1. Introduction
Human skin color is mainly determined by the content and distribution of various pigment substances, such as melanin, hemoglobin, and carotenoids [
1]. Genetic factors primarily determine skin color, but it is also strongly influenced by acquired factors. Melanin is produced through a process in which an amino acid called L-tyrosine is metabolized in a series of enzymatic reactions in melanosomes, which are organelles of melanocytes. There are different types of melanin, such as eumelanin and pheomelanin, which impart different colors [
2]. Melanosomes supply melanin to surrounding keratinocytes and, as a result, melanin is distributed throughout the skin and expressed to produce various skin color [
3]. In addition to its effects on visual appearance of the skin, melanin plays an important role in protecting the body from the toxicity of ultraviolet (UV) rays [
4]. Therefore, the metabolism of melanin in skin has become an important research topic from both a physiological and aesthetic perspective [
5,
6].
Abnormal melanin metabolism can cause various types of skin pigment diseases, which are divided into hyperpigmentation and hypopigmentation [
7,
8]. Hyperpigmentation occurs when melanin is excessively or unevenly accumulated due to inflammation, aging, UV rays, physical damage, and other internal/external stimulatory factors [
9,
10]. Meanwhile, genetic or epigenetic defects in melanin production can result in hypopigmentation, such as in albinism or vitiligo [
11,
12].
Prevention and treatment strategies for hyperpigmentation include photoprotection, pharmacotherapy, surgical treatment (chemical peeling and laser treatment), and cosmetic camouflage [
13,
14,
15]. Chemical peeling and laser treatment are frequently performed, but they have side effects, such as dermatitis and recurring pigmentation [
16,
17]. Hydroquinone is primarily used as a pharmacotherapeutic, but it can potentially cause skin irritation, allergies, mutations, and cancer [
18]. In the cosmetics field, skin lightening functional cosmetics containing arbutin, niacinamide, and vitamin C derivatives dominate, but the satisfaction of consumers regarding their safety and skin lightening efficacy is low [
19]. This research team has searched for skin lightening agents from various natural sources and identified numerous natural compounds, such as p-coumaric acid, resveratrol, and luteolin 7-sulfate, which inhibit cellular melanin synthesis though various mechanisms [
20,
21,
22,
23].
Peptides are being increasingly used as active ingredients in dermatology and skincare products [
24,
25]. The smaller the peptide, the less expensive it is to manufacture, the higher its stability, and the more easily it is absorbed by the skin.
Our recent studies identified certain low molecular anti-melanogenic peptides [
26,
27]. In these studies, a special algorithm was used to predict the sequences of active peptides using a positional scanning synthetic peptide combination library [
28,
29]. Using this method, it was possible to identify anti-melanogenic peptides by evaluating the activity of 80 tetra-peptide pools instead of evaluating the activity of all 160,000 possible types of tetra-peptides [
27]. The anti-melanogenic activity of the peptides was preliminarily evaluated in B16-F10 melanoma cells treated with α-melanocyte-stimulating hormone (MSH). The sequence of the active tetra-peptide was predicted to be R-(F/L)-(C/W)-(G/R)-NH
2. Of the individual tetra-peptides tested, RFWG-NH
2 and RLWG-NH
2 showed high anti-melanogenic activity. The tetra-peptide FRWG-NH
2, which has the same sequence as a part of α-MSH (acetyl-SYSMEHFRWGKPV-NH
2), also showed similar activity. Among the tri-peptides tested, FWG-NH
2, LWG-NH
2, and RWG-NH
2 were relatively active. The di-peptide WG-NH
2 and the G-NH
2 (glycinamide) retained their anti-melanogenic activity, while neither acety-G-NH
2 nor G (glycine) was active. These low molecular anti-melanogenic peptides are thought to target the melanocortin 1 receptor (MC1R), because they have a sequence similar to that of α-MSH. These low molecular anti-melanogenic peptides may be very useful in the study of the MC1R-dependent physiological functions of melanocytes [
30].
