
Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Extraction of Data
2.4. Data Items
2.5. Assessment of Methodological Quality
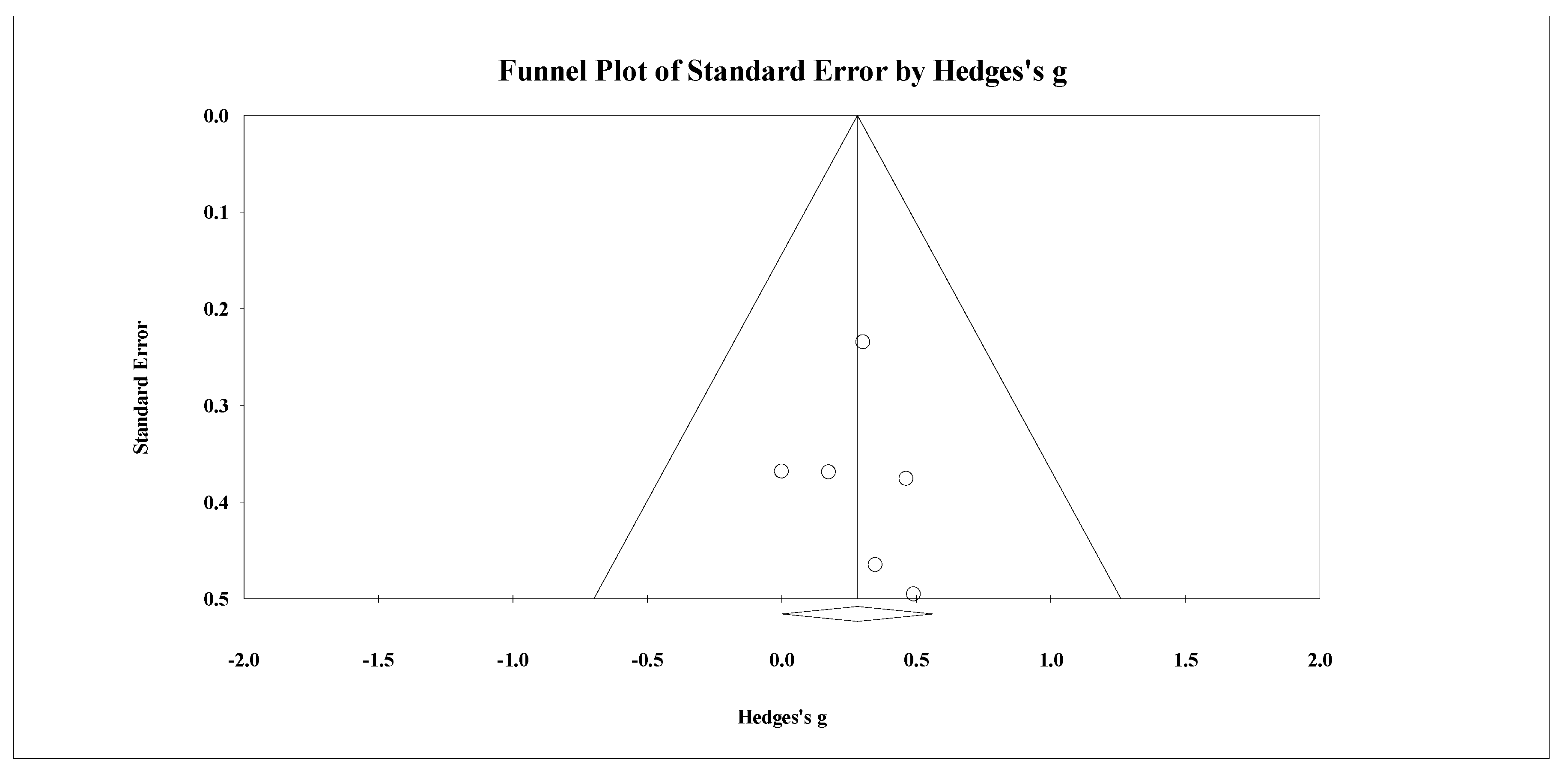
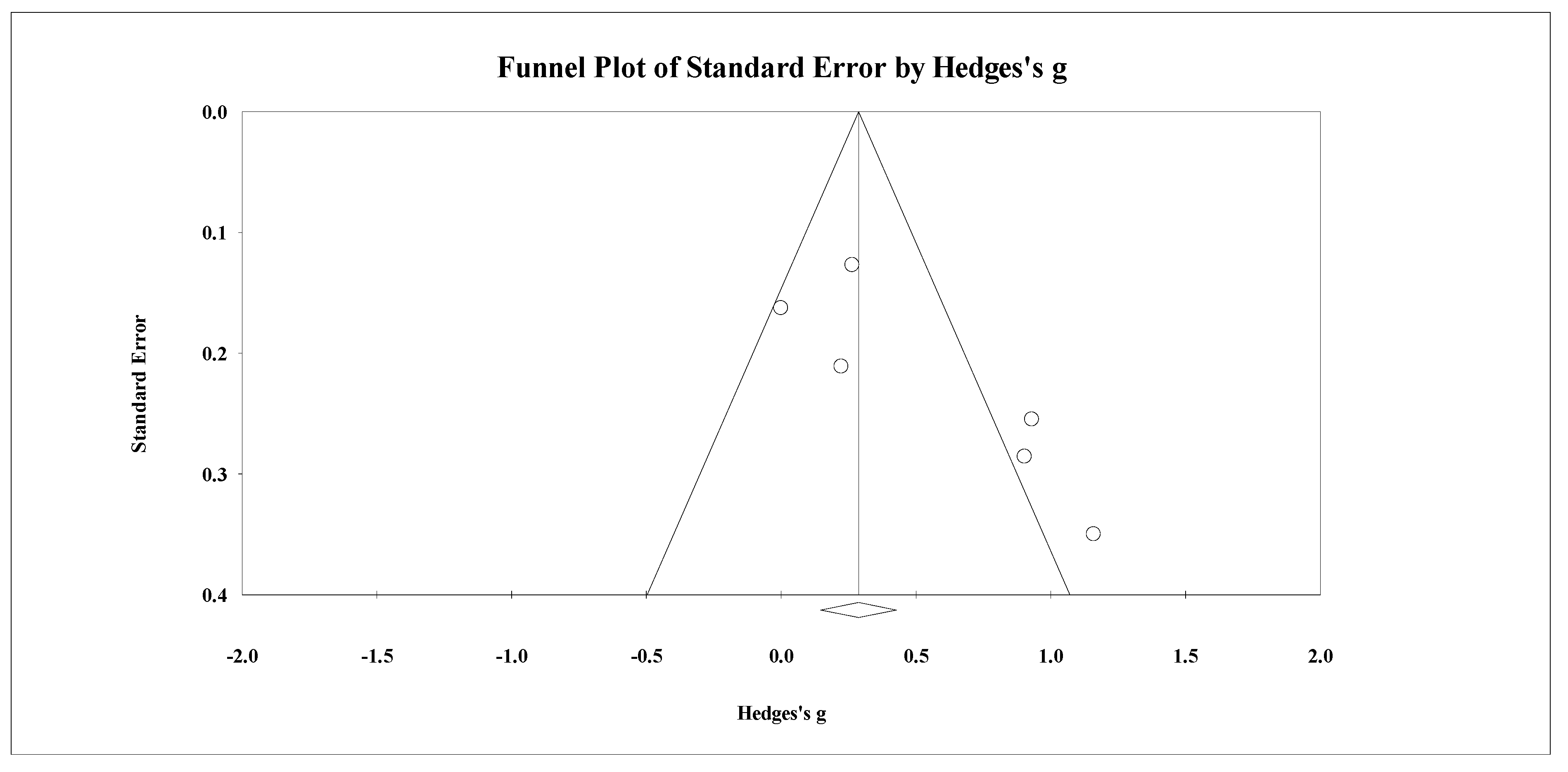
2.6. Summary Measures, Synthesis of Results, and Publication Bias
3. Results
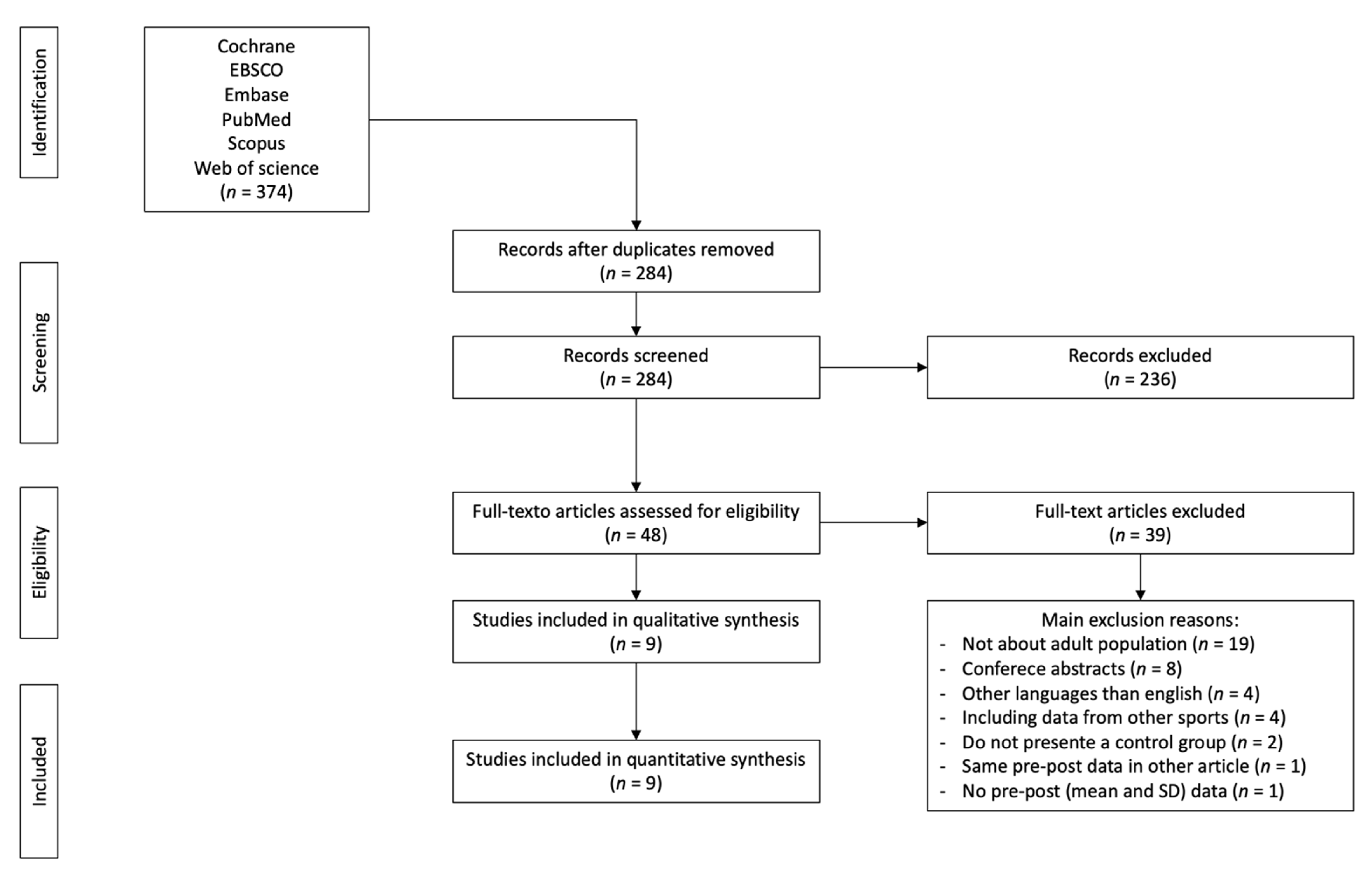
3.1. Study Identification and Selection
3.2. Study Characteristics
3.3. Methodological Quality
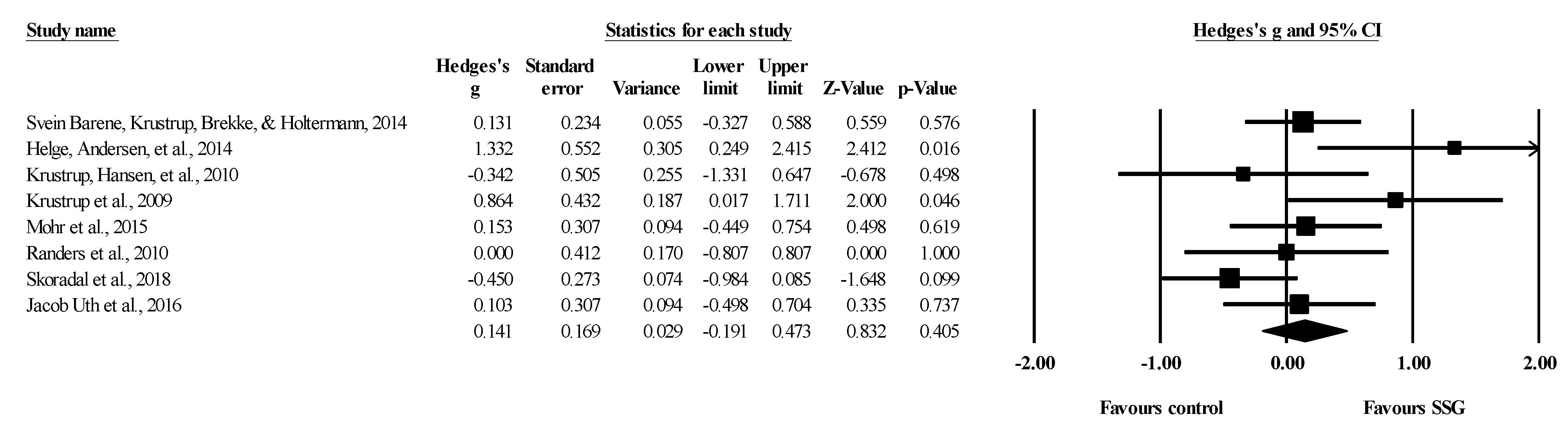
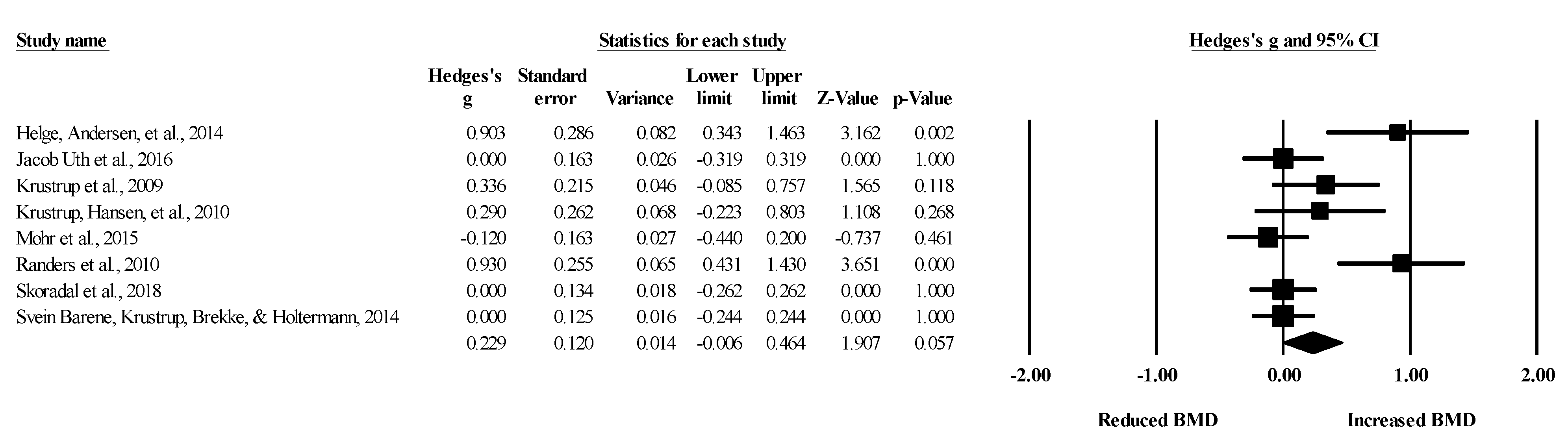
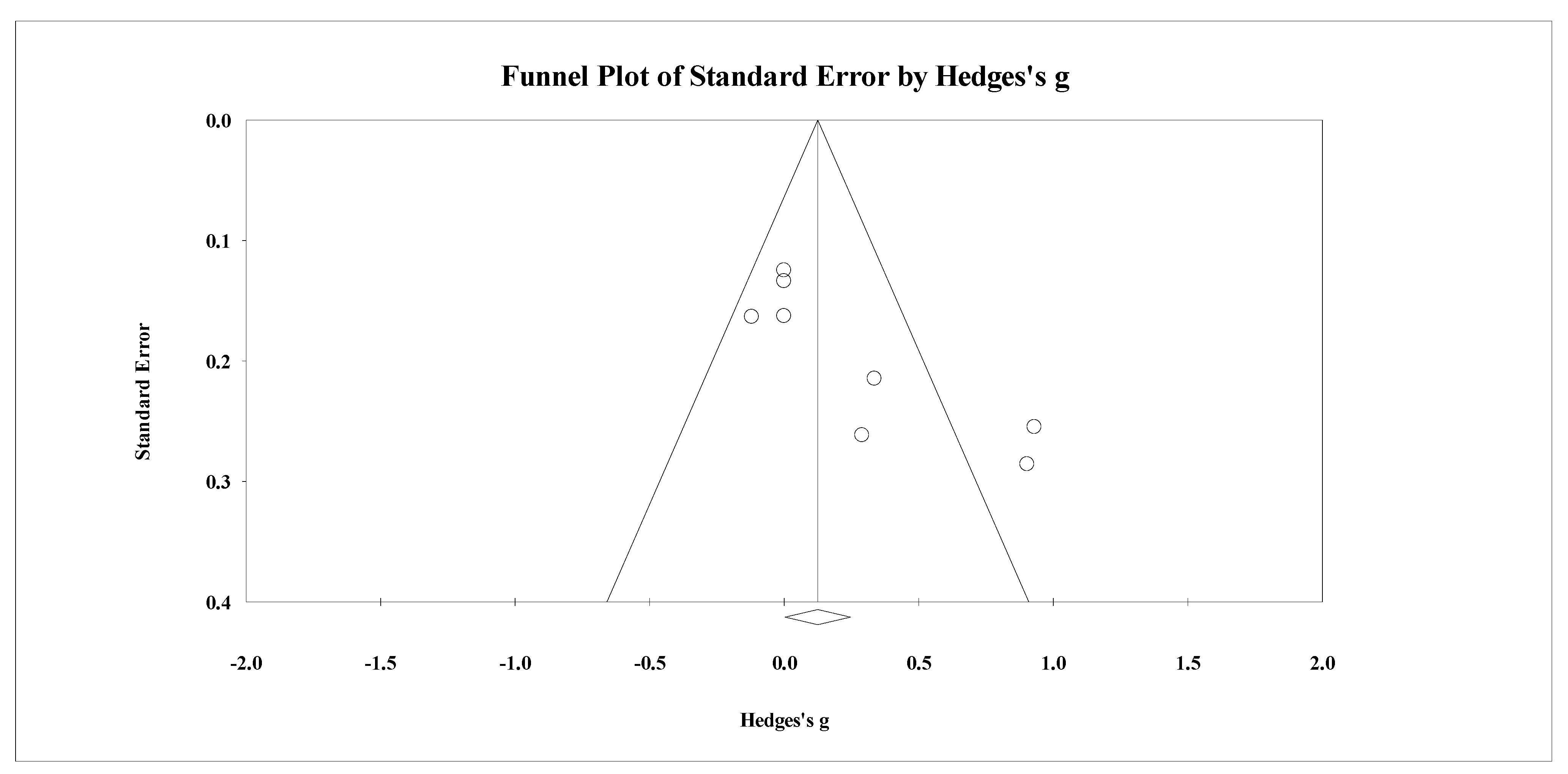
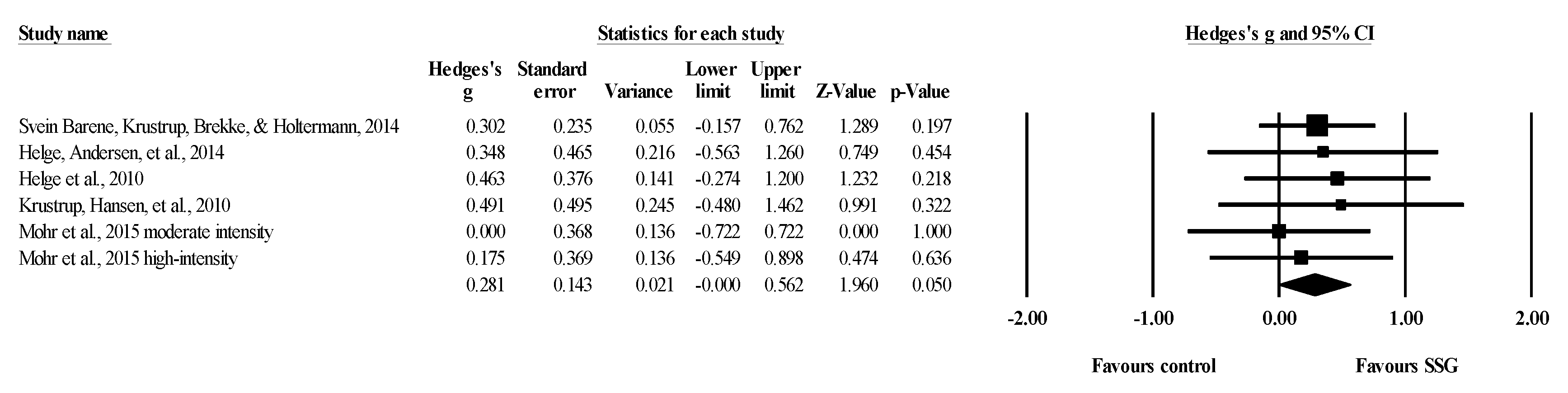
3.4. SSG vs. Control: Effects on Total Body BMD
3.5. SSG vs. Control: Effects on Spine BMD
3.6. SSG vs. Control: Effects on Pelvis BMD
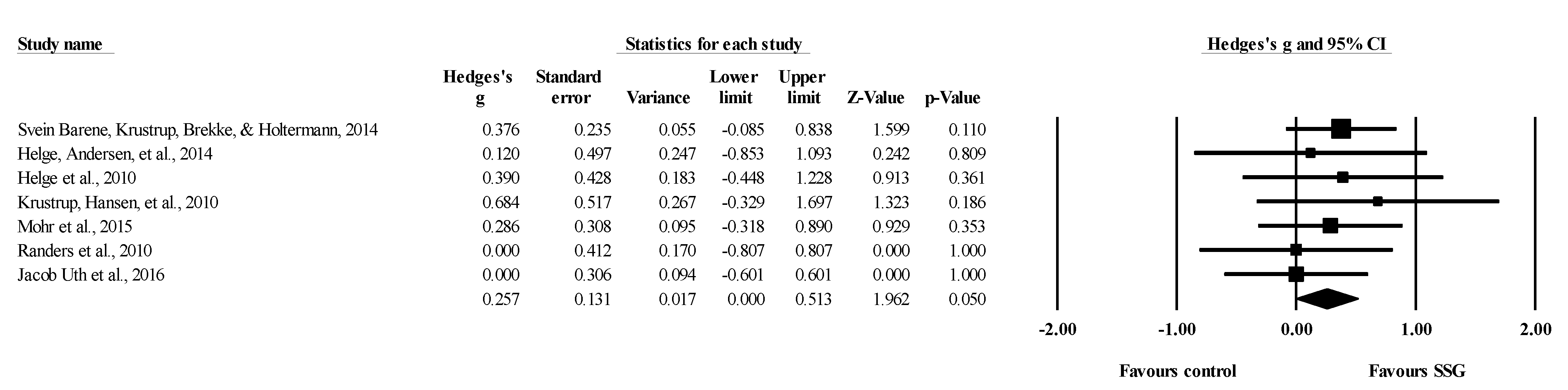
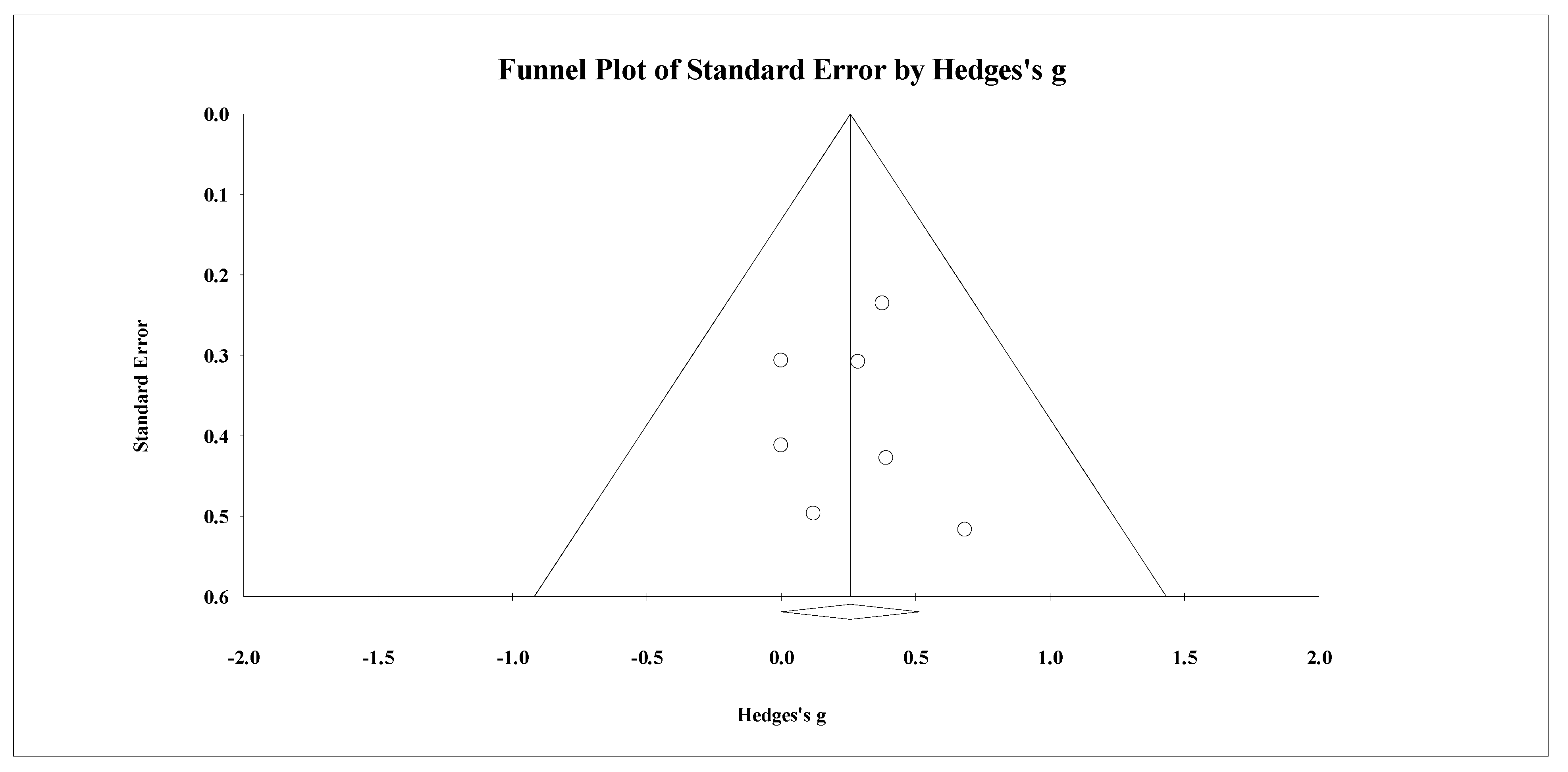
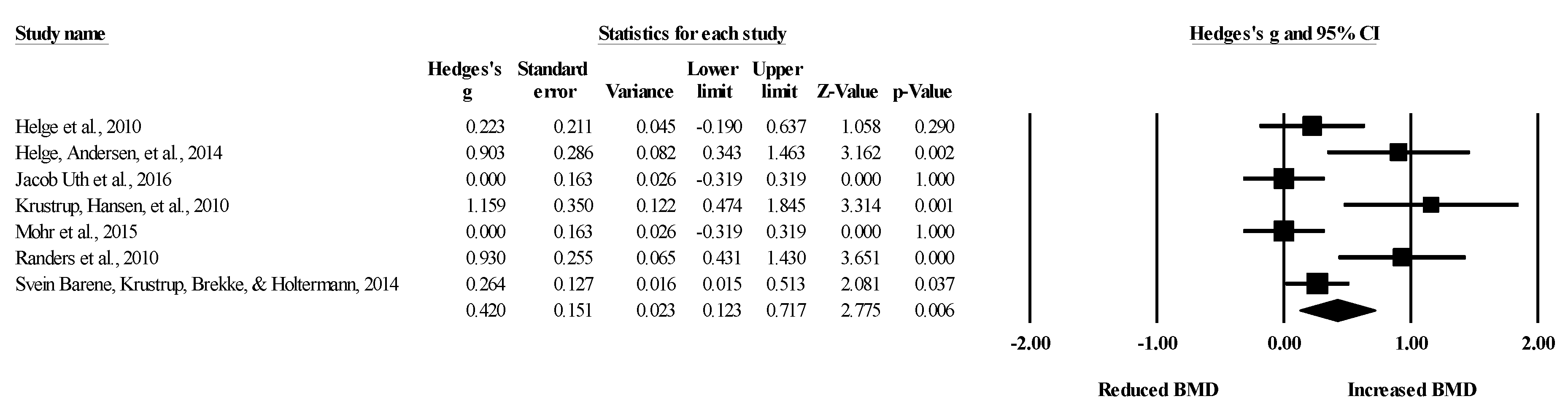
3.7. SSG vs. Control: Effects on Lower Limb BMD
4. Discussion
4.1. Effects of SSGs-Based Intervention on Total Body BMD
4.2. Effects of SSGs-Based Intervention on Lower Limb BMD
4.3. Effects of SSGs-Based Intervention on Spine and Pelvis
4.4. Study Limitations, Future Research and Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Morseth, B.; Emaus, N.; Jørgensen, L. Physical activity and bone: The importance of the various mechanical stimuli for bone mineral density. A review. Norsk Epidemiol. 2011, 20, 173–178. [Google Scholar] [CrossRef]
- MacKnight, J.M. Osteopenia and osteoporosis in female athletes. Clin. Sports Med. 2017, 36, 687–702. [Google Scholar] [CrossRef]
