Impact of Internet Use on Elderly Health: Empirical Study Based on Chinese General Social Survey (CGSS) Data


Abstract
1. Introduction
2. Related Works
3. Methods
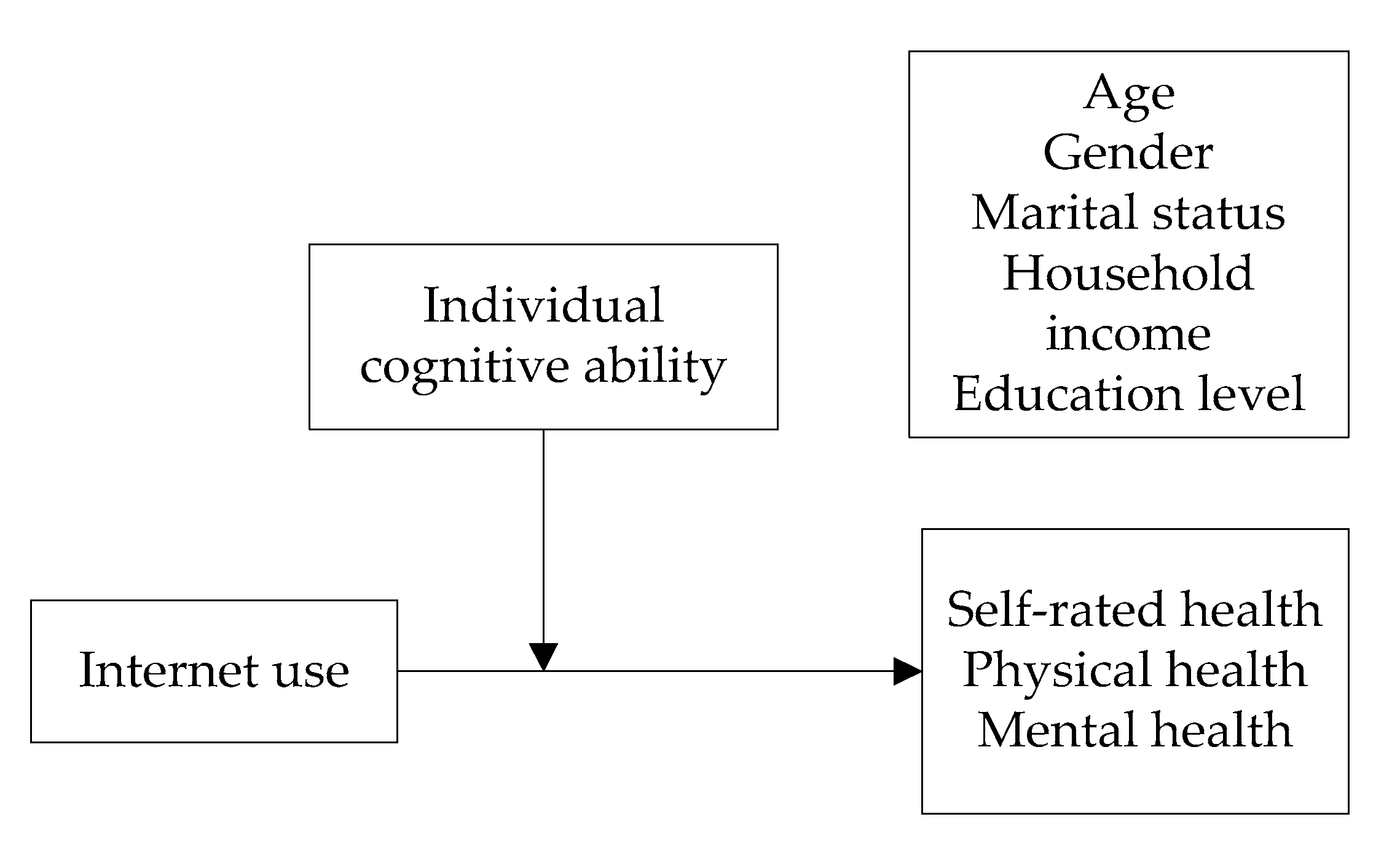
3.1. Study Design
3.2. Measures
3.2.1. Internet Use (Independent Variable)
3.2.2. Health Status (Dependent Variable)
3.2.3. Individual Cognitive Ability (Moderating Variable)
3.2.4. Sociodemographic Characteristics (Control Variable)
3.3. Hierarchical Regression Analysis
4. Results
4.1. Descriptive Statistics
4.2. Hierarchical Regression Analysis Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Bureau of Statistics, China. 2018 National Economic and Social Development Statistical Report; National Bureau of Statistics of China: Beijing, China, 2018.