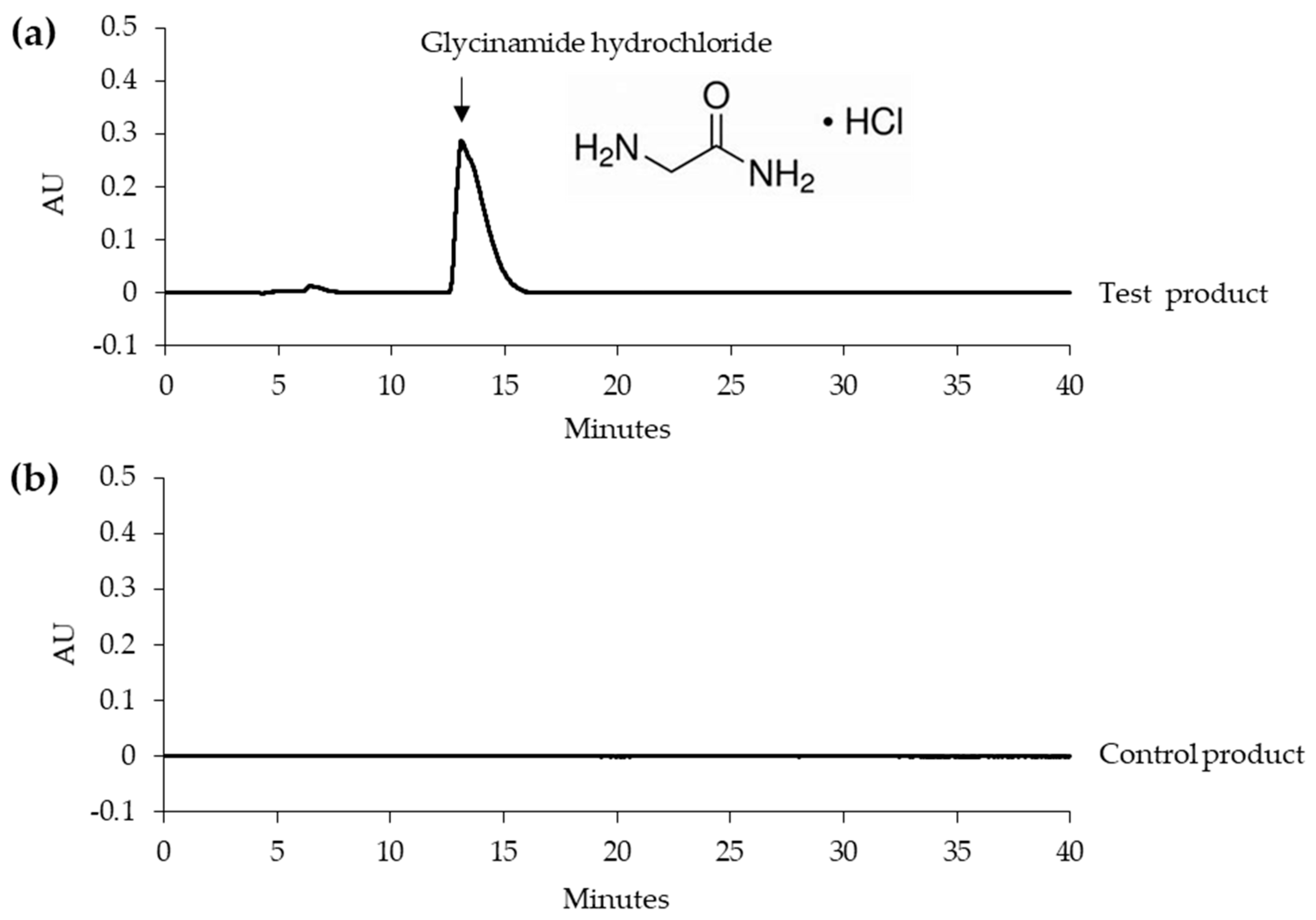
Glycinamide was shown to inhibit cellular melanin production very effectively by reducing the activation of cAMP-responsive element-binding protein (CREB) and the gene expression of microphthalmia-associated transcription factor (MITF), and tyrosinase (TYR) in response to α-MSH [
27]. In the present study, we report the results of the first human skin application test of glycinamide (in the form of hydrochloride salt), which is the smallest of the low molecular anti-melanogenic peptides.
4. Discussion
This study is the first to report the safety and depigmentation efficacy of glycinamide hydrochloride applied to human facial skin. In the primary skin irritation test, a test product containing 10% glycinamide hydrochloride did not induce any adverse reactions in 30 human subjects. In the double-blinded efficacy test, the test product and control product were used on the left and right sides, respectively, of the face in 21 subjects, randomly assigned to different groups. During the eight week-long test period, the skin sites at which the test product was applied became lighter than the sites at which the control product was applied. Both visual assessment of the degree of pigmentation, and instrumental evaluation of melanin index, skin lightness, and skin color supported the depigmentation efficacy of the test product containing glycinamide hydrochloride.
