
Lifestyle Behaviours Profile of Spanish Adolescents Who Actively Commute to School
 ,
,  ,
,  , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
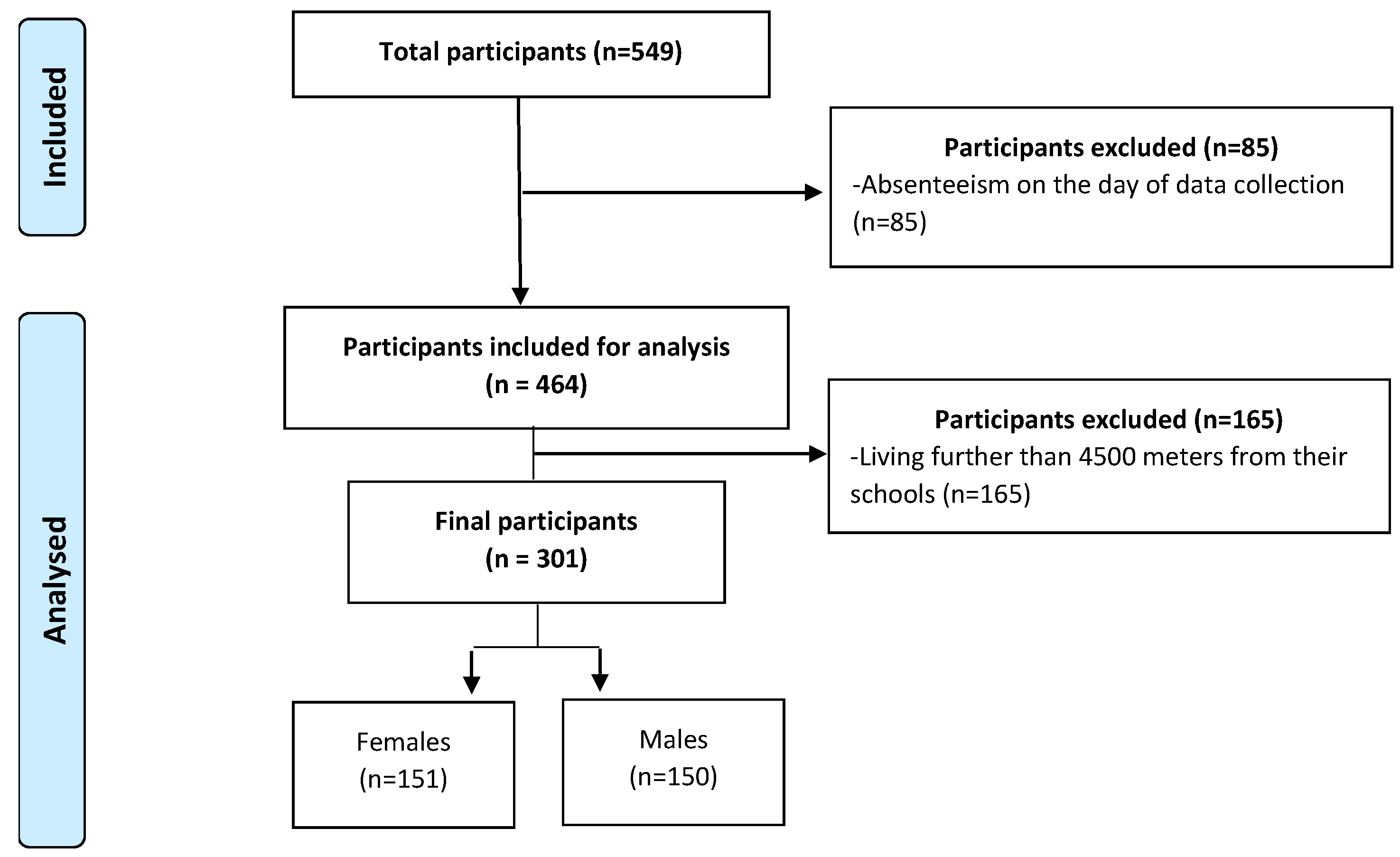
2.2. Participants and Recruitment
2.3. Instruments
2.4. Measures
2.4.1. Mode of Commuting and Distance to School
2.4.2. Lifestyle Behaviours
2.5. Procedure
2.6. Statistics Analysis
3. Results
4. Discussion
4.1. ACS and Gender
4.2. ACS and Distance between Home and School
4.3. ACS and Lifestyle Behaviours
4.3.1. Sedentary Behaviours
4.3.2. Sleep Patterns
4.3.3. Diet Quality
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed]
- Patton, G.C.; Coffey, C.; Carlin, J.B.; Sawyer, S.M.; Williams, J.; Olsson, C.A.; Wake, M. Overweight and obesity between adolescence and young adulthood: A 10-year prospective cohort study. J. Adolesc. Health 2011, 48, 275–280. [Google Scholar] [CrossRef] [PubMed]
- McGovern, C.M.; Militello, L.K.; Arcoleo, K.J.; Melnyk, B.M. Factors Associated With Healthy Lifestyle Behaviors among Adolescents. J. Pediatr. Health Care 2018, 32, 473–480. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia–Systematic Review; Commonwealth Avenue: Canberra, Australia, 2013.
