
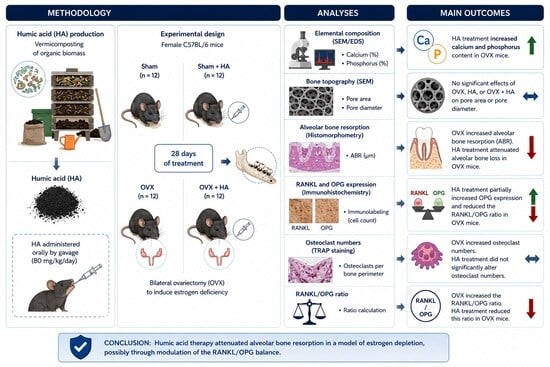
Humic Acid Therapy Mitigates Estrogen Deficiency-Induced Alveolar Bone Loss and Modulates the RANKL/OPG Balance

 , , , , , ,
, , , , , ,  , , , and
, , , and
Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Composting, Vermicomposting, Extraction, and Characterization of Humic Acids (HAs)
2.2. Animals
2.3. Experimental Design
2.4. Protocol for Sham Surgery and Ovariectomy (OVX)
2.5. Supplementation with Humic Acids (HAs)
2.6. Analysis of the Elemental Composition and Topography of the Mandibular Bone Using Scanning Electron Microscopy Coupled with Energy-Dispersive X-Ray Spectroscopy (SEM/EDS)
2.7. Quantitative Histomorphometric Assessment of Alveolar Bone Loss
2.8. Immunohistochemical Analysis of RANKL and OPG Expression in the Alveolar Bone
2.9. Tartrate-Resistant Acid Phosphatase (TRAP) Staining for Osteoclast Quantification in Alveolar Bone
2.10. Statistical Analyses
3. Results
3.1. Confirmation of Estrogen Deficiency Following Ovariectomy
3.2. Elemental Composition and Topography of Mandibular Alveolar Bone Assessed by SEM/EDS
3.3. Alveolar Bone Resorption (ABR) Assessed by Histomorphometry
3.4. Immunolabeling of Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL) and Osteoprotegerin (OPG)
3.5. Assessment of Osteoclasts by Tartrate-Resistant Acid Phosphatase (TRAP) Staining
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, C.H.; Chen, L.R.; Chen, K.H. Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover. Int. J. Mol. Sci. 2022, 23, 1376. [Google Scholar] [CrossRef]
- Ikebuchi, Y.; Aoki, S.; Honma, M.; Hayashi, M.; Sugamori, Y.; Khan, M.; Kariya, Y.; Kato, G.; Tabata, Y.; Penninger, J.M.; et al. Coupling of Bone Resorption and Formation by RANKL Reverse Signalling. Nature 2018, 561, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liang, J.; Liu, P.; Wang, Q.; Liu, L.; Zhao, H. The RANK/RANKL/OPG System and Tumor Bone Metastasis: Potential Mechanisms and Therapeutic Strategies. Front. Endocrinol. 2022, 13, 1063815. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Wang, J.; Yang, Y.; He, Y.; Li, L. The Interplay of Estrogen, Gut Microbiome, and Bone Immunity in Osteoporosis. Cell Commun. Signal. 2025, 23, 516. [Google Scholar] [CrossRef]
- Lee, K.I.-R.; Chen, J.-H.; Chen, K.-H. Osteoporosis After Menopause and After Drug Therapy: The Molecular Mechanism of Bone Loss and Its Treatment. Int. J. Mol. Sci. 2026, 27, 641. [Google Scholar] [CrossRef]
- Liang, H.; Chen, S.; Shi, M.; Xu, J.; Zhao, C.; Yang, B.; Zheng, S.; Tan, J. Global Epidemiology and Burden of Osteoporosis among Postmenopausal Women: Insights from the Global Burden of Disease Study 2021. npj Aging 2025, 11, 78. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.T.; Van Thai, C.; Hong, N.N.T.; Huu, T.D.; Elsheikh, R.; Alagbo, H.O.; Makram, A.M.; Huy, N.T. Clinical Manifestations and Quality of Life of Postmenopausal Women with Severe Osteoporosis: A Cross-Sectional Study on the Vietnamese Population. BMC Women’s Health 2025, 25, 509. [Google Scholar] [CrossRef]