The human skin depigmentation efficacy of a product can be evaluated while using artificial tanning and natural hyperpigmentation models [
34,
35,
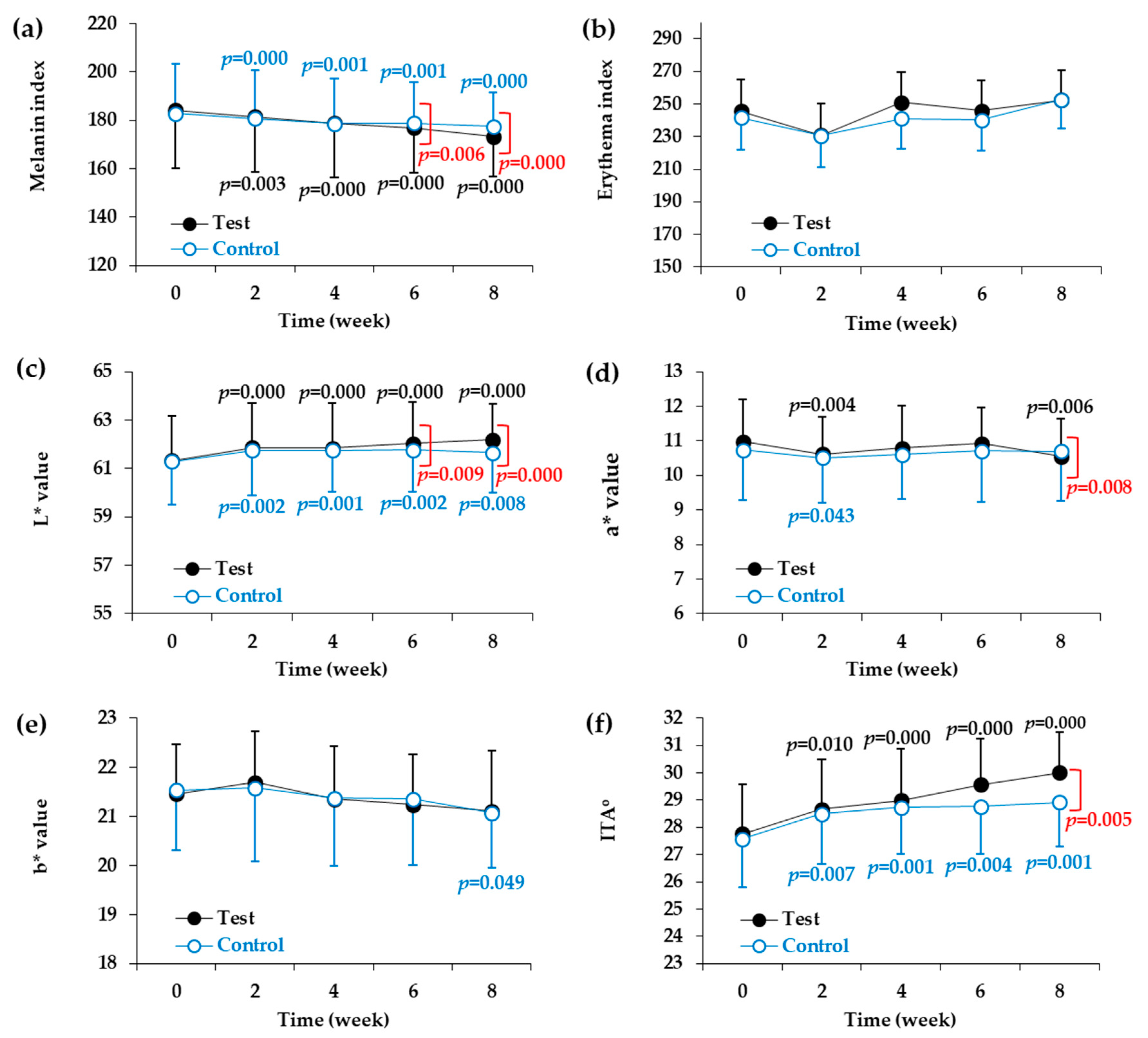
36]. In the present study, using a natural pigmentation model, changes in skin color parameters in the test and control groups over the eight weeks of test were tracked at two week intervals. The control product, which did not contain glycinamide hydrochloride, also produced significant changes in melanin index, L* value, and ITA
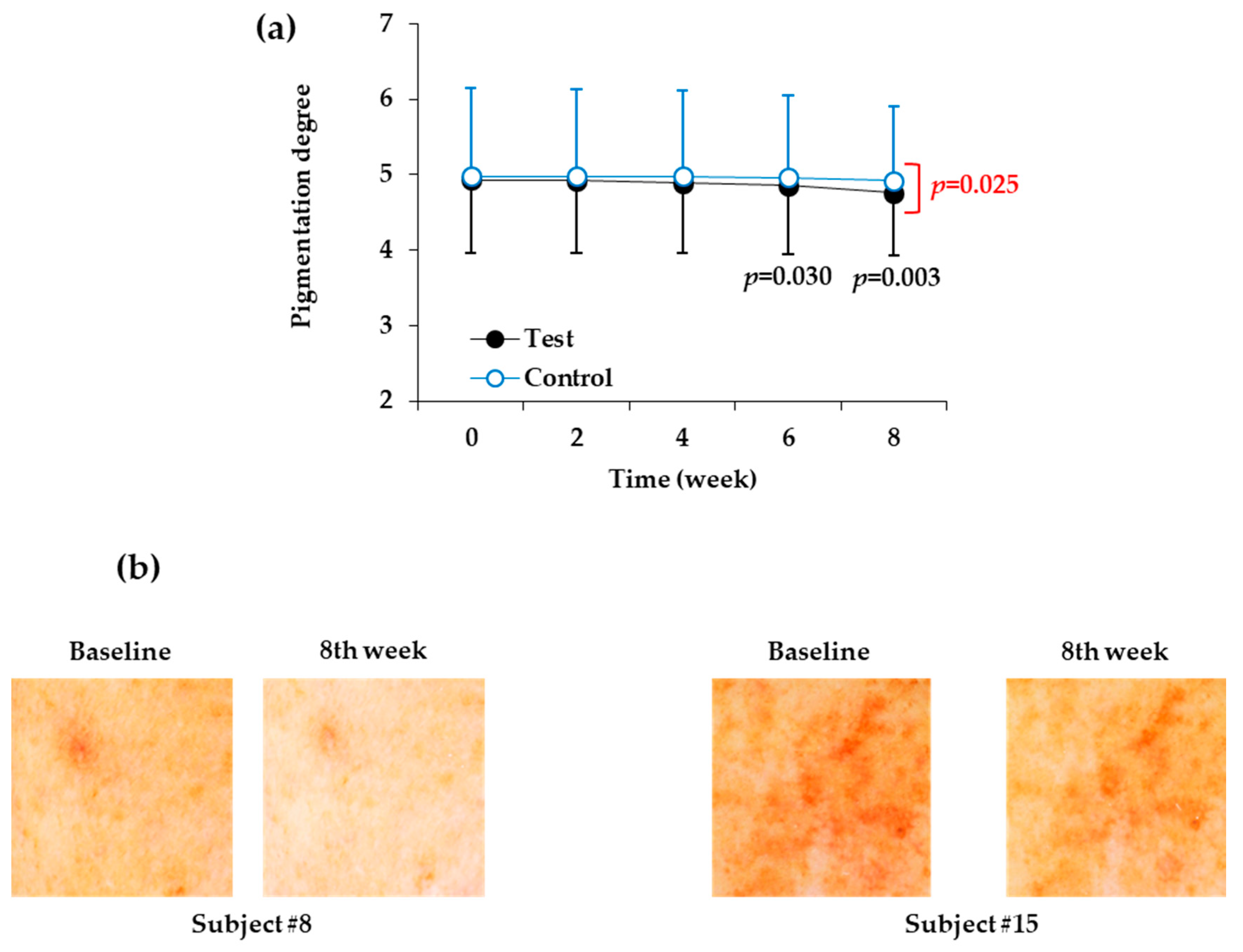
o from two weeks after the start of the test. The exact cause of this is currently unclear and several factors might have contributed to the changes. The ingredients contained in the control product, such as glycerin and 1,2-hexanediol, might have altered skin surface condition, improving cleanness, luster, and brightness. Nonetheless, additional changes in the parameters mentioned above after two weeks were not significant in the control group. In addition, the degree of pigmentation (evaluated visually) was not significantly reduced by the control product when compared to before the start of the test. Therefore, it is considered that the control product has a very weak skin lightening effect if any.
In the case of the test product, in addition to a significant change in the melanin index, L* value, and ITAo at two weeks after the start of the test, the change tended to increase gradually thereafter. Furthermore, the degree of pigmentation reached a significantly lower level than the baseline value. This suggests that use of the test product can improve skin color when compared to use of no product.