- Wang, N. Review of cellular mechanotransduction. J. Phys. D Appl. Phys. 2017, 50, 233002. [Google Scholar] [CrossRef]
- Mullender, M.G.; Huiskes, R. Proposal for the regulatory mechanism of Wolff’s law. J. Orthop. Res. 1995, 13, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Robling, A.G.; Turner, C.H. Mechanical signaling for bone modeling and remodeling. Crit. Rev. Eukaryot. Gene Express. 2009, 19, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Zernicke, R.; MacKay, C.; Lorincz, C. Mechanisms of bone remodeling during weight-bearing exercise. Appl. Physiol. Nutr. Metab. 2006, 31, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Guadalupe-Grau, A.; Fuentes, T.; Guerra, B.; Calbet, J.A.L. Exercise and bone mass in adults. Sport Med. 2009, 39, 439–468. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Shojaa, M.; Kohl, M.; von Stengel, S. Exercise effects on bone mineral density in older men: A systematic review with special emphasis on study interventions. Osteoporos. Int. 2018, 29, 1493–1504. [Google Scholar] [CrossRef]
- Duncan, R.L.; Turner, C.H. Mechanotransduction and the functional response of bone to mechanical strain. Calcif. Tissue Int. 1995, 57, 344–358. [Google Scholar] [CrossRef]
- Ammann, P.; Rizzoli, R. Bone strength and its determinants. Osteoporos. Int. 2003, 14, 13–18. [Google Scholar] [CrossRef]
