
A Potential Biomarker for Predicting Schizophrenia: Metallothionein-1


Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Taking Blood Samples from the Patients and Examining the Samples in the Laboratory
2.2.1. Metallothionein-1
2.2.2. Cu and Zn
2.3. Data Collection Tools
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schultz, S.H.; North, S.W.; Shields, C.G. Schizophrenia: A review. Am. Fam. Physician 2007, 75, 1821–1829. [Google Scholar] [PubMed]
- Walker, E.; Kestler, L.; Bollini, A.; Hochman, K.M. Schizophrenia: Etiology and course. Annu. Rev. Psychol. 2004, 55, 401–430. [Google Scholar] [CrossRef] [PubMed]
- Keefe, R.S.E.; Kahn, R.S. Cognitive Decline and Disrupted Cognitive Trajectory in Schizophrenia. JAMA Psychiatry 2017, 74, 535–536. [Google Scholar] [CrossRef]
- Haijma, S.V.; Haren, N.V.; Cahn, W.; Koolschijn, P.C.M.P.; Pol, H.E.H.; Kahn, R.S. Brain volumes in schizophrenia: A meta-analysis in over 18,000 subjects. Schizophr. Bull. 2013, 39, 1129–1138. [Google Scholar] [CrossRef]
- Kahn, R.S. On the Origins of Schizophrenia. Am. J. Psychiatry 2020, 177, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Hariri, A.G.; Özer, G.U.; Ceylan, M.E.; Ceylan, N.; Yazan, B.; Önal, O. Şizofreni Etyolojisinde Nörogelişimsel Hipotez [Neurodevelopmental Hypothesis in the Etiology of Schizophrenia]. Klin. Psikofarmakol. Bülteni 1999, 9, 99–103. (In Turkish) [Google Scholar]
- Yılmaz, S.; Öner, P. Could low α-N-acetylgalactosaminidase plasma concentration cause schizophrenia? World J. Biol. Psychiatry 2023, 24, 70–77. [Google Scholar] [CrossRef]
- Na, K.-S.; Jung, H.-Y.; Kim, Y.-K. The role of pro-inflammatory cytokines in the neuroinflammation and neurogenesis of schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 48, 277–286. [Google Scholar] [CrossRef]
- Siblerud, R.; Mutter, J. A Hypothesis and Additional Evidence that Mercury May be an Etiological Factor in Schizophrenia. Clin. Schizophr. Relat. Psychoses 2021, 15, 18–26. [Google Scholar]
- Mahadik, S.P.; Scheffer, R.E. Oxidative injury and potential use of antioxidants in schizophrenia. Prostaglandins Leukot. Essent. Fatty Acids 1996, 55, 45–54. [Google Scholar] [CrossRef]
