
EASY-NET Program: Effectiveness of an Audit and Feedback Intervention in the Emergency Care for Acute Conditions in the Lazio Region

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
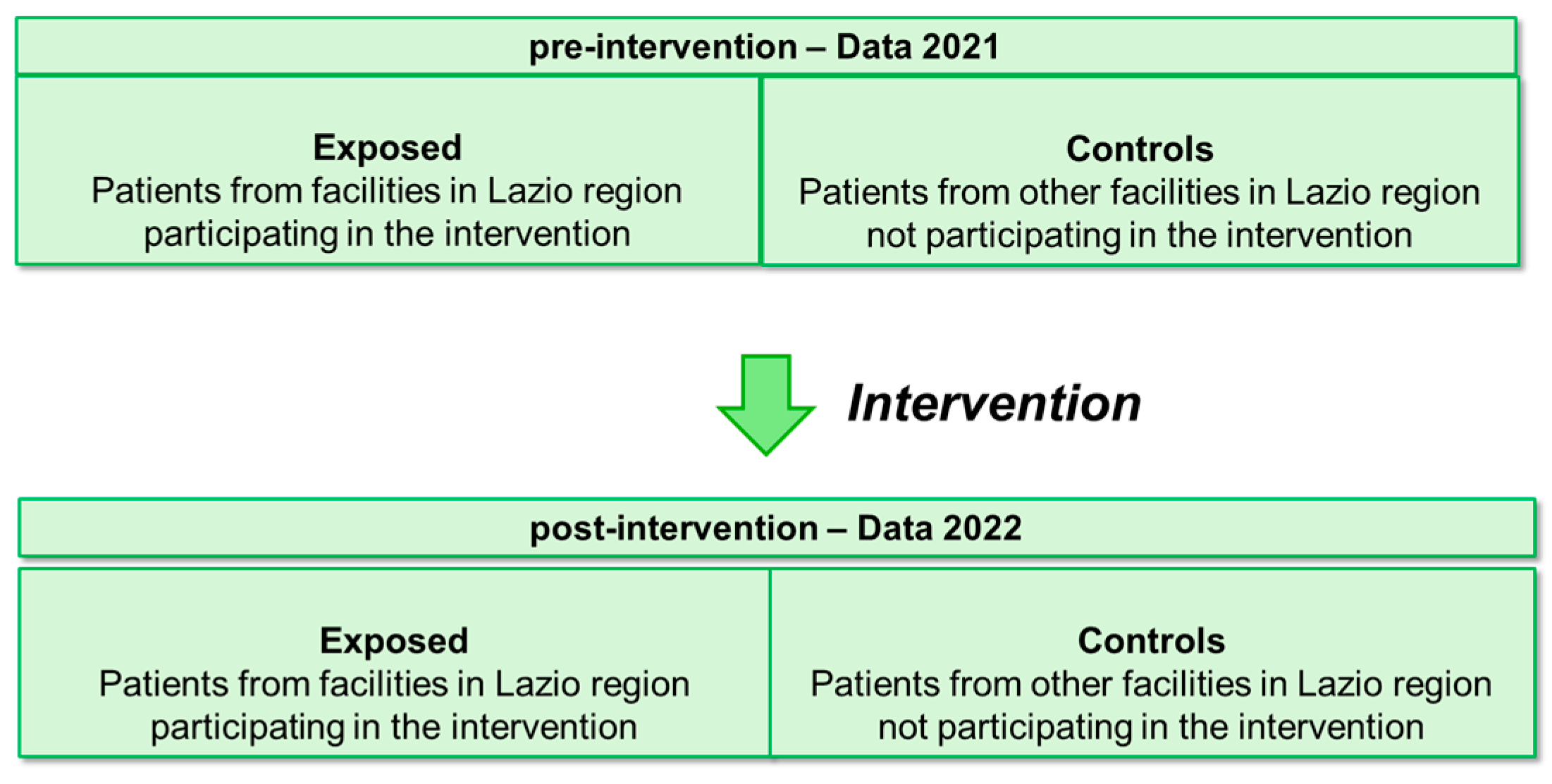
2.1. Study Design, Participants, and Patients
- -
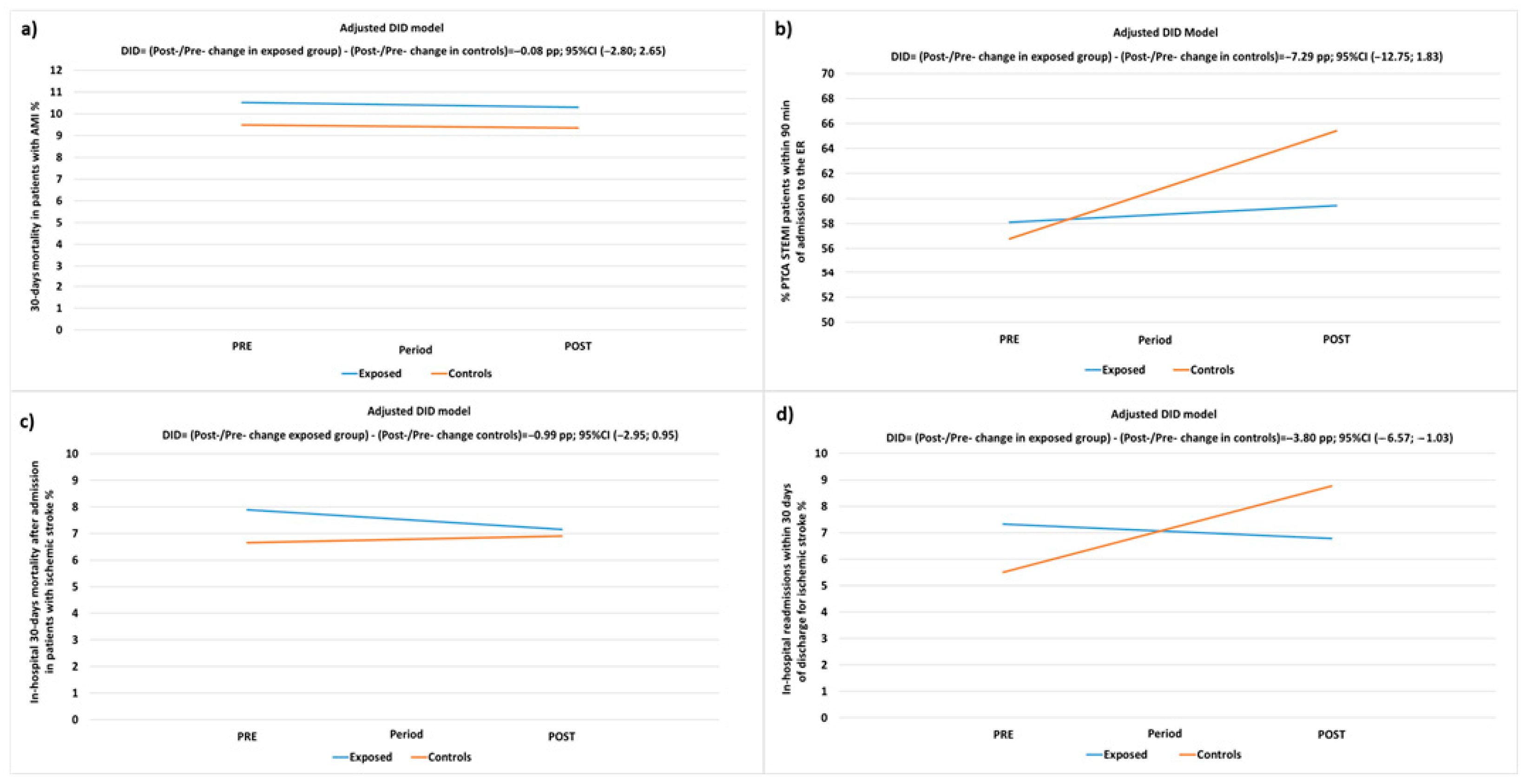
- A 30-day mortality rate after hospital admission in patients with AMI;
- -
- Proportion of PTCA (percutaneous transluminal coronary angioplasty) performed in STEMI (ST-elevation myocardial infarction) patients within 90 min of admittance to the hospital emergency room (ER);
- -
- In-hospital mortality in patients with ischemic stroke;
- -
- Proportion of hospital readmissions within 30 days of discharge in patients with ischemic stroke.
