
Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer



 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Endometrial Cancer Overview
3. Classification Systems of Endometrial Cancer and Related Risk Factors
3.1. Dualistic Model
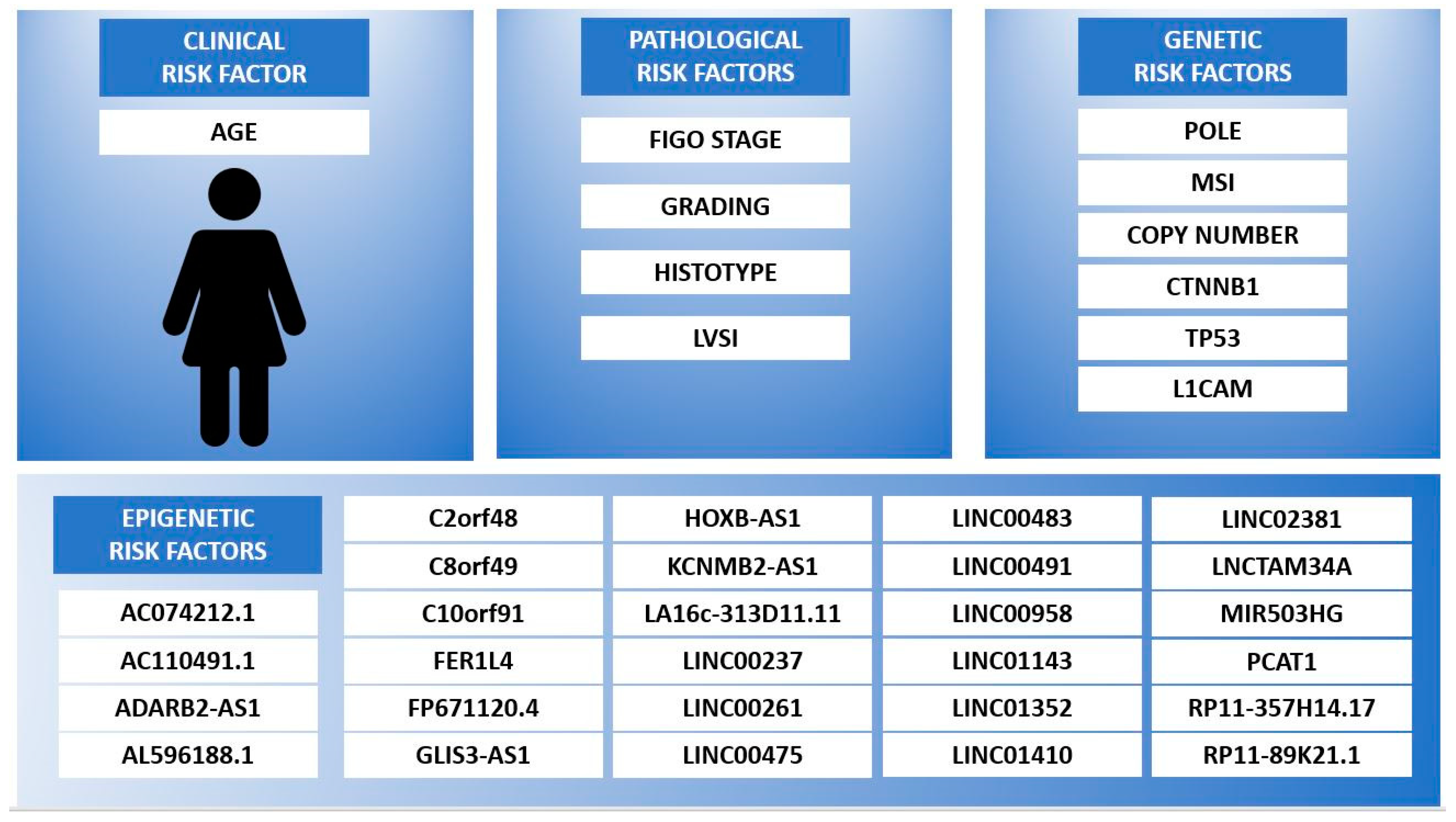
3.2. ESMO/ESGO/ESTRO Classification
- -
- Age.
- -
- FIGO stage.
- -
- Depth of myometrial invasion.
- -
- Tumor differentiation grade.
- -
- Tumor histotype.
- -
- LVSI.
3.3. TCGA Classification
- (1)
- POLE ultramutated
- (2)
- Microsatellite instability hypermutated
- (3)
- Low copy-number
- (4)
- High copy-number
3.4. PORTEC-4a Classification
- (1)
- Favorable:
- -
- POLE mutation,
- -
- or NSMP (No Specific Molecular Profile),
- -
- without CTNNB1 mutations.
- (2)
- Intermediate:
- -
- Mismatch repair-deficient (MMRd),
- -
- or NSMP,
- -
- with CTNNB1 mutations.
- (3)
- Unfavorable:
- -
- substantial LVSI,
- -
- TP53 abnormal immunohistochemical staining
- -
- or L1CAM overexpression.
4. Epigenetic Risk Factors of EC
4.1. ncRNA Role in EC Pathogenesis
4.2. ncRNA as Risk Factor for EC
4.3. ncRNA Selected for EC Patients Risk Stratification
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bokhman, J.V. Two Pathogenetic Types of Endometrial Carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated Genomic Characterization of Endometrial Carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PORTEC-4a, Version 2.5.1, 26 June 2020. NCT03469674. Available online: https://clinicaltrials.gov/ct2/show/NCT03469674 (accessed on 10 March 2021).