- Rosi, A.; Giopp, F.; Milioli, G.; Melegari, G.; Goldoni, M.; Parrino, L.; Scazzina, F. Weight Status, Adherence to the Mediterranean Diet, Physical Activity Level, and Sleep Behavior of Italian Junior High School Adolescents. Nutrients 2020, 12, 478. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ezzatvar, Y.; López-Gil, J.F.; Ramírez-Vélez, R.; Olloquequi, J.; Izquierdo, M. Is adherence to the Mediterranean diet associated with healthy habits and physical fitness? A systematic review and meta-analysis including 565 421 youths. Brit. J. Nutr. 2020, 128, 1433–1444. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Fan, J.; Yuan, F.; Feng, G.; Gong, W.; Song, C.; Ma, Y.; Chen, Z.; Liu, A. Association between Physical Activity, Sedentary Behaviors, Sleep, Diet, and Adiposity among Children and Adolescents in China. Obes. Facts 2022, 15, 26–35. [Google Scholar] [CrossRef]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef]
- Gomez, S.; Lorenzo, L.; Ribes, C.; Homs, C. Resultados Principales del Estudio PASOS 2019 Sobre la Actividad Física, Los Estilos de Vida y la Obesidad de la Población Española de 8 a 16 Años. 2019, Unpublished Work. Available online: https://www.munideporte.com/imagenes/documentacion/ficheros/025183D9.pdf (accessed on 19 November 2022).
- Aparicio-Ugarriza, R.; Mielgo-Ayuso, J.; Ruiz, E.; Ávila, J.M.; Aranceta-Bartrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; González-Gross, M. Active Commuting, Physical Activity, and Sedentary Behaviors in Children and Adolescents from Spain: Findings from the ANIBES Study. Int. J. Environ. Res. Public Health 2020, 17, 668. [Google Scholar] [CrossRef]
- Turconi, G.; Guarcello, M.; Maccarini, L.; Cignoli, F.; Setti, S.; Bazzano, R.; Roggi, C. Eating habits and behaviors, physical activity, nutritional and food safety knowledge and beliefs in an adolescent Italian population. J. Am. Coll. Nutr. 2008, 27, 31–43. [Google Scholar] [CrossRef]
- Lirola, M.J.; Trigueros, R.; Aguilar-Parra, J.M.; Mercader, I.; Fernandez Campoy, J.M.; Del Pilar Díaz-López, M. Physical Education and the Adoption of Habits Related to the Mediterranean Diet. Nutrients 2021, 13, 567. [Google Scholar] [CrossRef]
- Schoeppe, S.; Duncan, M.J.; Badland, H.; Oliver, M.; Curtis, C. Associations of children’s independent mobility and active travel with physical activity, sedentary behaviour and weight status: A systematic review. J. Sci. Med. Sport 2013, 16, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Tassitano, R.M.; Weaver, R.G.; Tenório, M.C.M.; Brazendale, K.; Beets, M.W. Clusters of non-dietary obesogenic behaviors among adolescents in Brazil: A latent profile analysis. Int. J. Public Health 2020, 65, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Pierson, S.; Khirani, S.; Touil, S.; Leger, D.; Amaddeo, A.; Ouss, L.; Fauroux, B. Sleep in preadolescents and adolescents with chronic disorders. Minerva Pediatr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bruce, E.S.; Lunt, L.; McDonagh, J.E. Sleep in adolescents and young adults. Clin. Med. 2017, 17, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Gómez, D.; Veiga, O.L.; Gomez-Martinez, S.; Zapatera, B.; Calle, M.E.; Marcos, A. Behavioural correlates of active commuting to school in Spanish adolescents: The AFINOS (physical activity as a preventive measure against overweight, obesity, infections, allergies, and cardiovascular disease risk factors in adolescents) study. Public Health Nutr. 2011, 14, 1779–1786. [Google Scholar] [CrossRef]
