
Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search
2.4. Search Strategy
(((“strength training” [Title/Abstract] OR “resistance training” [Title/Abstract] OR “weight training” [Title/Abstract] OR “plyometric*” [Title/Abstract] OR “calisthenics” [Title/Abstract]) AND (“flexibility” [Title/Abstract] OR “stretching” [Title/Abstract])) AND (“range of motion” [Title/Abstract])) AND (“random*” [Title/Abstract]).
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
2.8. Risk of Bias in Individual Studies
2.9. Summary Measures
2.10. Synthesis of Results
2.11. Risk of Bias Across Studies
2.12. Moderator Analyses
2.13. Quality and Confidence in Findings
3. Results
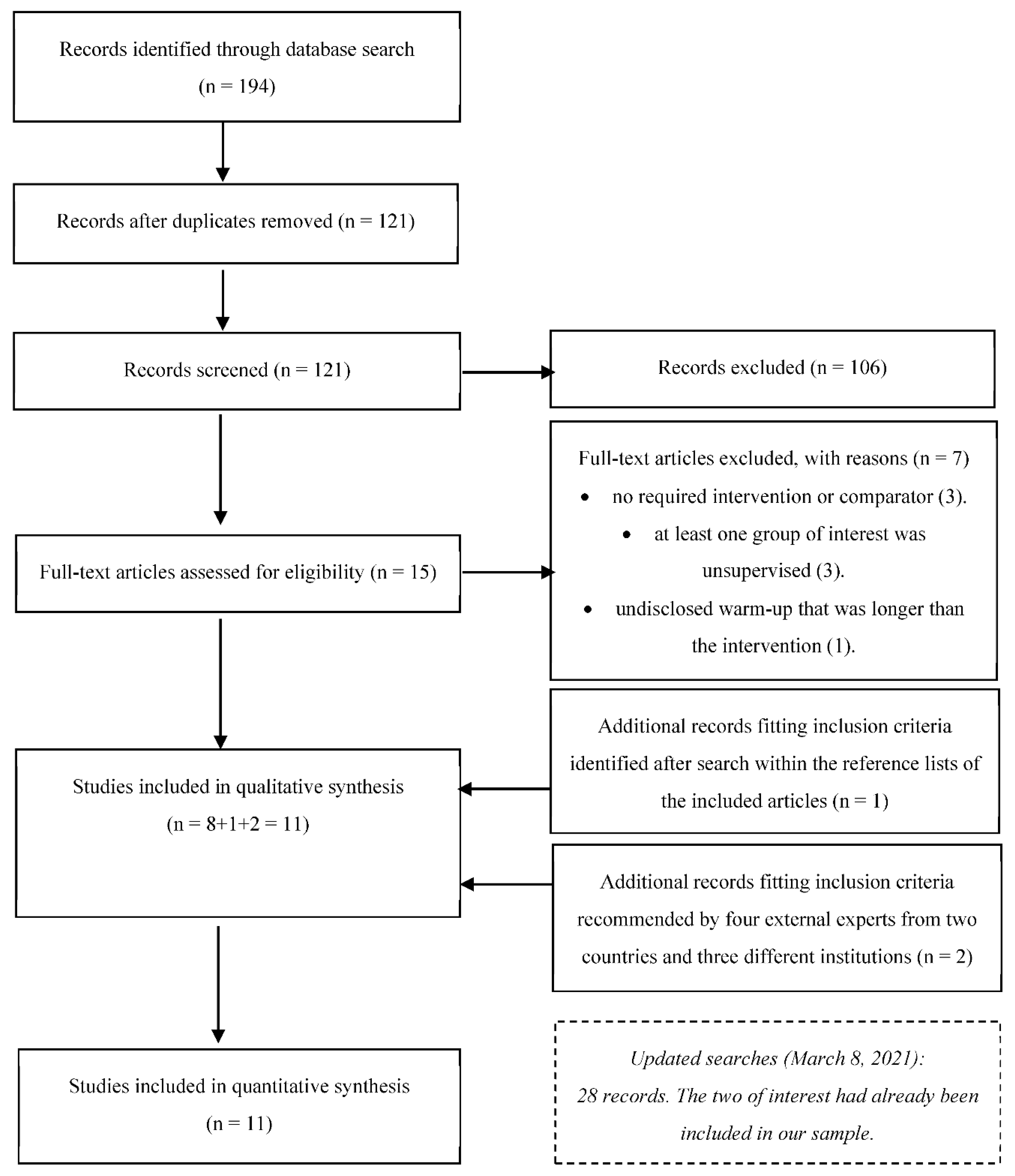
3.1. Study Selection
3.2. Study Characteristics and Results
3.3. Risk of Bias in Individual Studies
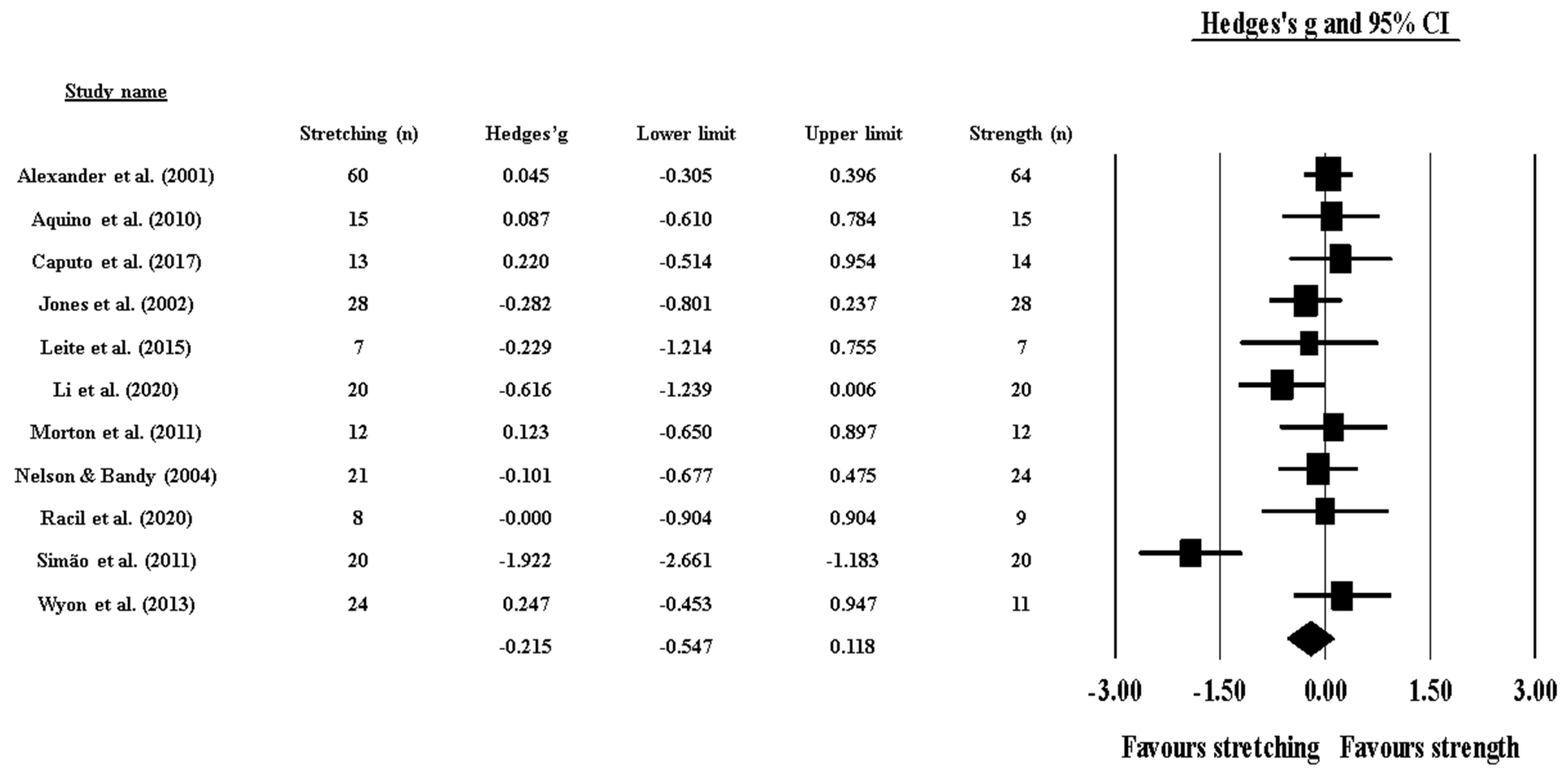
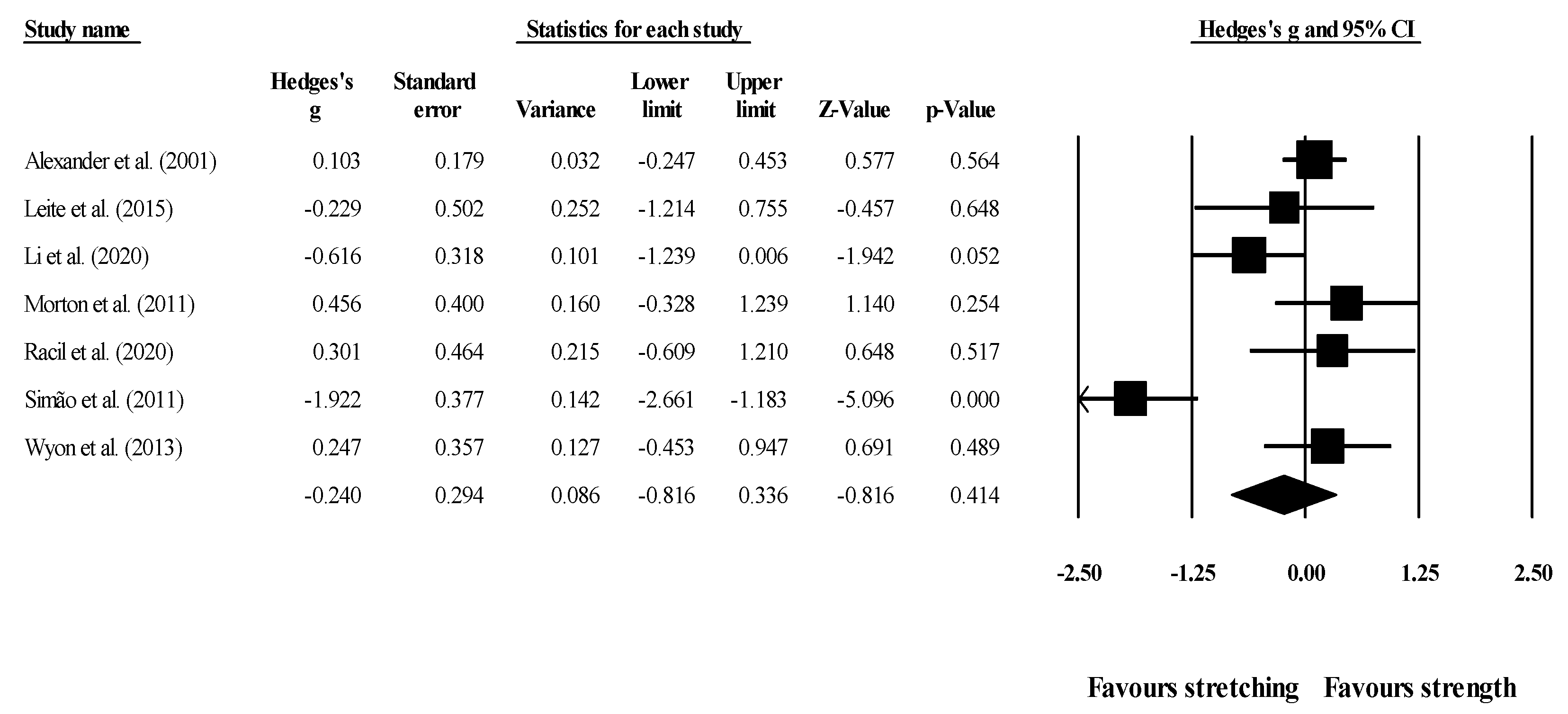
3.4. Synthesis of Results
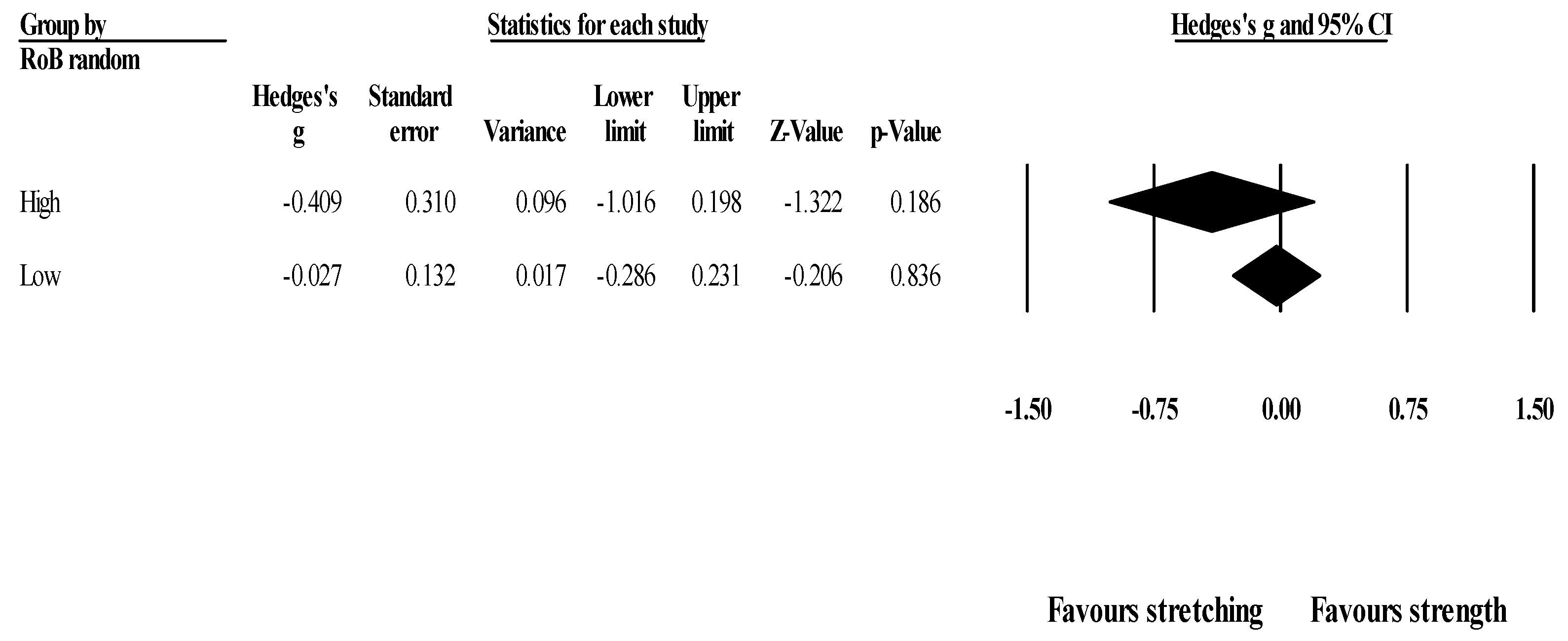
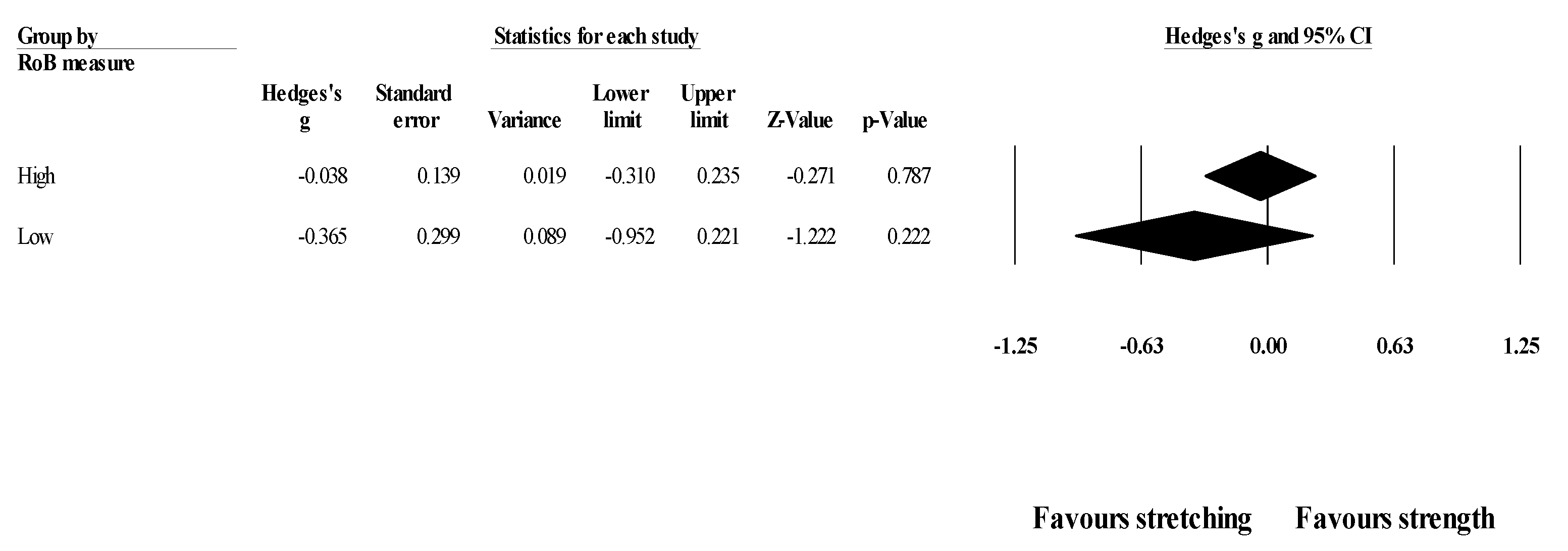
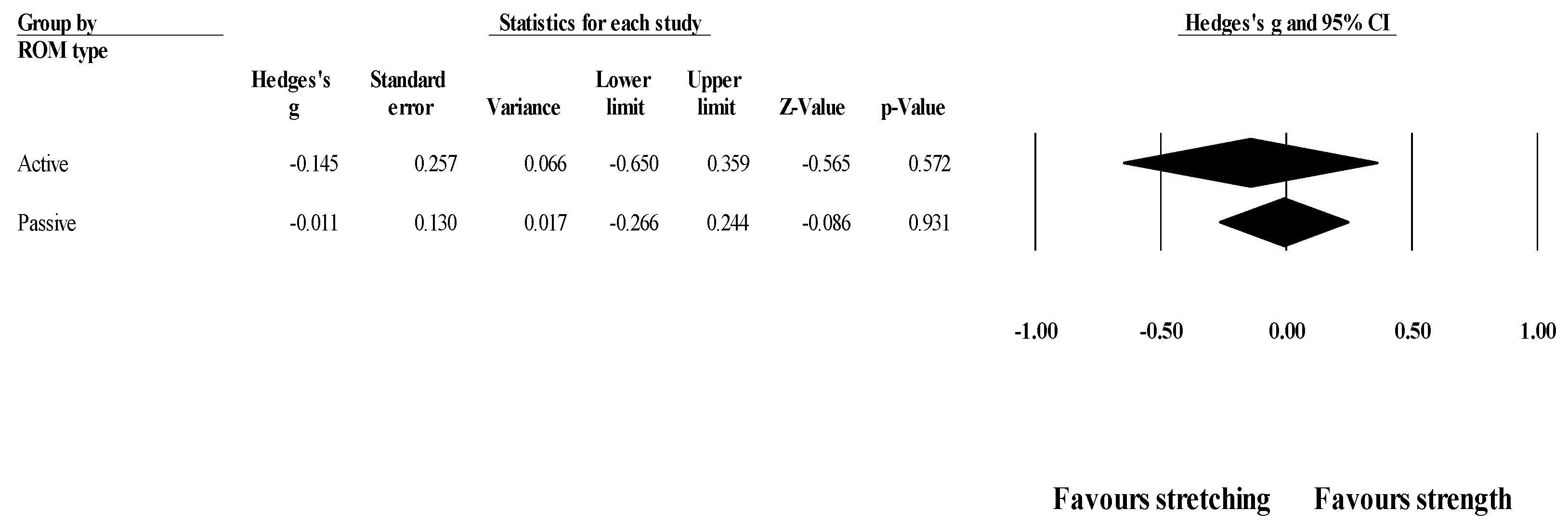
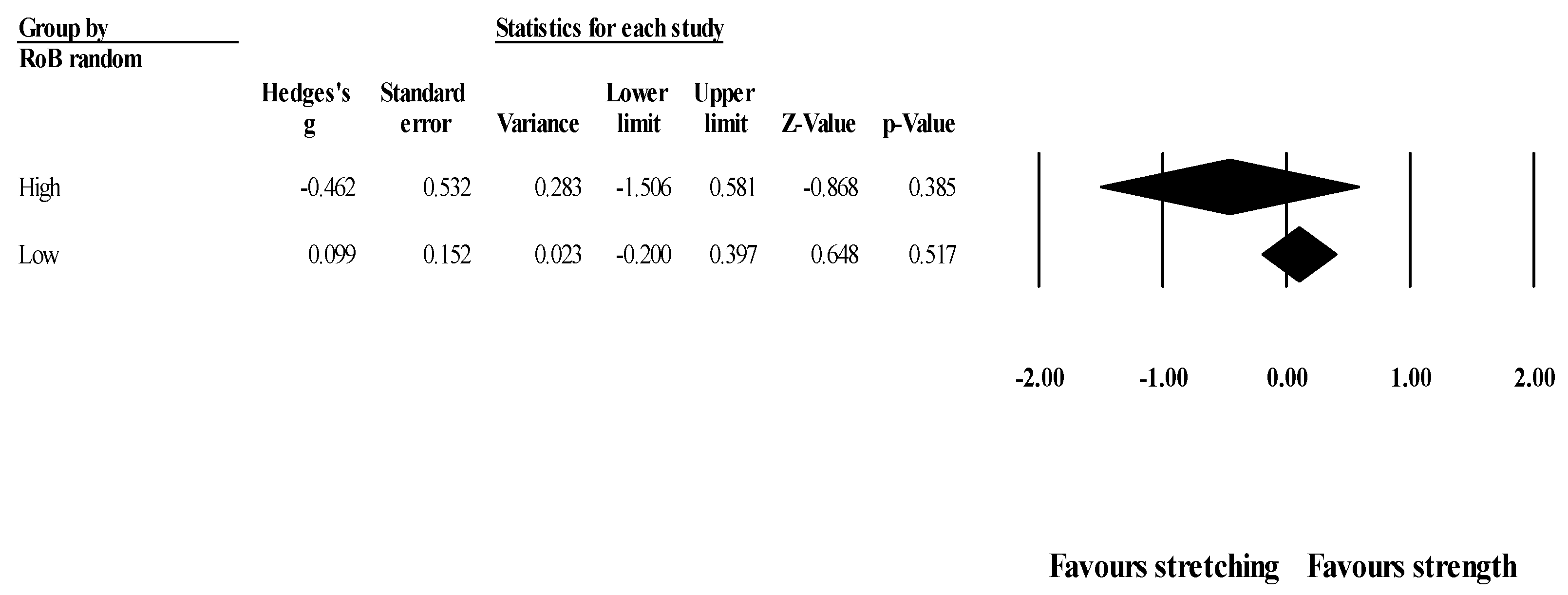
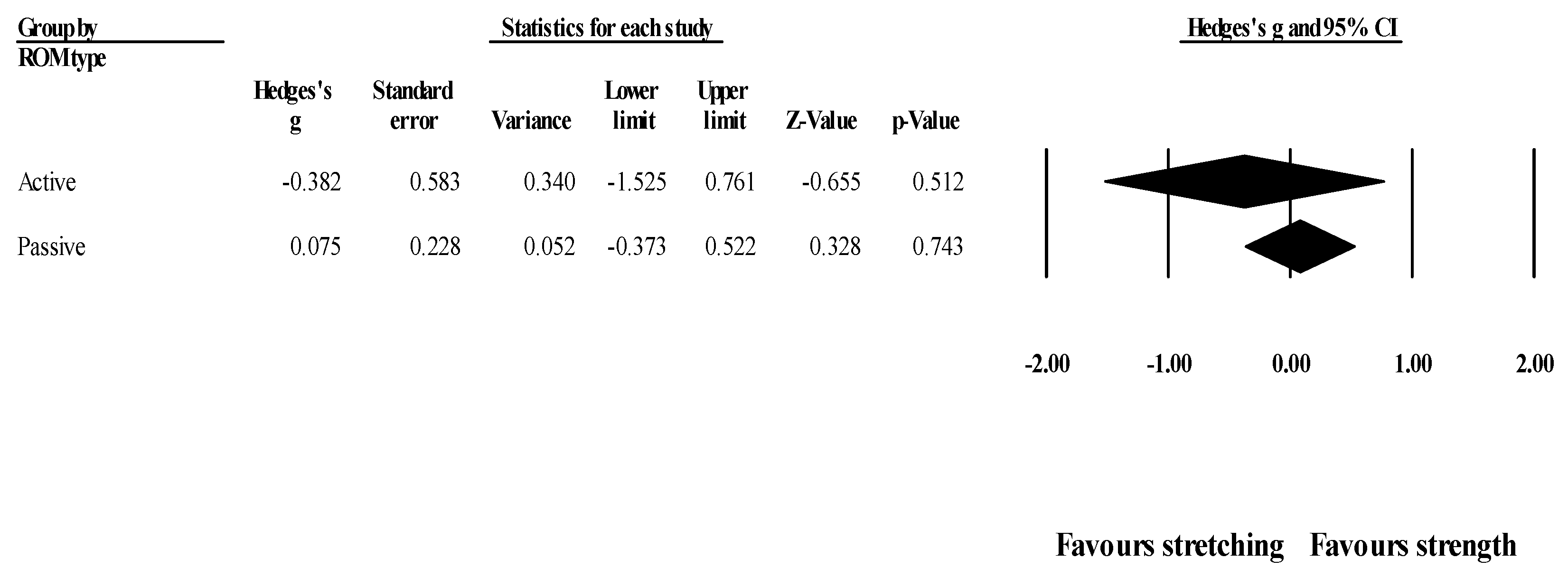
3.5. Additional Analyses
3.6. Confidence in Cumulative Evidence
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kent, M. The Oxford Dictionary of Sports Science & Medicine, 3rd ed.; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Bayles, M.P., Swank, A.M., Eds.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2018. [Google Scholar]
- De Zoete, R.M.; Armfield, N.R.; McAuley, J.H.; Chen, K.; Sterling, M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: A systematic review with network meta-analysis of 40 randomised controlled trials. Br. J. Sports Med. 2020. [Google Scholar] [CrossRef]
- Morris, P.E.; Berry, M.J.; Files, D.C.; Thompson, J.C.; Hauser, J.; Flores, L.; Dhar, S.; Chmelo, E.; Lovato, J.; Case, L.D.; et al. Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure: A randomized clinical trial. JAMA 2016, 315, 2694–2702. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.M.; Wolters, P.L.; Dombi, E.; Baldwin, A.; Whitcomb, P.; Fisher, M.J.; Weiss, B.; Kim, A.; Bornhorst, M.; Shah, A.C.; et al. Selumetinib in children with inoperable plexiform neurofibromas. N. Engl. J. Med. 2020, 382, 1430–1442. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, S.; Haddad, C.A.S.; Giron, P.S.; Figueira, P.V.G.; Estevão, A.; Elias, S.; Nazário, A.C.P.; Facina, G. Exercise protocol with limited shoulder range of motion for 15 or 30 days after conservative surgery for breast cancer with oncoplastic technique: A randomized clinical trial. Am. J. Clin. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Mou, P.; Zeng, W.N.; Chen, Y.; Zhou, Z. Synchronous or sequential cementless bilateral total hip arthroplasty for osseous ankylosed hips with ankylosing spondylitis. BMC Musculoskelet. Disord. 2021, 22, 302. [Google Scholar] [CrossRef]
- Bekteshi, S.; Vanmechelen, I.; Konings, M.; Ortibus, E.; Feys, H.; Monbaliu, E. Clinical presentation of spasticity and passive range of motion deviations in dyskinetic cerebral palsy in relation to dystonia, choreoathetosis, and functional classification systems. Dev. Neurorehabil. 2021, 24, 205–213. [Google Scholar] [CrossRef]
- Lloyd Morris, E.H.; Estilow, T.; Glanzman, A.M.; Cusack, S.V.; Yum, S.W. Improving temporomandibular range of motion in people with duchenne muscular dystrophy and spinal muscular atrophy. Am. J. Occup. Ther. 2020, 74. [Google Scholar] [CrossRef]
- Benner, R.W.; Shelbourne, K.D.; Bauman, S.N.; Norris, A.; Gray, T. Knee osteoarthritis: Alternative range of motion treatment. Orthop. Clin. N. Am. 2019, 50, 425–432. [Google Scholar] [CrossRef]
- Kojima, T.; Ishikawa, H.; Tanaka, S.; Haga, N.; Nishida, K.; Yukioka, M.; Hashimoto, J.; Miyahara, H.; Niki, Y.; Kimura, T.; et al. Characteristics of functional impairment in patients with long-standing rheumatoid arthritis based on range of motion of joints: Baseline data from a multicenter prospective observational cohort study to evaluate the effectiveness of joint surgery in the treat-to-target era. Mod. Rheumatol. 2018, 28, 474–481. [Google Scholar] [CrossRef]
- Pozzi, F.; Plummer, H.A.; Shanley, E.; Thigpen, C.A.; Bauer, C.; Wilson, M.L.; Michener, L.A. Preseason shoulder range of motion screening and in-season risk of shoulder and elbow injuries in overhead athletes: Systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, V.; del Coso, J.; Raya-González, J.; Nakamura, F.Y.; Castillo, D. Effects of basketball match-play on ankle dorsiflexion range of motion and vertical jump performance in semi-professional players. J. Sports Med. Phys. Fit. 2020, 60, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Downs, J.; Wasserberger, K.; Oliver, G.D. Influence of a pre-throwing protocol on range of motion and strength in baseball athletes. Int. J. Sports Med. 2020. [Google Scholar] [CrossRef]
- Li, Y.; Koldenhoven, R.M.; Jiwan, N.C.; Zhan, J.; Liu, T. Trunk and shoulder kinematics of rowing displayed by Olympic athletes. Sports Biomech. 2020. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, A.; Cannavan, D.; Waugh, C.M.; Miller, S.C.; Thorlund, J.B.; Aagaard, P.; Kay, A.D. Range of motion, neuromechanical, and architectural adaptations to plantar flexor stretch training in humans. J. Appl. Physiol. 2014, 117, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Guissard, N.; Duchateau, J. Effect of static stretch training on neural and mechanical properties of the human plantar-flexor muscles. Muscle Nerve 2004, 29, 248–255. [Google Scholar] [CrossRef]
