
Transcutaneous Cervical Spinal Cord Stimulation Combined with Robotic Exoskeleton Rehabilitation for the Upper Limbs in Subjects with Cervical SCI: Clinical Trial
 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Design
2.3. Clinical Assessment
2.3.1. Functionality Assessment of Upper Extremity
2.3.2. Maximal Voluntary Contraction
2.3.3. Neurological Assessment
2.3.4. Quality of Life Assessment
2.4. Interventions
2.4.1. Hand Training with Armeo®Power Protocol
2.4.2. Transcutaneous Electrical Spinal Cord Stimulation
2.5. Data and Statistical Analysis
3. Results
3.1. Subjects Clinical and Demographic Characteristics
3.2. Functionality Assessment of Upper Extremity
3.3. Maximal Voluntary Contraction (MVC)
3.4. Neurological Assessment
3.5. Quality of Life Assessment
3.6. Adverse Effects
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gomes-Osman, J.; Cortes, M.; Guest, J.; Pascual-Leone, A. A Systematic Review of Experimental Strategies Aimed at Improving Motor Function after Acute and Chronic Spinal Cord Injury. J. Neurotrauma 2016, 33, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Khorasanizadeh, M.; Yousefifard, M.; Eskian, M.; Lu, Y.; Chalangari, M.; Harrop, J.S.; Jazayeri, S.B.; Seyedpour, S.; Khodaei, B.; Hosseini, M.; et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurosurg. Spine 2019, 30, 683–699. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.C.; Wolfe, D.L.; Spinal Cord Injury Rehabilitation Evidence Scire Research Team. The Health and Life Priorities of Individuals with Spinal Cord Injury: A Systematic Review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Mao, Y.-R.; Yuan, T.-F.; Xu, D.-S.; Cheng, L.-M. Multimodal treatment for spinal cord injury: A sword of neuroregeneration upon neuromodulation. Neural Regen. Res. 2020, 15, 1437. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.W.; Weinstein, S.P. Chronic dorsal column stimulation in multiple sclerosis. Preliminary report. N. Y. State J. Med. 1973, 73, 2868–2872. [Google Scholar] [PubMed]
- Lu, D.C.; Edgerton, V.R.; Modaber, M.; AuYong, N.; Morikawa, E.; Zdunowski, S.; Sarino, M.E.; Sarrafzadeh, M.; Nuwer, M.R.; Roy, R.R.; et al. Engaging Cervical Spinal Cord Networks to Reenable Volitional Control of Hand Function in Tetraplegic Patients. Neurorehabil. Neural Repair. 2016, 30, 951–962. [Google Scholar] [CrossRef] [PubMed]
- Herman, R.; He, J.; D’Luzansky, S.; Willis, W.; Dilli, S. Spinal cord stimulation facilitates functional walking in a chronic, incomplete spinal cord injured. Spinal Cord 2002, 40, 65–68. [Google Scholar] [CrossRef]
- Carhart, M.R.; He, J.; Herman, R.; D’Luzansky, S.; Willis, W.T. Epidural spinal-cord stimulation facilitates recovery of functional walking following incomplete spinal-cord injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 32–42. [Google Scholar] [CrossRef]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.A.; Bryant, N.; Harkema, S.J. Effects of Stand and Step Training with Epidural Stimulation on Motor Function for Standing in Chronic Complete Paraplegics. J. Neurotrauma 2017, 34, 1787–1802. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; Jilge, B.; Rattay, F.; Pinter, M.M.; Binder, H.; Gerstenbrand, F.; Dimitrijevic, M.R. Stepping-like movements in humans with complete spinal cord injury induced by epidural stimulation of the lumbar cord: Electromyographic study of compound muscle action potentials. Spinal Cord 2004, 42, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain 2014, 137, 1394–1409. [Google Scholar] [CrossRef] [PubMed]
