underweight | 1.119 (0.651–1.923) | 1.103 (0.612–1.987) | 0.751 (0.530–1.065) | 1.362 (0.898–2.067) | 1.137 (0.575–2.249) | 0.701 (0.342–1.439) |
| Overweight | 1.197 (0.674–2.126) | 1.166 (0.717–1.896) | 1.052 (0.709–1.561) | 1.002 (0.691–1.453) | 1.195 (0.631–2.263) | 1.164 (0.662–2.046) |
| Obesity | 0.964 (0.513–1.814) | 0.799 (0.473–1.349) | 0.997 (0.706–1.407) | 1.070 (0.765–1.498) | 1.032 (0.539–1.974) | 0.887 (0.545–1.444) |
| Weight perception 2 | ||||||
| Thin/Very thin | 0.863 (0.528–1.409) | 1.159 (0.671–2.001) | 1.138 (0.854–1.514) | 0.980 (0.676–1.421) | 1.995 * (1.143–3.485) | 1.532 (0.868–2.702) |
| Fat/Very fat | 1.207 (0.660–2.207) | 1.963 † (1.272–3.030) | 1.448 (0.992–2.114) | 1.866 ‡ (1.389–2.506) | 1.193 (0.532–2.676) | 1.505 (0.978–2.315) |
| Weight misperception 2 | ||||||
| Discordance, underestimated | 1.543 (0.860–2.767) | 1.545 (0.782–3.052) | 1.391 (0.931–2.079) | 0.852 (0.512–1.418) | 1.329 (0.611–2.891) | 0.616 (0.301–1.261) |
| Discordance, overestimated | 1.234 (0.755–2.016) | 1.969 ‡ (1.359–2.852) | 1.232 (0.879–1.725) | 1.821 ‡ (1.376–2.409) | 1.074 (0.599–1.926) | 1.345 (0.896–2.018) |
| Depressed Mood | Perceived Stress | Suicidal Ideation | ||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Weight perception 1 | ||||||
| Average | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Fat/Very fat | 0.744 (0.205–2.702) | 0.876 (0.229–3.345) | 0.988 (0.452–2.160) | 2.109 (0.807–5.510) | 0.604 (0.157–2.323) | 6.179 (0.804–47.509) |
| Weight misperception 1 | ||||||
| Discordance, underestimated | 1.357 (0.644–2.859) | 1.157 (0.569–2.354) | 1.143 (0.727–1.798) | 0.745 (0.466–1.191) | 1.242 (0.531–2.908) | 0.561 (0.263–1.194) |
| Concordance | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Perceived health status 2 | ||||||
| Good/Very good | 0.901 (0.403–2.015) | 0.675 (0.332–1.372) | 0.818 (0.511–1.310) | 0.479 † (0.298–0.769) | 1.188 (0.433–3.259) | 0.653 (0.299–1.424) |
| Bad/Very bad | 0.690 (0.177–2.684) | 3.432 * (1.190–9.903) | 1.746 (0.819–3.722) | 2974 * (1.187–7.450) | 6.977 ‡ (2.402–20.265) | 5.534 † (2.038–15.028) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Hong, J. Association between Weight Status and Mental Health among Korean Adolescents: A Nationwide Cross-Sectional Study. Children 2023, 10, 620. https://doi.org/10.3390/children10040620
Choi Y, Hong J. Association between Weight Status and Mental Health among Korean Adolescents: A Nationwide Cross-Sectional Study. Children. 2023; 10(4):620. https://doi.org/10.3390/children10040620
Chicago/Turabian StyleChoi, Youngha, and Jeana Hong. 2023. "Association between Weight Status and Mental Health among Korean Adolescents: A Nationwide Cross-Sectional Study" Children 10, no. 4: 620. https://doi.org/10.3390/children10040620
APA StyleChoi, Y., & Hong, J. (2023). Association between Weight Status and Mental Health among Korean Adolescents: A Nationwide Cross-Sectional Study. Children, 10(4), 620. https://doi.org/10.3390/children10040620