From the sixth week of the start of the test, there was a significant difference in the melanin index and L* value between the test group and the control group and, at eight weeks, there was also a difference in ITAo and the degree of pigmentation. These results support the conclusion that the difference in efficacy between the test and control products was due to the presence or absence of glycinamide hydrochloride; therefore, the skin depigmentation efficacy of the test product was due to its main component, glycinamide hydrochloride.
In this study, glycinamide hydrochloride solution soaked into non-woven fabric sheets was applied to the face, and positive results were obtained regarding its skin depigmentation efficacy. This application method turned out to be effective, but it is worth investigating whether changing the formulation and application method would improve the efficacy of the product. In addition to topical application onto skin, oral administration and injection methods need to be examined in order to determine their clinical efficacy in future studies.
Statistical analysis for the differences between the test and control groups was conducted using the Repeated Measures ANOVA with paired comparisons. Additionally, the inter-group differences of melanin index, L* value, ITA
o, and pigmentation degree were all statistically significant after 8-week treatments. In the current study, the melanin index reduction rates by the test product containing 10% glycinamide hydrochloride was 5.88% (baseline, 184.03 ± 22.70; eighth week, 173.30 ± 20.79). Watanabe et al. reported skin-whitening effects of topical oxidized glutathione in a double-blind and placebo-controlled clinical trial in thirty healthy women [
36]. Topical treatments of a test product containing 2% oxidized glutathione for 10 weeks reduced melanin index by 10.7% (baseline, 272.77 ± 26.17; 10th week, 243.47 ± 26.31) [
36]. Even though the test conditions, such as baseline melanin index, test dose, and duration of test, are different each other, the indirect comparison of these two studies suggest that glycinamide hydrochloride has potential to be used as a hypopigmenting agent. Further studies are needed to optimize its dose, formulation, and application method to achieve better performance in skin depigmentation.
The steady state skin color reflects the relative ratio of the amount of melanin supplied from melanocytes to the amount of melanin lost due to desquamation of the skin’s keratin. Therefore, the inhibition of melanin synthesis or enhancement of melanin loss are two possible strategies for hyperpigmentation therapy. Glycinamide hydrochloride is a useful substance for the former strategy, because it can inhibit melanin synthesis by reducing the levels of TYR and other enzymes that are involved in melanin synthesis in melanocytes [
27]. If so, combining glycinamide hydrochloride with skin peeling agents, such as glycolic acid [