- Grahn, P.J.; Lavrov, I.A.; Sayenko, D.G.; Van Straaten, M.G.; Gill, M.L.; Strommen, J.A.; Calvert, J.S.; Drubach, D.I.; Beck, L.A.; Linde, M.B.; et al. Enabling Task-Specific Volitional Motor Functions via Spinal Cord Neuromodulation in a Human with Paraplegia. Mayo Clin. Proc. 2017, 92, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G.; et al. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef] [PubMed]
- Legg Ditterline, B.; Harkema, S.J.; Willhite, A.; Stills, S.; Ugiliweneza, B.; Rejc, E. Epidural stimulation for cardiovascular function increases lower limb lean mass in individuals with chronic motor complete spinal cord injury. Exp. Physiol. 2020, 105, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Sahni, K.S.; Zampieri, T.A.; Severs, S.L.; Greenstein, A.; Katz, P.G. Effect of Implanted Epidural Stimulator onLower Urinary Tract Function in Spinal-Cord-Injured Patients. Eur. Urol. 1991, 20, 103–106. [Google Scholar] [CrossRef]
- Walter, M.; Lee, A.H.X.; Kavanagh, A.; Phillips, A.A.; Krassioukov, A.V. Epidural Spinal Cord Stimulation Acutely Modulates Lower Urinary Tract and Bowel Function Following Spinal Cord Injury: A Case Report. Front. Physiol. 2018, 9, 1816. [Google Scholar] [CrossRef]
- Herrity, A.N.; Williams, C.S.; Angeli, C.A.; Harkema, S.J.; Hubscher, C.H. Lumbosacral spinal cord epidural stimulation improves voiding function after human spinal cord injury. Sci. Rep. 2018, 8, 8688. [Google Scholar] [CrossRef]
- Barolat-Romana, G.; Myklebust, J.B.; Hemmy, D.C.; Myklebust, B.; Wenninger, W. Immediate effects of spinal cord stimulation in spinal spasticity. J. Neurosurg. 1985, 62, 558–562. [Google Scholar] [CrossRef]
- Pinter, M.; Gerstenbrand, F.; Dimitrijevic, M. Epidural electrical stimulation of posterior structures of the human lumbosacral cord: 3. Control of spasticity. Spinal Cord 2000, 38, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Midha, M.; Schmitt, J.K. Epidural spinal cord stimulation for the control of spasticity in spinal cord injury patients lacks long-term efficacy and is not cost-effective. Spinal Cord 1998, 36, 190–192. [Google Scholar] [CrossRef]
- Gad, P.; Lee, S.; Terrafranca, N.; Zhong, H.; Turner, A.; Gerasimenko, Y.; Edgerton, V.R. Non-Invasive Activation of Cervical Spinal Networks after Severe Paralysis. J. Neurotrauma 2018, 35, 2145–2158. [Google Scholar] [CrossRef] [PubMed]
- Freyvert, Y.; Yong, N.A.; Morikawa, E.; Zdunowski, S.; Sarino, M.E.; Gerasimenko, Y.; Edgerton, V.R.; Lu, D.C. Engaging cervical spinal circuitry with non-invasive spinal stimulation and buspirone to restore hand function in chronic motor complete patients. Sci. Rep. 2018, 8, 15546. [Google Scholar] [CrossRef] [PubMed]
- Inanici, F.; Samejima, S.; Gad, P.; Edgerton, V.R.; Hofstetter, C.P.; Moritz, C.T. Transcutaneous electrical spinal stimulation promotes long-term recovery of upper extremity function in chronic tetraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Inanici, F.; Brighton, L.N.; Samejima, S.; Hofstetter, C.P.; Moritz, C.T. Transcutaneous Spinal Cord Stimulation Restores Hand and Arm Function after Spinal Cord Injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 310–319. [Google Scholar] [CrossRef]
- Zhang, F.; Momeni, K.; Ramanujam, A.; Ravi, M.; Carnahan, J.; Kirshblum, S.; Forrest, G.F. Cervical Spinal Cord Transcutaneous Stimulation Improves Upper Extremity and Hand Function in People with Complete Tetraplegia: A Case Study. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 3167–3174. [Google Scholar] [CrossRef]
