

Validation of the Concise Assessment Scale for Children’s Handwriting (BHK) in an Italian Population



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Informed Consent and Ethical Approval
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Sample
3.2. Handwriting Quality (BHK Quality)
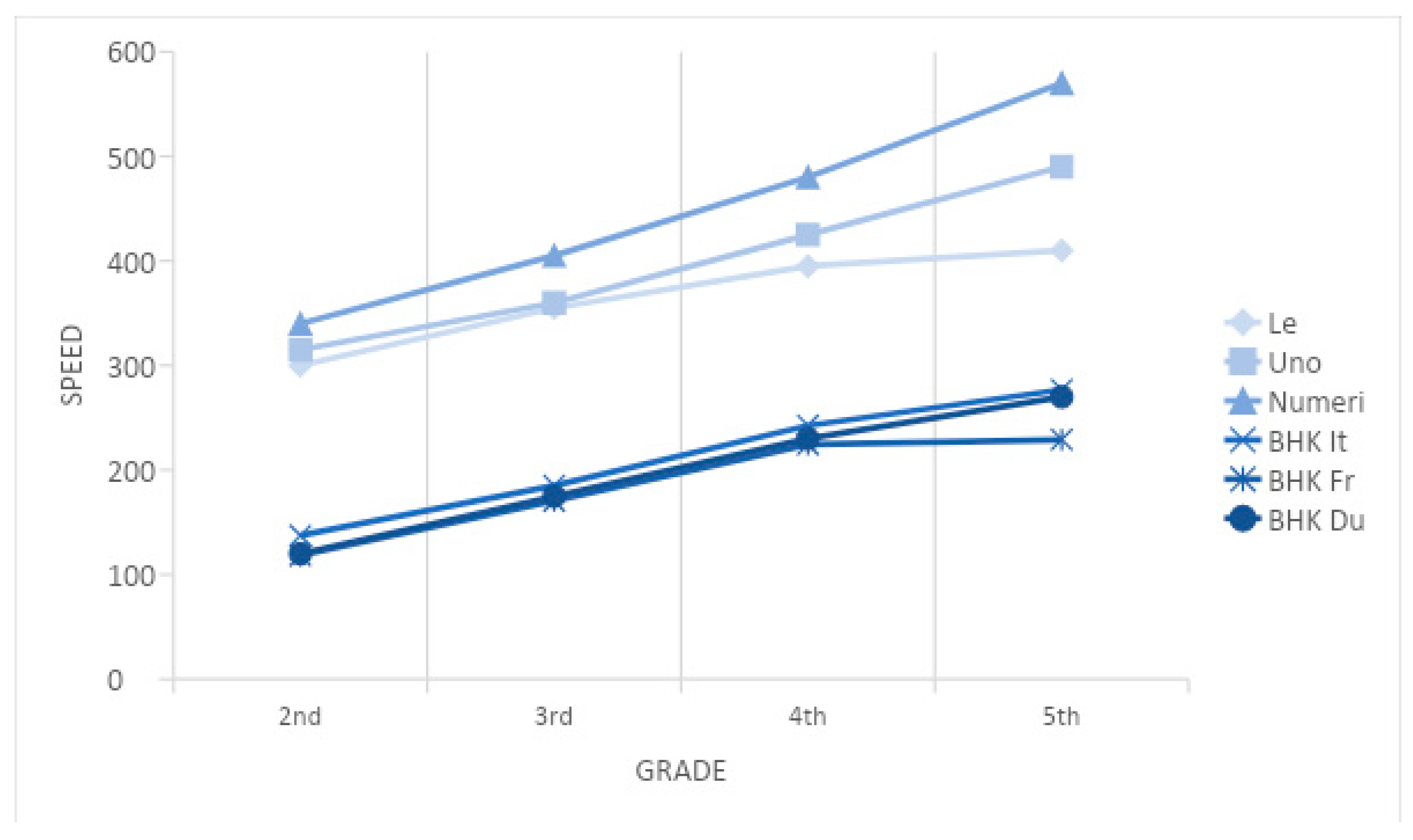
3.3. Copying Speed (BHK Speed)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, L.T.; Missiuna, C.A.; Macnab, J.J.; Malloy-Miller, T.; Polatajko, H.J. Clinical description of children with developmental coordination disorder. Can. J. Occup. Ther. 2001, 68, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Karlsdottir, R.; Stefansson, T. Problems in developing functional handwriting. Percept Mot Skills. 2002, 94, 623–662. [Google Scholar] [CrossRef] [PubMed]
- Smits-Engelsman, B.C.M.; Niemeijer, G.P.; van Galen, G.P. Fine motor deficiencies in children diagnosed as DCD based on poor grapho-motor ability. Hum. Mov. Sci. 2001, 20, 161–182. [Google Scholar] [CrossRef] [PubMed]
- McHale, K.; Cermak, S.A. Fine Motor Activities in Elementary School: Preliminary Findings and Provisional Implications for Children with Fine Motor Problems. Am. J. Occup. Ther. 1992, 46, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Tse, L.; Siu, A.; Li-Tsang, C. Developmental skills between kindergarten children with handwriting difficulties in Chinese and/or English. Aust. Occup. Ther. J. 2018, 66, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Yu, N.Y. Evaluation and classification of types of Chinese handwriting deficits in elementary school children. Percept. Mot. Ski. 2005, 101, 631–647. [Google Scholar] [CrossRef] [PubMed]
- Gubbay, S.S.; de Klerk, N.H. A study and review of developmental dysgraphia in relation to acquired dysgraphia. Brain Dev. 1995, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Am. Psychiatr. Assoc. 2013, 21, 591–643. [Google Scholar] [CrossRef]
- Rosenblum, S.; Parush, S.; Weiss, P.L. The In Air phenomenon: Temporal and spatial correlates of the handwriting process. Percept. Mot. Ski. 2003, 96, 933–954. [Google Scholar] [CrossRef] [PubMed]
- Dinehart, L.H. Handwriting in early childhood education: Current research and future implications. J. Early Child. Liter. 2015, 15, 97–118. [Google Scholar] [CrossRef]
- Prunty, M.M.; Barnett, A.L.; Wilmut, K.; Plumb, M.S. The impact of handwriting difficulties on compositional quality in children with developmental coordination disorder. Br. J. Occup. Ther. 2016, 79, 591–597. [Google Scholar] [CrossRef]
- Rosenblum, S. Handwriting measures as reflectors of executive functions among adults with Developmental Coordination Disorders (DCD). Front. Psychol. 2013, 4, 357. [Google Scholar] [CrossRef]