- Turner, C.H. Biomechanics of bone: Determinants of skeletal fragility and bone quality. Osteoporos. Int. 2002, 13, 97–104. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A.; Oden, A.; Johansson, H.; De Laet, C.; Delmas, P.; Eisman, J.A.; Fujiwara, S.; Kroger, H.; Mellstrom, D.; et al. Predictive value of BMD for hip and other fractures. J. Bone Miner. Res. 2005, 20, 1185–1194. [Google Scholar] [CrossRef]
- Cummings, S.R.; Bates, D.; Black, D.M. Clinical use of bone densitometry. JAMA 2002, 288, 1889. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Shojaa, M.; Kohl, M.; von Stengel, S. Effects of different types of exercise on bone mineral density in postmenopausal women: A systematic review and meta-analysis. Calcif. Tissue Int. 2020, 107, 409–439. [Google Scholar] [CrossRef]
- Wayne, P.M.; Kiel, D.P.; Krebs, D.E.; Davis, R.B.; Savetsky-German, J.; Connelly, M.; Buring, J.E. The effects of tai chi on bone mineral density in postmenopausal women: A systematic review. Arch. Phys. Med. Rehabil. 2007, 88, 673–680. [Google Scholar] [CrossRef]
- Martyn-St James, M.; Carroll, S. Effects of different impact exercise modalities on bone mineral density in premenopausal women: A meta-analysis. J. Bone Miner. Metab. 2010, 28, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Abrahin, O.; Rodrigues, R.P.; Marçal, A.C.; Alves, E.A.C.; Figueiredo, R.C.; de Sousa, E.C. Swimming and cycling do not cause positive effects on bone mineral density: A systematic review. Rev. Bras. Reumatol. 