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Juergenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; Van Der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer—Combined Analysis of the PORTEC Cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef] [Green Version]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Radiother. Oncol. 2021, 154, 327–353. [Google Scholar] [CrossRef]
- Vallone, C.; Rigon, G.; Gulia, C.; Baffa, A.; Votino, R.; Morosetti, G.; Zaami, S.; Briganti, V.; Catania, F.; Gaffi, M.; et al. Non-Coding RNAs and Endometrial Cancer. Genes 2018, 9, 187. [Google Scholar] [CrossRef] [Green Version]
- Piergentili, R.; Zaami, S.; Cavaliere, A.F.; Signore, F.; Scambia, G.; Mattei, A.; Marinelli, E.; Gulia, C.; Perelli, F. Non-Coding RNAs as Prognostic Markers for Endometrial Cancer. Int. J. Mol. Sci. 2021, 22, 3151. [Google Scholar] [CrossRef]
- Cancer Stat Facts: Uterine Cancer. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 10 March 2021).
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Braun, M.M.; Overbeek-Wager, E.A.; Grumbo, R.J. Diagnosis and Management of Endometrial Cancer. Am. Fam. Phys. 2016, 93, 468–474. [Google Scholar]
- Lu, K.H.; Schorge, J.O.; Rodabaugh, K.J.; Daniels, M.S.; Sun, C.C.; Soliman, P.T.; White, K.G.; Luthra, R.; Gershenson, D.M.; Broaddus, R.R. Prospective Determination of Prevalence of Lynch Syndrome in Young Women with Endometrial Cancer. J. Clin. Oncol. 2007, 25, 5158–5164. [Google Scholar] [CrossRef]
- Shaw, E.; Farris, M.; McNeil, J.; Friedenreich, C. Obesity and Endometrial Cancer. Recent Results Cancer Res. 2016, 208, 107–136. [Google Scholar] [CrossRef]
- Fung-Kee-Fung, M.; Dodge, J.; Elit, L.; Lukka, H.; Chambers, A.; Oliver, T. Follow-up after Primary Therapy for Endometrial Cancer: A Systematic Review. Gynecol. Oncol. 2006, 101, 520–529. [Google Scholar] [CrossRef]
- Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. S2), 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travaglino, A.; Raffone, A.; Stradella, C.; Esposito, R.; Moretta, P.; Gallo, C.; Orlandi, G.; Insabato, L.; Zullo, F. Impact of endometrial carcinoma histotype on the prognostic value of the TCGA molecular subgroups. Arch. Gynecol Obstet. 2020, 301, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Ritterhouse, L.L.; Howitt, B.E. Molecular Pathology. Surg. Pathol. Clin. 2016, 9, 405–426. [Google Scholar] [CrossRef]
- Yu, S.; Shao, H.; Ban, X.; Zhang, H.; You, Y.; Zhou, N.; Mao, X.; Zhao, H.; Chen, J.; Lu, Z. Detection of POLE Subtypes in High-Grade Endometrioid Carcinoma by BaseScope-ISH Assay. Front. Oncol. 2019, 9, 831. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, L.E.; Li, T.; Tone, A.; Aronson, M.; Edwards, M.; Holter, S.; Quevedo, R.; Van De Laar, E.; Lerner-Ellis, J.; Pollett, A.; et al. An Integrative DNA Sequencing and Methylation Panel to Assess Mismatch Repair Deficiency. J. Mol. Diagn. 2021, 23, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Klaus, A.; Birchmeier, W. Wnt Signalling and Its Impact on Development and Cancer. Nat. Rev. Cancer 2008, 8, 387–398. [Google Scholar] [CrossRef]
- Levine, A.J. p53: 800 Million Years of Evolution and 40 Years of Discovery. Nat. Rev. Cancer 2020, 20, 471–480. [Google Scholar] [CrossRef]
- Rathjen, F.; Schachner, M. Immunocytological and Biochemical Characterization of a New Neuronal Cell Surface Component (L1 Antigen) Which Is Involved in Cell Adhesion. EMBO J. 1984, 3, 1–10. [Google Scholar] [CrossRef]
- Zeimet, A.G.; Reimer, D.; Huszar, M.; Winterhoff, B.; Puistola, U.; Azim, S.A.; Müller-Holzner, E.; Ben-Arie, A.; Van Kempen, L.C.; Petru, E.; et al. L1CAM in Early-Stage Type I Endometrial Cancer: Results of a Large Multicenter Evaluation. J. Natl. Cancer Inst. 2013, 105, 1142–1150. [Google Scholar] [CrossRef]
- Handy, D.E.; Castro, R.; Loscalzo, J. Epigenetic Modifications. Circulation 2011, 123, 2145–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurcevic, S.; Olsson, B.; Klinga-Levan, K. MicroRNA Expression in Human Endometrial Adenocarcinoma. Cancer Cell Int. 2014, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, D.; Li, R.; Li, Y.; Zhu, X. Construction of a Competitive Endogenous RNA Network in Uterine Corpus Endometrial Carcinoma. Med. Sci. Monit. 2019, 25, 7998–8010. [Google Scholar] [CrossRef]