- Bandela, V.; Munagapati, B.; Reddy Karnati, R.K.; Venkata, G.R.S.; Nidudhur, S.R. Osteoporosis: Its Prosthodontic Considerations—A Review. J. Clin. Diagn. Res. 2015, 9, ZE04. [Google Scholar] [CrossRef]
- Thompson, D.M.; Lee, H.M.; Stoner, J.A.; Golub, L.M.; Nummikoski, P.V.; Payne, J.B. Loss of Alveolar Bone Density in Post-Menopausal, Osteopenic Women Is Associated with Circulating Levels of Gelatinases. J. Periodontal Res. 2019, 54, 532. [Google Scholar] [CrossRef]
- Jayusman, P.A.; Nasruddin, N.S.; Baharin, B.; Ibrahim, N.I.; Ahmad Hairi, H.; Shuid, A.N. Overview on Postmenopausal Osteoporosis and Periodontitis: The Therapeutic Potential of Phytoestrogens against Alveolar Bone Loss. Front. Pharmacol. 2023, 14, 1120457. [Google Scholar] [CrossRef]
- Tsuchida, S.; Nakayama, T. Recent Clinical Treatment and Basic Research on the Alveolar Bone. Biomedicines 2023, 11, 843. [Google Scholar] [CrossRef]
- Ruivo, A.K.; Calsa, B.; Cancellara, M.G.; Lima, J.P.N.; da Silva, K.R.; Esquisatto, M.A.M.; Santamaria, M., Jr. Effect of Estrogen Depression on Alveolar Bone Microarchitecture and Periodontal Ligament Cells during Orthodontic Movement. Eur. J. Oral Sci. 2024, 132, e13014. [Google Scholar] [CrossRef]
- Schroeder, R.J.; Staszkiewicz, J.; O’Quin, C.; Carroll, B.; Doan, N.; Patel, S.; Ahmadzadeh, S.; Kallurkar, A.; Viswanath, O.; Varrassi, G.; et al. Oral Therapeutics Post Menopausal Osteoporosis. Cureus 2023, 15, e42870. [Google Scholar] [CrossRef] [PubMed]
- Oka, P.; Moosa, A.S.; Koh, E.Y.L.; Ng, C.J. Health and Adverse Events Associated with Extended Oral Bisphosphonates among Postmenopausal Women: A Systematic Review. J. Clin. Endocrinol. Metab. 2026, 111, e1226–e1238. [Google Scholar] [CrossRef]
- Liu, B.; Mao, X.; Gao, Z.J.Y.; Wang, H. Natural Traditional Chinese Medicine Products: Emerging Therapeutic Targets for the Treatment of Osteoporosis. J. Orthop. Surg. Res. 2025, 20, 469. [Google Scholar] [CrossRef]
- Gvozdeva, Y.; Peneva, P.; Katsarov, P.; Gvozdeva, Y.; Peneva, P.; Katsarov, P. Biomedical Applications of Humic Substances: From Natural Biopolymers to Therapeutic Agents. Antioxidants 2025, 14, 1139. [Google Scholar] [CrossRef] [PubMed]
- Nabi, F.; Sarfaraz, A.; Kama, R.; Kanwal, R.; Li, H. Structure-Based Function of Humic Acid in Abiotic Stress Alleviation in Plants: A Review. Plants 2025, 14, 1916. [Google Scholar] [CrossRef] [PubMed]
- Zykova, M.V.; Trofimova, E.S.; Azarkina, L.A.; Lasukova, T.V.; Mihalyov, D.A.; Drygunova, L.A.; Danilets, M.G.; Ligacheva, A.A.; Tsupko, A.V.; Bashirov, S.R.; et al. Pharmacological Effects of Humic Substances and Their Signaling Mechanisms. Molecules 2025, 31, 114. [Google Scholar] [CrossRef]
- Maffia, A.; Oliva, M.; Marra, F.; Mallamaci, C.; Nardi, S.; Muscolo, A. Humic Substances: Bridging Ecology and Agriculture for a Greener Future. Agronomy 2025, 15, 410. [Google Scholar] [CrossRef]