- Juárez-Rebollar, D.; Rios, C.; Nava-Ruíz, C.; Méndez-Armenta, M. Metallothionein in Brain Disorders. Oxid. Med. Cell Longev. 2017, 2017, 5828056. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.K. Regulation of metallothionein gene expression by oxidative stress and metal ions. Biochem. Pharmacol. 2000, 59, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Coyle, P.; Philcox, J.C.; Carey, L.C.; Rofe, A.M. Metallothionein: The multipurpose protein. Cell. Mol. Life Sci. 2002, 59, 627–647. [Google Scholar] [CrossRef] [PubMed]
- Chiaverini, N.; De Ley, M. Protective effect of metallothionein on oxidative stress-induced DNA damage. Free Radic. Res. 2010, 44, 605–613. [Google Scholar] [CrossRef]
- Vidović, B.; Đorđević, B.; Milovanović, S.; Škrivanj, S.; Pavlović, Z.; Stefanović, A.; Kotur-Stevuljević, J. Selenium, zinc, and copper plasma levels in patients with schizophrenia: Relationship with metabolic risk factors. Biol. Trace Elem. Res. 2013, 156, 22–28. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Kostakoğlu, E.; Batur, S.; Tiryaki, A.; Göğüş, A. Pozitif ve Negatif Sendrom Ölçeğinin (PANSS) Türkçe Uygulamasının Geçerlik ve Güvenilirliği [Validity and Reliability of the Turkish Application of the Positive and Negative Syndrome Scale (PANSS)]. Türk Psikoloji Dergisi 1999, 14, 23–32. (In Turkish) [Google Scholar]
- Raffa, M.; Mechri, A.; Othman, L.B.; Fendri, C.; Gaha, L.; Kerkeni, A. Decreased glutathione levels and antioxidant enzyme activities in untreated and treated schizophrenic patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 1178–1183. [Google Scholar] [CrossRef]
- Dadheech, G.; Mishra, S.; Gautam, S.; Sharma, P. Evaluation of antioxidant deficit in schizophrenia. Indian J. Psychiatry 2008, 50, 16–20. [Google Scholar]
- Zhang, M.; Zhao, Z.; He, L.; Wan, C. A meta-analysis of oxidative stress markers in schizophrenia. Sci. China Life Sci. 2010, 53, 112–124. [Google Scholar] [CrossRef]
- Yao, J.K.; Leonard, S.; Reddy, R. Altered glutathione redox state in schizophrenia. Dis. Markers 2006, 22, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Keshavan, M.; Yao, J.K. Reduced plasma antioxidants in first-episode patients with schizophrenia. Schizophr. Res. 2003, 62, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Kondoh, M. Recent studies on metallothionein: Protection against toxicity of heavy metals and oxygen free radicals. Tohoku J. Exp. Med. 2002, 196, 9–22. [Google Scholar] [CrossRef]