2016, 56, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Bruton, A.; Montero-Marín, J.; González-Agüero, A.; García-Campayo, J.; Moreno, L.A.; Casajús, J.A.; Vicente-Rodríguez, G. The effect of swimming during childhood and adolescence on bone mineral density: A Systematic review and meta-analysis. Sport Med. 2016, 46, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Chilibeck, P.D.; Sale, D.G.; Webber, C.E. Exercise and bone mineral density. Sport Med. 1995, 19, 103–122. [Google Scholar] [CrossRef]
- Chao, D.; Foy, C.G.; Farmer, D. Exercise adherence among older adults. Control. Clin. Trials 2000, 21, S212–S217. [Google Scholar] [CrossRef]
- Owen, N.; Sugiyama, T.; Eakin, E.E.; Gardiner, P.A.; Tremblay, M.S.; Sallis, J.F. Adults’ sedentary behavior. Am. J. Prev. Med. 2011, 41, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Jekauc, D. Enjoyment during exercise mediates the effects of an intervention on exercise adherence. Psychology 2015, 06, 48–54. [Google Scholar] [CrossRef]
- Castagna, C.; de Sousa, M.; Krustrup, P.; Kirkendall, D.T. Recreational team sports: The motivational medicine. J. Sport Healh Sci. 2018, 7, 129–131. [Google Scholar] [CrossRef]
- Clemente, F.M.; Afonso, J.; Sarmento, H. Small-sided games: An umbrella review of systematic reviews and meta-analyses. PLoS ONE 2021, 16, e0247067. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, H.; Clemente, F.M.; Harper, L.D.; Costa, I.T.D.; Owen, A.; Figueiredo, A.J. Small sided games in soccer—a systematic review. Int. J. Perform. Anal. Sport 2018, 18, 693–749. [Google Scholar] [CrossRef]