- Minassian, K.; Hofstoetter, U.S.; Danner, S.M.; Mayr, W.; McKay, W.B.; Tansey, K.; Dimitrijevic, M.R. Mechanisms of rhythm generation of the human lumbar spinal cord in response to tonic stimulation without and with step-related sensory feedback. Biomed. Eng./Biomed. Tech. 2013, 58, Sl-1. [Google Scholar] [CrossRef]
- Shapkova, E.Y.; Pismennaya, E.V.; Emelyannikov, D.V.; Ivanenko, Y. Exoskeleton Walk Training in Paralyzed Individuals Benefits from Transcutaneous Lumbar Cord Tonic Electrical Stimulation. Front. Neurosci. 2020, 14, 416. [Google Scholar] [CrossRef] [PubMed]
- McHugh, L.V.; Miller, A.A.; Leech, K.A.; Salorio, C.; Martin, R.H. Feasibility and utility of transcutaneous spinal cord stimulation combined with walking-based therapy for people with motor incomplete spinal cord injury. Spinal Cord Ser. Cases 2020, 6, 104. [Google Scholar] [CrossRef]
- Gad, P.; Gerasimenko, Y.; Zdunowski, S.; Turner, A.; Sayenko, D.; Lu, D.C.; Edgerton, V.R. Weight Bearing Over-ground Stepping in an Exoskeleton with Non-invasive Spinal Cord Neuromodulation after Motor Complete Paraplegia. Front. Neurosci. 2017, 11, 333. [Google Scholar] [CrossRef] [PubMed]
- Al’joboori, Y.; Massey, S.J.; Knight, S.L.; Donaldson, N.d.N.; Duffell, L.D. The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study. JCM 2020, 9, 2765. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; Hofstoetter, U.S.; Danner, S.M.; Mayr, W.; Bruce, J.A.; McKay, W.B.; Tansey, K.E. Spinal Rhythm Generation by Step-Induced Feedback and Transcutaneous Posterior Root Stimulation in Complete Spinal Cord–Injured Individuals. Neurorehabil. Neural Repair. 2016, 30, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Hofstoetter, U.S.; Krenn, M.; Danner, S.M.; Hofer, C.; Kern, H.; McKay, W.B.; Mayr, W.; Minassian, K. Augmentation of Voluntary Locomotor Activity by Transcutaneous Spinal Cord Stimulation in Motor-Incomplete Spinal Cord-Injured Individuals: Augmentation of Locomotion by tSCS in Incomplete SCI. Artif. Organs 2015, 39, E176–E186. [Google Scholar] [CrossRef]
- Gerasimenko, Y.P.; Lu, D.C.; Modaber, M.; Zdunowski, S.; Gad, P.; Sayenko, D.G.; Morikawa, E.; Haakana, P.; Ferguson, A.R.; Roy, R.R.; et al. Noninvasive Reactivation of Motor Descending Control after Paralysis. J. Neurotrauma 2015, 32, 1968–1980. [Google Scholar] [CrossRef]
- Rath, M.; Vette, A.H.; Ramasubramaniam, S.; Li, K.; Burdick, J.; Edgerton, V.R.; Gerasimenko, Y.P.; Sayenko, D.G. Trunk Stability Enabled by Noninvasive Spinal Electrical Stimulation after Spinal Cord Injury. J. Neurotrauma 2018, 35, 2540–2553. [Google Scholar] [CrossRef]
- Sayenko, D.G.; Rath, M.; Ferguson, A.R.; Burdick, J.W.; Havton, L.A.; Edgerton, V.R.; Gerasimenko, Y.P. Self-Assisted Standing Enabled by Non-Invasive Spinal Stimulation after Spinal Cord Injury. J. Neurotrauma 2019, 36, 1435–1450. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Danner, S.M.; Krenn, M.J.; Mayr, W.; Binder, H.; Minassian, K. Transcutaneous Spinal Cord Stimulation Induces Temporary Attenuation of Spasticity in Individuals with Spinal Cord Injury. J. Neurotrauma 2020, 37, 481–493. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; McKay, W.B.; Tansey, K.E.; Mayr, W.; Kern, H.; Minassian, K. Modification of spasticity by transcutaneous spinal cord stimulation in individuals with incomplete spinal cord injury. J. Spinal Cord Med. 2014, 37, 202–211. [Google Scholar] [CrossRef]