- Kang, Y.J. Metallothionein redox cycle and function. Exp. Biol. Med. 2006, 231, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.V.; Hiramatsu, M.; Ebadi, M. Free radical scavenging actions of metallothionein isoforms I and II. Free Radic. Res. 1998, 29, 93–101. [Google Scholar] [CrossRef]
- Mahadik, S.P.; Mukherjee, S. Free radical pathology and antioxidant defense in schizophrenia: A review. Schizophr. Res. 1996, 19, 1–17. [Google Scholar] [CrossRef]
- Scuderi, C.; Stecca, C.; Iacomino, A.; Steardo, L. Role of astrocytes in major neurological disorders: The evidence and implications. IUBMB Life 2013, 65, 957–961. [Google Scholar] [CrossRef]
- Molinero, A.; Penkowa, M.; Hernández, J.; Camats, J.; Giralt, M.; Lago, N.; Carrasco, J.; Campbell, I.L.; Hidalgo, J. Metallothionein-I overexpression decreases brain pathology in transgenic mice with astrocyte-targeted expression of interleukin-6. J. Neuropathol. Exp. Neurol. 2003, 62, 315–328. [Google Scholar] [CrossRef]
- Ganguli, R.; Yang, Z.; Shurin, G.; Chengappa, K.; Brar, J.S.; Gubbi, A.V.; Rabin, B.S. Serum interleukin-6 concentration in schizophrenia: Elevation associated with duration of illness. Psychiatry Res. 1994, 51, 1–10. [Google Scholar] [CrossRef]
- Wang, C.; Gong, Z.; Hu, S.; Zhang, G. Metallothionein-1 is associated with osteoarthritis disease activity and suppresses proinflammatory cytokines production in synovial cells. Int. Immunopharmacol. 2019, 75, 105815. [Google Scholar] [CrossRef]
- Camacho-Abrego, I.; González-Cano, S.I.; Aguilar-Alonso, P.; Brambila, E.; de la Cruz, F.; Flores, G. Changes in nitric oxide, zinc and metallothionein levels in limbic regions at pre-pubertal and post-pubertal ages presented in an animal model of schizophrenia. J. Chem. Neuroanat. 2021, 111, 101889. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Elashoff, M.; Higgs, B.W.; Song, J.; Kim, S.; Sabunciyan, S.; Diglisic, S.; Yolken, R.H.; Knable, M.B.; Fuller, E.F.; et al. Putative psychosis genes in the prefrontal cortex: Combined analysis of gene expression microarrays. BMC Psychiatry 2008, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Yanik, M.; Kocyigit, A.; Tutkun, H.; Vural, H.; Herken, H. Plasma manganese, selenium, zinc, copper, and iron concentrations in patients with schizophrenia. Biol. Trace Elem. Res. 2004, 98, 109–117. [Google Scholar] [CrossRef]