- Lima, C.D.; Brown, L.E.; Li, Y.; Herat, N.; Behm, D. Periodized versus non-periodized stretch training on gymnasts flexibility and performance. Int. J. Sports Med. 2019, 40, 779–788. [Google Scholar] [CrossRef]
- Behm, D.G.; Kay, A.D.; Trajano, G.S.; Blazevich, A.J. Mechanisms underlying performance impairments following prolonged static stretching without a comprehensive warm-up. Eur. J. Appl. Physiol. 2020. [Google Scholar] [CrossRef]
- Deyo, R.A.; Walsh, N.E.; Martin, D.C.; Schoenfeld, L.S.; Ramamurthy, S. A controlled trial of transcutaneous electrical nerve stimulation (TENS) and exercise for chronic low back pain. N. Engl. J. Med. 1990, 322, 1627–1634. [Google Scholar] [CrossRef]
- Lamb, S.E.; Williamson, E.M.; Heine, P.J.; Adams, J.; Dosanjh, S.; Dritsaki, M.; Glover, M.J.; Lord, J.; McConkey, C.; Nichols, V.; et al. Exercises to improve function of the rheumatoid hand (SARAH): A randomised controlled trial. Lancet 2015, 385, 421–429. [Google Scholar] [CrossRef]
- Kokkonen, J.; Nelson, A.G.; Eldredge, C.; Winchester, J.B. Chronic static stretching improves exercise performance. Med. Sci. Sports Exerc. 2007, 39, 1825–1831. [Google Scholar] [CrossRef]
- Santos, C.; Beltrão, N.B.; Pirauá, A.L.T.; Durigan, J.L.Q.; Behm, D.; de Araújo, R.C. Static stretching intensity does not influence acute range of motion, passive torque, and muscle architecture. J. Sport Rehabil. 2020, 29, 1–6. [Google Scholar] [CrossRef]
- Iwata, M.; Yamamoto, A.; Matsuo, S.; Hatano, G.; Miyazaki, M.; Fukaya, T.; Fujiwara, M.; Asai, Y.; Suzuki, S. Dynamic stretching has sustained effects on range of motion and passive stiffness of the hamstring muscles. J. Sports Sci. Med. 2019, 18, 13–20. [Google Scholar]
- Lempke, L.; Wilkinson, R.; Murray, C.; Stanek, J. The effectiveness of PNF versus static Stretching on increasing hip-flexion range of motion. J. Sport Rehabil. 2018, 27, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Ford, G.S.; Mazzone, M.A.; Taylor, K. The effect of 4 different durations of static hamstring stretching on passive knee-extension range of motion. J. Sport Rehabil. 2005, 14, 95–107. [Google Scholar] [CrossRef]
- Frasson, V.B.; Vaz, M.A.; Morales, A.B.; Torresan, A.; Telöken, M.A.; Gusmão, P.D.F.; Crestani, M.V.; Baroni, B.M. Hip muscle weakness and reduced joint range of motion in patients with femoroacetabular impingement syndrome: A case-control study. Braz. J. Phys. Ther. 2020, 24, 39–45. [Google Scholar] [CrossRef]
- Pettersson, H.; Boström, C.; Bringby, F.; Walle-Hansen, R.; Jacobsson, L.T.H.; Svenungsson, E.; Nordin, A.; Alexanderson, H. Muscle endurance, strength, and active range of motion in patients with different subphenotypes in systemic sclerosis: A cross-sectional cohort study. Scand. J. Rheumatol. 2019, 48, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Takeda, H.; Nakagawa, T.; Nakamura, K.; Engebretsen, L. Prevention and management of knee osteoarthritis and knee cartilage injury in sports. Br. J. Sports Med. 2011, 45, 304–309. [Google Scholar] [CrossRef]
- Bompa, T.O.; Buzzichelli, C.A. Periodization: Theory and Methodology of Training, 6th ed.; Human Kinetics: Champaign, IL, USA, 2018. [Google Scholar]
- Moscão, J.; Vilaça-Alves, J.; Afonso, J. A review of the effects of static stretching in human mobility and strength training as a more powerful alternative: Towards a different paradigm. Motricidade 2020, 16, 18–27. [Google Scholar] [CrossRef]
- Racil, G.; Jlid, M.C.; Bouzid, M.S.; Sioud, R.; Khalifa, R.; Amri, M.; Gaied, S.; Coquart, J. Effects of flexibility combined with plyometric exercises vs. isolated plyometric or flexibility mode in adolescent male hurdlers. J. Sports Med. Phys. Fit. 2020, 60, 45–52. [Google Scholar] [CrossRef]
- Saraiva, A.R.; Reis, V.M.; Costa, P.B.; Bentes, C.M.; Costae Silva, G.V.; Novaes, J.S. Chronic effects of different resistance training exercise orders on flexibility in elite judo athletes. J. Hum. Kinet. 2014, 40, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, N.H.; Ribeiro, A.S.; Nascimento, M.A.; Gobbo, L.A.; Schoenfeld, B.J.; Achour, A.; Gobbi, S.; Oliveira, A.R.; Cyrino, E.S. Effects of different resistance training frequencies on flexibility in older women. Clin. Interv. Aging 2015, 10, 531–538. [Google Scholar] [CrossRef]
- Ylinen, J.; Takala, E.P.; Nykänen, M.; Häkkinen, A.; Mälkiä, E.; Pohjolainen, T.; Karppi, S.L.; Kautiainen, H.; Airaksinen, O. Active neck muscle training in the treatment of chronic neck pain in women: A randomized controlled trial. JAMA 2003, 289, 2509–2516. [Google Scholar] [CrossRef]
- Valamatos, M.J.; Tavares, F.; Santos, R.M.; Veloso, A.P.; Mil-Homens, P. Influence of full range of motion vs. equalized partial range of motion training on muscle architecture and mechanical properties. Eur. J. Appl. Physiol. 2018, 118, 1969–1983. [Google Scholar] [CrossRef]
- Marušič, J.; Vatovec, R.; Marković, G.; Šarabon, N. Effects of eccentric training at long-muscle length on architectural and functional characteristics of the hamstrings. Scand. J. Med. Sci. Sports 2020. [Google Scholar] [CrossRef] [PubMed]
- Bourne, M.N.; Duhig, S.J.; Timmins, R.G.; Williams, M.D.; Opar, D.A.; Al Najjar, A.; Kerr, G.K.; Shield, A.J. Impact of the Nordic hamstring and hip extension exercises on hamstring architecture and morphology: Implications for injury prevention. Br. J. Sports Med. 2017, 51, 469–477. [Google Scholar] [CrossRef] [PubMed]