- Estes, S.P.; Iddings, J.A.; Field-Fote, E.C. Priming Neural Circuits to Modulate Spinal Reflex Excitability. Front. Neurol. 2017, 8, 17. [Google Scholar] [CrossRef]
- Gad, P.N.; Kreydin, E.; Zhong, H.; Latack, K.; Edgerton, V.R. Non-invasive Neuromodulation of Spinal Cord Restores Lower Urinary Tract Function After Paralysis. Front. Neurosci. 2018, 12, 432. [Google Scholar] [CrossRef]
- Kreydin, E.; Zhong, H.; Latack, K.; Ye, S.; Edgerton, V.R.; Gad, P. Transcutaneous Electrical Spinal Cord Neuromodulator (TESCoN) Improves Symptoms of Overactive Bladder. Front. Syst. Neurosci. 2020, 14, 1. [Google Scholar] [CrossRef]
- Phillips, A.A.; Squair, J.W.; Sayenko, D.G.; Edgerton, V.R.; Gerasimenko, Y.; Krassioukov, A.V. An Autonomic Neuroprosthesis: Noninvasive Electrical Spinal Cord Stimulation Restores Autonomic Cardiovascular Function in Individuals with Spinal Cord Injury. J. Neurotrauma 2018, 35, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, R.; Nightingale, T.E.; Pawar, K.; Kalimullina, T.; Mesa, A.; Marwaha, A.; Williams, A.M.M.; Lam, T.; Krassioukov, A.V. Noninvasive Neuroprosthesis Promotes Cardiovascular Recovery after Spinal Cord Injury. Neurotherapeutics 2021, 18, 1244–1256. [Google Scholar] [CrossRef]
- Kumru, H.; Flores, Á.; Rodríguez-Cañón, M.; Edgerton, V.R.; García, L.; Benito-Penalva, J.; Navarro, X.; Gerasimenko, Y.; García-Alías, G.; Vidal, J. Cervical Electrical Neuromodulation Effectively Enhances Hand Motor Output in Healthy Subjects by Engaging a Use-Dependent Intervention. JCM 2021, 10, 195. [Google Scholar] [CrossRef] [PubMed]
- Duret, C.; Grosmaire, A.-G.; Krebs, H.I. Robot-Assisted Therapy in Upper Extremity Hemiparesis: Overview of an Evidence-Based Approach. Front. Neurol. 2019, 10, 412. [Google Scholar] [CrossRef] [PubMed]
- Duret, C.; Mazzoleni, S. Upper limb robotics applied to neurorehabilitation: An overview of clinical practice. NeuroRehabilitation 2017, 41, 5–15. [Google Scholar] [CrossRef]
- Kalsi-Ryan, S.; Beaton, D.; Curt, A.; Duff, S.; Popovic, M.R.; Rudhe, C.; Fehlings, M.G.; Verrier, M.C. The Graded Redefined Assessment of Strength Sensibility and Prehension: Reliability and Validity. J. Neurotrauma 2012, 29, 905–914. [Google Scholar] [CrossRef]
- Platz, T.; Pinkowski, C.; van Wijck, F.; Kim, I.-H.; di Bella, P.; Johnson, G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A multicentre study. Clin. Rehabil. 2005, 19, 404–411. [Google Scholar] [CrossRef]
- Itzkovich, M.; Gelernter, I.; Biering-Sorensen, F.; Weeks, C.; Laramee, M.T.; Craven, B.C.; Tonack, M.; Hitzig, S.L.; Glaser, E.; Zeilig, G.; et al. The Spinal Cord Independence Measure (SCIM) version III: Reliability and validity in a multi-center international study. Disabil. Rehabil. 2007, 29, 1926–1933. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (Revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Salvador-De La Barrera, S.; Mora-Boga, R.; Ferreiro-Velasco, M.E.; Seoane-Pillado, T.; Montoto-Marqués, A.; Rodríguez-Sotillo, A.; Pertega Díaz, S. A validity study of the Spanish—World Health Organization Quality of Life short version instrument in persons with traumatic spinal cord injury. Spinal Cord 2018, 56, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Kumru, H.; Rodríguez-Cañón, M.; Edgerton, V.R.; García, L.; Flores, Á.; Soriano, I.; Opisso, E.; Gerasimenko, Y.; Navarro, X.; García-Alías, G.; et al. Transcutaneous electrical neuromodulation of the cervical spinal cord depends both on the stimulation intensity and the degree of voluntary activity for training. A pilot study. J. Clin. Med. 2021, 10, 3278. [Google Scholar] [CrossRef] [PubMed]