- Joe, P.; Petrilli, M.; Malaspina, D.; Weissman, J. Zinc in schizophrenia: A meta-analysis. Gen. Hosp. Psychiatry 2018, 53, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, Y.; Li, X.; Ju, W.; Wu, G.; Yang, X. Association of Elements with Schizophrenia and Intervention of Selenium Supplements. Biol. Trace Elem. Res. 2018, 183, 16–21. [Google Scholar] [CrossRef]
- Gupta, S.K.; Singh, S.P.; Shukla, V.K. Copper, zinc, and Cu/Zn ratio in carcinoma of the gallbladder. J. Surg. Oncol. 2005, 91, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Durnam, D.M.; Palmiter, R.D. Transcriptional regulation of the mouse metallothionein-I gene by heavy metals. J. Biol. Chem. 1981, 256, 5712–5716. [Google Scholar] [CrossRef]
- Malavolta, M.; Cipriano, C.; Costarelli, L.; Giacconi, R.; Tesei, S.; Muti, E.; Piacenza, F.; Pierpaoli, S.; Larbi, A.; Pawelec, G.; et al. Metallothionein downregulation in very old age: A phenomenon associated with cellular senescence? Rejuvenation Res. 2008, 11, 455–459. [Google Scholar] [CrossRef]
- Billatos, E.; Faiz, A.; Gesthalter, Y.; Leclerc, A.; Alekseyev, Y.O.; Xiao, X.; Liu, G.; Hacken, N.H.T.; Heijink, I.H.; Timens, W.; et al. Impact of acute exposure to cigarette smoke on airway gene expression. Physiol. Genom. 2018, 50, 705–713. [Google Scholar] [CrossRef]
- Bitanihirwe, B.K.Y.; Woo, T.-U.W. Oxidative stress in schizophrenia: An integrated approach. Neurosci. Biobehav. Rev. 2011, 35, 878–893. [Google Scholar] [CrossRef]
- Hidalgo, J.; Aschner, M.; Zatta, P.; Vasák, M. Roles of the metallothionein family of proteins in the central nervous system. Brain Res. Bull. 2001, 55, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Demir, F.; Taşcı, B. An effective and robust approach based on R-CNN+ LSTM model and ncar feature selection for ophthalmological disease detection from fundus images. J. Pers. Med. 2021, 11, 1276. [Google Scholar] [CrossRef]