- De Boer, M.D.; Morse, C.I.; Thom, J.M.; de Haan, A.; Narici, M.V. Changes in antagonist muscles’ coactivation in response to strength training in older women. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 1022–1027. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Silva-Batista, C.; Mattos, E.C.; Corcos, D.M.; Wilson, J.M.; Heckman, C.J.; Kanegusuku, H.; Piemonte, M.E.; Túlio de Mello, M.; Forjaz, C.; Roschel, H.; et al. Resistance training with instability is more effective than resistance training in improving spinal inhibitory mechanisms in Parkinson’s disease. J. Appl. Physiol. 2017, 122, 1–10. [Google Scholar] [CrossRef]
- Kubo, K.; Ishigaki, T.; Ikebukuro, T. Effects of plyometric and isometric training on muscle and tendon stiffness in vivo. Physiol. Rep. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.B.; Galecki, A.T.; Grenier, M.L.; Nyquist, L.V.; Hofmeyer, M.R.; Grunawalt, J.C.; Medell, J.L.; Fry-Welch, D. Task-specific resistance training to improve the ability of activities of daily living-impaired older adults to rise from a bed and from a chair. J. Am. Geriatr. Soc. 2001, 49, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Aquino, C.F.; Fonseca, S.T.; Goncalves, G.G.; Silva, P.L.; Ocarino, J.M.; Mancini, M.C. Stretching versus strength training in lengthened position in subjects with tight hamstring muscles: A randomized controlled trial. Man. Ther. 2010, 15, 26–31. [Google Scholar] [CrossRef]
- Leite, T.; de Souza Teixeira, A.; Saavedra, F.; Leite, R.D.; Rhea, M.R.; Simão, R. Influence of strength and flexibility training, combined or isolated, on strength and flexibility gains. J. Strength Cond. Res. 2015, 29, 1083–1088. [Google Scholar] [CrossRef]
- Caputo, G.M.; di Bari, M.; Naranjo Orellana, J. Group-based exercise at workplace: Short-term effects of neck and shoulder resistance training in video display unit workers with work-related chronic neck pain-a pilot randomized trial. Clin. Rheumatol. 2017, 36, 2325–2333. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, C.; MacAuley, D. The quality of research in sports journals. Br. J. Sports Med. 2002, 36, 124. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Skrede, T.; Steene-Johannessen, J.; Anderssen, S.A.; Resaland, G.K.; Ekelund, U. The prospective association between objectively measured sedentary time, moderate-to-vigorous physical activity and cardiometabolic risk factors in youth: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 55–74. [Google Scholar] [CrossRef]
- Drahota, A.; Beller, E. RevMan Calculator for Microsoft Excel; Cochrane: London, UK, 2020. [Google Scholar]
- Chiu, Y.H.; Chang, K.V.; Chen, I.J.; Wu, W.T.; Özçakar, L. Utility of sonoelastography for the evaluation of rotator cuff tendon and pertinent disorders: A systematic review and meta-analysis. Eur. Radiol. 2020, 30, 6663–6672. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Lee, T.M.; Han, D.S.; Chang, K.V. The prevalence of sarcopenia and its impact on clinical outcomes in lumbar degenerative spine disease—A systematic review and meta-analysis. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Al-Wahab, M.G.A.; Salem, E.E.S.; El-Hadidy, E.I.; El-Barbary, H.M. Effect of plyometric training on shoulder strength and active movements in children with Erb’s palsy. Int. J. Pharmtech. Res. 2016, 9, 25–33. [Google Scholar]
- Fernandez-Fernandez, J.; Ellenbecker, T.; Sanz-Rivas, D.; Ulbricht, A.; Ferrauti, A. Effects of a 6-week junior tennis conditioning program on service velocity. J. Sports Sci. Med. 2013, 12, 232–239. [Google Scholar]
- De Resende-Neto, A.G.; do Nascimento, M.A.; de Sa, C.A.; Ribeiro, A.S.; Desantana, J.M.; da Silva-Grigoletto, M.E. Comparison between functional and traditional training exercises on joint mobility, determinants of walking and muscle strength in older women. J. Sports Med. Phys. Fit. 2019, 59, 1659–1668. [Google Scholar] [CrossRef]
- Hajihosseini, E.; Norasteh, A.; Shamsi, A.; Daneshmandi, H.; Shahheidari, S. Effects of strengthening, stretching and comprehensive exercise program on the strength and range of motion of the shoulder girdle muscles in upper crossed syndrome. Med. Sport 2016, 69, 24–40. [Google Scholar]
- Fukuchi, R.K.; Stefanyshyn, D.J.; Stirling, L.; Ferber, R. Effects of strengthening and stretching exercise programmes on kinematics and kinetics of running in older adults: A randomised controlled trial. J. Sports Sci. 2016, 34, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Häkkinen, A.; Kautiainen, H.; Hannonen, P.; Ylinen, J. Strength training and stretching versus stretching only in the treatment of patients with chronic neck pain: A randomized one-year follow-up study. Clin. Rehabil. 2008, 22, 592–600. [Google Scholar] [CrossRef]
- Kalkman, B.M.; Holmes, G.; Bar-On, L.; Maganaris, C.N.; Barton, G.J.; Bass, A.; Wright, D.M.; Walton, R.; O’Brien, T.D. Resistance training combined with stretching increases tendon stiffness and is more effective than stretching alone in children with cerebral palsy: A randomized controlled trial. Front. Pediatr. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.K.; Whitehead, J.R.; Brinkert, R.H.; Caine, D.J. Resistance training vs. static stretching: Effects on flexibility and strength. J. Strength Cond. Res. 2011, 25, 3391–3398. [Google Scholar] [CrossRef]
- Li, S.; Garrett, W.E.; Best, T.M.; Li, H.; Wan, X.; Liu, H.; Yu, B. Effects of flexibility and strength interventions on optimal lengths of hamstring muscle-tendon units. J. Sci. Med. Sport 2020, 23, 200–205. [Google Scholar] [CrossRef]
- Wyon, M.A.; Smith, A.; Koutedakis, Y. A comparison of strength and stretch interventions on active and passive ranges of movement in dancers: A randomized controlled trial. J. Strength Cond. Res. 2013, 27, 3053–3059. [Google Scholar] [CrossRef]