- Razavi, Z.S.; Tajiknia, V.; Majidi, S.; Ghandali, M.; Mirzaei, H.R.; Rahimian, N.; Hamblin, M.R.; Mirzaei, H. Gynecologic Cancers and Non-coding RNAs: Epigenetic Regulators with Emerging Roles. Crit. Rev. Oncol. 2021, 157, 103192. [Google Scholar] [CrossRef]
- Bartosch, C.; Lopes, J.M.; Jerónimo, C. Epigenetics in Endometrial Carcinogenesis—Part 1: DNA Methylation. Epigenomics 2017, 9, 737–755. [Google Scholar] [CrossRef]
- Bartosch, C.; Lopes, J.M.; Jerónimo, C. Epigenetics in Endometrial Carcinogenesis—Part 2: Histone Modifications, Chromatin Remodeling and Noncoding RNAs. Epigenomics 2017, 9, 873–892. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Wang, Y.; Meng, Q.; Su, X.; Shen, J.; Wang, J.; He, H.; Wen, B.; Zhang, C.; Xu, M. Integrated Bioinformatic Analysis of a Competing Endogenous RNA Network Reveals a Prognostic Signature in Endometrial Cancer. Front. Oncol. 2019, 9, 448. [Google Scholar] [CrossRef]
- Ala, U. Competing Endogenous RNAs, Non-Coding RNAs and Diseases: An Intertwined Story. Cells 2020, 9, 1574. [Google Scholar] [CrossRef] [PubMed]
- Lou, W.; Ding, B.; Fu, P. Pseudogene-Derived lncRNAs and Their miRNA Sponging Mechanism in Human Cancer. Front. Cell Dev. Biol. 2020, 8, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Cheng, X.; Klimasauskas, S.; Sha, M.; Posfai, J.; Roberts, R.J.; Wilson, G.G. The DNA (cytosine-5) Methyltransferases. Nucleic Acids Res. 1994, 22, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deaton, A.M.; Bird, A. CpG Islands and the Regulation of Transcription. Genes Dev. 2011, 25, 1010–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.; Ren, C.; Yao, Y.; Wang, Q.; Li, F.; Li, Y.; Jiang, A.; Wang, G. Identifying Prognostic Biomarkers in Endometrial Carcinoma Based on Cerna Network. J. Cell. Biochem. 2019, 121, 2437–2446. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, T.; Sun, X.; Wang, Y. Identification of a Potential Prognostic lncRNA-miRNA-mRNA Signature in Endometrial Cancer Based on the Competing Endogenous RNA Network. J. Cell. Biochem. 2019, 120, 18845–18853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Z.-R.; Liu, Q. The LncRNA AL161431.1 Targets miR-1252-5p and Facilitates Cellular Proliferation and Migration via MAPK Signaling in Endometrial Carcinoma. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2294–2302. [Google Scholar] [PubMed]
- Liu, J.; Nie, S.; Liang, J.; Jiang, Y.; Wan, Y.; Zhou, S.; Cheng, W. Competing Endogenous RNA Network of Endometrial Carcinoma: A Comprehensive Analysis. J. Cell. Biochem. 2019, 120, 15648–15660. [Google Scholar] [CrossRef]
- Yu, J.; Jiang, L.; Gao, Y.; Sun, Q.; Liu, B.; Hu, Y.; Han, X. LncRNA CCAT1 Negatively Regulates miR 181a 5p to Promote Endometrial Carcinoma Cell Proliferation and Migration. Exp. Ther. Med. 2019, 17, 4259–4266. [Google Scholar] [CrossRef] [Green Version]
- Treeck, O.; Skrzypczak, M.; Schüler-Toprak, S.; Weber, F.; Ortmann, O. Long Non-coding RNA CCAT1 Is Overexpressed in Endometrial Cancer and Regulates Growth and Transcriptome of Endometrial Adenocarcinoma Cells. Int. J. Biochem. Cell Biol. 2020, 122, 105740. [Google Scholar] [CrossRef]
- Xie, P.; Cao, H.; Li, Y.; Wang, J.; Cui, Z. Knockdown of lncRNA CCAT2 Inhibits Endometrial Cancer Cells Growth and Metastasis via Sponging miR-216b. Cancer Biomark. 2017, 21, 123–133. [Google Scholar] [CrossRef]
- Shang, C.; Ao, C.N.; Cheong, C.C.; Meng, L. Long Non-coding RNA CDKN2B Antisense RNA 1 Gene Contributes to Paclitaxel Resistance in Endometrial Carcinoma. Front. Oncol. 2019, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Zha, J.; Zuo, M.; Yan, Q.; Song, H. Long Noncoding RNA CHL1-AS1 Promotes Cell Proliferation and Migration by Sponging miR-6076 to Regulate CHL1 Expression in Endometrial Cancer. J. Cell. Biochem. 2019, 121, 2655–2663. [Google Scholar] [CrossRef]
- Shen, Q.; He, T.; Yuan, H. Hsa_circ_0002577 Promotes Endometrial Carcinoma Progression via Regulating miR-197/CTNND1 Axis and Activating Wnt/β-Catenin Pathway. Cell Cycle 2019, 18, 1229–1240. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Gong, Z.; Shen, Y.; Fang, Y.; Zhong, S. Circular RNA Expression in Extracellular Vesicles Isolated from Serum of Patients with Endometrial Cancer. Epigenomics 2018, 10, 187–197. [Google Scholar] [CrossRef]