- Taşcı, B.; Acharya, M.R.; Barua, P.D.; Yildiz, A.M.; Gun, M.V.; Keles, T.; Dogan, S.; Tuncer, T. A new lateral geniculate nucleus pattern-based environmental sound classification using a new large sound dataset. Appl. Acoust. 2022, 196, 108897. [Google Scholar] [CrossRef]
- Macin, G.; Tasci, B.; Tasci, I.; Faust, O.; Barua, P.D.; Dogan, S.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. An accurate multiple sclerosis detection model based on exemplar multiple parameters local phase quantization: ExMPLPQ. Appl. Sci. 2022, 12, 4920. [Google Scholar] [CrossRef]
- Tasci, B.; Tasci, I. Deep feature extraction based brain image classification model using preprocessed images: PDRNet. Biomed. Signal Process. Control 2022, 78, 103948. [Google Scholar] [CrossRef]
- Dogan, S.; Baygin, M.; Tasci, B.; Loh, H.W.; Barua, P.D.; Tuncer, T.; Tan, R.-S.; Acharya, U.R. Primate brain pattern-based automated Alzheimer’s disease detection model using EEG signals. Cogn. Neurodynamics 2022, 1–13. [Google Scholar] [CrossRef]
- Tasci, G.; Loh, H.W.; Barua, P.D.; Baygin, M.; Tasci, B.; Dogan, S.; Tuncer, T.; Palmer, E.E.; Tan, R.-S.; Acharya, U.R. Automated accurate detection of depression using twin Pascal’s triangles lattice pattern with EEG Signals. Knowl.-Based Syst. 2023, 260, 110190. [Google Scholar] [CrossRef]
- Tasci, B. Automated ischemic acute infarction detection using pre-trained CNN models’ deep features. Biomed. Signal Process. Control 2023, 82, 104603. [Google Scholar] [CrossRef]
- Demir, F.; Akbulut, Y.; Taşcı, B.; Demir, K. Improving brain tumor classification performance with an effective approach based on new deep learning model named 3ACL from 3D MRI data. Biomed. Signal Process. Control 2023, 81, 104424. [Google Scholar] [CrossRef]
- Tasci, B.; Tasci, G.; Dogan, S.; Tuncer, T. A novel ternary pattern-based automatic psychiatric disorders classification using ECG signals. Cogn. Neurodynamics 2022, 1–14. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Schizophrenia (n = 52) | Control (n = 38) | x2 (p) | ||||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | |||
| Gender | Male | 42 | (80.8) | 31 | (81.6) | 0.009 (0.573) |
| Female | 10 | (19.2) | 7 | (18.4) | ||
| Marital Status | Married | 11 | (21.2) | 19 | (50) | 8.221 (0.004) |
| Single | 41 | (78.8) | 19 | (50) | ||
| Educational Status | Illiterate | 29 | (55.8) | 7 | (18.4) | 12.856 (0.005) |