- Girouard, C.K.; Hurley, B.F. Does strength training inhibit gains in range of motion from flexibility training in older adults? Med. Sci. Sports Exerc. 1995, 27, 1444–1449. [Google Scholar] [CrossRef]
- Raab, D.M.; Agre, J.C.; McAdam, M.; Smith, E.L. Light resistance and stretching exercise in elderly women: Effect upon flexibility. Arch. Phys. Med. Rehabil. 1988, 69, 268–272. [Google Scholar] [PubMed]
- Klinge, K.; Magnusson, S.P.; Simonsen, E.B.; Aagaard, P.; Klausen, K.; Kjaer, M. The effect of strength and flexibility training on skeletal muscle electromyographic activity, stiffness, and viscoelastic stress relaxation response. Am. J. Sports Med. 1997, 25, 710–716. [Google Scholar] [CrossRef]
- Nóbrega, A.C.; Paula, K.C.; Carvalho, A.C. Interaction between resistance training and flexibility training in healthy young adults. J. Strength Cond. Res. 2005, 19, 842–846. [Google Scholar] [CrossRef]
- Simão, R.; Lemos, A.; Salles, B.; Leite, T.; Oliveira, É.; Rhea, M.; Reis, V.M. The influence of strength, flexibility, and simultaneous training on flexibility and strength gains. J. Strength Cond. Res. 2011, 25, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-H.; Lin, C.-R.; Liang, W.-A.; Huang, C.-Y. Motor control integrated into muscle strengthening exercises has more effects on scapular muscle activities and joint range of motion before initiation of radiotherapy in oral cancer survivors with neck dissection: A randomized controlled trial. PLoS ONE 2020, 15, e0237133. [Google Scholar] [CrossRef]
- Venkataraman, K.; Tai, B.C.; Khoo, E.Y.H.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; Phua, M.S.L.A.; Wee, H.L.; Koh, G.C.H.; Tai, E.S. Short-term strength and balance training does not improve quality of life but improves functional status in individuals with diabetic peripheral neuropathy: A randomised controlled trial. Diabetologia 2019, 62, 2200–2210. [Google Scholar] [CrossRef] [PubMed]
- Pallarés, J.G.; Cava, A.M.; Courel-Ibáñez, J.; González-Badillo, J.J.; Morán-Navarro, R. Full squat produces greater neuromuscular and functional adaptations and lower pain than partial squats after prolonged resistance training. Eur. J. Sport Sci. 2020, 20, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Çergel, Y.; Topuz, O.; Alkan, H.; Sarsan, A.; Sabir Akkoyunlu, N. The effects of short-term back extensor strength training in postmenopausal osteoporotic women with vertebral fractures: Comparison of supervised and home exercise program. Arch. Osteoporos. 2019, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- Albino, I.L.R.; Freitas, C.D.L.R.; Teixeira, A.R.; Gonçalves, A.K.; Santos, A.M.P.V.D.; Bós, Â.J.G. Influência do treinamento de força muscular e de flexibilidade articular sobre o equilíbrio corporal em idosas. Rev. Bras. Geriatr. Gerontol. 2012, 15, 17–25. [Google Scholar] [CrossRef]
- LeCheminant, J.D.; Hinman, T.; Pratt, K.B.; Earl, N.; Bailey, B.W.; Thackeray, R.; Tucker, L.A. Effect of resistance training on body composition, self-efficacy, depression, and activity in postpartum women. Scand. J. Med. Sci. Sports 2014, 24, 414–421. [Google Scholar] [CrossRef]
- Jones, K.D.; Burckhardt, C.S.; Clark, S.R.; Bennett, R.M.; Potempa, K.M. A randomized controlled trial of muscle strengthening versus flexibility training in fibromyalgia. J. Rheumatol. 2002, 29, 1041–1048. [Google Scholar]
- Nelson, R.T.; Bandy, W.D. Eccentric training and static stretching improve hamstring flexibility of high school males. J. Athl. Train. 2004, 39, 254–258. [Google Scholar]
- Wyon, M.A.; Felton, L.; Galloway, S. A comparison of two stretching modalities on lower-limb range of motion measurements in recreational dancers. J. Strength Cond. Res. 2009, 23, 2144–2148. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.R.; Vaz, J.R.; Gomes, L.; Silvestre, R.; Hilário, E.; Cordeiro, N.; Carnide, F.; Pezarat-Correia, P.; Mil-homens, P. A new tool to assess the perception of stretching intensity. J. Strength Cond. Res. 2015, 29, 2666–2678. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Kambas, A.; Katrabasas, I.; Leontsini, D.; Chatzinikolaou, A.; Jamurtas, A.Z.; Douroudos, I.; Aggelousis, N.; Taxildaris, K. Resistance training and detraining effects on flexibility performance in the elderly are intensity-dependent. J. Strength Cond. Res. 2006, 20, 634–642. [Google Scholar] [CrossRef]
- Gérard, R.; Gojon, L.; Decleve, P.; van Cant, J. The effects of eccentric training on biceps femoris architecture and strength: A systematic review with meta-analysis. J. Athl. Train. 2020, 55, 501–514. [Google Scholar] [CrossRef]
- Reeves, N.D.; Maganaris, C.N.; Longo, S.; Narici, M.V. Differential adaptations to eccentric versus conventional resistance training in older humans. Exp. Physiol. 2009, 94, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Medina-Mirapeix, F.; Escolar-Reina, P.; Gascón-Cánovas, J.J.; Montilla-Herrador, J.; Jimeno-Serrano, F.J.; Collins, S.M. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: An observational study. BMC Musculoskelet. Disord. 2009, 10. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Population and Common Program Features | Strength Training Group | Comparator Group(s) * | ROM Testing | Qualitative Results for ROM |
|---|---|---|---|---|---|