- Villa-González, E.; Huertas-Delgado, F.J.; Chillón, P.; Ramírez-Vélez, R.; Barranco-Ruiz, Y. Associations between active commuting to school, sleep duration, and breakfast consumption in Ecuadorian young people. BMC Public Health 2019, 19, 85. [Google Scholar] [CrossRef]
- Loureiro, N.; Marques, A.; Loureiro, V.; de Matos, M.G. Active Transportation to School. Utopia or a Strategy for a Healthy Life in Adolescence. Int. J. Environ. Res. Public Health 2021, 18, 4503. [Google Scholar] [CrossRef]
- Zaragoza, J.; Corral, A.; Estrada, S.; Abós, Á.; Aibar, A. Active or passive commuter? Discrepancies in cut-off criteria among adolescents. Int. J. Environ. Res. Public Health 2019, 16, 3796. [Google Scholar] [CrossRef]
- Chillón, P.; Herrador-Colmenero, M.; Migueles, J.H.; Cabanas-Sánchez, V.; Fernández-Santos, J.R.; Veiga, Ó.L.; Castro-Piñero, J. Convergent validation of a questionnaire to assess the mode and frequency of commuting to and from school. Scand J. Public Health 2017, 45, 612–620. [Google Scholar] [CrossRef]
- Segura-Díaz, J.M.; Rojas-Jiménez, Á.; Barranco-Ruiz, Y.; Murillo-Pardo, B.; Saucedo-Araujo, R.G.; Aranda-Balboa, M.J.; Herrador-Colmenero, M.; Villa-González, E.; Chillón, P. Feasibility and Reliability of a Questionnaire to Assess the Mode, Frequency, Distance and Time of Commuting to and from School: The PACO Study. Int. J. Environ. Res. Public Health 2020, 17, 5039. [Google Scholar] [CrossRef]
- Villa-González, E.; Rodríguez-López, C.; Barranco-Ruiz, Y.; Cabezas-Arévalo, L.F.; Chillón, P. Evaluación de la concordancia de dos métodos para determinar la distancia del desplazamiento activo al colegio en escolares. Nutr. Hosp. 2016, 33, 283. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Gottrand, F.; Huybrechts, I.; Ruiz, J.R.; González-Gross, M.; DeHenauw, S. Nutrition and lifestyle in european adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Adv. Nutr. 2014, 5, 615s–623s. [Google Scholar] [CrossRef] [PubMed]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Keiranchish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2006, 1, 40–43. [Google Scholar] [CrossRef]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Gálvez-Fernández, P.; Saucedo Araújo, R.G.; Campos-Garzón, P.; Aranda-Balboa, M.J.; Molina Soberanes, D.; Segura Díaz, J.M.; Herrador Colmenero, M.; Huertas-Delgado, F.J.; Villa González, E.; Barranco Ruiz, Y.M. El desplazamiento activo al centro educativo e indicadores de salud asociados: Protocolo de evaluación del estudio PACO Pedalea y Anda al COlegio y su aplicación en educación secundaria. Retos 2021, 39, 649–657. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef]
- Lu, W.; McKyer, E.L.J.; Lee, C.; Goodson, P.; Ory, M.G.; Wang, S. Perceived barriers to children’s active commuting to school: A systematic review of empirical, methodological and theoretical evidence. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–20. [Google Scholar] [CrossRef]
- Mielgo-Ayuso, J.; Aparicio-Ugarriza, R.; Castillo, A.; Ruiz, E.; Ávila, J.M.; Aranceta-Batrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; et al. Physical Activity Patterns of the Spanish Population Are Mostly Determined by Sex and Age: Findings in the ANIBES Study. PLoS ONE 2016, 11, e0149969. [Google Scholar] [CrossRef]
- Uddin, R.; Mandic, S.; Khan, A. Active commuting to and from school among 106,605 adolescents in 27 Asia-Pacific countries. J. Transp. Health 2019, 15, 100637. [Google Scholar] [CrossRef]