- National Bureau of Statistics, China. 2019 National Economic and Social Development Statistical Report; National Bureau of Statistics of China: Beijing, China, 2019.
- Cangping Wu, X.J. On the strategy of “healthy Aging”. Soc. Sci. China 1996, 5, 52–64. [Google Scholar]
- Wang, H.T.; Wang, T.H.; Zhou, X.F.; Ni, Y.; Pan, Z.G. Health information needs regarding diabetes mellitus in China: An internet-based analysis. BMC Public Health 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Choi, J.; Kim, S.T. All things considered? Investigating the diversity of public affairs issues that individuals think about in the Internet age. Comput. Hum. Behav. 2014, 32, 112–122. [Google Scholar] [CrossRef]
- Alkalay, S.; Dolev, A. Public educational psychology services in Israel on the internet. Isr. J. Health Policy Res. 2019, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Babaei, G.; Bamdad, S. A multi-objective instance-based decision support system for investment recommendation in peer-to-peer lending. Expert Syst. Appl. 2020, 150, 1–11. [Google Scholar] [CrossRef]
- China Internet Nerwork Information Center, China. The 45th China Statistical Report on Internet Development; China Internet Nerwork Information Center: Beijing, China, 2020.
- Aalbers, T.; Baars, M.; Rikkert, M.O. Characteristics of effective Internet-mediated interventions to change lifestyle in people aged 50 and older: A systematic review. Ageing Res. Rev. 2011, 10, 487–497. [Google Scholar] [CrossRef]
- Cresci, M.K.; Jarosz, P.A.; Templin, T.N. Are health answers online for older adults? Educ. Gerontol. 2012, 38, 10–19. [Google Scholar] [CrossRef]
- Hakkarainen, P. ‘No good for shovelling snow and carrying firewood’: Social representations of computers and the internet by elderly Finnish non-users. New Media Soc. 2012, 14, 1198–1215. [Google Scholar] [CrossRef]
- Xue, X.D.; Ge, K.X. The effect of socioeconomic status on the health of the elderly in China: Evidence from the Chinese longitudinal healthy longevity survey. Popul. Dev. 2017, 23, 61–69. [Google Scholar] [CrossRef]
- Borg, C.; Hallberg, I.R.; Blomqvist, K. Life satisfaction among older people (65+) with reduced self-care capacity: The relationship to social, health and financial aspects. J. Clin. Nurs. 2006, 15, 607–618. [Google Scholar] [CrossRef]
- Schneider, G.; Driesch, G.; Kruse, A.; Wachter, M.; Nehen, H.-G.; Heuft, G. What influences self-perception of health in the elderly? The role of objective health condition, subjective well-being and sense of coherence. Arch. Gerontol. Geriatr. 2004, 39, 227–237. [Google Scholar] [CrossRef] [PubMed]
- WHO. Constitution of the World Health Organisation; World Health Organization: Geneva, Switzerland, 1948.