- Krustrup, P.; Dvorak, J.; Junge, A.; Bangsbo, J. Executive summary: The health and fitness benefits of regular participation in small-sided football games. Scand. J. Med. Sci. Sports 2010, 20, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, H.; Manuel Clemente, F.; Marques, A.; Milanovic, Z.; David Harper, L.; Figueiredo, A. Recreational football is medicine against non-communicable diseases: A systematic review. Scand. J. Med. Sci. Sports 2020, 30, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Newton, R.U.; Ma’ayah, F.; Galvão, D.A.; Taaffe, D.R. Recreational soccer as sport medicine for middle-aged and older adults: A systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000336. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Čović, N.; Sporiš, G.; Mohr, M.; Krustrup, P. Broad-spectrum physical fitness benefits of recreational football: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 926–939. [Google Scholar] [CrossRef]
- Zouhal, H.; Hammami, A.; Tijani, J.M.; Jayavel, A.; de Sousa, M.; Krustrup, P.; Sghaeir, Z.; Granacher, U.; Ben Abderrahman, A. Effects of small-sided soccer games on physical fitness, physiological responses, and health indices in untrained individuals and clinical populations: A systematic review. Sport Med. 2020, 50, 987–1007. [Google Scholar] [CrossRef]
- Green, S.; Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2005. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Collaboration, C. Data Extraction Template for Included Studies. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/det_2015_revised_final_june_20_2016_nov_29_revised.doc (accessed on 2 January 2021).