| Task-Specific Resistance Training to Improve the Ability of Activities of Daily Living–Impaired Older Adults to Rise from a Bed and from a Chair. [43] | Subjects: 161. Health status: Elderly people dependent on help for performing at least one of four tasks: transferring, bathing, toileting and walking. Gender: ST: 84% women; STRE: 88% women. Age: ST: 82.0 ± 6.4; STRE: 82.4 ± 6.3. Training status: Not participating in regular strenuous exercise. Selection of subjects: Seven congregate housing facilities. Length (weeks): 12. Weekly sessions: 3. Adherence: average 81% of the sessions. Funding National Institute on Aging (NIA) Claude Pepper Older Adults Independence Center (Grant AG0 8808 and NIA Grant AG10542), the Department of Veterans Affairs Rehabilitation Research and Development, and the AARP-Andrus Foundation. Conflicts of interest: N/A. | n = 81 (60 completed). Weekly volume (minutes): 180. Session duration in minutes: 60. No. exercises per session: 16. No. sets and repetitions: 1*7–8 based on maximum target of 9 (bed-rise tasks). 1*5 based on maximum target of 6 (chair-rise tasks). Load: Unclear. Loads were incremented if subjects were not feeling challenged enough. Full or partial ROM: N/A. Supervision ratio: 1:1. | STRE n = 80 (64 completed). Weekly volume (minutes): 180. Session duration in minutes: 60. No. exercises per session: N/A. No. sets and repetitions: N/A. Stretching modality: Dynamic. Load: Low-intensity, but without a specified criterion. Full or partial ROM: N/A. Supervision ratio: One supervisor per group, but group size was N/A. | Joints and actions: Elbow (extension), shoulder (abduction), hip (flexion and abduction), knee (flexion and extension), ankle (dorsiflexion) and trunk (flexion, extension, lateral flexion). Positions: Supine (elbow, shoulder, hip, knee and ankle); standing (lumbar spine). Mode: Active for trunk, passive for the other joints. Warm-up: N/A. Timing: Baseline, 6 weeks, 12 weeks. Results considered in the tests: N/A. Data reliability: ICCs of 0.65 to 0.86 for trunk measures. Unreported for other measures. No. testers: N/A. Instructions during testing: N/A. | The ST group had significant improvements in all ROM measures, except hip flexion and abduction. The STRE group had no significant change in any of the ROM values. |
| Stretching versus strength training in lengthened position in subjects with tight hamstring muscles: A randomized controlled trial. [44] | Subjects: 45 undergraduate students. Health status: 30° knee extension deficit with the hip at 90° when in supine position. No injuries in the lower limbs and no lower back pain. Gender: 39 women, 6 men. Age: 21.33 ± 1.76 years (ST); 22.60 ± 1.84 years (STRE). Training status: No participation in ST or STRE programs in the previous year. Selection of subjects: announcements posted at the University. Length (weeks): 8. Weekly sessions: 3. Adherence: N/A. Funding N/A. Conflicts of interest: N/A. | n = 15. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 1. No. sets and repetitions: 3*12. Load: 60% of 1RM. Full or partial ROM: Partial. Supervision ratio: N/A. | STRE n = 15. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 1. No. sets and repetitions: 4*30″. Stretching modality: Static. Load: Unclear. Full or partial ROM: Full. Supervision ratio: N/A. | Joints and actions: Knee (extension). Positions: Sitting. Mode: Passive. Warm-up: Yes, but unclear with regard to specifications. Timing: Baseline, 1-week post-protocol. Results considered in the tests: mean of three measures. Data reliability: High. No. testers: 1 (blinded). Instructions during testing: N/A. | None of the groups experienced significant improvements in ROM. |
| Group-based exercise at workplace: short-term effects of neck and shoulder resistance training in video display unit workers with work-related chronic neck pain—a pilot randomized trial. [46] | Subjects: 35 video display unit workers, 27 completed the program. Health status: chronic neck pain. Gender: 27 women, 8 men. Age: 43 (41–45) in ST; 42 (38.5–44) in STRE. Training status: N/A. Selection of subjects: intranet form. Length (weeks): 7. Weekly sessions: 2. Adherence: average 85% of the sessions in ST and 86% in STRE. Funding Under “disclosures”, the authors stated “none”. Conflicts of interest: Under “disclosures”, the authors stated “none”. | n = 14. Weekly volume (minutes): 90. Session duration in minutes: 45. No. exercises per session: 10. No. sets and repetitions: 2–3*8–20. Isometric contractions up to 30″. Load: free-weights with a maximum of 75% MVC and elastic bands of unspecified load. Full or partial ROM: N/A. Supervision ratio: ~1:8. | STRE n = 13. Weekly volume (minutes): 90. Session duration in minutes: 45. No. exercises per session: 11. No. sets and repetitions: 10*10″. Stretching modality: Static. Load: N/A. Full or partial ROM: N/A. Supervision ratio: ~1:8. | Joints and actions: Cervical spine (flexion, extension, lateral flexion, rotation). Positions: Sitting (flexion, extension, lateral flexion) and supine position (rotation). Mode: Active. Warm-up: N/A. Timing: Baseline, 1-week post-protocol. Results considered in the tests: N/A. Data reliability: N/A. No. testers: 1 (blinded). Instructions during testing: N/A. | Significant improvements in both groups for all ROM measurements. No differences between the two groups. |