- Tavares, H.G.; Orlando, P.R.; de Souza Pereira, R.R.; Magalhães, C.O.D.e.; Silva, G.; dos Santos Nunes Ferreira, A.; Garcia, B.C.C.; Lima, K.R.; Vieira, E.R.; Dobbss, L.B.; et al. Humic Acid from Vermicompost Effectively Regulates the Redox Status and Mitigates the Progression of Experimental Periodontitis. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2025, 398, 8345–8358. [Google Scholar] [CrossRef]
- Santos, T.C.d.; Silva, H.P.; Lima, K.R.; Salvador, M.L.N.; Cândido, G.d.S.; Pimenta, L.C.J.P.; Bertolini, N.O.; Ribeiro, L.B.; Fagundes, F.G.; Orlando, D.R.; et al. Humic Acid Derived from Vermicompost Improves Bone Mineral Content and Alters Oxidative Stress Markers in Ovariectomized Mice. Biomedicines 2025, 13, 495. [Google Scholar] [CrossRef]
- Lima, K.R.; Tavares, H.G.; Pereira, R.R.d.S.; Carvalho, J.d.C.L.; Botelho, R.d.O.; Spuri, A.C.R.; Dobbss, L.B.; Machado, A.R.T.; Orlando, D.R.; Remédio, R.N.; et al. Humic Acid Derived from Vermicompost Inhibits Alveolar Bone Degradation and Protects Against Renal Injury in an Experimental Model of Periodontitis. Biomedicines 2024, 12, 2710. [Google Scholar] [CrossRef] [PubMed]
- Orlando, P.R.; Tavares, H.G.; Pereira, R.R.d.S.; Silva, G.; Carvalho, J.d.C.L.; Machado, A.R.T.; Dobbs, L.B.; Dias-Peixoto, M.F.; Pereira, L.J.; Andrade, E.F. Humic Acid Derived from Agricultural Biomass Mitigates Alveolar Bone Loss and Modulates Systemic Inflammatory Cytokines in Rats with Periodontitis. Curr. Top. Med. Chem. 2024, 25, 645–656. [Google Scholar] [CrossRef]
- Pereira, R.R.d.S.; Castro, G.B.d.; Magalhães, C.O.D.e.; Costa, K.B.; Garcia, B.C.C.; Silva, G.; Carvalho, J.d.C.L.; Machado, A.R.T.; Vieira, E.R.; Cassilhas, R.C.; et al. High-Intensity Interval Training Mitigates the Progression of Periodontitis and Improves Behavioural Aspects in Rats. J. Clin. Periodontol. 2024, 51, 1222–1235. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.R.d.S.; Magalhães, C.O.D.e.; Miguel, E.L.M.; Toledo, L.V.; Orlando, D.R.; Machado, A.R.T.; Borges, B.D.B.; Pereira, L.J.; Dias-Peixoto, M.F.; Andrade, E.F. Alterations in Brain Metabolites in Rats with Experimental Periodontitis: A Metabolomic Approach. J. Periodontol. 2026. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kuntjoro, M.; Hendrijantini, N.; Rantam, F.A.; Hong, G.; Salim, S.; Ari, M.D.A. Osteoclast Activity in Osteoporosis Mandibular Bone Based on RANKL and Osteoprotegerin Ratio. J. Pharm. Pharmacogn. Res. 2021, 9, 870–877. [Google Scholar] [CrossRef]
- Justo, M.P.; Cardoso, C.d.B.M.; Cantiga-Silva, C.; de Oliveira, P.H.C.; Sivieri-Araújo, G.; Azuma, M.M.; Ervolino, E.; Cintra, L.T.A. Curcumin Reduces Inflammation in Rat Apical Periodontitis. Int. Endod. J. 2022, 55, 1241–1251. [Google Scholar] [CrossRef]
- Çalışır, M.; Akpınar, A.; Poyraz, Ö.; Göze, F.; Çınar, Z. The Histopathological and Morphometric Investigation of the Effects of Systemically Administered Humic Acid on Alveolar Bone Loss in Ligature-Induced Periodontitis in Rats. J. Periodontal Res. 2016, 51, 499–507. [Google Scholar] [CrossRef]