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Abt, G.; Boreham, C.; Davison, G.; Jackson, R.; Nevill, A.; Wallace, E.; Williams, M. Power, precision, and sample size estimation in sport and exercise science research. J. Sports Sci. 2020, 38, 1933–1935. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: New York, NY, USA, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the cochrane library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sport. Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef] [PubMed]
- Barene, S.; Krustrup, P.; Brekke, O.L.; Holtermann, A. Soccer and Zumba as health-promoting activities among female hospital employees: A 40-weeks cluster randomised intervention study. J. Sports Sci. 2014, 32, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- Helge, E.W.; Andersen, T.R.; Schmidt, J.F.; Jørgensen, N.R.; Hornstrup, T.; Krustrup, P.; Bangsbo, J. Recreational football improves bone mineral density and bone turnover marker profile in elderly men. Scand. J. Med. Sci. Sports 2014, 24, 98–104. [Google Scholar] [CrossRef]
- Helge, E.W.; Aagaard, P.; Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Karlsson, M.K.; Krustrup, P. Recreational football training decreases risk factors for bone fractures in untrained premenopausal women. Scand. J. Med. Sci. Sports 2010, 20, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Hansen, P.R.; Andersen, L.J.; Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Christiansen, L.; Helge, E.W.; Pedersen, M.T.; Søgaard, P.; et al. Long-term musculoskeletal and cardiac health effects of recreational football and running for premenopausal women. Scand. J. Med. Sci. Sports 2010, 20, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Nielsen, J.J.; Krustrup, B.R.; Christensen, J.F.; Pedersen, H.; Randers, M.B.; Aagaard, P.; Petersen, A.M.; Nybo, L.; Bangsbo, J. Recreational soccer is an effective health-promoting activity for untrained men. Br. J. Sports Med. 2009, 43, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Mohr, M.; Helge, E.W.; Petersen, L.F.; Lindenskov, A.; Weihe, P.; Mortensen, J.; Jørgensen, N.R.; Krustrup, P. Effects of soccer vs swim training on bone formation in sedentary middle-aged women. Eur. J. Appl. Physiol. 2015, 115, 2671–2679. [Google Scholar] [CrossRef]
- Randers, M.B.; Nielsen, J.J.; Krustrup, B.R.; Sundstrup, E.; Jakobsen, M.D.; Nybo, L.; Dvorak, J.; Bangsbo, J.; Krustrup, P. Positive performance and health effects of a football training program over 12 weeks can be maintained over a 1-year period with reduced training frequency. Scand. J. Med. Sci. Sports 2010, 20, 80–89. [Google Scholar] [CrossRef]
- Skoradal, M.B.; Helge, E.W.; Jørgensen, N.R.; Mortensen, J.; Weihe, P.; Krustrup, P.; Mohr, M. Osteogenic impact of football training in 55 to 70-year-old women and men with prediabetes. Scand. J. Med. Sci. Sports 2018, 28, 52–60. [Google Scholar] [CrossRef]
- Uth, J.; Hornstrup, T.; Christensen, J.F.; Christensen, K.B.; Jørgensen, N.R.; Helge, E.W.; Schmidt, J.F.; Brasso, K.; Helge, J.W.; Jakobsen, M.D.; et al. Football training in men with prostate cancer undergoing androgen deprivation therapy: Activity profile and short-term skeletal and postural balance adaptations. Eur. J. Appl. Physiol. 2016, 116, 471–480. [Google Scholar] [CrossRef]
- Orchard, T.; Yildiz, V.; Steck, S.E.; Hébert, J.R.; Ma, Y.; Cauley, J.A.; Li, W.; Mossavar-Rahmani, Y.; Johnson, K.C.; Sattari, M.; et al. Dietary inflammatory index, bone mineral density, and risk of fracture in postmenopausal women: Results from the women’s health initiative. J. Bone Miner. Res. 2017, 32, 1136–1146. [Google Scholar] [CrossRef]
- Bruun, D.M.; Bjerre, E.; Krustrup, P.; Brasso, K.; Johansen, C.; Rørth, M.; Midtgaard, J. Community-based recreational football: A novel approach to promote physical activity and quality of life in prostate cancer survivors. Int. J. Environ. Res. Public Health 2014, 11, 5567–5585. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Furlini, G.; Zati, A.; Mauro, G.L. The effectiveness of physical exercise on bone density in osteoporotic patients. Biomed Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Castillo, D.; Raya-gonzález, J.; Yanci, J.; Clemente, F.M. Influence of pitch size on short-term high intensity actions and body impacts in soccer sided games. J. Hum. Kinet. 2021. [Google Scholar] [CrossRef]
- Di Salvo, V.; Gregson, W.; Atkinson, G.; Tordoff, P.; Drust, B. Analysis of high intensity activity in premier league soccer. Int. J. Sports Med. 2009, 30, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Brüggemann, G.P.; Rittweger, J. What do we currently know from in vivo bone strain measurements in humans? J. Musculoskelet. Neuronal Interact. 2011, 11, 8–20. [Google Scholar]
- Turner, C.H.; Robling, A.G. Designing exercise regimens to increase bone strength. Exerc. Sport Sci. Rev. 2003, 31, 45–50. [Google Scholar] [CrossRef]
- Muntean, L.; Rojas-Vargas, M.; Font, P.; Simon, S.P.; Rednic, S.; Schiotis, R.; Stefan, S.; Tamas, M.M.; Bolosiu, H.D.; Collantes-Estévez, E. Relative value of the lumbar spine and hip bone mineral density and bone turnover markers in men with ankylosing spondylitis. Clin. Rheumatol. 2011, 30, 691–695. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Untrained adults (>18 years old) from any sex, with or without a noncommunicable disease. Adults were not exposed to specific pharmacological or diet-oriented plans | Trained adults, athletes, youth (above 18 years old); participants were not exposed to specific pharmacological or diet-oriented plans |
| Intervention | SSG-based programs restricted to a minimum of 4 weeks (duration) and no restricted to frequency (number of sessions per week) | Other types of exercises; other types of SSGs; combined interventions (SSG and other types of exercise or intervention); or regular full-sized game (11 vs. 11); interventions with less than 4 weeks |
| Comparator | Passive or active control groups | Passive control with evidence of participation in structured exercise |
| Outcome | Pre-post intervention values (mean and standard deviation) of bone mineral density (BMD) measured in any body part | Other outcomes no, including bone mineral density (e.g., bone turnover markers); no information pre-post intervention (e.g., follow-up excluded); pre-post data the same in more than one article |
| Study Design | Randomized controlled trials | Nonrandomized studies |