- Liu, Y.; Chang, Y.; Cai, Y. Hsa_circ_0061140 Promotes Endometrial Carcinoma Progression via Regulating miR-149-5p/STAT3. Gene 2020, 745, 144625. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Gao, S.; Lu, C. Knockdown of Differentiation Antagonizing Non-protein Coding RNA Exerts Anti-tumor Effect by up-Regulating miR-214 in Endometrial Carcinoma. Mol. Cell. Biochem. 2019, 460, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Shao, W.; Li, Y.; Chen, F.; Jia, H.; Jia, J.; Fu, Y. Long Non-Coding RNA DLEU1 Contributes to the Development of Endometrial Cancer by Sponging miR-490 to Regulate SP1 Expression. Die Pharm. 2018, 73, 379–385. [Google Scholar]
- Du, Y.; Wang, L.; Chen, S.; Liu, Y.; Zhao, Y. lncRNA DLEU1 Contributes to Tumorigenesis and Development of Endometrial Carcinoma by Targeting mTOR. Mol. Carcinog. 2018, 57, 1191–1200. [Google Scholar] [CrossRef]
- Tanos, V.; Ariel, I.; Prus, D.; De-Groot, N.; Hochberg, A. H19 and IGF2 Gene Expression in Human Normal, Hyperplastic, and Malignant Endometrium. Int. J. Gynecol. Cancer 2004, 14, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Lottin, S.; Adriaenssens, E.; Berteaux, N.; Lepretre, A.; Vilain, M.-O.; Denhez, E.; Coll, J.; Dugimont, T.; Curgy, J.-J. The Human H19 Gene Is Frequently Overexpressed in Myometrium and Stroma during Pathological Endometrial Proliferative Events. Eur. J. Cancer 2005, 41, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Li, Z.; Chen, W.; Zhai, W.; Pan, J.; Pang, H.; Li, X. H19 Promotes Endometrial Cancer Progression by Modulating Epithelial-Mesenchymal Transition. Oncol. Lett. 2017, 13, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wang, D.-L.; Yu, P. LncRNA H19 Regulates the Expression of Its Target Gene HOXA10 in Endometrial Carcinoma through Competing With miR-612. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4820–4827. [Google Scholar]
- Zhu, H.; Jin, Y.-M.; Lyu, X.-M.; Fan, L.-M.; Wu, F. Long Noncoding RNA H19 Regulates HIF-1α/AXL Signaling through Inhibiting miR-20b-5p in Endometrial Cancer. Cell Cycle 2019, 18, 2454–2464. [Google Scholar] [CrossRef]
- Liu, S.; Qiu, J.; Tang, X.; Cui, H.; Zhang, Q.; Yang, Q. LncRNA-H19 Regulates Cell Proliferation and Invasion of Ectopic Endometrium by Targeting ITGB3 via Modulating miR-124-3p. Exp. Cell Res. 2019, 381, 215–222. [Google Scholar] [CrossRef]
- He, X.; Bao, W.; Li, X.; Chen, Z.; Che, Q.; Wang, H.; Wan, X.-P. The Long Non-coding RNA HOTAIR Is Upregulated in Endometrial Carcinoma and Correlates with Poor Prognosis. Int. J. Mol. Med. 2013, 33, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Ke, P.; Guo, L.; Wang, W.; Tan, H.; Liang, Y.; Yao, S. Lentivirus-Mediated RNA Interference Targeting the Long Noncoding RNA HOTAIR Inhibits Proliferation and Invasion of Endometrial Carcinoma Cells In Vitro and In Vivo. Int. J. Gynecol. Cancer 2014, 24, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.-Y.; Zhu, J.-Y.; Zhang, C.-Y.; Zhang, M.; Song, Y.-N.; Rahman, K.; Zhang, L.-J.; Zhang, H. Autophagy Regulated by lncRNA HOTAIR Contributes to the Cisplatin-Induced Resistance in Endometrial Cancer Cells. Biotechnol. Lett. 2017, 39, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.-X.; Wang, C.; Mao, L.-W.; Wang, Y.-L.; Xia, L.-Q.; Zhao, W.; Shen, J.; Chen, J. Long Noncoding RNA HOTAIR Mediates the Estrogen-Induced Metastasis of Endometrial Cancer Cells via the miR-646/NPM1 Axis. Am. J. Physiol. Physiol. 2018, 314, C690–C701. [Google Scholar] [CrossRef] [PubMed]
- Chi, S.; Liu, Y.; Zhou, X.; Feng, D.; Xiao, X.; Li, W.; Zhao, Y.; Wang, H. Knockdown of Long Non-coding HOTAIR Enhances the Sensitivity to Progesterone in Endometrial Cancer by Epigenetic Regu-Lation of Progesterone Receptor Isoform, B. Cancer Chemother. Pharmacol. 2019, 83, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-H.; Hu, P.; Xie, Y.-Q.; Kang, Y.-J.; Li, M. Long Noncoding RNA HOTAIR Promotes Endometrial Carcinoma Cell Proliferation by Binding to PTEN via the Activating Phosphatidylinositol 3-Kinase/Akt Signaling Pathway. Mol. Cell. Biol. 2019, 39, e00251-19. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Pang, L.; Yang, Z.; Liu, J.; Li, W.; Wang, D. LncRNA HOTAIRM1/HOXA1 Axis Promotes Cell Proliferation, Migration and Invasion in Endometrial Cancer. OncoTargets Ther. 2019, 12, 10997–11015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Qiu, M.; Jiang, L.; Liu, K. Long Noncoding RNA HOXB-AS1 Is Upregulated in Endometrial Carcinoma and Sponged miR-149-3p to Upregulate Wnt10b. Technol. Cancer Res. Treat. 2020, 19, 153303382096746. [Google Scholar] [CrossRef]