37,
38], may result in further increases in depigmentation efficacy due to synergism between substances with different mechanisms of action.
Many existing depigmentation agents reduce the synthesis of melanin by inhibiting the intracellular signal transduction process responsible for TYR gene expression or inhibiting the activity of TYR directly [
39,
40]. However, glycinamide hydrochloride can prevent the binding of a hormone to its receptors and block the initiation of intracellular signal transduction processes, thereby inhibiting the expression of TYR [
27]. Accordingly, glycinamide hydrochloride can act via a different mechanism from many existing depigmenting agents, and synergistic effects are expected if it is used in combination with other depigmenting agents.
Proopiomelanocortin-derived peptide hormones, such as α-MSH, β-MSH, and adrenocorticotrophic hormone (ACTH), regulate skin pigmentation, inflammation and fibrosis [
8,
30,
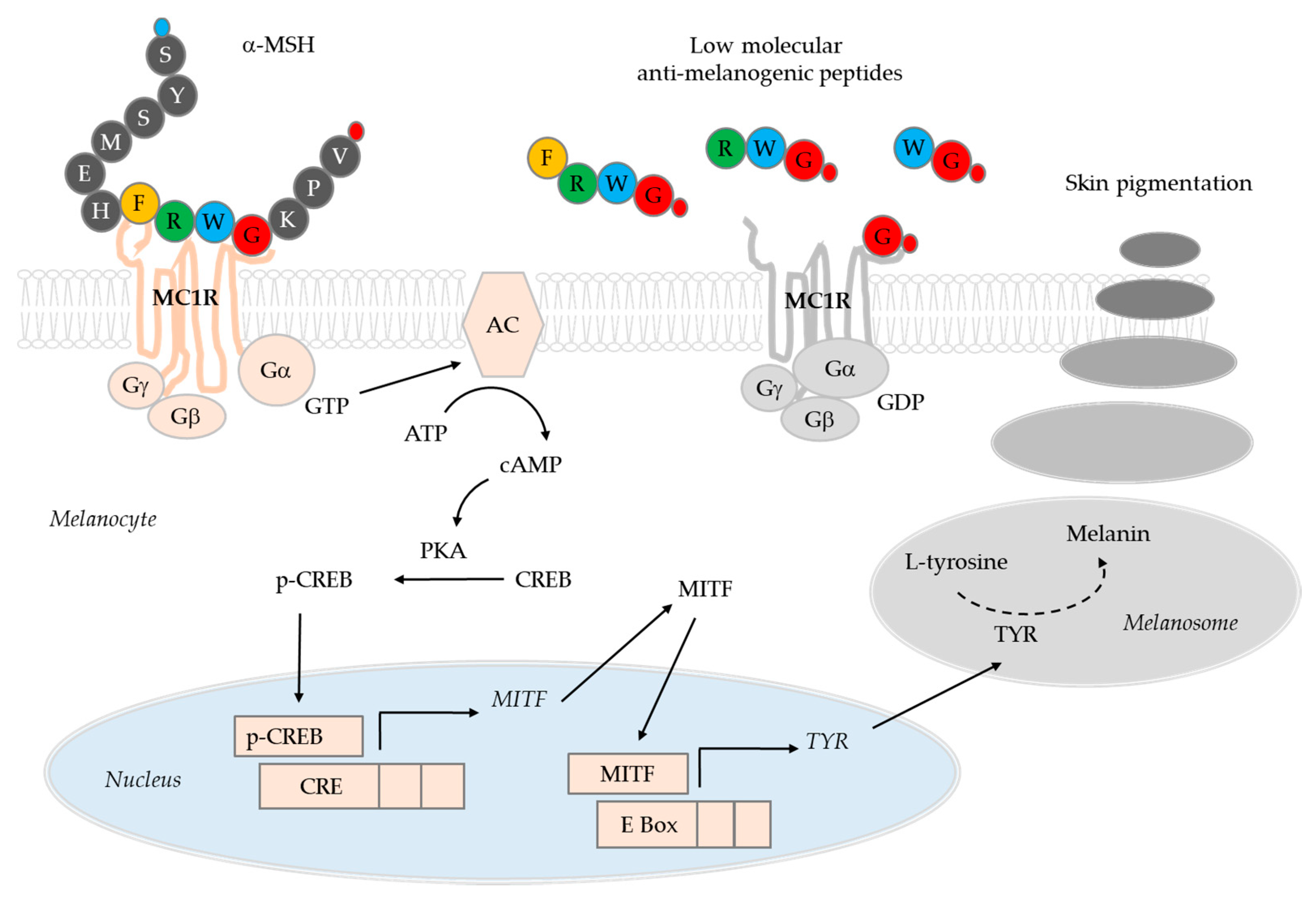
41]. On the binding of these agonists to MC1R and the consecutive activations of adenylate cyclase (AC) and protein kinase A (PKA) phosphorylates CREB transcription factor, which, in turn, induces MITF expression [
42]. MITF expression is also induced by other signaling pathways that involve Wnt/Frizzled/glycogen synthase kinase 3β/β-catenin cascade, and stem cell factor/c-Kit/mitogen-activated protein kinases cascade [
43,
44]. MITF directs not only gene expression of melanogenic enzymes, but also the biogenesis of melanosomes [
2,
45].
The low molecular anti-melanogenic peptides identified in the previous study include FRWG-NH
2, RWG-NH
2, WG-NH
2, and G-NH
2 (glycinamide), which share common sequences with α-MSH (acetyl-SYSMEHFRWGKPV-NH
2) [
27]. It was hypothesized that these low molecular anti-melanogenic peptides might interfere with the receptor binding of α-MSH in a competitive manner thereby blocking the initiation of intracellular signal transduction processes (
Figure 4). If the low molecular anti-melanogenic peptides act as MC1R antagonists, they may inhibit the activation of MC1R by other agonists, such as β-MSH and ACTH as well, and affect other physiological evets associate with inflammation and fibrosis as well as pigmentation [
30].
Although more direct evidence is needed for the mechanism of action, the present study demonstrates that the hydrochloride salt form of glycinamide, the smallest essential moiety of the anti-melanogenic peptides, exhibited skin depigmentation efficacy without causing skin irritation in humans. Further studies are needed in order to examine the depigmentation efficacy of the other anti-melanogenic tetra-peptides, tri-peptides, and a di-peptide mentioned above.
In conclusion, the present study suggests that glycinamide hydrochloride has great potential to be used in the control of skin hyperpigmentation.








{kind=link}
{kind=link}
{kind=link}
{kind=link}