| Primary School | 9 | (17.3) | 13 | (34.2) | ||
| Secondary School | 8 | (15.4) | 11 | (28.9) | ||
| University | 6 | (11.5) | 7 | (18.4) | ||
| Smoking | Present | 38 | (73.1) | 26 | (68.4) | 0.232 (0.401) |
| None | 14 | (26.9) | 12 | (31.6) | ||
| Antipsychotic Drugs Used | Olanzapine | 11 | (21.2) | - | - | - |
| Olanzapine + risperidone | 11 | (21.2) | - | - | ||
| Olanzapine + haloperidol | 10 | (19.2) | - | - | ||
| Risperidone | 10 | (19.2) | - | - | ||
| Olanzapine + quetiapine | 10 | (19.2) | - | - | ||
| Mean ± SD | Mean ± SD | t (p) | ||||
| Age | 36.135 ± 9.826 | 34.737 ± 9.246 | 0.683 (0.496) | |||
| BMI (kg/m2) | 26.211 ± 4.006 | 25.315 ± 3.595 | 1.093 (0.277) | |||
| Illness Duration (years) | 7.712 ± 5.932 | - | - | |||
| Groups | Schizophrenia (n = 52) | Control (n = 38) | t | sd | p | |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||||
| Metallothionein-1 (ng/mL) | 37.522 ± 17.408 | 68.652 ± 13.589 | −9.165 | 88 | <0.001 | |
| Cu (µg/dL) | 74.906 ± 13.887 | 88.934 ± 19.828 | −3.949 | 88 | <0.001 | |
| Zn (µg/dL) | 81.884 ± 12.330 | 82.244 ± 14.628 | −0.126 | 88 | 0.900 | |
| Cu/Zn | 0.938 ± 0.228 | 1.125 ± 0.356 | −3.030 | 88 | 0.003 | |
| PANSS total | 61.058 ± 11.187 | - | - | - | - | - |
| PANSS positive | 26.404 ± 10.628 | - | - | - | - | - |
| PANSS negative | 14.519 ± 4.327 | - | - | - | - | - |
| PANSS general psychopathology | 20.135 ± 2.635 | - | - | - | - | - |
| Groups | One Antipsychotic Drug Users (n = 21) | Two Antipsychotic Drugs Users (n = 31) | t | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Metallothionein-1 (ng/mL) | 38.445 ± 16.597 | 36.896 ± 18.180 | 0.312 | 0.752 |
| Metallothionein-1 (ng/mL) | ||
|---|---|---|
| r | p | |
| Age | −0.167 | 0.237 |
| Gender | 0.163 | 0.247 |
| BMI | 0.151 | 0.285 |
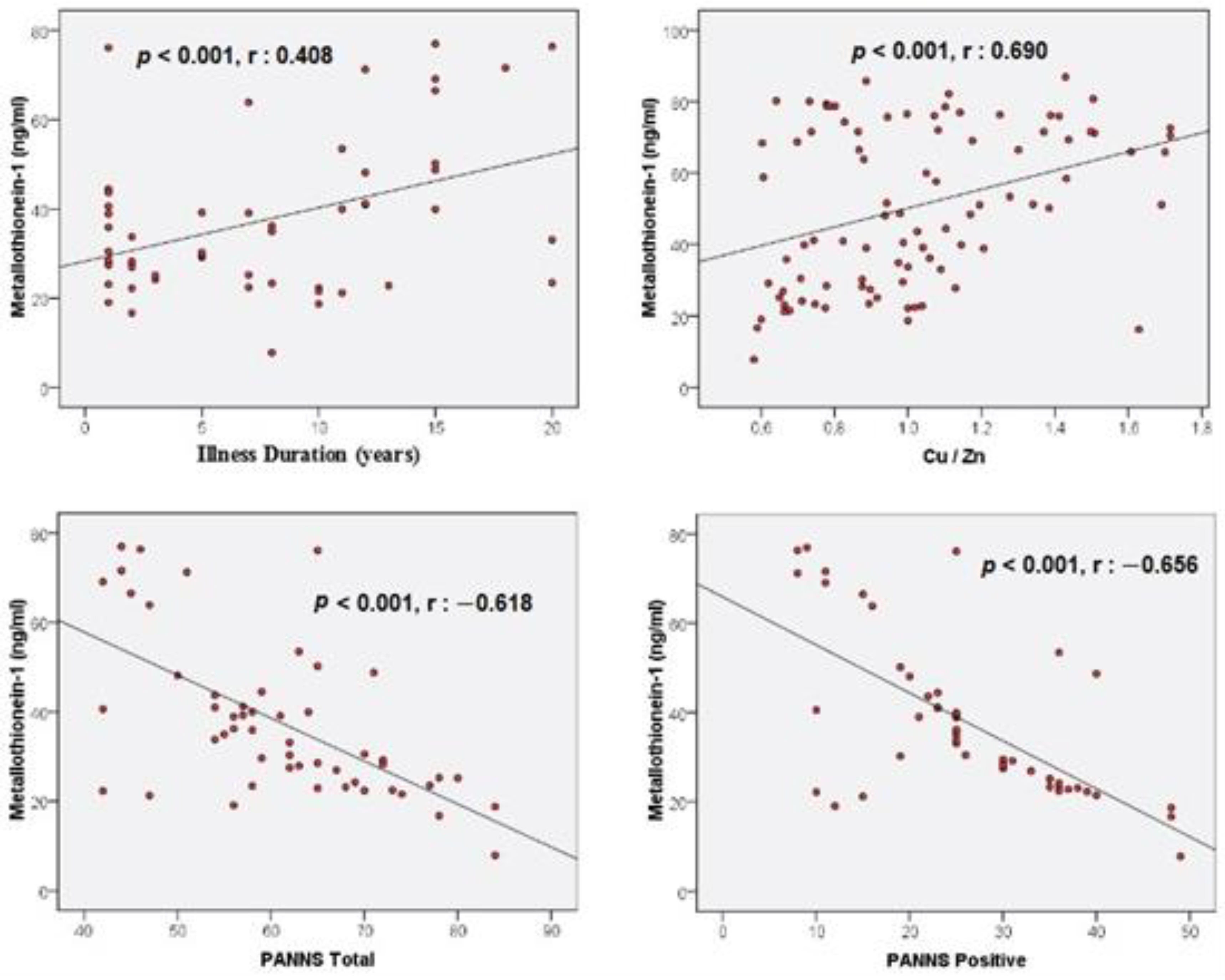
| Illness Duration | 0.408 ** | 0.003 |
| Cu/Zn | 0.690 ** | <0.001 |
| PANSS total | −0.618 ** | <0.001 |
| PANSS positive | −0.656 ** | <0.001 |
| PANSS negative | 0.031 | 0.829 |
| PANSS general psychopathology | −0.031 | 0.826 |
| β | S.E. | p | OR | 95% C.I. for OR | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Cu/Zn | −0.193 | 1.309 | 0.883 | 0.824 | 0.063 | 10.722 |
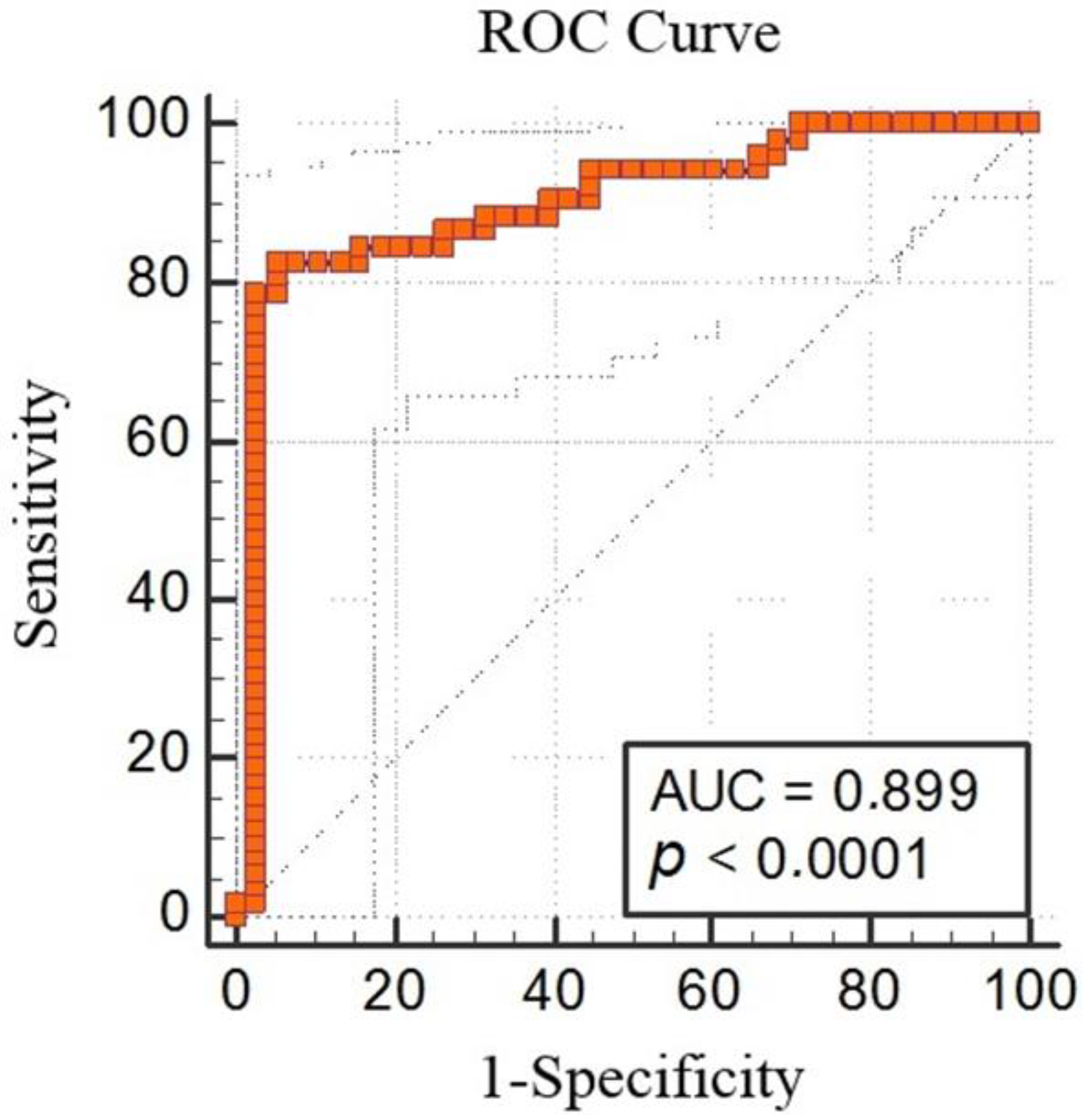