- Pan, X.; Li, D.; Huo, J.; Kong, F.; Yang, H.; Ma, X. LINC01016 Promotes the Malignant Phenotype of Endometrial Cancer Cells by Regulating the miR-302a-3p/miR-3130-3p/NFYA/SATB1. Cell Death Dis. 2018, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Ding, N.; Zhuang, S.; Li, Y. LINC01410/miR-23c/CHD7 Functions as a ceRNA Network to Affect the Prognosis of Patients with Endometrial Cancer and Strengthen the Malignant Properties of Endometrial Cancer Cells. Mol. Cell. Biochem. 2020, 469, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Gao, Q.; Wang, J.; Zhang, X.; Liu, K.; Duan, Z. Linc-RNA-RoR Acts as a “Sponge” against Mediation of the Differentiation of Endometrial Cancer Stem Cells by microRNA-145. Gynecol. Oncol. 2014, 133, 333–339. [Google Scholar] [CrossRef]
- Liu, Y.; Chang, Y.; Cai, Y.-X. Inhibition of Lnc-OC1 Induced Cell Apoptosis and Decreased Cell Viability by Releasing miR-34a and Inhibiting PD-L1 in Endometrial Carcinoma. Reprod. Sci. 2020, 27, 1848–1856. [Google Scholar] [CrossRef]
- Zheng, X.; Liu, M.; Song, Y.; Feng, C. Long Noncoding RNA-ATB Impairs the Function of Tumor Suppressor miR-126-Mediated Signals in Endometrial Cancer for Tumor Growth and Metastasis. Cancer Biother. Radiopharm. 2019, 34, 47–55. [Google Scholar] [CrossRef]
- Yang, X.; Xing, G.; Liu, S.; Li, B.; He, Y.; Wang, F. LncRNA LOXL1-AS1 Promotes Endometrial Cancer Progression by Sponging miR-28-5p to Upregulate RAP1B Expression. BioMed. Pharmacother. 2020, 125, 109839. [Google Scholar] [CrossRef]
- Wang, W.; Ge, L.; Xu, X.-J.; Yang, T.; Yuan, Y.; Ma, X.-L.; Zhang, X.-H. LncRNA NEAT1 Promotes Endometrial Cancer Cell Proliferation, Migration and Invasion by Regulating the miR-144-3p/EZH2 Axis. Radiol. Oncol. 2019, 53, 434–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, P.; Xiong, Y.; Yue, J.; Xu, D.; Ihira, K.; Konno, Y.; Kobayashi, N.; Todo, Y.; Watari, H. Long Noncoding RNA NEAT1 Drives Aggressive Endometrial Cancer Progression via Mir-361-Regulated Networks Involving STAT3 and Tumor Microenvi-Ronment-Related Genes. J. Exp. Clin. Cancer Res. 2019, 38, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Zhong, R.; He, X.; Deng, Q.; Peng, X.; Li, J.; Luo, X. Investigations on the Mechanism of Progesterone in Inhibiting Endometrial Cancer Cell Cycle and Viability via Regulation of Long Noncoding RNA NEAT1/microRNA-146b-5p Mediated Wnt/β-catenin signaling. IUBMB Life 2019, 71, 223–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Zhao, S.; Mingxin, Y.U. LncRNA NR2F1-AS1 Is Involved in the Progression of Endometrial Cancer by Sponging miR-363 to target SOX4. Die Pharm. 2019, 74, 295–300. [Google Scholar]
- Li, Q.; Shen, F.; Zhao, L. The Relationship between lncRNA PCGEM1 and STAT3 During the Occurrence and Development of Endometrial Carcinoma. BioMed. Pharmacother. 2018, 107, 918–928. [Google Scholar] [CrossRef]
- Kong, F.; Ma, J.; Yang, H.; Yang, D.; Wang, C.; Ma, X. Long Non-Coding RNA PVT1 Promotes Malignancy in Human Endometrial Carcinoma Cells through Negative Regulation of miR-195-5p. Biochim. Biophys. Acta Bioenerg. 2018, 1865, 1479–1490. [Google Scholar] [CrossRef] [PubMed]
- Xing, T.-R.; Chen, P.; Wu, J.-M.; Gao, L.-L.; Yang, W.; Cheng, Y.; Tong, L.-B. UPF1 Participates in the Progression of Endometrial Cancer by Inhibiting the Expression of lncRNA PVT1. Onco Targets Ther. 2020, 13, 2103–2114. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Nie, X.; Zhang, W.; Gou, R.; Hu, Y.; Qi, Y.; Li, X.; Liu, Q.; Liu, J.; Lin, B. Identification of Long Noncoding RNA RP11-89K21.1 and RP11-357H14.17 as Prognostic Signature of Endometrial Carcinoma via Integrated Bioinformatics Analysis. Cancer Cell Int. 2020, 20, 268. [Google Scholar] [CrossRef]
- Zhang, G.; Ma, A.; Jin, Y.; Pan, G.; Wang, C. LncRNA SNHG16 Induced by TFAP2A Modulates Glycolysis and Proliferation of Endometrial Carcinoma Through miR-490-3p/HK2. Am. J. Transl. Res. 2019, 11, 7137–7145. [Google Scholar]
- Yang, C.-H.; Zhang, X.-Y.; Zhou, L.-N.; Wan, Y.; Song, L.-L.; Gu, W.-L.; Liu, R.; Ma, Y.-N.; Meng, H.-R.; Tian, Y.-L.; et al. LncRNA SNHG8 Participates in the Development of Endometrial Carcinoma through Regulating c-MET Expression by miR-152. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1629–1637. [Google Scholar]