- Benavides, F.D.; Jo, H.J.; Lundell, H.; Edgerton, V.R.; Gerasimenko, Y.; Perez, M.A. Cortical and Subcortical Effects of Transcutaneous Spinal Cord Stimulation in Humans with Tetraplegia. J. Neurosci. 2020, 40, 2633–2643. [Google Scholar] [CrossRef]
- Milosevic, M.; Masugi, Y.; Sasaki, A.; Sayenko, D.G.; Nakazawa, K. On the reflex mechanisms of cervical transcutaneous spinal cord stimulation in human subjects. J. Neurophysiol. 2019, 121, 1672–1679. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Binder, H.; Minassian, K. Common neural structures activated by epidural and transcutaneous lumbar spinal cord stimulation: Elicitation of posterior root-muscle reflexes. PLoS ONE 2018, 13, e0192013. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age | Gender | NLI | AIS | Total UEMS | Etiology | Time since SCI (Months) | Washout (Days) | Intensity tSCS at C3-C4 (mA) | Intensity tSCS at C6-C7 (mA) |
|---|---|---|---|---|---|---|---|---|---|---|
| Intervention group (tSCS + Armeo®Power) | ||||||||||
| 1 ** | 46 | M | C4 | C | 15 | Trauma | 4 | 59 | 80 | 80 |
| 2 ** | 25 | M | C4 | A | 11 | Trauma | 4 | 111 | 67 | 86 |
| 4 * | 36 | M | C5 | B | 14 | Trauma | 6 | 74 | 86 | |
| 6 | 36 | M | C7 | D | 41 | Trauma | 6 | 63 | 85 | |
| 8 | 28 | M | C5 | A | 28 | Trauma | 4 | 86 | 86 | |
| 10 | 28 | M | C5 | C | 26 | Trauma | 6 | 63 | 85 | |
| 12 * | 38 | M | C4 | B | 48 | Trauma | 5 | 54 | 77 | |
| 15 * | 56 | M | C4 | C | 33 | Medical | 9 | 86 | 86 | |
| 17 * | 21 | M | C5 | D | 42 | Trauma | 5 | 39 | 45 | |
| 19 | 60 | M | C5 | D | 43 | Trauma | 3 | 86 | 86 | |
| 20 ** | 21 | M | C6 | B | 22 | Trauma | 8 | 42 | 61 | 72 |
| 26 * | 22 | F | C7 | C | 43 | Trauma | 5 | 85 | 86 | |
| 27 | 55 | M | C3 | D | 41 | Trauma | 4 | 86 | 86 | |
| 28 | 47 | M | C6 | D | 31 | Trauma | 10 | 86 | 86 | |
| 29 | 42 | M | C4 | D | 31 | Trauma | 3 | 80 | 76 | |
| Control group (Armeo®Power) | ||||||||||
| 3 * | 36 | M | C4 | B | 12 | Trauma | 5 | 30 | ||
| 5 ** | 46 | M | C4 | C | 17 | Trauma | 6 | |||
| 7 ** | 25 | M | C4 | A | 15 | Trauma | 8 | |||
| 9 | 36 | F | C4 | C | 37 | Trauma | 6 | |||
| 11 * | 38 | M | C7 | B | 48 | Trauma | 3 | 58 | ||
| 13 * | 56 | M | C4 | C | 32 | Medical | 6 | 79 | ||
| 14 * | 21 | M | C5 | D | 42 | Trauma | 4 | 30 | ||
| 16 | 70 | M | C5 | C | 29 | Trauma | 8 | |||
| 18 | 58 | M | C6 | A | 44 | Trauma | 6 | |||
| 21 ** | 21 | M | C6 | B | 22 | Trauma | 9 | |||
| 22 | 53 | M | T1 | B | 47 | Medical | 3 | |||
| 23 | 32 | M | C5 | D | 40 | Trauma | 3 | |||
| 24 | 18 | M | C6 | B | 17 | Trauma | 4 | |||
| 25 * | 22 | F | C7 | C | 41 | Trauma | 4 | 35 | ||
| p-value | 0.43 | 0.19 | 0.63 | 0.61 | 0.51 | 0.19 | 0.89 | |||
| Outcome Measure | Upper Extremity | p-Value |
|---|---|---|
| GRASSP | R | 0.631 |
| L | 0.827 | |
| R + L | 0.861 | |
| BBT | R | 0.740 |
| L | 0.615 | |
| R + L | 0.740 | |
| SCIM III | R | - |
| L | - | |
| R + L | 0.194 | |
| MVC: cylindrical grip force | R | 0.772 |
| L | 0.982 | |
| R + L | 0.757 | |
| MVC: lateral pinch force | R | 0.876 |
| L | 0.705 | |
| R + L | 0.540 | |
| MVC: tip-to-tip pinch force | R | 0.559 |
| L | 0.947 | |
| R + L | 0.740 |
| Outcome Measures | Intervention Group (tSCS + Armeo®Power) | Control Group (Armeo®Power) | Change Score | ||||
|---|---|---|---|---|---|---|---|
| Time | Mean ± SD | p Value | Mean ± SD | p Value | p Value Baseline-Post between Intervention vs. Control Group | p Value Baseline-Follow between Intervention vs. Control Group | |