| Additional criteria | Only original and full-text studies written in English | Written in another language than English; other article types than original (e.g., reviews, letters to editors, trial registrations, proposals for protocols, editorials, book chapters and conference abstracts) |
| Study | N | Mean Age (y) | Sex | Population | Type of Control Group | Test Used for Assessing the BMD | Body Parts Analyzed | Body Part Extracted for Meta-Analysis as Main Outcome |
|---|---|---|---|---|---|---|---|---|
| Barene et al. [43] | SSGs group: 37 Zumba group: 35 Passive control: 35 | SSGs group: 44.1 ± 8.7 Zumba group: 45.9 ± 9.6 Passive control: 47.4 ± 9.5 | Women a | Health female hospital employees | One active control group (Zumba) One passive control group | DXA | Total body (g/cm2) Lumbar spine (g/cm2) Lower limb (g/cm2) | Total body (g/cm2) Lumbar spine (g/cm2) Lower limb (g/cm2) |
| Helge et al. [44] | SSGs group: 9 Resistance training: 8 Passive control: 6 | SSGs group: 68.0 ± 4.0 Resistance training: 69.1 ± 3.1 Passive control: 67.4 ± 2.7 | Men | Healthy elderly | One active control group (resistance training) One passive control group | DXA | Femoral neck (g/cm2) Femoral shaft (g/cm2) Proximal femur (g/cm2) Whole body (g/cm2) | Whole body (g/cm2) Femoral shaft (right) (g/cm2) |
| Helge et al. [45] | SSGs group: 12 Running group: 16 Passive control: 9 | All: 36.3 ± 8.2 | Women | Premenopausal women | One active control group (running training) One passive control group | pQCT | Total distal tibia (mg/cm3) Trabecular distal tibia (mg/cm3) Cortical + subcortical distal tibia (mg/cm3) | Total distal tibia right (mg/cm3) |
| Krustrup et al. [46] | SSGs group: 7 Running group: 8 Passive control: 7 | SSGs group: 40 ± 3 Running group: 40 ± 2 Passive control: 38 ± 4 | Women | Premenopausal women | One active control group (running training) One passive control group | DXA | Whole body (g/cm2) Legs (g/cm2) | Whole body (g/cm2) Legs (g/cm2) |
| Krustrup et al. [47] | SSGs group: 12 Running group: 9 Passive control: 10 | SSGs group: 30 ± 2 Running group: 31 ± 2 Passive control: 30 ± 2 | Men | Healthy | One active control group (running training) One passive control group | DXA | Whole body (g/cm2) | Whole body (g/cm2) |
| Mohr et al. [48] | SSGs group: 21 Swimming moderate: 21 Swimming high: 21 Passive control: 20 | SSGs group: 45 ± 14 Swimming moderate: 46 ± 9 Swimming high: 44 ± 9 Passive control: 45 ± 9 | Women | Premenopausal women | Two active control group (swimming at moderate and high-intensity) One passive control group | DXA | Total body (g/cm2) Leg right (g/cm2) Pelvis (g/cm2) Arm (g/cm2) Head (g/cm2) | Total body (g/cm2) Leg right (g/cm2) Pelvis (g/cm2) |
| Randers et al. [49] | SSGs group: 12 Passive control: 10 | All: 20–43 | Men | Healthy | One passive control group | DXA | Total body (g/cm2) Leg (g/cm2) | Total body (g/cm2) Leg (g/cm2) |
| Skoradal et al. [50] | SSGs group: 32 (14 women) Passive control: 23 (11 women) | All: 61 ± 9 | Men and women | Prediabetes | One passive control group | DXA | Whole body (g/cm2) Head (g/cm2) Chest (g/cm2) Midriff (g/cm2) Pelvis (g/cm2) Arms (g/cm2) | Whole body (g/cm2) Midriff (g/cm2) Pelvis (g/cm2) |
| Uth et al. [51] | SSGs group: 21 Passive control: 20 | SSGs group: 67.1 ± 7.1 Passive control: 66.5 ± 4.9 | Men | Prostate cancer | One passive control group | DXA | Total body (g/cm2) Leg (g/cm2) | Total body (g/cm2) Leg (g/cm2) |
| Study | Duration (W) | d/w | Session/Person Per Week (n) | Total Sessions | SSG Formats | SSG Pitch Dimension (Length × Width) | SSG Area Per Player (m2) | Sets | Reps | Recovery between Sets (min) | Recovery between Sets (Intensity) | Total Work Duration (min) | Work Duration Per Set (min) | Work Intensity (HRmax) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barene et al. [43] | 40 W | 2–3 | 55.4 ± 8.8 | - | 3 vs.3 to 4 vs. 4 | 10 × 20 m | 25 to 33 | 2 | ND | 5 | - | 50 | 25 | 78.6 ± 3.2% |
| Helge et al. [44] | 52 W | ND | 1.7 ± 0.3 | ND | ND | ND | ND | 3–4 | ND | 2 | - | 45 | 15 | 82% |
| Helge et al. [45] | 14 W | 2 | ND | 28.8 ± 5.0 | 5 vs. 5, 7 vs. 7 and 9 vs.9 | 30 to 40 wide to 45 to 60 m long | ND | 4 | ND | ND | ND | 48 | 12 | 83 ± 0% |
| Krustrup et al. [46] | 16 W | 2 | 1.9 ± 0.1 to 1.7 ± 0.2 | ND | 4 vs. 4 to 5 vs. 5 | 20 to 30 wide × 30 to 40 m long | ND | ND | ND | ND | ND | 60 | ND | 82 ± 2% |
| Krustrup et al. [47] | 12 W | 2–3 | 2.3 | 27.6 | 5 vs. 5 to 7 vs. 7 | 40 × 60 m | 171 to 240 | 3–4 | ND | ND | ND | 60 | ND | 82 ± 2% |
| Mohr et al. [48] | 15 W | 3 | 3.0 ± 0.5 | 45 ± 5 | 4 vs. 4 to 10 vs. 10 | ND | ND | ND | ND | ND | ND | 60 | ND | ND |
| Randers et al. [49] | 64 W | ND | 1.3–2.4 | 28.5 + 66.7 | 4 vs. 4 to 5 vs. 5 | 25 to 40 wide × 30 to 50 m long | ND | ND | ND | ND | ND | 60 | ND | 81 ± 3 to 82 ± 2 |
| Skoradal et al. [50] | 16 W | 2 | 2.0 ± 0.1 | 32 ± 2 | 4 vs. 4 to 6 vs. 6 | ND | ND | 2 | ND | 2–3 | ND | 30–60 | 15–30 | 79 ± 1 |
| Uth et al. [51] | 12 W | 2–3 | ND | 20.6 ± 8.0 | 3 vs. 3 to 7 vs. 7 | 25 × 50 m for 6vs.6 | 100 | 2–3 | ND | ND | ND | 30–45 | 15 | ND |
| Study | Active Control | Passive Control |
|---|---|---|
| Barene et al. [43] | Continuous dance movement using Latin music with varying intensity. | Only measurements were made; no intervention |
| Helge et al. [44] | Resistance training: 5 min low-intensity warm-up, followed by leg press, seated leg extension, hamstring curl, pull-down, and lateral dumbbell raises. Sets were interspaced by 1.5 min rest, and at the end of the session, 5 min of core training was made. Exercise progressed from 3 × 16–20RM (week 0–4), 3 × 12RM (week 5–8), 3 × 10RM (week 9–12) and 4 × 8RM (week13–52). | Inactive; no details |
| Helge et al. [45] | Running group: 5 min of low-intensity warm-up, followed by 4 × 12 min of continuous running and moderate intensity. After the 6 weeks, all runners were able to run for 55 min continuously. | Inactive; no details |
| Krustrup et al. [46] | One hour of running two times a week. Running speed was adjusted to fit 81% HRmax during the first 4 weeks and 82% in the last 12 months. | Continued daily live activities |
| Krustrup et al. [47] | The participants completed 3 to 4 sets within one hour of running, with an average intensity of 82% HRmax. | Continued daily live activities |
| Mohr et al. [48] | Moderate intensity swim: one hour per session, continuous front crawl swimming High-intensity swim: 15–25 min per session (3–5 min of effective swimming) consisting of 6–10 sets of 30 s bouts of all-out front crawl swimming with 2 min of passive recovery. | No training or lifestyle changes during the same period |