2.2. A&F Intervention and Control Group
- -
- Arranging regular meetings to update on project activities, as well as to present and discuss the contents of the feedback;
- -
- Subsequent to each meeting, the feedback report was disseminated via email in various formats (comprising a comprehensive main document and a hospital-specific PowerPoint presentation) to the designated contact person within the hospital (pertaining to AMI and/or stroke, respectively). Simultaneously, a form was provided to gather information on audit meetings conducted after the feedback;
- -
- Issuing formal invitations to plan and execute audit meetings after each feedback session;
- -
- Returning the completed form containing details on the characteristics of the conducted audits (such as date, participants, discussion points on indicators, identification of improvement activities, audit minutes, etc.) to the research group.
2.3. Data Sources
2.4. Variables in Analysis
2.5. Data Management and Statistical Analysis
3. Results
3.1. Participating Hospitals
3.2. Patient Populations
3.2.1. AMI Patient Cohort
3.2.2. STEMI Patient Cohort
3.2.3. Ischemic Stroke Patient Cohort
Thirty-Day In-Hospital Mortality after First Hospital Admission in Patients with Ischemic Stroke
Proportion of Hospital Readmission within 30 Days of Discharge for Ischemic Stroke
3.3. Intervention Effectiveness Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Programma Nazionale Esiti—Edition 2021. Available online: https://www.agenas.gov.it/comunicazione/primo-piano/2005-pne-2021-agenas-presenta-i-risultati-al-ministero-della-salute (accessed on 10 September 2022).
- P.Re.Val.E. (Programma Regionale Valutazione Esiti”—Regional Program for Outcomes and Processes Evaluation) Edition 2022 Web Sites. Available online: https://www.dep.lazio.it/prevale2022/ (accessed on 15 September 2023).
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2012, 6, 1465–1858. [Google Scholar] [CrossRef] [PubMed]
- Desveaux, L.; Ivers, N.M.; Devotta, K.; Ramji, N.; Weyman, K.; Kiran, T. Unpacking the intention to action gap: A qualitative study understanding how physicians engage with audit and feedback. Implement. Sci. 2021, 16, 19. [Google Scholar] [CrossRef]
- Moore, L.; Guertin, J.R.; Tardif, P.-A.; Ivers, N.M.; Hoch, J.; Conombo, B.; Antony, J.; Stelfox, H.T.; Berthelot, S.; Archambault, P.; et al. Economic evaluations of audit and feedback interventions: A systematic review. BMJ Qual. Saf. 2022, 31, 754–767. [Google Scholar] [CrossRef] [PubMed]
- Schondelmeyer, A.C.; Bettencourt, A.P.; Xiao, R.; Beidas, R.S.; Wolk, C.B.; Landrigan, C.P.; Brady, P.W.; Brent, C.R.; Parthasarathy, P.; Kern-Goldberger, A.S.; et al. Evaluation of an Educational Outreach and Audit and Feedback Program to Reduce Continuous Pulse Oximetry Use in Hospitalized Infants with Stable Bronchiolitis: A Nonrandomized Clinical Trial. JAMA Netw. Open 2021, 4, e2122826. [Google Scholar] [CrossRef]
- Goulao, B.; Scott, C.; Black, I.; Clarkson, J.; McArthur, L.; Ramsay, C.; Young, L.; Duncan, E. Audit and feedback with or without training in-practice targeting antibiotic prescribing (TiPTAP): A study protocol of a cluster randomised trial in dental primary care. Implement. Sci. 2021, 16, 32. [Google Scholar] [CrossRef]
- Lau, R.; Stevenson, F.; Ong, B.N.; Dziedzic, K.; Treweek, S.; Eldridge, S.; Everitt, H.; Kennedy, A.; Qureshi, N.; Rogers, A.; et al. Achieving change in primary care-effectiveness of strategies for improving implementation of complex interventions: Systematic review of reviews. BMJ Open 2015, 5, e009993. [Google Scholar] [CrossRef]