| GRASSP strength (R) | Baseline Post Follow-up | 26.13 ± 12.95 28.13 ± 12.90 26.75 ± 12.76 | 0.001 $ 0.002 $ | 28.64 ± 14.77 29.57 ± 15.11 27.00 ± 14.43 | 0.016 $ 0.011 $ | 0.022 | 0.024 |
| GRASPP strength (L) | Baseline Post Follow-up | 28.53 ± 13.33 31.53 ± 13.29 31.33 ± 13.94 | 0.001 $ 0.002 $ | 28.07 ± 12.12 29.78 ± 13.32 30.08 ± 14.33 | 0.007 $ 0.005 $ | 0.110 | 0.073 |
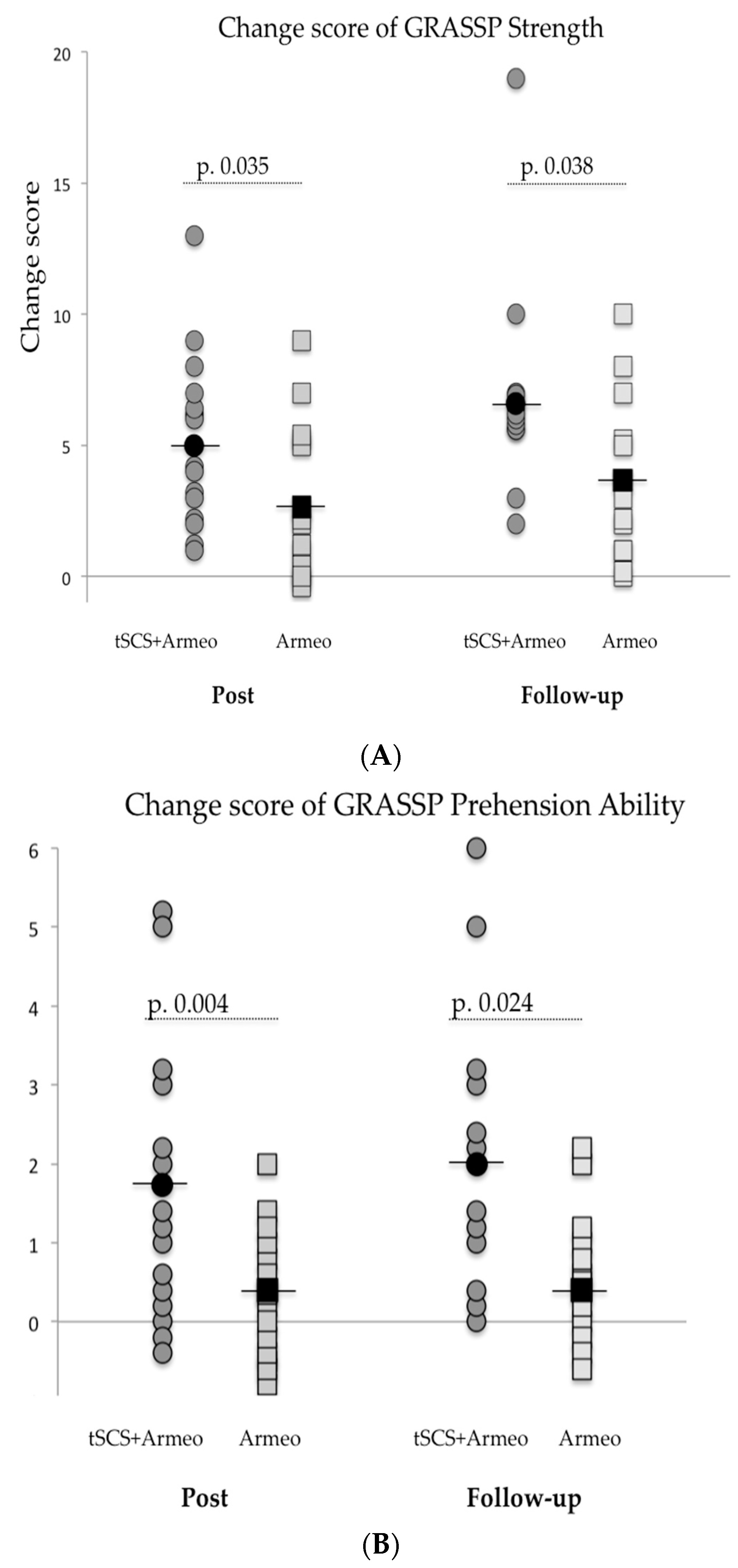
| GRASSP strength (R+ L) | Baseline Post Follow-up | 54.67 ± 24.31 59.67 ± 24.59 58.08 ± 25.26 | 0.001 $ 0.002 $ | 56.71 ± 25.83 59.36 ± 27.24 57.08 ± 28.33 | 0.007 $ 0.005 $ | 0.035 | 0.038 |
| GRASSP sensation (R) | Baseline Post Follow-up | 9.53 ± 3.89 10.33 ± 3.37 10.25 ± 3.52 | 0.039 $ 0.066 $ | 10.21 ± 3.53 10.00 ± 3.57 9.83 ± 3.59 | 0.607 * | 0.014 | 0.095 |
| GRASSP sensation (L) | Baseline Post Follow-up | 9.93 ± 3.49 10.27 ± 3.39 10.33 ± 3.68 | 0.202 * | 10.71 ± 3.20 10.71 ± 3.20 10.50 ± 3.42 | 1.000 * | 0.233 | 0.166 |
| GRASSP Sensation (R + L) | Baseline Post Follow-up | 19.47 ± 7.26 20.60 ± 6.74 20.58 ± 7.14 | 0.017 $ 0.042 $ | 20.93 ± 6.53 20.71 ± 6.56 20.33 ± 6.88 | 0.717 * | 0.011 | 0.113 |
| GRASSP prehension ability: cylindrical (R) | Baseline Post Follow-up | 1.67 ± 1.67 1.73 ± 1.71 1.75 ± 1.71 | 0.156 * | 2.00 ± 1.71 1.93 ± 1.73 1.58 ± 1.62 | 0.368 * | 0.164 | 0.088 |
| GRASSP prehension ability cylindrical (L) | Baseline Post Follow-up | 2.00 ± 1.73 2.13 ± 1.77 2.17 ± 1.80 | 0.135 * | 1.93 ± 1.68 2.07 ± 1.77 2.25 ± 1.81 | 0.135 * | 0.942 | 1.000 |
| GRASSP prehension ability: cylindrical grasp (R + L) | Baseline Post Follow-up | 3.67 ± 3.22 3.87 ± 3.27 3.92 ± 3.42 | 0.082 * | 3.93 ± 3.07 4.00 ± 3.09 3.83 ± 3.30 | 0.368 * | 0.563 | 0.248 |
| GRASSP prehension ability: lateral key pinch (R) | Baseline Post Follow-up | 1.53 ± 1.24 2.00 ± 1.56 1.67 ± 1.37 | 0.024 $ 0.046 $ | 1.86 ± 1.51 1.86 ± 1.51 1.67 ± 1.37 | 1.000 $ 0.317 $ | 0.009 | 0.140 |
| GRASSP prehension ability: lateral key pinch (L) | Baseline Post Follow-up | 2.00 ± 1.56 2.40 ± 1.64 2.25 ± 1.60 | 0.041 *,⌘ | 2.21 ± 1.31 2.43 ± 1.50 2. 33 ± 1.57 | 0.083 0.157 | 0.620 | 0.286 |
| GRASSP prehension ability: lateral key pinch (R + L) | Baseline Post Follow-up | 3.53 ± 2.69 4.40 ± 3.11 3.91 ± 2.87 | 0.017 $ 0.026 $ | 4.07 ± 2.70 4.28 ± 2.87 4.00 ± 2.79 | 0.097 * | 0.092 | 0.131 |
| GRASSP prehension ability: tip-to-tip pinch (R) | Baseline Post Follow-up | 1.73 ± 1.33 1.93 ± 1.39 1.58 ± 1.16 | 0.247 * | 1.78 ± 1.31 1.78 ± 1.31 1.66 ± 1.30 | 0.368 * | 0.163 | 0.596 |
| GRASSP prehension ability: tip-to-tip pinch (L) | Baseline Post Follow-up | 1.93 ± 1.33 2.40 ± 1.50 2.33 ± 1.56 | 0.020 $ 0.034 $ | 1.93 ± 1.33 2.00 ± 1.36 2.08 ± 1.56 | 0.040 $ 0.167 $ | 0.040 | 0.167 |
| GRASSP prehension ability: tip-to-tip pinch (R + L) | Baseline Post Follow-up | 3.67 ± 2.44 4.33 ± 2.66 3.91 ± 2.43 | 0.016 $ 0.026 $ | 3.71 ± 2.40 3.78 ± 2.42 3.75 ± 2.70 | 0.017 $ 0.111 $ | 0.017 | 0.111 |
| GRASSP total prehension ability (R) | Baseline Post Follow-up | 4.93 ± 4.08 5.67 ± 4.50 5.00 ± 3.95 | 0.010 $ 0.016 $ | 5.64 ± 4.36 5.57 ± 4.36 4.92 ± 4.16 | 0.368 * | 0.001 | 0.021 |
| GRASSP total prehension ability (L) | Baseline Post Follow-up | 5.93 ± 4.33 6.93 ± 4.62 6.75 ± 4.71 | 0.011 $ 0.016 $ | 6.07 ± 4.14 6.50 ± 4.41 6.67 ± 4.81 | 0.039 *,⌘ | 0.140 | 0.084 |
| GRASSP total prehension ability (R + L) | Baseline Post Follow-up | 10.87 ± 7.98 12.60 ± 8.74 11.75 ± 8.38 | 0.002 $ 0.008 $ | 11.71 ± 7.95 12.07 ± 8.16 11.58 ± 8.64 | 0.059 $ 0.038 $ | 0.004 | 0.024 |