- Liu, L.; Chen, X.; Zhang, Y.; Hu, Y.; Shen, X.; Zhu, W. Long Non-Coding RNA TUG1 Promotes Endometrial Cancer Development via Inhibiting miR-299 and miR-34a-5p. Oncotarget 2017, 8, 31386–31394. [Google Scholar] [CrossRef]
- Ke, J.; Shen, Z.; Hu, W.; Li, M.; Shi, Y.; Xie, Z.; Wu, D. LncRNA DCST1-AS1 Was Upregulated in Endometrial Carcinoma and May Sponge miR-92a-3p to Upregulate Notch1. Cancer Manag. Res. 2020, 12, 1221–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, Y.; Ren, Z. Overexpression of LncRNA FER1L4 in Endometrial Carcinoma Is Associated with Favorable Survival Out-come. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8113–8118. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Song, W.-Q.; Sun, P.; Jin, L.; Dai, H.-Y. LncRNA-GAS5 Induces PTEN Expression through Inhibiting miR-103 in Endometrial Cancer Cells. J. BioMed. Sci. 2015, 22, 100. [Google Scholar] [CrossRef] [Green Version]
- Xin, W.; Zhao, S.; Han, X.; Zhao, P.; Yu, H.; Gao, X.; Li, P.; Wu, Q.; Ding, J.; Hua, K. lncRNA LA16c-313D11.11 Modulates the Development of Endometrial Cancer by Binding to and Inhibiting microRNA 205 5p Function and Indirectly in-Creasing PTEN activity. Int. J. Oncol. 2020, 57, 355–363. [Google Scholar] [CrossRef]
- Fang, Q.; Sang, L.; Du, S. Long Noncoding RNA LINC00261 Regulates Endometrial Carcinoma Progression by Modulating miRNA/FOXO1 Expression. Cell Biochem. Funct. 2018, 36, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Sun, Y.; Ma, Z.; Xu, X.; Qin, L.; Luo, B. LOC134466 Methylation Promotes Oncogenesis of Endometrial Carcinoma Through LOC134466/hsa-miR-196a-5p/TAC1 axis. Aging 2018, 10, 3353–3370. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, C.; Chen, R.; Xiong, H.; Qiu, F.; Liu, S.; Zhang, M.; Wang, F.; Wang, Y.; Zhou, X.; et al. Disrupting MALAT1/miR-200c Sponge Decreases Invasion and Migration in Endometrioid Endometrial Carcinoma. Cancer Lett. 2016, 383, 28–40. [Google Scholar] [CrossRef]
- Shi, F.; Wang, T.; Liu, Z.; Zhang, Y.; Wang, J.; Zhang, K.; Su, J. LncRNA miR143HG Up-Regulates p53 In Endometrial Carcinoma by Sponging miR-125a. Cancer Manag. Res. 2019, 11, 10117–10123. [Google Scholar] [CrossRef] [Green Version]
- Cui, Z.; An, X.; Li, J.; Liu, Q.; Liu, W. LncRNA MIR22HG Negatively Regulates miR-141-3p to Enhance DAPK1 Expression and Inhibits Endometrial Carcinoma Cells Proliferation. BioMed. Pharmacother. 2018, 104, 223–228. [Google Scholar] [CrossRef]
- Zhou, Y.-X.; Zhao, W.; Mao, L.-W.; Wang, Y.-L.; Xia, L.-Q.; Cao, M.; Shen, J.; Chen, J. Long Non-Coding RNA NIFK-AS1 Inhibits M2 Polarization of Macrophages in Endometrial Cancer through Targeting miR-146a. Int. J. Biochem. Cell Biol. 2018, 104, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.; Gao, X.; Zhao, S.; Zhao, P.; Yu, H.; Wu, Q.; Hua, K. LncRNA RP11-395G23.3 Suppresses the Endometrial Cancer Progression via Regulating microRNA-205-5p/PTEN axis. Am. J. Transl. Res. 2020, 12, 4422–4433. [Google Scholar]
- Li, S.; Shan, Y.; Li, X.; Zhang, C.; Wei, S.; Dai, S.; Zhao, R.; Zhao, X.; Zhao, L.; Shan, B. lncRNA SNHG5 Modulates Endometrial Cancer Progression via the miR-25-3p/BTG2 Axis. J. Oncol. 2019, 2019, 7024675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, C.; Lang, B.; Ao, C.N.; Meng, L. Long Non-Coding RNA Tumor Suppressor Candidate 7 Advances Chemotherapy Sensitivity of Endometrial Carcinoma through Targeted Silencing of miR-23b. Tumor Biol. 2017, 39, 1010428317707883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Cai, D.; Zhang, F.; Li, M.; Wan, Q. Long Noncoding RNA TUSC7 Inhibits Cell Proliferation, Migration and Invasion by Regulating SOCS4 (SOCS5) Expression through Targeting miR-616 in Endometrial Carcinoma. Life Sci. 2019, 231, 116549. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y.; Guan, Y.; Li, H.; Liu, Y.; Zhang, M.; Cui, P.; Kong, D.; Chen, X.; Yin, H. Integrated analysis of immune-related genes in endometrial carcinoma. Cancer Cell Int. 2020, 20, 477. [Google Scholar] [CrossRef]
- Tang, H.; Wu, Z.; Zhang, Y.; Xia, T.; Liu, D.; Cai, J.; Ye, Q. Identification and Function Analysis of a Five-Long Noncoding RNA Prognostic Signature for Endometrial Cancer Patients. DNA Cell Biol. 2019, 38, 1480–1498. [Google Scholar] [CrossRef]