| Randers et al. [49] | - | Instructed to remain physically inactive |
| Skoradal et al. [50] | - | No details |
| Uth et al. [51] | - | Encouraged to maintain their normal level of physical activity |
| No. 1 * | No. 2 | No. 3 | No. 4 | No. 5 | No. 6 | No. 7 | No. 8 | No. 9 | No. 10 | No. 11 | Total ** | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barene et al. [43] | + | + | + | + | - | - | - | + | + | + | + | 7 |
| Helge et al. [44] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| Helge et al. [45] | + | + | - | + | - | - | - | - | + | + | + | 5 |
| Krustrup et al. [46] | + | + | - | + | - | - | - | - | + | + | + | 5 |
| Krustrup et al. [47] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| Mohr et al. [48] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| Randers et al. [49] | + | + | - | + | - | - | - | - | + | + | + | 5 |
| Skoradal et al. [50] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| Uth et al. [51] | + | + | - | + | - | - | - | + | + | + | + | 6 |
| Study | Group | Sex | N | Before Mean ± SD | After Mean ± SD | After–Before (∆%) |
|---|---|---|---|---|---|---|
| Barene et al. [43] | SSG | W | 37 | 1.12 ± 0.09 | 1.12 ± 0.10 | 0.0 |
| Helge et al. [44] | SSG | M | 9 | 1.17 ± 0.04 | 1.21 ± 0.04 | 3.4 |
| Krustrup et al. [46] | SSG | W | 7 | 1.22 ± 0.03 | 1.23 ± 0.03 | 0.8 |
| Krustrup et al. [47] | SSG | M | 12 | 1.24 ± 0.03 | 1.25 ± 0.02 | 0.8 |
| Mohr et al. [48] | SSG | W | 21 | 1.00 ± 0.08 | 0.99 ± 0.08 | −1.0 |
| Randers et al. [49] | SSG | M | 12 | 1.30 ± 0.02 | 1.32 ± 0.02 | 1.5 |
| Skoradal et al. [50] | SSG | M&W | 32 | 1.01 ± 0.02 | 1.01 ± 0.02 | 0.0 |
| Uth et al. [51] | SSG | M | 21 | 1.17 ± 0.11 | 1.17 ± 0.11 | 0.0 |
| Barene et al. [43] | AC | W | 35 | 1.11 ± 0.08 | 1.11 ± 0.08 | 0.0 |
| Helge et al. [44] | AC | M | 8 | 1.23 ± 0.02 | 1.23 ± 0.02 | 0.0 |
| Krustrup et al. [46] | AC | W | 8 | 1.16 ± 0.03 | 1.16 ± 0.02 | 0.0 |
| Krustrup et al. [47] | AC | M | 9 | 1.33 ± 0.03 | 1.33 ± 0.03 | 0.0 |
| Mohr et al. [48] | AC1 | W | 21 | 1.00 ± 0.12 | 1.00 ± 0.11 | 0.0 |
| Mohr et al. [48] | AC2 | W | 21 | 1.00 ± 0.08 | 0.98 ± 0.08 | −2.0 |
| Randers et al. [49] | PC | M | 10 | 1.26 ± 0.03 | 1.28 ± 0.03 | 1.6 |
| Skoradal et al. [50] | PC | M&W | 23 | 1.02 ± 0.04 | 1.03 ± 0.03 | 1.0 |
| Uth et al. [51] | PC | M | 20 | 1.21 ± 0.14 | 1.20 ± 0.13 | −0.8 |
| Barene et al. [43] | PC | W | 35 | 1.11 ± 0.10 | 1.10 ± 0.10 | −0.9 |
| Helge et al. [44] | PC | M | 6 | 1.27 ± 0.03 | 1.27 ± 0.03 | 0.0 |
| Krustrup et al. [46] | PC | W | 7 | 1.19 ± 0.04 | 1.21 ± 0.04 | 1.7 |
| Krustrup et al. [47] | PC | M | 10 | 1.28 ± 0.03 | 1.27 ± 0.03 | −0.8 |
| Mohr et al. [48] | PC | W | 20 | 1.01 ± 0.09 | 0.99 ± 0.08 | −2.0 |
| Study | Group | Sex | N | Before Mean ± SD | After Mean ± SD | After–before ∆(%) |
|---|---|---|---|---|---|---|
| Barene et al. [43] | SSG | W | 37 | 1.12 ± 0.19 | 1.11 ± 0.17 | −0.9% |
| Skoradal et al. [50] | SSG | M and W | 32 | 1.38 ± 0.04 | 1.32 ± 0.04 | −4.3 |
| Barene et al. [43] | AC | W | 35 | 1.07 ± 0.13 | 1.07 ± 0.16 | 0.0% |
| Barene et al. [43] | PC | W | 35 | 1.10 ± 0.19 | 1.09 ± 0.18 | −0.9% |
| Skoradal et al. [50] | PC | M&W | 23 | 1.36 ± 0.07 | 1.33 ± 0.07 | −2.2 |
| Study | Group | Sex | N | Before Mean ± SD | After Mean ± SD | After–before (∆%) |
|---|---|---|---|---|---|---|
| Mohr et al. [48] | SSG | W | 21 | 1.06 ± 0.11 | 1.04 ± 0.11 | −1.9 |
| Skoradal et al. [50] | SSG | M&W | 32 | 1.12 ± 0.03 | 1.11 ± 0.03 | −0.9 |
| Mohr et al. [48] | AC1 | W | 21 | 1.12 ± 0.21 | 1.08 ± 0.20 | −3.6 |
| Mohr et al. [48] | AC2 | W | 21 | 1.04 ± 0.12 | 1.03 ± 0.13 | −1.0 |
| Mohr et al. [48] | PC | W | 20 | 1.09 ± 0.11 | 1.07 ± 0.13 | −1.8 |
| Skoradal et al. [50] | PC | M&W | 23 | 1.14 ± 0.05 | 1.13 ± 0.05 | −0.9 |
| Study | Group | Sex | N | Before Mean ± SD | After Mean ± SD | After–Before (∆%) |
|---|---|---|---|---|---|---|
| Barene et al. [43] | SSG | W | 37 | 2.24 ± 0.18 | 2.29 ± 0.19 | 2.2 |
| Helge et al. [44] | SSG | M | 9 | 1.12 ± 0.04 | 1.16 ± 0.04 | 3.6 |
| Helge et al. [45] | SSG | W | 12 | 301.4 ± 29.6 | 307.6 ± 28.7 | 2.1 |
| Krustrup et al. [46] | SSG | W | 7 | 1.32 ± 0.03 | 1.36 ± 0.03 | 3.0 |
| Mohr et al. [48] | SSG | W | 21 | 1.04 ± 0.08 | 1.04 ± 0.07 | 0.0 |
| Randers et al. [49] | SSG | M | 12 | 1.53 ± 0.03 | 1.56 ± 0.03 | 2.0 |
| Uth et al. [51] | SSG | M | 21 | 1.28 ± 0.13 | 1.28 ± 0.13 | 0.0 |
| Barene et al. [43] | AC | W | 35 | 2.26 ± 0.24 | 2.26 ± 0.23 | 0.0 |
| Helge et al. [44] | AC | M | 8 | 290.3 ± 19.5 | 293.6 ± 21.1 | 1.1 |
| Helge et al. [45] | AC | W | 16 | 1.24 ± 0.06 | 1.23 ± 0.06 | −0.8 |
| Krustrup et al. [46] | AC | W | 8 | 1.23 ± 0.02 | 1.26 ± 0.01 | 2.4 |
| Mohr et al. [48] | AC1 | W | 21 | 1.05 ± 0.09 | 1.05 ± 0.09 | 0.0 |
| Mohr et al. [48] | AC2 | W | 21 | 1.04 ± 0.07 | 1.03 ± 0.07 | −1.0 |
| Barene et al. [43] | PC | W | 35 | 2.29 ± 0.21 | 2.28 ± 0.23 | −0.4 |
| Helge et al. [44] | PC | M | 6 | 279.1 ± 34.1 | 276.5 ± 32.3 | −0.9 |
| Helge et al. [45] | PC | W | 9 | 1.24 ± 0.06 | 1.25 ± 0.06 | 0.8 |
| Krustrup et al. [46] | PC | W | 7 | 1.31 ± 0.04 | 1.33 ± 0.04 | 1.5 |
| Mohr et al. [48] | PC | W | 20 | 1.05 ± 0.10 | 1.03 ± 0.10 | −1.9 |
| Randers et al. [49] | PC | M | 10 | 1.41 ± 0.03 | 1.44 ± 0.04 | 2.1 |
| Uth et al. [51] | PC | M | 20 | 1.31 ± 0.16 | 1.31 ± 0.16 | 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemente, F.M.; Ramirez-Campillo, R.; Sarmento, H.; Castillo, D.; Raya-González, J.; Rosemann, T.; Knechtle, B. Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 457. https://doi.org/10.3390/healthcare9040457
Clemente FM, Ramirez-Campillo R, Sarmento H, Castillo D, Raya-González J, Rosemann T, Knechtle B. Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis. Healthcare. 2021; 9(4):457. https://doi.org/10.3390/healthcare9040457
Chicago/Turabian StyleClemente, Filipe Manuel, Rodrigo Ramirez-Campillo, Hugo Sarmento, Daniel Castillo, Javier Raya-González, Thomas Rosemann, and Beat Knechtle. 2021. "Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis" Healthcare 9, no. 4: 457. https://doi.org/10.3390/healthcare9040457
APA StyleClemente, F. M., Ramirez-Campillo, R., Sarmento, H., Castillo, D., Raya-González, J., Rosemann, T., & Knechtle, B. (2021). Effects of Recreational Small-Sided Soccer Games on Bone Mineral Density in Untrained Adults: A Systematic Review and Meta-Analysis. Healthcare, 9(4), 457. https://doi.org/10.3390/healthcare9040457