| GRASSP prehension Performance (R) | Baseline Post Follow-up | 10.07 ± 6.45 10.87 ± 6.43 11.25 ± 6.94 | 0.066 $ 0.026 $ | 10.50 ± 6.78 11.21 ± 6.74 10.25 ± 6.56 | 0.059 $ 0.038 $ | 0.887 | 0.077 |
| GRASSP prehension performance (L) | Baseline Post Follow-up | 11.20 ± 7.51 12.07 ± 7.25 12.42 ± 7.21 | 0.025 $ 0.011 $ | 10.07 ± 6.85 11.28 ± 7.03 12.50 ± 6.93 | 0.011 $ 0.008 $ | 0.890 | 0.638 |
| GRASSP prehension performance (R + L) | Baseline Post Follow-up | 21.27± 13.44 22.93 ± 13.22 23.67 ± 18.84 | 0.019 $ 0.004 $ | 20.57 ± 12.69 29.94 ± 12.57 22.75 ± 13.14 | 0.004 $ 0.005 $ | 0.639 | 0.448 |
| GRASSP (R) | Baseline Post Follow-up | 50.67 ± 25.08 55.00 ± 25.19 53.25 ± 25.10 | 0.001 $ 0.016 $ | 55.00 ± 27.67 56.36 ± 27.71 52.00 ± 26.40 | 0.016 $ 0.015 $ | 0.003 | 0.003 |
| GRASSP (L) | Baseline Post Follow-up | 55.60 ± 26.65 60.80 ± 26.67 60.83 ± 27.67 | 0.001 $ 0.002 $ | 54.93 ± 24.12 58.28 ± 25.81 59.75 ± 27.37 | 0.002 $ 0.002 $ | 0.108 | 0.308 |
| GRASSP (R + L) | Baseline Post Follow-up | 106.27 ± 49.92 115.80 ± 49.91 114.08 ± 51.25 | 0.001 $ 0.002 $ | 109.93 ± 49.54 114.64 ± 51.05 111.75 ± 52.94 | 0.001 $ 0.002 $ | 0.004 | 0.011 |
| BBT (R) | Baseline Post Follow-up | 35.31 ± 16.96 40.23 ± 15.66 43.10 ± 15.95 | 0.004 & 0.000 & | 28.14 ± 19.47 33.00 ± 21.98 31.00 ± 21.48 | 0.008 & 0.007 & | 0.715 | 0.164 |
| BBT (L) | Baseline Post Follow-up | 36.54 ± 18.18 40.00 ± 17.43 45.20 ± 16.18 | 0.008 & 0.000 & | 27.71 ± 20.60 31.36 ± 21.74 34.58 ± 20.79 | 0.010 & 0.003 & | 0.826 | 0.163 |
| BBT (R+ L) | Baseline Post Follow-up | 66.71 ± 37.67 74.50 ± 36.96 80.27 ± 39.00 | 0.002 & 0.000 & | 55.86 ± 38.15 64.36 ± 41.72 65.58 ± 41.41 | 0.003 & 0.001 & | 0.629 | 0.185 |
| MVC: cylindrical grasp force (R) | Baseline Post Follow-up | 12.51 ± 10.96 14.37 ± 10.91 11.84 ± 7.95 | 0.007 $ 0.017 $ | 11.37 ± 9.13 12.23 ± 9.91 10.87 ± 6.37 | 0.046 $ 0.018 $ | 0.152 | 0.247 |
| MVC: cylindrical grasp force (L) | Baseline Post Follow-up | 9.54 ± 5.50 10.90 ± 5.81 12.77 ± 7.31 | 0.009 $ 0.008 $ | 9.40 ± 6.26 10.92 ± 7.35 12.49 ± 6.65 | 0.059 $ 0.036 $ | 0.860 | 0.211 |
| MVC: cylindrical grasp force (R + L) | Baseline Post Follow-up | 20.90 ± 12.25 23.96 ± 12.64 23.29 ± 11.21 | 0.005 $ 0.008 $ | 19.63 ± 12.22 21.93 ± 14.16 22.00 ± 12.64 | 0.037 $ 0.017 $ | 0.398 | 0.083 |
| MVC: lateral pinch force (R) | Baseline Post Follow-up | 2.67 ± 2.41 3.11 ± 2.60 2.26 ± 1.54 | 0.012 $ 0.093 $ | 2.39 ± 2.37 2.82 ± 2.51 2.28 ± 1.88 | 0.042 $ 0.114 $ | 0.837 | 0.815 |
| MVC: lateral pinch force (L) | Baseline Post Follow-up | 2.24 ± 1.46 2.82 ± 1.44 3.55 ± 1.92 | 0.008 $ 0.028 $ | 2.40 ± 1.45 2.44 ± 1.64 2.91 ± 1.54 | 0.368 * | 0.033 | 0.090 |
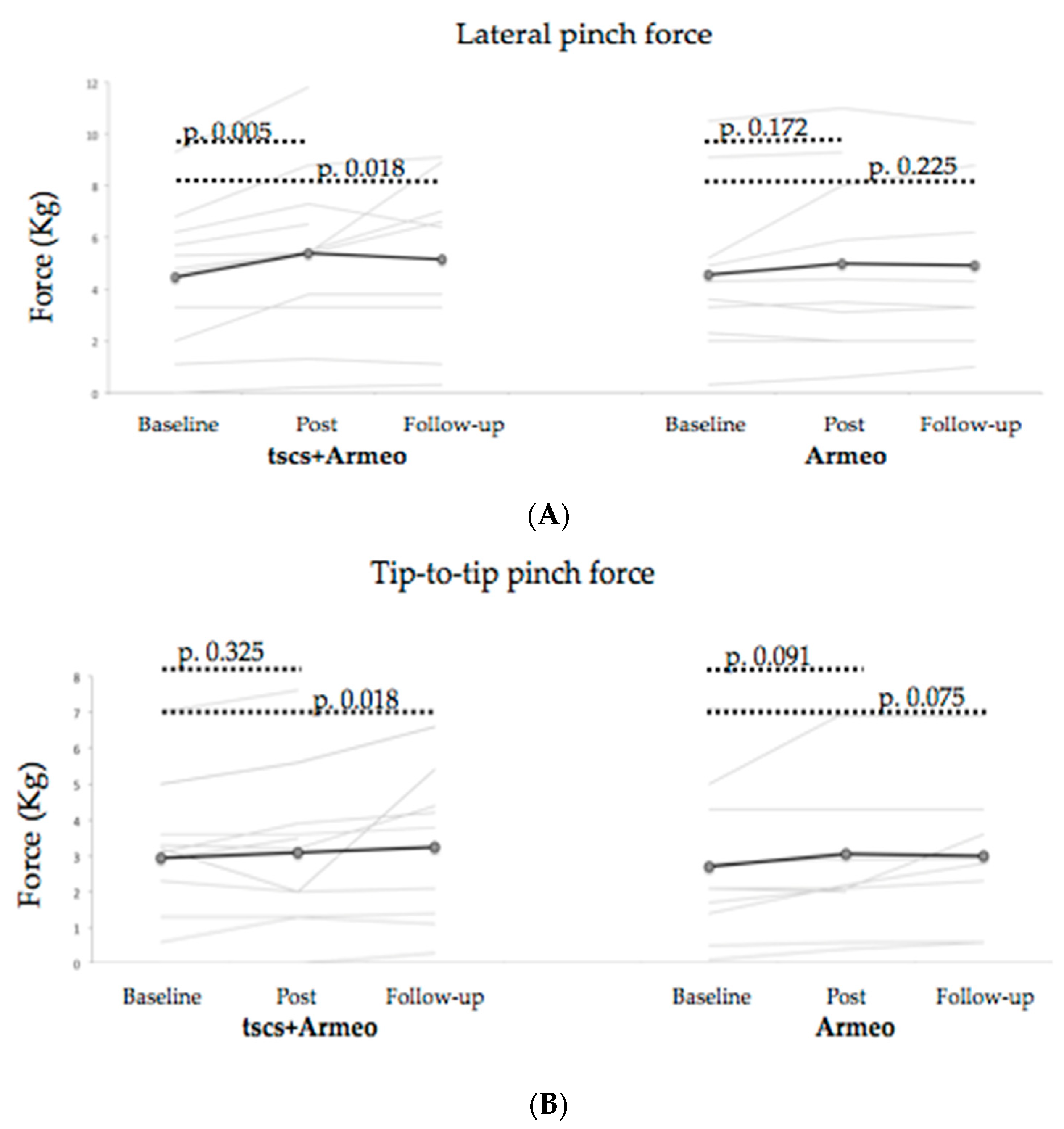
| MVC: lateral pinch force (R + L) | Baseline Post Follow-up | 4.46 ± 2.70 5.39 ± 3.29 5.17 ± 3.29 | 0.005 $ 0.018 $ | 4.55 ± 3.14 4.98 ± 3.46 4.91 ± 3.30 | 0.341 * | 0.138 | 0.107 |
| MVC: tip-to-tip pinch force (R) | Baseline Post Follow-up | 1.64 ± 1.60 1.72 ± 1.69 1.57 ± 1.46 | 0.232 $ 0.031 $ | 1.31 ± 1.36 1.70 ± 1.84 1.30± 1.33 | 0.128 * | 0.435 | 0.815 |
| MVC: tip-to-tip pinch force (L) | Baseline Post Follow-up | 1.59± 0.89 1.68 ± 0.91 2.09 ± 1.11 | 0.360 $ 0.021 $ | 1.53 ± 1.19 1.52 ± 0.91 1.86 ± 1.00 | 0.125 * | 0.647 | 0.342 |
| MVC: tip-to-tip pinch force (R + L) | Baseline Post Follow-up | 2.94 ± 1.96 3.09 ± 2.15 3.25 ± 2.13 | 0.325 $ 0.018 $ | 2.71 ± 2.17 3.05 ± 2.32 3.00 ± 2.05 | 0.034 *,⌘ | 0.776 | 0.358 |