- Potoglou, D.; Arslangulova, B. Factors influencing active travel to primary and secondary schools in Wales. Transp. Plan Technol. 2017, 40, 80–99. [Google Scholar] [CrossRef]
- Kek, C.C.; Bengoechea, E.G.; Spence, J.C.; Mandic, S. The relationship between transport-to-school habits and physical activity in a sample of New Zealand adolescents. J. Sport Health Sci. 2019, 8, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Campos-Sánchez, F.S.; Abarca-Álvarez, F.J.; Molina-García, J.; Chillón, P. A GIS-Based Method for Analysing the Association Between School-Built Environment and Home-School Route Measures with Active Commuting to School in Urban Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 2295. [Google Scholar] [CrossRef]
- D’Haese, S.; De Meester, F.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. Criterion distances and environmental correlates of active commuting to school in children. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 88. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, C.; Salas-Fariña, Z.M.; Villa-González, E.; Borges-Cosic, M.; Herrador-Colmenero, M.; Medina-Casaubón, J.; Ortega, F.B.; Chillón, P. The Threshold Distance Associated With Walking From Home to School. Health Educ. Behav. 2017, 44, 857–866. [Google Scholar] [CrossRef]
- Gutiérrez-Zornoza, M.; Sánchez-López, M.; García-Hermoso, A.; González-García, A.; Chillón, P.; Martínez-Vizcaíno, V. Active commuting to school, weight status, and cardiometabolic risk in children from rural areas: The Cuenca study. Health Educ. Behav. 2015, 42, 231–239. [Google Scholar] [CrossRef]
- Khan, A.; Mandic, S.; Uddin, R. Association of active school commuting with physical activity and sedentary behaviour among adolescents: A global perspective from 80 countries. J. Sci. Med. Sport 2021, 24, 567–572. [Google Scholar] [CrossRef]
- Pereira, E.F.; Moreno, C.; Louzada, F.M. Increased commuting to school time reduces sleep duration in adolescents. Chronobiol. Int. 2014, 31, 87–94. [Google Scholar] [CrossRef]
- Santomauro, F.; Lorini, C.; Tanini, T.; Indiani, L.; Lastrucci, V.; Comodo, N.; Bonaccorsi, G. Adherence to Mediterranean diet in a sample of Tuscan adolescents. Nutrition 2014, 30, 1379–1383. [Google Scholar] [CrossRef]


{kind=link}
| Variable | % (n) | Mean (SD) |
|---|---|---|
| Age (years old) | 14.9 (0.48) | |
| City | ||
| Toledo | 34.2 (103) | |
| Sevilla | 17.6 (53) | |
| Granada | 27.2 (82) | |
| Valencia | 20.9 (63) | |
| Girls | 50.2 (151) | |
| Distance to school (meters) | 1275 (901.42) | |
| Media sleep hours (hours) | 7.9 (1.04) | |
| Meet sleep recommendations ≥ 8 h | 56 (17.2) | |
| KIDMED (mean points) | 6.3 (2.65) | |
| Breakfast every day | 67.8 (204) | |
| ACS | 64.5 (194) | |
| Usual mode of commuting to and from school | ||
| Walk | 63.5 (191) | |
| Car | 29.6 (89) | |
| Scholar bus | 3.0 (9) | |
| Public bus | 2.3 (7) | |
| Bike | 0.7 (2) | |
| Underground | 0.7 (2) | |
| Scooter | 0.3 (1) |
| Media Use | ACS | Screen Time Per Day | 2 | Mann Whitney–U | |||||
|---|---|---|---|---|---|---|---|---|---|
| None | Less than 30 min | Between 30–60 min | Between 1–2 h | Between 2–3 h | More than 3 h | p Value | p Value | ||
| TV viewing | Non-ACS | 9.4 (10) | 29.2 (31) | 25.5 (27) | 17.9 (19) | 9.4 (10) | 8.5 (9) | 0.35 | 0.83 |
| ACS | 16.0 (31) | 23.7 (46) | 18.6 (36) | 18.0 (35) | 12.9 (25) | 10.8 (21) | |||
| Missing = 1 | |||||||||