- Zhao, X.; Fan, Y.; Lu, C.; Li, H.; Zhou, N.; Sun, G.; Fan, H. PCAT1 is a poor prognostic factor in endometrial carcinoma and associated with cancer cell proliferation, migration and invasion. Bosn. J. Basic Med. Sci. 2019, 19, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, S.K.D.; Rao, G.; Dey, A.; Mukherjee, P.; Wren, J.D.; Bhattacharya, R. Small Non-Coding-RNA in Gynecological Malignancies. Cancers 2021, 13, 1085. [Google Scholar] [CrossRef]
- Miki, Y. New Insights into Breast and Endometrial Cancers. Cancers 2020, 12, 2595. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| FIGO Stage | Tumor Spread |
|---|---|
| Stage I | The tumor is limited to the uterus (it can affect the glands of the cervix and isthmus but not the cervical stroma) |
| IA | Myometrial invasion <50% of its full thickness |
| IB | Myometrial invasion >50% of its full thickness |
| Stage II | The tumor involves the cervical stroma (it does not invade tissues outside the uterus) |
| Stage III | The tumor has spread outside the uterus (it does not involve the rectum or bladder) |
| IIIA | Uterine serosa and/or adnexa invasion |
| IIIB | Vagina and/or parametrial invasion |
| IIIC | Lymph nodes involvement |
| IIIC1 | Pelvic lymph nodes involvement |
| IIIC2 | Para-aortic lymph nodes involvement |
| Stage IV | The tumor has spread to rectum, bladder or distant locations |
| IVA | Rectum and/or bladder invasion |
| IVB | Distant site metastasis |
| Risk Category | Risk Factor Status |
|---|---|
| Low | FIGO Stage I |
| Endometrioid histotype | |
| grade 1–2 | |
| <50% myometrial invasion | |
| LVSI negative | |
| Intermediate | FIGO Stage I |
| Endometrioid histotype | |
| grade 1–2 | |
| ≥50% myometrial invasion | |
| LVSI negative | |
| High-intermediate | FIGO Stage I |
| Endometrioid histotype | |
| grade 3 | |
| <50% myometrial invasion | |
| regardless of LVSI status | |
| OR | |
| FIGO Stage I | |
| Endometrioid histotype | |
| grade 1–2 | |
| LVSI unequivocally positive | |
| regardless of depth of invasion | |
| High | FIGO Stage I |
| Endometrioid histotype | |
| grade 3 | |
| ≥50% myometrial invasion | |
| regardless of LVSI status | |
| OR | |
| FIGO Stage II | |
| OR | |
| FIGO Stage III | |
| Endometrioid histotype | |
| no residual disease | |
| OR | |
| Non-endometrioid histotype | |
| (serous, clear-cell, undifferentiated carcinoma or carcinosarcoma) | |
| Advanced | FIGO Stage III |
| residual disease | |
| OR | |
| Stage IVA | |
| Metastatic | FIGO Stage IVB |
| ncRNA Name | Exp. | Function | miR Interactions | Mechanism | Refs. |
|---|---|---|---|---|---|
| AL161431.1 | up | oncogene | miR-1252-5p | a | [37] |
| C2orf48 | up | oncogene | miR-183 | n/a | [38] |
| CCAT1 | up | oncogene | miR-181a-5p | n/a | [39,40] |
| CCAT2 | up | oncogene | miR-216b | a; c | [41] |
| CDKN2B-AS | up | oncogene | miR-125a-5p | d | [42] |
| CHL1-AS1 | up | oncogene | miR-6076 | n/a | [43] |
| circ_0002577 | up | oncogene | miR-197 | a; b; e | [44,45] |
| circ_0061140 * | up | oncogene | miR-149-5p | a | [46] |
| DANCR | up | oncogene | miR-214 | b | [47] |
| DLEU1 | up | oncogene | miR-490 | b; e | [48,49] |
| H19 | up | oncogene | miR-20b-5p; miR-124-3p; miR-612 | a; b; c; e | [50,51,52,53,54,55] |
| HOTAIR * | up | oncogene | miR-646 | b; f | [56,57,58,59,60,61,62] |
| HOXB-AS1 | up | oncogene | miR-149-3p | a; c | [63] |
| LINC00483 | up | oncogene | miR-183; miR-192 | b | [38] |
| LINC00958 | up | oncogene | miR-761 | c | [36] |
| LINC01016 | up | oncogene | miR-302a-3p; miR-3130-3p | n/a | [64] |
| LINC01410 | up | oncogene | miR-23c | a; b | [65] |
| LINC-ROR | up | oncogene | miR-145 | n/a | [66] |
| lnc-OC1 | up | oncogene | miR-34a | b | [67] |
| lncRNA-ATB | up | oncogene | miR-126 | a; b; e | [68] |
| LOXL1-AS1 | up | oncogene | miR-28-5p | a; b | [69] |
| NEAT1 | up | oncogene | miR-361; miR-144-3p; miR-146b-5p | a | [70,71,72] |
| NR2F1-AS1 | up | oncogene | miR-363 | a; b; c | [73] |
| PCGEM1 | up | oncogene | miR-129-5p | a; c; b | [74] |
| PVT1 * | up | oncogene | miR-195-5p | a; b | [75,76] |
| RP11-357H14.17 | up | oncogene | miR-24-1-5p; miR-27b; miR-143; miR-204; miR-503; miR-4770 | n/a | [77] |
| RP11-89K21.1 | up | oncogene | miR-27b; miR-4770; miR-143; miR-204; miR-125a-5p; miR-125b-5p; miR-139-5p; miR-670-3p | n/a | [77] |
| SNHG16 | up | oncogene | miR-490-3p | a | [78] |
| SNHG8 | up | oncogene | miR-152 | a | [79] |
| TUG1 | up | oncogene | miR-34a-5p; miR-299 | n/a | [80] |
| ncRNA Name | Exp. | Function | miR Interactions | Mechanism | Refs. |