- Zhang, C.; Zhang, D. The influences of social activities on urban elderly people’s health: Based on CHARLS2011. Popul. Econ. 2016, 5, 55–63. [Google Scholar] [CrossRef]
- Zimmer, Z.; Kwong, J. Socioeconomic status and health among older adults in rural and urban China. J. Aging Health 2004, 16, 44–70. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zheng, J.; Kurosawa, M.; Inaba, Y. Relationships between age and gender differentials in health among older people in China. Agng Soc. 2009, 29, 1141–1154. [Google Scholar] [CrossRef]
- Angelini, V.; Cavapozzi, D.; Corazzini, L.; Paccagnella, O. Age, health and life satisfaction among older Europeans. Soc. Indic. Res. 2012, 105, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Manaf, M.R.A.; Mustafa, M.; Rahman, M.R.A.; Yusof, K.H.; Aziz, N.A.A. factors influencing the prevalence of mental health problems among malay elderly residing in a rural community: A cross sectional study. PLoS ONE 2016, 11, e0156937. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Ahn, K.-S.; Cho, K.-H.; Kang, C.H.; Cho, S.B.; Han, K.; Rho, Y.-K.; Park, Y.-G. Gender differences in the relationship between socioeconomic status and height loss among the elderly in South Korea. Medicine 2017, 96, e7131. [Google Scholar] [CrossRef]
- Liu, C.P.; Wang, L.J. A study of the impact of socio-economic status on the health of the elderly. Chin. J. Popul. Sci. 2017, 5, 40–50. [Google Scholar]
- Schetter, C.D.; Schafer, P.; Lanzi, R.G.; Clark-Kauffman, E.; Raju, T.N.K.; Hillemeier, M.M. The community child health network shedding light on the mechanisms underlying health disparities through community participatory methods: The stress pathway. Perspect. Psychol. Sci. 2013, 8, 613–633. [Google Scholar] [CrossRef]
- Wang Hongliang, Z.X. Analysis on the influencing factors of health difference between middle-aged and elderly population. Chin. J. Popul. Sci. 2018, 3, 109–120. [Google Scholar]
- Cutler, D.M.; Lleras-Muney, A. Understanding differences in health behaviors by education. J. Health Econ. 2010, 29, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Gracia, E.; Herrero, J. Internet use and self-rated health among older people: A national survey. J. Med. Internet Res. 2009, 11, e49. [Google Scholar] [CrossRef] [PubMed]
- Wang, L. The influence mechanism of internet use on the physical and mental health of the elderly—An empirical analysis based on CGSS2013 data. Mod. Econ. Res. 2018, 4, 101–108. [Google Scholar]
- Bolle, S.; Van Weert, J.C.M.; Daams, J.G.; Loos, E.F.; De Haes, H.C.J.M.; Smets, E.M.A. Online health information tool effectiveness for older patients: A systematic review of the literature. J. Health Commun. 2015, 20, 1067–1083. [Google Scholar] [CrossRef]
- Bolle, S.; Romijn, G.A.; Smets, E.M.A.; Loos, E.F.; Kunneman, M.; van Weert, J. Older cancer patients’ user experience of online health information tools: A think aloud study. J. Med. Internet Res. 2016, 18, e208. [Google Scholar] [CrossRef]
- Meischke, H.; Eisenberg, M.; Rowe, S.; Cagle, A. Do older adults use the Internet for information on heart attacks? Results from a survey of seniors in King County, Washington. Heart Lung 2005, 34, 3–12. [Google Scholar] [CrossRef]