| Upper motor extremity AIS | Baseline Post Follow-up | 31.27 ± 11.83 33.20 ± 11.58 33.00 ± 12.99 | 0.001 & 0.002 & | 31.64 ± 12.83 32.86 ± 13.17 32.17 ± 13.74 | 0.009 & 0.002 & | 0.241 | 0.129 |
| Total Motor Score AIS | Baseline Post Follow-up | 50.27 ± 27.44 53.33 ± 28.43 50.25 ± 27.45 | 0.017 & 0.015 & | 45.50 ± 26.52 47.71 ± 27.50 42.33 ± 24.85 | 0.051 & 0.023 & | 0.583 | 0.394 |
| Total Sensitive Score AIS | Baseline Post Follow-up | 68.00 ± 24.37 67.67 ± 25.05 66.92 ± 23.80 | 0.628 & 0.199 & | 64.67 ± 28.31 64.33 ± 27.72 63.17 ± 25.96 | 0.547 & 0.191 & | 0.456 | 0.759 |
| SCIM III | Baseline Post Follow-up | 53.87 ± 26.65 57.40 ± 27.57 52.75 ± 26.72 | 0.007 & 0.033 & | 41.28 ± 24.21 43.00 ± 24.53 43.00 ± 24.53 | 0.019 & 0.019 & | 0.208 | 0.130 |
| WHO-QoL-BREF Quality of life | Baseline Post Follow-up | 2.80 ± 1.15 2.86 ± 0.99 2.83 ± 1.11 | 0.449 * | 2.38 ± 1.04 2.85 ± 1.14 2.54 ± 1,51 | 0.143 * | 0.083 | 0.657 |
| WHO-QoL-BREF Health satisfaction | Baseline Post Follow-up | 3.00 ± 1.00 3.00 ± 1.00 2.83 ± 1.27 | 0.584 * | 2.31 ± 1,18 2.69 ± 1.25 2.63 ± 1.43 | 0.116 * | 0.067 | 0.101 |
| WHO-QoL-BREF Physical Health | Baseline Post Follow-up | 46.73 ± 14.07 49.33 ± 13.79 45.92 ± 15.86 | 0.267 * | 41.61 ± 10.96 45.38 ± 13.28 42.18 ± 20.42 | 0.317 * | 0.599 | 0.706 |
| WHO-QoL-BREF Psychological | Baseline Post Follow-up | 54.60 ± 19.74 54.60 ± 20.12 51.08 ± 20.43 | 0.670 * | 52.00 ± 17.10 56.31 ± 17.85 50.55 ± 25.97 | 0.183 * | 0.168 | 0.611 |
| WHO-QoL-BREF Social relationships | Baseline Post Follow-up | 53.73 ± 19.89 53.33 ± 21.15 46.42 ± 22.50 | 0.101 * | 53.92 ± 18.74 15. 12 ± 51.85 48.27 ± 22.40 | 0.444 * | 0.289 | 0.972 |
| WHO-QoL-BREF Environment | Baseline Post Follow-up | 48.40 ± 18.53 48.73 ± 16.50 48.42 ± 15.49 | 0.453 * | 47.23 ± 11.36 46.15 ± 15.25 46.15 ± 15.25 | 0.867 * | 0.745 | 0.562 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Alén, L.; Kumru, H.; Castillo-Escario, Y.; Benito-Penalva, J.; Medina-Casanovas, J.; Gerasimenko, Y.P.; Edgerton, V.R.; García-Alías, G.; Vidal, J. Transcutaneous Cervical Spinal Cord Stimulation Combined with Robotic Exoskeleton Rehabilitation for the Upper Limbs in Subjects with Cervical SCI: Clinical Trial. Biomedicines 2023, 11, 589. https://doi.org/10.3390/biomedicines11020589
García-Alén L, Kumru H, Castillo-Escario Y, Benito-Penalva J, Medina-Casanovas J, Gerasimenko YP, Edgerton VR, García-Alías G, Vidal J. Transcutaneous Cervical Spinal Cord Stimulation Combined with Robotic Exoskeleton Rehabilitation for the Upper Limbs in Subjects with Cervical SCI: Clinical Trial. Biomedicines. 2023; 11(2):589. https://doi.org/10.3390/biomedicines11020589
Chicago/Turabian StyleGarcía-Alén, Loreto, Hatice Kumru, Yolanda Castillo-Escario, Jesús Benito-Penalva, Josep Medina-Casanovas, Yury P. Gerasimenko, Victor Reggie Edgerton, Guillermo García-Alías, and Joan Vidal. 2023. "Transcutaneous Cervical Spinal Cord Stimulation Combined with Robotic Exoskeleton Rehabilitation for the Upper Limbs in Subjects with Cervical SCI: Clinical Trial" Biomedicines 11, no. 2: 589. https://doi.org/10.3390/biomedicines11020589
APA StyleGarcía-Alén, L., Kumru, H., Castillo-Escario, Y., Benito-Penalva, J., Medina-Casanovas, J., Gerasimenko, Y. P., Edgerton, V. R., García-Alías, G., & Vidal, J. (2023). Transcutaneous Cervical Spinal Cord Stimulation Combined with Robotic Exoskeleton Rehabilitation for the Upper Limbs in Subjects with Cervical SCI: Clinical Trial. Biomedicines, 11(2), 589. https://doi.org/10.3390/biomedicines11020589