|---|---|---|---|---|---|
| circ_0061140 * | down | tumor suppressor | miR-149-5p | a | [46] |
| DCST1-AS1 | down | tumor suppressor | miR-92a-3p | c | [81] |
| GAS5 | down | tumor suppressor | miR-103; miR-222-3p | b | [82,83] |
| HOTAIR * | down | tumor suppressor | miR-646 | b; f | [56,57,58,59,60,61,62] |
| LA16c-313D11.11 | down | tumor suppressor | miR-205-5p | a; c | [84] |
| LINC00261 | down | tumor suppressor | miR-27a; miR-96; miR-153; miR-182; miR-183 | a; c | [85] |
| LOC134466 | down | tumor suppressor | miR-196a-5p | b | [86] |
| MALAT1 | down | tumor suppressor | miR-200c | c; e | [87] |
| miR143HG | down | tumor suppressor | miR-125a | b | [88] |
| MIR22HG | down | tumor suppressor | miR-141-3p | a; b | [89] |
| NIFK-AS1 | down | tumor suppressor | miR-146a | a | [90] |
| PVT1 * | down | tumor suppressor | miR-195-5p | a; b | [78,79] |
| RP11-395G23.3 | down | tumor suppressor | miR-205-5p | a; c | [91] |
| SNHG5 | down | tumor suppressor | miR-25-3p | a; c | [92] |
| TUSC7 | down | tumor suppressor | miR-23b; miR-616 | a; e | [93,94] |
| ncRNA Name | Exp. | Function | Deregulation-Related Prognosis | Author | Year | Refs. |
|---|---|---|---|---|---|---|
| AC074212.1 | up | oncogene | poor | Wang, Y. | 2020 | [95] |
| AC110491.1 * | n/a down | n/a tumor suppressor | poor good | Ouyang, D. Liu, J. | 2019 2019 | [26,38] |
| ADARB2-AS1 ^ | n/a n/a | n/a n/a | poor poor | Ouyang, D. Xia, L. | 2019 2019 | [26,30] |
| AL596188.1 | n/a | n/a | good | Ouyang, D. | 2019 | [26] |
| C2orf48 ^ | n/a up | n/a oncogene | poor poor | Ouyang, D. Liu, J. | 2019 2019 | [26,38] |
| C8orf49 | n/a | n/a | poor | Xia, L. | 2019 | [30] |
| C10orf91 | n/a | n/a | poor | Ouyang, D. | 2019 | [26] |
| FER1L4 | down | tumor suppressor | poor | Kong, Y. | 2018 | [82] |
| FP671120.4 | up | oncogene | poor | Wang, Y. | 2020 | [95] |
| GLIS3-AS1 | n/a | n/a | poor | Ouyang, D. | 2019 | [26] |
| HOXB-AS1 | up | oncogene | poor | Liu, D. | 2020 | [63] |
| KCNMB2-AS1 | up | oncogene | good | Tang, H. | 2019 | [96] |
| LA16c-313D11.11 | down | tumor suppressor | good | Xin, W. | 2020 | [84] |
| LINC00237 | n/a | n/a | good | Ouyang, D. | 2019 | [26] |
| LINC00261 * | up down | oncogene tumor suppressor | good poor | Ouyang, D. Zhao, D. | 2019 2019 | [26,35] |
| LINC00475 | down | tumor suppressor | good | Tang, H. | 2019 | [96] |
| LINC00483 ^ | up n/a | oncogene n/a | poor poor | Liu, J. Xia, L. | 2019 2019 | [30,38] |
| LINC00491 ^ | n/a n/a | n/a n/a | poor poor | Xia, L. Ouyang, D. | 2019 2019 | [26,30] |
| LINC00958 | up | oncogene | good | Wang, Y. | 2019 | [36] |
| LINC01143 | up | oncogene | poor | Tang, H. | 2019 | [96] |
| LINC01352 | down | tumor suppressor | poor | Tang, H. | 2019 | [96] |
| LINC01410 | up | oncogene | poor | Lu, M. | 2020 | [65] |
| LINC02381 | up | oncogene | poor | Wang, Y. | 2020 | [95] |
| LNCTAM34A | down | tumor suppressor | good | Wang, Y. | 2020 | [95] |
| MIR503HG | down | tumor suppressor | poor | Tang, H. | 2019 | [96] |
| PCAT1 | up | oncogene | poor | Zhao, X. | 2019 | [97] |
| RP11-357H14.17 | up | oncogene | poor | Gao, L. | 2020 | [77] |
| RP11-89K21.1 | up | oncogene | poor | Gao, L. | 2020 | [77] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavaliere, A.F.; Perelli, F.; Zaami, S.; Piergentili, R.; Mattei, A.; Vizzielli, G.; Scambia, G.; Straface, G.; Restaino, S.; Signore, F. Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare 2021, 9, 965. https://doi.org/10.3390/healthcare9080965
Cavaliere AF, Perelli F, Zaami S, Piergentili R, Mattei A, Vizzielli G, Scambia G, Straface G, Restaino S, Signore F. Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare. 2021; 9(8):965. https://doi.org/10.3390/healthcare9080965
Chicago/Turabian StyleCavaliere, Anna Franca, Federica Perelli, Simona Zaami, Roberto Piergentili, Alberto Mattei, Giuseppe Vizzielli, Giovanni Scambia, Gianluca Straface, Stefano Restaino, and Fabrizio Signore. 2021. "Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer" Healthcare 9, no. 8: 965. https://doi.org/10.3390/healthcare9080965
APA StyleCavaliere, A. F., Perelli, F., Zaami, S., Piergentili, R., Mattei, A., Vizzielli, G., Scambia, G., Straface, G., Restaino, S., & Signore, F. (2021). Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare, 9(8), 965. https://doi.org/10.3390/healthcare9080965