- Quintana, D.; Cervantes, A.; Sáez, Y.; Isasi, P. Internet use and psychological well-being at advanced age: Evidence from the English longitudinal study of aging. Int. J. Environ. Res. Public Health 2018, 15, 480. [Google Scholar] [CrossRef]
- Heo, J.; Chun, S.; Lee, S.; Lee, K.H.; Kim, J. Internet use and well-being in older adults. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 268–272. [Google Scholar] [CrossRef]
- Lelkes, O. Happier and less isolated: Internet use in old age. J. Poverty Soc. Justice 2013, 21, 33–46. [Google Scholar] [CrossRef]
- Han, X.; Shi, D.; Zhou, X.; Yang, Y.; Zhu, Z. The training and transfer effect of cognitive training in old adults. Adv. Psychol. Sci. 2016, 24, 909–922. [Google Scholar] [CrossRef]
- Song, X.; Chen, G. Effects of chronic physical diseases and cognitive ability on self-care ability in elderly. Chin. J. Popul. Sci. 2001, S1, 42–47. [Google Scholar] [CrossRef]
- Schaie, K.W. The hazards of cognitive aging. Gerontologist 1989, 29, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Lövdén, M.; Bäckman, L.; Lindenberger, U.; Schaefer, S.; Schmiedek, F. A theoretical framework for the study of adult cognitive plasticity. Psychol. Bull. 2010, 136, 659–676. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. Selective review of cognitive aging. J. Int. Neuropsychol. Soc. 2010, 16, 754–760. [Google Scholar] [CrossRef]
- Peng, H.; Wang, D.-H. The cognitive mechanisms of primary mental abilities aging. Adv. Psychol. Sci. 2012, 20, 1251–1258. [Google Scholar] [CrossRef]
- Maitra, S. Can patient self-management explain the health gradient? Goldman and Smith’s “Can patient self-management help explain the SES health gradient?” (2002) revisited. Soc. Sci. Med. 2010, 70, 802–812. [Google Scholar] [CrossRef]
- Wang, B. The determinants of the Chinese elderly’s internet use from a multidimensional perspective. Popul. Dev. 2020, 26, 98–106. [Google Scholar]
- Erhag, H.F.; Ahlner, F.; Sterner, T.R.; Skoog, I.; Bergström, A. Internet use and self-rated health among Swedish 70-year-olds: A cross-sectional study. BMC Geriatr. 2019, 19, 365. [Google Scholar] [CrossRef]
- Lam, S.S.M.; Jivraj, S.; Scholes, S. Exploring the relationship between internet use and mental health among older adults in England: Longitudinal observational study. J. Med. Internet Res. 2020, 22, e15683. [Google Scholar] [CrossRef]
- Forsman, A.K.; Nordmyr, J. Psychosocial links between internet use and mental health in later life: A systematic review of quantitative and qualitative evidence. J. Appl. Gerontol. 2017, 36, 1471–1518. [Google Scholar] [CrossRef]
- Chyi, H.; Chyi, H.; Mao, S.; Mao, S. The determinants of happiness of China’s elderly population. J. Happiness Stud. 2012, 13, 167–185. [Google Scholar] [CrossRef]
- Liang, Y.; Wang, P. Influence of prudential value on the subjective well-being of Chinese urban–rural residents. Soc. Indic. Res. 2013, 118, 1249–1267. [Google Scholar] [CrossRef]
- Lubinski, D. Exceptional cognitive ability: The phenotype. Behav. Genet. 2009, 39, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Anna, P.; Kroncke, M.W.; Huckabee, H. Assessment of Autism Spectrum Disorder; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Sims, T.; Reed, A.E.; Carr, D.C. Information and communication technology use is related to higher well-being among the oldest-old. J. Gerontol. Ser. B 2016, 72, 761–770. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | 2012 | 2015 | ||