| Videogames | Non-ACS | 43.0 (46) | 20.6 (22) | 15.0 (16) | 10.3 (11) | 5.6 (6) | 5.6 (6) | 0.34 | 0.96 |
| ACS | 47.9 (92) | 12.5 (24) | 10.9 (21) | 15.1 (29) | 6.3 (12) | 7.3 (14) | |||
| Missing = 2 | |||||||||
| Mobile pone | Non-ACS | 0.9 (1) | 5.6 (6) | 15.9 (17) | 20.6 (22) | 19.6 (21) | 37.4 (40) | 0.69 | 0.85 |
| ACS | 1.0 (2) | 7.8 (15) | 9.8 (19) | 21.8 (42) | 23.3 (45) | 36.3 (70) | |||
| Missing = 1 | |||||||||
| Computer | Non-ACS | 12.3 (13) | 18.9 (20) | 17.9 (19) | 20.8 (22) | 13.2 (14) | 17.0 (18) | 0.97 | 0.85 |
| ACS | 14.5 (28) | 17.1 (33) | 16.6 (32) | 18.7 (36) | 13.5 (26) | 19.7 (38) | |||
| Missing = 2 | |||||||||
| Mode of Transport | Bivariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| Variable | Non Active n = 107 | Active n = 194 | OR 95% CI | aOR 95% CI | p-Value |
| Age (years) Mean (SD) | 14.89 (0.50) | 14.92 (0.47) | 1.16 (0.70, 1.92) | 1.58 (0.77, 3.24) | 0.21 |
| Gender | 0.02 | ||||
| Girls | 40.7 (61) | 59.3 (89) | 1 (Ref.) | 1 (Ref.) | |
| Boys | 30.5 (46) | 69.5 (105) | 1.56 (0.97, 2.52) | 2.28 (1.12, 4.64) * | |
| Distance from home to school (hectometres) | 20.21 (10.18) | 8.63 (4.63) | 0.77 (0.72, 0.82) ** | 0.74 (0.69, 0.80) ** | <0.001 |
| Sleep hours Mean (SD) | 8.04 (0.97) | 7.82 (1.07) | 0.81 (0.64, 1.02) | 0.51 (0.30, 0.89) * | 0.02 |
| Sleep recommendations | 0.04 | ||||
| <8 h | 36.3 (49) | 63.7 (86) | 1 | 1 | |
| ≥8 h | 34.9 (58) | 65.1 (108) | 1.06 (0.66, 1.71) | 3.05 (1.07, 8.69) * | |
| KIDMED punctuation Mean (SD) | 6.21 (2.45) | 6.33 (2.75)) | 1.02 (0.93, 1.11) | 1.16 (1.00, 1.33) * | 0.05 |
| Take breakfast every day | 0.04 | ||||
| No | 29.9 (29) | 70.1 (68) | 1 | 1 | |
| Yes | 38.2 (78) | 61.8 (194) | 0.69 (0.41, 1.16) | 0.41 (0.18, 0.96) * | |
| Screen variable composite (sum of punctuations) Mean (SD) | 13.6 (3.83) | 13.86 (4.21) | 1.01 (0.96, 1.07) | 0.97 (0.88, 1.06) | 0.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Moraleda, E.; Pinilla-Quintana, I.; Romero-Blanco, C.; Hernández-Martínez, A.; Jiménez-Zazo, F.; Dorado-Suárez, A.; García-Coll, V.; Cabanillas-Cruz, E.; Martínez-Romero, M.T.; Herrador-Colmenero, M.; et al. Lifestyle Behaviours Profile of Spanish Adolescents Who Actively Commute to School. Children 2023, 10, 95. https://doi.org/10.3390/children10010095
Martín-Moraleda E, Pinilla-Quintana I, Romero-Blanco C, Hernández-Martínez A, Jiménez-Zazo F, Dorado-Suárez A, García-Coll V, Cabanillas-Cruz E, Martínez-Romero MT, Herrador-Colmenero M, et al. Lifestyle Behaviours Profile of Spanish Adolescents Who Actively Commute to School. Children. 2023; 10(1):95. https://doi.org/10.3390/children10010095
Chicago/Turabian StyleMartín-Moraleda, Evelyn, Iván Pinilla-Quintana, Cristina Romero-Blanco, Antonio Hernández-Martínez, Fabio Jiménez-Zazo, Alberto Dorado-Suárez, Virginia García-Coll, Esther Cabanillas-Cruz, Maria Teresa Martínez-Romero, Manuel Herrador-Colmenero, and et al. 2023. "Lifestyle Behaviours Profile of Spanish Adolescents Who Actively Commute to School" Children 10, no. 1: 95. https://doi.org/10.3390/children10010095
APA StyleMartín-Moraleda, E., Pinilla-Quintana, I., Romero-Blanco, C., Hernández-Martínez, A., Jiménez-Zazo, F., Dorado-Suárez, A., García-Coll, V., Cabanillas-Cruz, E., Martínez-Romero, M. T., Herrador-Colmenero, M., Queralt, A., Castro-Lemus, N., & Aznar, S. (2023). Lifestyle Behaviours Profile of Spanish Adolescents Who Actively Commute to School. Children, 10(1), 95. https://doi.org/10.3390/children10010095