- Anggraeni, A.; Soetrisno, S.; Nurwati, I.; Budihastuti, U.R.; Pamungkasari, E.P.; Wasita, B.; Dirgahayu, P. Experimental Model of Menopausal Genitourinary Syndrome: Ovariectomy and Vaginectomy Protocols in Rats. Open Vet. J. 2025, 15, 3630. [Google Scholar] [CrossRef]
- Baek, D.C.; Kang, J.Y.; Lee, J.S.; Lee, E.J.; Son, C.G. Linking Alterations in Estrogen Receptor Expression to Memory Deficits and Depressive Behavior in an Ovariectomy Mouse Model. Sci. Rep. 2024, 14, 6854. [Google Scholar] [CrossRef]
- De Leon-Oliva, D.; Barrena-Blázquez, S.; Jiménez-Álvarez, L.; Fraile-Martinez, O.; García-Montero, C.; López-González, L.; Torres-Carranza, D.; García-Puente, L.M.; Carranza, S.T.; Álvarez-Mon, M.Á.; et al. The RANK–RANKL–OPG System: A Multifaceted Regulator of Homeostasis, Immunity, and Cancer. Medicina 2023, 59, 1752. [Google Scholar] [CrossRef]
- Ena, G.; Soyfoo, M. Postmenopausal Osteoporosis: From Molecular Pathways to Therapeutic Targets-A Mechanism-to-Practice Framework Integrating Pharmacotherapy, Fall Prevention, and Adherence into Patient-Centered Care. J. Clin. Med. 2025, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Ames, M.S.; Hong, S.; Lee, H.R.; Fields, H.W.; Johnston, W.M.; Kim, D.G. Estrogen Deficiency Increases Variability of Tissue Mineral Density of Alveolar Bone Surrounding Teeth. Arch. Oral Biol. 2010, 55, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Palanisamy, S. The Impact of Estrogen on Periodontal Tissue Integrity and Inflammation—A Mini Review. Front. Dent. Med. 2025, 6, 1455755. [Google Scholar] [CrossRef]
- Leung, K.C.M.; Chu, C.H. Dental Care for Older Adults. Int. J. Environ. Res. Public Health 2022, 20, 214. [Google Scholar] [CrossRef]
- Maspero, C.; Farronato, D.; Giannini, L.; Farronato, G. Orthodontic Treatment in Elderly Patients. Prog. Orthod. 2010, 11, 62–75. [Google Scholar] [CrossRef]
- Zhang, Y.; Yan, J.; Zhang, Y.; Liu, H.; Han, B.; Li, W. Age-Related Alveolar Bone Maladaptation in Adult Orthodontics: Finding New Ways Out. Int. J. Oral Sci. 2024, 16, 52. [Google Scholar] [CrossRef] [PubMed]
- Xin, P.; Liu, Q.; Zhang, K.; Zhang, C. Functional Groups as Functional Drivers: Structure–Activity Relationships in Humic Substances for Medical Applications. Environ. Geochem. Health 2025, 47, 564. [Google Scholar] [CrossRef]
- Ozkan, A.; Sen, H.M.; Sehitoglu, I.; Alacam, H.; Guven, M.; Aras, A.B.; Akman, T.; Silan, C.; Cosar, M.; Karaman, H.I.O. Neuroprotective Effect of Humic Acid on Focal Cerebral Ischemia Injury: An Experimental Study in Rats. Inflammation 2014, 38, 32–39. [Google Scholar] [CrossRef]
- Wang, X.; Liu, L.; Liang, D.; Chen, S.; Fan, W. Influence of Humic Acid on Oxidative Stress Induced by Arsenite and Arsenate Waterborne Exposure in Danio Rerio. Bull. Environ. Contam. Toxicol. 2021, 106, 786–791. [Google Scholar] [CrossRef]