| A randomized controlled trial of muscle strengthening versus flexibility training in fibromyalgia. [85] | Subjects: 68; 56 completed the program. Health status: Diagnosed with fibromyalgia (FM). Gender: Women. Age: 49.2 ± 6.36 years in ST, 46.4 ± 8.56 in STRE. Training status: 87% were sedentary. Not engaged in regular strength training programs. Selection of subjects: FM patients referred to rheumatology practice at a teaching university. Length (weeks): 12. Weekly sessions: 2. Adherence: 85% of the initial participants attended ≥13 of 24 classes. N/A for the 46 women that completed the interventions. Funding Individual National Research Service Award (#1F31NR07337-01A1) from the National Institutes of Health, a doctoral dissertation grant (#2324938) from the Arthritis Foundation, and funds from the Oregon Fibromyalgia Foundation. Conflicts of interest: N/A. | n = 28. Weekly volume (minutes): 120. Session duration in minutes: 60. No. exercises per session: Presumably 12. No. sets and repetitions: 1*4–5, progressing to 1*12. Load: Low intensity. Slower concentric contractions with a 4″ isometric hold in the end, and a faster eccentric contraction. Full or partial ROM: Full. Supervision ratio: Presumably 1:28. | STRE n = 28. Weekly volume (minutes): 120. Session duration in minutes: 60. No. exercises per session: Presumably 12. No. sets and repetitions: N/A. Stretching modality: Static. Load: Low intensity. Full or partial ROM: N/A. Supervision ratio: Presumably 1:28. | Joints and actions: Shoulder (the authors report on internal and external rotation, but the movements used actually required a combination of motions). Positions: Presumably standing. Mode: Active. Warm-up: N/A. Timing: Baseline, 12 weeks. Results considered in the tests: N/A. Data reliability: Referral to a previous study, but no values for these data. No. testers: 1. Instructions during testing: Reach as far as possible. | Both groups had significant improvements in ROM. No differences between groups. |
| Influence of Strength and Flexibility Training, Combined or Isolated, on Strength and Flexibility Gains. [45] | Subjects:28 women. Health status: Presumably healthy. Gender: Women. Age: 46 ± 6.5. Training status: Trained in strength and stretching. Selection of subjects: Volunteers that would refrain from exercise outside the intervention. Length (weeks):12. Weekly sessions: 4. Not explicit; 48 sessions over 12 weeks. Adherence: Minimum was 44 of the 48 sessions. Funding N/A. Conflicts of interest: N/A. | n = 7. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 8. No. sets and repetitions: 3*8–12 during the 1st month; 3*6–10RM in the 2nd month; 3*10–15RM in the 3rd month. Load: 6–15RM, depending on the month. Full or partial ROM: N/A. Supervision ratio: N/A. | STRE n = 7. Weekly volume (minutes): 240. Session duration in minutes: 60. No. exercises per session: N/A. No. sets and repetitions: 3*30. Stretching modality: Dynamic. Load: Stretch to mild discomfort. Full or partial ROM: Full. Supervision ratio: N/A. STRE + ST n = 7. Completion of both protocols. Unknown duration. ST + STRE n = 7. Completion of both protocols in reverse order. Unknown duration. | Joints and actions: Shoulder (flexion, extension, abduction and horizontal adduction) elbow (flexion), hip (flexion and extension), knee (flexion), and trunk (flexion and extension). Positions: Supine (shoulder flexion, abduction, horizontal adduction, elbow and hip flexion), prone (shoulder and hip extension, and knee flexion) and upright (trunk flexion and extension) for goniometric evaluations. Sitting for sit-and-reach. Mode: Passive for goniometry. Active for sit-and-reach. Warm-up: 5- minute walking on treadmill at mild to moderate intensity and four stretching exercises. Timing: Baseline, 12 weeks. Results considered in the tests: Best of 3 trials. Data reliability: Very high. No. testers: 1. Instructions during testing: N/A. | None of the groups experienced significant improvements in ROM. |
| Effects of Flexibility and Strength Interventions on Optimal Lengths of Hamstring Muscle-Tendon Units. [72] | Subjects: 40 college students. Health status: No history of lower extremity injury in the 2 years prior to the study. Gender: 20 men, 20 women. Age: 18–24 years. Training status: participating in exercise 2–3 times per week. Selection of subjects: college students. Length (weeks): 8. Weekly sessions: 3. Adherence: N/A. Funding Partially supported by the National Natural Science Foundation of China (Grant No.: 81572212) and the Fundamental Research Fund for the Central Universities, Beijing Sport University (Grant No.: 2017XS017). Conflicts of interest: N/A. | n = 20. Weekly volume (minutes): N/A. Session duration in minutes: N/A No. exercises per session: 4. No. sets and repetitions: 2–4*8–15. For one exercise, 2*50–60″. Load: N/A. Full or partial ROM: N/A. Supervision ratio: N/A. | STRE n = 20. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 4. No. sets and repetitions: 2*15 for dynamic stretching, 2*40–60″ for static stretching, 3*50″ for PNF and 3*40–50″ for foam roll. Stretching modality: active static, dynamic and PNF. Load: N/A. Full or partial ROM: N/A. Supervision ratio: N/A. | Joints and actions: Hip (flexion). Positions: Supine. Mode: Passive. Warm-up: Six-minute warm-up including jogging and jumping. Timing: Baseline, 8 weeks. Results considered in the tests: Mean of three trials. Data reliability: Very high. No. testers: N/A. Instructions during testing: N/A. | Men and women in both groups significantly improved ROM. No differences between groups. |