|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | |
| Internet use | 1.22 | 0.785 | 1.35 | 0.934 |
| Self-rated health | 3.01 | 1.053 | 3.18 | 1.062 |
| Physical health | 3.42 | 1.217 | 3.45 | 1.117 |
| Mental health | 3.73 | 1.038 | 3.72 | 0.927 |
| Individual cognitive ability | 2.06 | 0.607 | 2.09 | 0.607 |
| Gender | 0.56 | 0.497 | 0.49 | 0.500 |
| Age | 69.10 | 7.209 | 69.39 | 7.469 |
| Marital status | 0.73 | 0.444 | 0.74 | 0.436 |
| Household income | 43,072.49 | 269,983.171 | 61,361.82 | 380,656.167 |
| Education level | 2.40 | 1.276 | 2.39 | 1.263 |
| N | 2821 | 2821 | 3185 | 3185 |
| Predictor | 2012 | 2015 | ||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Age | −0.08 * (0.003) | −0.07 * (0.003) | −0.06 * (0.003) | −0.011 *** (0.003) | −0.010 *** (0.003) | −0.010 *** (0.003) |
| Gender | 0.179 *** (0.041) | 0.191 *** (0.041) | 0.192 *** (0.041) | 0.188 *** (0.039) | 0.214 *** (0.038) | 0.216 *** (0.039) |
| Marital status | 0.05 (0.048) | 0.05 (0.048) | 0.05 (0.048) | −0.011 (0.045) | −0.018 (0.045) | −0.021 (0.045) |
| Household income | 1.902 × 10−7 * (0.000) | 1.690 × 10−7 * (0.000) | 1.700 × 10−7 * (0.000) | 1.248 × 10−7 * (0.000) | 1.266 × 10−7 ** (0.000) | 1.245 × 10−7 ** (0.000) |
| Education level | 0.114 *** (0.016) | 0.054 ** (0.019) | 0.045 * (0.019) | 0.069 *** (0.015) | −0.001 (0.018) | −0.009 (0.018) |
| Individual cognitive ability | 0.224 *** (0.039) | 0.215 *** (0.039) | 0.270 *** (0.036) | 0.261 *** (0.036) | ||
| Internet use | 0.048 (0.027) | 0.033 (0.022) | ||||
| Constant | 3.143 *** (0.217) | 2.725 *** (0.228) | 2.685 *** (0.229) | 3.704 *** (0.199) | 3.218 *** (0.207) | 3.188 *** (0.208) |
| Adjusted R2 | 0.042 | 0.053 | 0.053 | 0.026 | 0.043 | 0.043 |
| Predictor | 2012 | 2015 | ||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Age | −0.13 *** (0.003) | −0.11 ** (0.003) | −0.11 ** (0.003) | −0.012 *** (0.003) | −0.011 *** (0.003) | −0.010 *** (0.003) |
| Gender | 0.116 * (0.047) | 0.129 ** (0.047) | 0.131 *** (0.047) | 0.171 *** (0.040) | 0.203 *** (0.040) | 0.207 *** (0.040) |
| Marital status | 0.006 (0.055) | 0.005 (0.055) | 0.009 (0.055) | −0.045 (0.047) | −0.054 (0.046) | −0.058 (0.046) |
| Household income | 1.299 × 10−7 (0.000) | 1.069 × 10−7 (0.000) | 1.092 × 10−7 (0.000) | 1.468 × 10−7 ** (0.000) | 1.508 × 10−7 ** (0.000) | 1.466 × 10−7 ** (0.000) |
| Education level | 0.212 *** (0.018) | 0.128 *** (0.022) | 0.126 *** (0.022) | 0.169 *** (0.016) | 0.083 ** (0.018) | 0.068 *** (0.019) |
| Individual cognitive ability | 0.243 *** (0.044) | 0.224 *** (0.044) | 0.331 *** (0.037) | 0.314 *** (0.038) | ||
| Internet use | 0.106 ** (0.031) | 0.064 ** (0.023) | ||||
| Constant | 3.719 *** (0.248) | 3.264 *** (0.260) | 3.176 *** (0.261) | 3.851 *** (0.205) | 3.256 *** (0.214) | 3.197 *** (0.214) |
| Adjusted R2 | 0.067 | 0.077 | 0.080 | 0.060 | 0.082 | 0.084 |
| Predictor | 2012 | 2015 | ||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Age | 0.001 (0.003) | 0.003 (0.003) | 0.004 (0.003) | −0.001 (0.002) | 0.001 (0.002) | 0.001 *** (0.002) |