- Rosenblum, S.; Livneh-Zirinski, M. Handwriting process and product characteristics of children diagnosed with developmental coordination disorder. Hum. Mov. Sci. 2008, 27, 200–214. [Google Scholar] [CrossRef]
- Rosenblum, S.; Margieh, J.A.; Engel-Yeger, B. Handwriting features of children with developmental coordination disorder--results of triangular evaluation. Res. Dev. Disabil. 2013, 34, 4134–4141. [Google Scholar] [CrossRef] [PubMed]
- Geuze, R.H. Constraints in Neuromotor Development. In Developmental Motor Disorders: A Neuropsychological Perspective; Tupper, D., Dewey, D., Eds.; Guilford Press: New York, NY, USA, 2004; pp. 391–404. [Google Scholar]
- Cousins, M.; Smyth, M.M. Development coordination impairments in adulthood. Hum. Mov. Sci. 2003, 22, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Baldi, S.; Nunzi, M.; Di Brina, C. Efficacy of a task-based training approach in the rehabilitation of three children with poor handwriting quality: A pilot study. Percept. Mot. Ski. 2015, 120, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Chu, S. Occupational Therapy for Children with Handwriting Difficulties: A Framework for Evaluation and Treatment. Br. J. Occup. Ther. 1997, 60, 514–520. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A. Movement Assessment Battery for Children Manual; Psychological Corporation/Harcour Brace-Jovanovich: New York, NY, USA, 1992. [Google Scholar]
- Beery, K.E.; Beery, N.A. Beery VMI: The Beery-Buktenica Developmental Test of Visual-Motor Integration, 5th ed.; Pearson: Minneapolis, MN, USA, 2004. [Google Scholar]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef] [PubMed]
- Hamstra-Bletz, E.; De Bie, J.; den Brinker, B.P.O.L. Beknopte Beoordelings Methode Voor Kinder Handschiften; The concise assessment method for children handwriting; Swets and Zeitlinger: Lisse, The Netherlands, 1987. [Google Scholar]
- Overvelde, A.; Hulstijn, W. Handwriting development in grade 2 and grade 3 primary school children with normal, at risk, or dysgraphic characteristics. Res. Dev. Disabil. 2011, 32, 540–548. [Google Scholar] [CrossRef]
- Rubin, N.; Henderson, S.E. Two sides of the same coin: Variation in teaching methods and failure to learn to write. Spec. Educ. Forw. Trends 1982, 9, 17–24. [Google Scholar] [CrossRef]
- Charles, M.; Soppelsa, R.; Albaret, J.M. BHK- Echelle D’evaluation Rapide de L’ecriture chez L’enfant; Editions et Applications Psychologiques: Paris, France, 2003. [Google Scholar]
- Di Brina, C.; Rossini, G. Test BHK–Scala Sintetica per la Valutazione della Scrittura in Età Evolutiva. Trento: Erickson (Italian Adaptation of Hamstra-Bletz, L.; De Bie, J.; Den Brinker, B.P.L.M.; 1987). Beknopte beoordelingsmethode voor kinderhandschriften: Experimentele Versie. Concise Evaluation Scale for Children’s Handwriting: Experimental Version; Swets and Zeitlinger: Lisse, The Netherlands, 2010. [Google Scholar]