| Metallothionein-1 (ng/mL) | −0.109 | 0.024 | <0.001 | 0.897 | 0.855 | 0.941 |
| Constant | 14.232 | 7058.684 | 0.998 | 1,517,275.075 | - | - |
| Unstandardized Coefficients | Standardized Coefficients | t | p | ||
|---|---|---|---|---|---|
| B | Std. Error | β | |||
| (Constant) | 15.120 | 18.745 | 0.807 | 0.425 | |
| Smoking | 8.482 | 4.925 | 0.170 | 1.780 | 0.095 |
| Olanzapine + Risperidone | 0.962 | 4.723 | 0.023 | 0.204 | 0.840 |
| Olanzapine + Haloperidol | −1.292 | 4.754 | −0.030 | −0.272 | 0.787 |
| Risperidone | 2.118 | 4.863 | 0.048 | 0.436 | 0.666 |
| Olanzapin + Quetiapine | 0.310 | 4.710 | 0.007 | 0.066 | 0.948 |
| PANSS positive | −0.773 | 0.176 | −0.472 | −4.403 | <0.001 |
| PANSS negative | 0.232 | 0.355 | 0.058 | 0.653 | 0.518 |
| PANSS general psychopathology | −0.645 | 0.592 | −0.098 | −1.089 | 0.283 |
| Unstandardized Coefficients | Standardized Coefficients | t | p | ||
|---|---|---|---|---|---|
| B | Std. Error | β | |||
| (Constant) | 25.709 | 17.002 | - | 1.512 | 0.138 |
| Smoking | 8.375 | 4.814 | 0.166 | 1.740 | 0.090 |
| Olanzapine + Risperidone | −1.055 | 4.932 | −0.025 | −0.214 | 0.832 |
| Olanzapine + Haloperidol | −2.014 | 5.070 | −0.046 | −0.397 | 0.693 |
| Risperidone | 0.556 | 5.052 | 0.013 | 0.110 | 0.913 |
| Olanzapin + Quetiapine | −1.190 | 5.001 | −0.027 | −0.238 | 0.813 |
| PANSS total | −0.574 | 0.168 | −0.369 | −3.407 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yılmaz, S.; Kılıç, N.; Kaya, Ş.; Taşcı, G. A Potential Biomarker for Predicting Schizophrenia: Metallothionein-1. Biomedicines 2023, 11, 590. https://doi.org/10.3390/biomedicines11020590
Yılmaz S, Kılıç N, Kaya Ş, Taşcı G. A Potential Biomarker for Predicting Schizophrenia: Metallothionein-1. Biomedicines. 2023; 11(2):590. https://doi.org/10.3390/biomedicines11020590
Chicago/Turabian StyleYılmaz, Seda, Nülüfer Kılıç, Şüheda Kaya, and Gülay Taşcı. 2023. "A Potential Biomarker for Predicting Schizophrenia: Metallothionein-1" Biomedicines 11, no. 2: 590. https://doi.org/10.3390/biomedicines11020590
APA StyleYılmaz, S., Kılıç, N., Kaya, Ş., & Taşcı, G. (2023). A Potential Biomarker for Predicting Schizophrenia: Metallothionein-1. Biomedicines, 11(2), 590. https://doi.org/10.3390/biomedicines11020590