| Resistance training vs. static stretching: Effects on flexibility and strength. [71] | Subjects: 37 college students. Health status: Healthy. Gender: 30 men, 12 women; ratio is unclear in the final sample. Age: 21.91 ± 3.64 years. Training status: Untrained. Selection of subjects: Recruited from Physical Education or Exercise Science Classes. Length (weeks): 5. Weekly sessions: 3. Adherence: N/A. Funding N/A. Conflicts of interest: N/A. | n = 12. Weekly volume (minutes): 135–180. Session duration in minutes: 45–60. No. exercises per session: eight in days 1 and 2, four in day 3. No. sets and repetitions: 4 sets of unspecified repetitions. Load: N/A. Full or partial ROM: Full. Supervision ratio: 1:12. | STRE n = 12. Weekly volume (minutes): 75–90. Session duration in minutes: 25–35. No. exercises per session: 13. No. sets and repetitions: 1*30″ for most stretches. 3*30″ for one exercise and 3*20″ for two. Stretching modality: Static. Load: N/A. Full or partial ROM: Full. Supervision ratio: 1:12. | Joints and actions: Hip (flexion, extension), knee (extension) and shoulder (extension). Positions: Supine (knee and hip). Prone (shoulder). Mode: Passive for hip and knee, active for shoulder. Warm-up: 5 min of stationary bicycle with minimal resistance. Timing: Baseline, 1-week post-protocol. Results considered in the tests: N/A. Data reliability: N/A. No. testers: 1. Instructions during testing: Technical instructions specific to each test. | Both groups had significant improvements in knee extension, hip flexion and hip extension, but not shoulder extension. No differences between the interventions. |
| Eccentric training and static stretching improve hamstring flexibility of high school men. [86] | Subjects: 69 high-schoolers. Health status: Healthy, but with a 30° loss of knee extension. Gender: Men. Age: 16.45 ± 0.96 years. Training status: Some sedentary, others involved in exercise programs. Selection of subjects: Volunteers with tight hamstrings. Length (weeks): 6. Weekly sessions: 3 for STRE. N/A for ST. Adherence: N/A for ST. STRE: subjects missing >4 sessions were excluded. Funding N/A. Conflicts of interest: N/A. | n = 24. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 1. No. sets and repetitions: 6 repetitions with 5″ isometric hold between each. Load: N/A. Full or partial ROM: Full. Supervision ratio: Description suggests a 1:1 ratio. | STRE n= 21. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 1. No. sets and repetitions: Unknown number of repetitions, each lasting 30″. Stretching modality: Static. Load: Stretch until a gentle stretch was felt on the posterior thigh. Full or partial ROM: Full. Supervision ratio: Description suggests a 1:1 ratio. | Joints and actions: Knee (extension). Positions: Supine. Mode: Passive. Warm-up: No warm-up. Timing: Baseline, 6 weeks. Results considered in the tests: Two measures for previous reliability calculations, but unclear for the groups’ evaluation. Data reliability: Very high. No. testers: 2 (1 blinded). Instructions during testing: N/A. | Both groups improved ROM. No differences between the interventions. |
| Effects of flexibility combined with plyometric exercises vs. isolated plyometric or flexibility mode in adolescent men hurdlers. [33] | Subjects: 34 trained hurdlers. Health status: No lower extremity injury in the previous 30 days. Gender: Men. Age: 15 ± 0.7 years. Training status: ≥3 years of experience in hurdle racing. Selection of subjects: Recruited from three athletic teams. Length (weeks): 12. Weekly sessions: 4. Adherence: N/A. Funding No funding. Conflicts of interest: No conflicts of interest. | n = 9. Weekly volume (minutes): 320. Session duration in minutes: 80. No. exercises per session: 4. No. sets and repetitions: 3*30″. Load: Evolved from low to hard intensity, but no criteria were provided. Full or partial ROM: N/A. Supervision ratio: N/A. | STRE n = 8. Weekly volume (minutes): 320. Session duration in minutes: 80. No. exercises per session: 7. No. sets and repetitions: 5*10″. Stretching modality: Dynamic with 10″ static hold. Load: Evolved from low to hard intensity, but no criteria were provided. Full or partial ROM: N/A. Supervision ratio: N/A. STRE+ ST n = 9. Weekly volume (minutes): 320. Session duration in minutes: 80. No. exercises per session: 11 (4 plyometric; 7 flexibility). No. sets and repetitions: 3*30″ for plyometrics, 5*10″ for stretching. Stretching modality: Dynamic with 10″ static hold. Load: Evolved from low to hard intensity, but no criteria were provided. Full or partial ROM: N/A. Supervision ratio: N/A. | Joints and actions: Hip (flexion and extension). Positions: Supine. Mode: Active. Warm-up: N/A. Timing: Baseline, 12 weeks. Results considered in the tests: Best of 3 attempts. Data reliability: Referral to a previous study, but no values for these data. No. testers: 2. Instructions during testing: N/A. | All interventions had significant improvements in ROM. No differences between the interventions. |
| The influence of strength, flexibility, and simultaneous training on flexibility and strength gains. [78] | Subjects: 80 women. Health status: Healthy. Gender: Women. Age: 35 ± 2.0 (ST), 34 ± 1.2 (STRE), 35 ± 1.8 (ST + STRE), 34 ± 2.1 (non-exercise). Training status: Sedentary. Selection of subjects: Volunteers that were sedentary ≥12 months. Length (weeks): 16. Weekly sessions: 3. Adherence: Minimum was 46 of the 48 sessions. Funding N/A. Conflicts of interest: N/A. | n = 20. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 8. No. sets and repetitions: 3*8–12 in the 1st and 4th months; 3*6–10 in 2nd month; 3*10–15 in 3rd month. Load: 8–12RM (1st and 4th months); 6–10RM (2nd month); 10–15RM (3rd month). Full or partial ROM: N/A. Supervision ratio: N/A. | STRE n = 20. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: N/A. No. sets and repetitions: 4*15–60″. Duration of each set started at 15″ and progressed to 60″ during the intervention. Stretching modality: Static. Load: Performed at the point of mild discomfort. Full or partial ROM: N/A. Supervision ratio: N/A. ST + STRE n = 20. STRE protocol followed by the ST protocol. | Joints and actions: Hip (flexion) and knee (extension) combined. Positions: Sitting. Mode: Active. Warm-up: 4 stretching exercises (2*10″). Timing: Baseline, 16 weeks. Results considered in the tests: Maximum of 3 attempts. Data reliability: Very high. No. testers: 1. Instructions during testing: N/A. | The interventions significantly improved ROM. No differences between the interventions. |