- Tressoldi, P.E.; Cornoldi, C.; Re, A.M. BVSCO-2: Test for the Evaluation of Writing and Orthographic Ability; Giunti OS: Florence, Italy, 2013. [Google Scholar]
- Hamstra-Bletz, L.; Blote, A.W. Development of handwriting in primary school: A longitudinal study. Percept. Mot. Ski. 1990, 70, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Van Waelvelde, H.; Hellinckx, T.; Peersman, W.; Smits-Engelsman, B.C. SOS: A screening instrument to identify children with handwriting impairments. Phys. Occup. Ther. Pediatr. 2012, 32, 306–319. [Google Scholar] [CrossRef] [PubMed]
- Ministero dell’Istruzione, dell’Università e della Ricerca. Indicazioni Nazionali per le Scuole dell’infanzia e del Primo Ciclo di Istruzione. Trasmissione dei Risultati Sintetici della Consultazione delle Scuole e Testo Aggiornato del Documento. Prot. 5559. 2012. Available online: https://www.istruzione.it/archivio/web/istruzione/prot5559_12.html (accessed on 19 January 2023).
- Di Brina, C.; Caravale, B.; Mirante, N. Handwriting in Children with Developmental Coordination Disorder: Is Legibility the Only Indicator of a Poor Performance? Occup. Ther. Health Care 2022, 36, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Jongmans, M.J.; Linthorst-Bakker, E.; Westenberg, Y.; Smits-Engelsman, B.C. Use of a task-oriented self-instruction method to support children in primary school with poor handwriting quality and speed. Hum. Mov. Sci. 2003, 22, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Dolek, O.; Hamzadayi, E. Comparison of Writing Skills of Students of Different Socioeconomic Status. Int. J. Progress. Educ. 2018, 14, 6. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.C.; Schoemaker, M.M. Consequences of comorbidity of developmental coordination disorders and learning disabilities for severity and pattern of perceptual-motor dysfunction. J. Learn. Disabil. 2003, 36, 528–537. [Google Scholar]
- Martins, M.R.; Bastos, J.A.; Cecato, A.T.; Araujo, M.L.; Magro, R.R.; Alaminos, V. Screening for motor dysgraphia in public schools. J. De Pediatr. 2013, 89, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Feder, K.; Majnemer, A. Handwriting development, Competency and Intervention. Dev. Med. Child Neurol. 2006, 49, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Sugden, D.A. (Ed.) Leeds Consensus Statement. Developmental Coordination Disorder as a Specific Learning Difficulty. Economic and Social Research Council Research Seminar. 2006. Available online: http://www.dcd-uk.org (accessed on 19 January 2023).