| Gender | 0.078 (0.040) | 0.095 * (0.039) | 0.097 * (0.039) | 0.075 * (0.034) | 0.099 ** (0.033) | 0.102 ** (0.033) |
| Marital status | 0.142 ** (0.047) | 0.140 ** (0.046) | 0.143 * (0.046) | 0.034 (0.039) | 0.027 (0.039) | 0.023 (0.046) |
| Household income | 1.684 × 10−7 * (0.000) | 1.372 × 10−7 * (0.000) | 1.391 × 10−7 * (0.000) | 5.670 × 10−8 (0.000) | 5.838 × 10−8 (0.000) | 5.465 × 10−8 (0.000) |
| Education level | 0.198 *** (0.015) | 0.329 *** (0.037) | 0.095 *** (0.019) | 0.121 *** (0.013) | 0.057 ** (0.015) | 0.043 ** (0.016) |
| Individual cognitive ability | 0.329 *** (0.037) | 0.314 *** (0.037) | 0.250 *** (0.031) | 0.234 *** (0.032) | ||
| Internet use | 0.083 ** (0.026) | 0.057 ** (0.019) | ||||
| Constant | 3.023 *** (0.210) | 2.408 *** (0.219) | 2.338 *** (0.219) | 3.431 *** (0.173) | 2.981 *** (0.180) | 2.929 *** (0.214) |
| Adjusted R2 | 0.077 | 0.102 | 0.105 | 0.033 | 0.052 | 0.054 |
| Predictor | 2012 | 2015 | ||||
|---|---|---|---|---|---|---|
| Self-Rated Health | Physical Health | Mental Health | Self-Rated Health | Physical Health | Mental Health | |
| Age | −0.006 * (0.003) | −0.010 ** (0.003) | 0.004 (0.003) | −0.010 *** (0.003) | −0.010 *** (0.003) | 0.001 (0.002) |
| Gender | 0.192 *** (0.041) | 0.132 ** (0.47) | 0.097 * (0.039) | 0.214 *** (0.039) | 0.204 *** (0.040) | 0.100 ** (0.033) |
| Marital status | 0.050 (0.048) | 0.006 (0.055) | 0.142 ** (0.046) | −0.024 (0.045) | −0.062 (0.046) | 0.019 (0.039) |
| Household income | 1.687 × 10−7 * (0.000) | 1.066 × 10−7 (0.000) | 1.375 × 10−7 * (0.000) | 1.257 × 10−7 ** (0.000) | 1.481 × 10−7 ** (0.000) | 5.616 × 10−8 (0.000) |
| Education level | 0.045 * (0.019) | 0.126 *** (0.022) | 0.095 *** (0.019) | −0.009 (0.018) | 0.069 *** (0.019) | 0.044 ** (0.016) |
| Individual cognitive ability | 0.220 *** (0.039) | 0.234 *** (0.045) | 0.320 *** (0.038) | 0.267 *** (0.037) | 0.322 *** (0.038) | 0.242 *** (0.032) |
| Internet use | 0.086 * (0.035) | 0.178 *** (0.040) | 0.126 *** (0.034) | 0.057 * (0.027) | 0.096 ** (0.038) | 0.089 ** (0.023) |
| Internet use * Individual cognitive ability | −0.029 (0.017) | −0.056 ** (0.020) | −0.033 * (0.017) | −0.027 (0.017) | −0.036 * (0.17) | −0.036 * (0.015) |
| Constant | 2.634 *** (0.231) | 3.077 *** (0.263) | 2.280 *** (0.221) | 3.150 *** (0.209) | 3.147 *** (0.216) | 2.879 *** (0.182) |
| Adjusted R2 | 0.054 | 0.082 | 0.106 | 0.044 | 0.085 | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Liang, C.; Li, K. Impact of Internet Use on Elderly Health: Empirical Study Based on Chinese General Social Survey (CGSS) Data. Healthcare 2020, 8, 482. https://doi.org/10.3390/healthcare8040482
Wang J, Liang C, Li K. Impact of Internet Use on Elderly Health: Empirical Study Based on Chinese General Social Survey (CGSS) Data. Healthcare. 2020; 8(4):482. https://doi.org/10.3390/healthcare8040482
Chicago/Turabian StyleWang, Jing, Changyong Liang, and Keqing Li. 2020. "Impact of Internet Use on Elderly Health: Empirical Study Based on Chinese General Social Survey (CGSS) Data" Healthcare 8, no. 4: 482. https://doi.org/10.3390/healthcare8040482
APA StyleWang, J., Liang, C., & Li, K. (2020). Impact of Internet Use on Elderly Health: Empirical Study Based on Chinese General Social Survey (CGSS) Data. Healthcare, 8(4), 482. https://doi.org/10.3390/healthcare8040482