| A comparison of strength and stretch interventions on active and passive ranges of movement in dancers: a randomized control trial. [73] | Subjects: 39 dance students, 35 completed. Health status: N/A. Gender: Women (39). Age: 17 ± 0.49 years (ST group); 17 ± 0.56 years (low-intensity STRE); 17 ± 0.56 years (moderate to high intensity STRE). Training status: Moderately trained dance students. Selection of subjects: Recruited from dance college. Length (weeks): 6. Weekly sessions: 5. Adherence: N/A. Funding N/A. Conflicts of interest: N/A. | n = 11. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 1. No. sets and repetitions: 3*5, increasing to 3*10 during the program. Each repetition included a 3″ isometric hold. Load: Unclear, but using body weight. Full or partial ROM: Partial (final 10°). Supervision ratio: N/A. | Low-intensity STRE n = 13. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 5. No. sets and repetitions: N/A, but 1′ for each stretch. Stretching modality: Active static. Load: 3/10 perceived exertion. Full or partial ROM: N/A. Supervision ratio: N/A. Moderate-intensity or high-intensity STRE n = 11. Weekly volume (minutes): N/A. Session duration in minutes: N/A. No. exercises per session: 5. No. sets and repetitions: N/A. Stretching modality: Passive. Load: 8/10 perceived exertion. Full or partial ROM: N/A. Supervision ratio: N/A. | Joints and actions: Hip (flexion). Positions: Standing. Mode: Active and passive. Warm-up: 10 min of cardiovascular exercise and lower limb stretches. Timing: Baseline, 6 weeks. Results considered in the tests: N/A. Data reliability: N/A. No. testers: N/A. Instructions during testing: Positioning cues for ensuring proper posture. | The three groups significantly improved passive ROM, without differences between the groups. The moderate-to-high intensity STRE group did not improve in active ROM. The two other interventions did. |
| Article | Randomization Process | Deviations from Intended Interventions (EAI 1) | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Results |
|---|---|---|---|---|---|
| Alexander, Galecki, Grenier, Nyquist, Hofmeyer, Grunawalt, Medell and Fry-Welch [43] |  | | |  | |
| Aquino, Fonseca, Goncalves, Silva, Ocarino and Mancini [44] | | | | | |
| Caputo, Di Bari and Naranjo Orellana [46] |  | | | | |
| Jones, Burckhardt, Clark, Bennett and Potempa [85] | | | | | |
| Leite, De Souza Teixeira, Saavedra, Leite, Rhea and Simão [45] | | | | | |
| Li, Garrett, Best, Li, Wan, Liu and Yu [72] | | | | | |
| Morton, Whitehead, Brinkert and Caine [71] | | | | | |
| Nelson and Bandy [86] | | | | | |
| Racil, Jlid, Bouzid, Sioud, Khalifa, Amri, Gaied and Coquart [33] | | | | | |
| Simão, Lemos, Salles, Leite, Oliveira, Rhea and Reis [78] | | | | | |
| Wyon, Smith and Koutedakis [73] | | | | | |
Low risk of bias; Some concerns; High risk of bias.| Outcome | Study Design | RoB 1 | Publication Bias | Inconsistency | Indirectness | Imprecision | Quality of Evidence | Recommendation |
|---|---|---|---|---|---|---|---|---|
| ROM | 11 RCTs, 452 participants in meta-analysis. | Randomization—low in four articles, moderate in one, and high in six. | No publication bias. | 9 RCTs showed improvements in ROM in both groups. 2 RCTs showed no changes in ROM in either group. 11 RCTs showed effects of equal magnitude for ST and stretching. 2 | No serious indirectness. | Moderate. 3 | Moderate. ⨁⨁⨁ | Moderate recommendation for either strength training or stretching 4. No recommendation for choosing one of the protocols over the other, as their efficacy in ROM gains was statistically not different. |
| Deviations from intended interventions—Low. | ||||||||
| Missing outcome data—Low. | ||||||||
| Measurement of the outcome—low in six articles and high in five. | ||||||||
| Selection of the reported results—Low. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afonso, J.; Ramirez-Campillo, R.; Moscão, J.; Rocha, T.; Zacca, R.; Martins, A.; Milheiro, A.A.; Ferreira, J.; Sarmento, H.; Clemente, F.M. Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 427. https://doi.org/10.3390/healthcare9040427
Afonso J, Ramirez-Campillo R, Moscão J, Rocha T, Zacca R, Martins A, Milheiro AA, Ferreira J, Sarmento H, Clemente FM. Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis. Healthcare. 2021; 9(4):427. https://doi.org/10.3390/healthcare9040427
Chicago/Turabian StyleAfonso, José, Rodrigo Ramirez-Campillo, João Moscão, Tiago Rocha, Rodrigo Zacca, Alexandre Martins, André A. Milheiro, João Ferreira, Hugo Sarmento, and Filipe Manuel Clemente. 2021. "Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis" Healthcare 9, no. 4: 427. https://doi.org/10.3390/healthcare9040427
APA StyleAfonso, J., Ramirez-Campillo, R., Moscão, J., Rocha, T., Zacca, R., Martins, A., Milheiro, A. A., Ferreira, J., Sarmento, H., & Clemente, F. M. (2021). Strength Training versus Stretching for Improving Range of Motion: A Systematic Review and Meta-Analysis. Healthcare, 9(4), 427. https://doi.org/10.3390/healthcare9040427