{kind=link}
| Grade | Gender | ||
|---|---|---|---|
| Male N (%) | Female N (%) | Total N | |
| 2nd | 73 (55) | 59 (45) | 132 |
| 3rd | 57 (48) | 62 (52) | 119 |
| 4th | 81 (52) | 74 (48) | 155 |
| 5th | 72 (47) | 84 (53) | 156 |
| Total | 283 (50) | 279 (50) | 562 |
| EFFECT | Wilks’ λ | Rao’s ρ | dF 1 | dF 2 | p-Level |
|---|---|---|---|---|---|
| Class | 0.545400 | 65.14954 | 6 | 1104 | 0.000000 * |
| Gender | 0.968243 | 9.05249 | 2 | 552 | 0.000135 * |
| 1, 2 | 0.995753 | 0.39194 | 6 | 1104 | 0.884502 |
| dF | MS | dF | MS | |||
|---|---|---|---|---|---|---|
| EFFECT | EFFECT | EFFECT | ERROR | ERROR | F | p-Level |
| 1 | 3 | 75.97 | 553 | 41.76 | 1.819 | 0.1425 |
| 2 | 1 | 743.16 | 553 | 41.76 | 17.796 | 0.000029 * |
| 1, 2 | 3 | 16.11 | 553 | 41.76 | 0.386 | 0.7632 |
| Total | Males | Females | |
|---|---|---|---|
| Mean | 19.3 | 20.3 | 18.1 |
| SD | 6.5 | 6.1 | 6.7 |
| dF | MS | dF | MS | |||
|---|---|---|---|---|---|---|
| EFFECT | EFFECT | EFFECT | ERROR | ERROR | F | p-Level |
| 1 | 3 | 531,550 | 553 | 3,540,189 | 150.14 | 0.000000 * |
| 2 | 1 | 1822.4 | 553 | 3,540,189 | 0.5148 | 0.4733 |
| 1, 2 | 3 | 1448.9 | 533 | 3,540,189 | 0.4093 | 0.7464 |
| School Grade | BHK It | BHK Fr | BHK Du |
|---|---|---|---|
| 2nd | 137.4 | 118.3 | 120 |
| 3rd | 185.2 | 170.5 | 175 |
| 4th | 242.5 | 224.5 | 230 |
| 5th | 276.9 | 229.1 | 270 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loizzo, A.; Zaccaria, V.; Caravale, B.; Di Brina, C. Validation of the Concise Assessment Scale for Children’s Handwriting (BHK) in an Italian Population. Children 2023, 10, 223. https://doi.org/10.3390/children10020223
Loizzo A, Zaccaria V, Caravale B, Di Brina C. Validation of the Concise Assessment Scale for Children’s Handwriting (BHK) in an Italian Population. Children. 2023; 10(2):223. https://doi.org/10.3390/children10020223
Chicago/Turabian StyleLoizzo, Annalivia, Valerio Zaccaria, Barbara Caravale, and Carlo Di Brina. 2023. "Validation of the Concise Assessment Scale for Children’s Handwriting (BHK) in an Italian Population" Children 10, no. 2: 223. https://doi.org/10.3390/children10020223
APA StyleLoizzo, A., Zaccaria, V., Caravale, B., & Di Brina, C. (2023). Validation of the Concise Assessment Scale for Children’s Handwriting (BHK) in an Italian Population. Children, 10(2), 223. https://doi.org/10.3390/children10020223