- Móritz, A.V.; Farkas, O.; Jerzsele, Á.; Pézsa, N.P. Protective Effects of Humic Acid on Intestinal Barrier Dysfunction and Inflammatory Activation in Canine Cell-Based Models. Animals 2026, 16, 173. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Zhou, C.; Chen, S.; Huang, D.; Jiang, Y.; Lan, Y.; Zou, S.; Li, Y. Osteoporosis and Alveolar Bone Health in Periodontitis Niche: A Predisposing Factors-Centered Review. Cells 2022, 11, 3380. [Google Scholar] [CrossRef]
- Yu, B.; Wang, C.Y. Osteoporosis and Periodontal Diseases—An Update on Their Association and Mechanistic Links. Periodontology 2000 2022, 89, 99–113. [Google Scholar] [CrossRef]
- Marcucci, G.; Domazetovic, V.; Nediani, C.; Ruzzolini, J.; Favre, C.; Brandi, M.L. Oxidative Stress and Natural Antioxidants in Osteoporosis: Novel Preventive and Therapeutic Approaches. Antioxidants 2023, 12, 373. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xie, X.; Ding, C.; Zhang, S.; Hu, L.; Mi, B.; Liu, M.; Liu, G. Immunomodulatory Biomaterials for Bone and Soft Tissue Chronic Inflammation Diseases. Small Sci. 2025, 5, e202500260. [Google Scholar] [CrossRef] [PubMed]
- Poundarik, A.A.; Boskey, A.; Gundberg, C.; Vashishth, D. Biomolecular Regulation, Composition and Nanoarchitecture of Bone Mineral. Sci. Rep. 2018, 8, 1191. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Toledo, L.V.; Ribeiro, M.G.d.A.; Santos, T.C.d.; Salvador, M.L.N.; Bertolini, N.O.; Carvalho, J.d.C.L.; Orlando, D.R.; Remedio, R.N.; Machado, A.R.T.; Dobbss, L.B.; et al. Humic Acid Therapy Mitigates Estrogen Deficiency-Induced Alveolar Bone Loss and Modulates the RANKL/OPG Balance. Biomedicines 2026, 14, 1244. https://doi.org/10.3390/biomedicines14061244
Toledo LV, Ribeiro MGdA, Santos TCd, Salvador MLN, Bertolini NO, Carvalho JdCL, Orlando DR, Remedio RN, Machado ART, Dobbss LB, et al. Humic Acid Therapy Mitigates Estrogen Deficiency-Induced Alveolar Bone Loss and Modulates the RANKL/OPG Balance. Biomedicines. 2026; 14(6):1244. https://doi.org/10.3390/biomedicines14061244
Chicago/Turabian StyleToledo, Larissa Vieira, Maíra Gabrielle de Abreu Ribeiro, Thays Cristina dos Santos, Maria Luiza Nonato Salvador, Natália Oliveira Bertolini, Jaqueline do Carmo Lima Carvalho, Débora Ribeiro Orlando, Rafael Neodini Remedio, Alan Rodrigues Teixeira Machado, Leonardo Barros Dobbss, and et al. 2026. "Humic Acid Therapy Mitigates Estrogen Deficiency-Induced Alveolar Bone Loss and Modulates the RANKL/OPG Balance" Biomedicines 14, no. 6: 1244. https://doi.org/10.3390/biomedicines14061244
APA StyleToledo, L. V., Ribeiro, M. G. d. A., Santos, T. C. d., Salvador, M. L. N., Bertolini, N. O., Carvalho, J. d. C. L., Orlando, D. R., Remedio, R. N., Machado, A. R. T., Dobbss, L. B., Dourado, S. M. P., Pereira, L. J., & Andrade, E. F. (2026). Humic Acid Therapy Mitigates Estrogen Deficiency-Induced Alveolar Bone Loss and Modulates the RANKL/OPG Balance. Biomedicines, 14(6), 1244. https://doi.org/10.3390/biomedicines14061244