- Tuti, T.; Nzinga, J.; Njoroge, M.; Brown, B.; Peek, N.; English, M.; Paton, C.; van der Veer, S.N. A systematic review of electronic audit and feedback: Intervention effectiveness and use of behaviour change theory. Implement. Sci. 2017, 12, 61. [Google Scholar] [CrossRef]
- Chatzopoulou, M.; Kyriakaki, A.; Reynolds, L. Review of antimicrobial resistance control strategies: Low impact of prospective audit with feedback on bacterial antibiotic resistance within hospital settings. Infect. Dis. 2021, 53, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Ivers, N.M.; Grimshaw, J.M.; Jamtvedt, G.; Flottorp, S.; O’brien, M.A.; French, S.D.; Young, J.; Odgaard-Jensen, J. Growing literature, stagnant Science? Systematic review, meta-regression and cumulative analysis of audit and feedback interventions in health care. J. Gen. Intern. Med. 2014, 29, 1534–1541. [Google Scholar] [CrossRef]
- Grimshaw, J.; Ivers, N.; Linklater, S.; Foy, R.; Francis, J.J.; Gude, W.T.; Hysong, S.J. Reinvigorating stagnant science: Implementation laboratories and a meta-laboratory to efficiently advance the science of audit and feedback. BMJ Qual. Saf. 2019, 28, 416–423. [Google Scholar] [CrossRef]
- Foy, R.; Skrypak, M.; Alderson, S.; Ivers, N.M.; McInerney, B.; Stoddart, J.; Ingham, J.; Keenan, D. Revitalising audit and feedback to improve patient care. BMJ 2020, 368, m213. [Google Scholar] [CrossRef]
- Brehaut, J.C.; Colquhoun, H.L.; Eva, K.W.; Carroll, K.; Sales, A.; Michie, S.; Ivers, N.; Grimshaw, J.M. Practice feedback interventions: 15 suggestions for optimizing effectiveness. Ann. Intern. Med. 2016, 164, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Willis, T.A.; Hartley, S.; Glidewell, L.; Farrin, A.J.; Lawton, R.; McEachan, R.R.C.; Ingleson, E.; Heudtlass, P.; Collinson, M.; Clamp, S.; et al. Action to Support Practices Implement Research Evidence (ASPIRE): Protocol for a cluster-randomised evaluation of adaptable implementation packages targeting ‘high impact’ clinical practice recommendations in general practice. Implement. Sci. 2016, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.; Presseau, J.; Podolsky, E.; McIntyre, L.; Papoulias, M.; Brehaut, J.C. How well do critical care audit and feedback interventions adhere to best practice? Development and application of the REFLECT-52 evaluation tool. Implement. Sci. 2021, 16, 81. [Google Scholar] [CrossRef]
- Angelici, L.; Angioletti, C.; Pinnarelli, L.; Colais, P.; de Mattia, E.; Agabiti, N.; Davoli, M.; Acampora, A. EASY-NET Program: Methods and Preliminary Results of an Audit and Feedback Intervention in the Emergency Care for Acute Myocardial Infarction in the Lazio Region, Italy. Healthcare 2023, 11, 1651. [Google Scholar] [CrossRef] [PubMed]
- EASY-NET Project Web Site. Available online: https://easy-net.info/ (accessed on 15 July 2022).
- Colquhoun, H.L.; Carroll, K.; Eva, K.W.; Grimshaw, J.M.; Ivers, N.; Michie, S.; Sales, A.; Brehaut, J.C. Advancing the literature on designing audit and feedback interventions: Identifying theory-informed hypotheses. Implement. Sci. 2017, 12, 117. [Google Scholar] [CrossRef] [PubMed]
- Bourrée, F.; Michel, P.; Salmi, L. Méthodes de consensus: Revue des méthodes originales et de leurs grandes variantes utilisées en santé publique [Consensus methods: Review of original methods and their main alternatives used in public health]. Rev. Epidemiol. Sante Publique 2008, 56, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Laforgia, P.L.; Auguadro, C.; Bronzato, S.; Durante, A. The reduction of mortality in acute myocardial infarction: From bed rest to future directions. Int. J. Prev. Med. 2022, 13, 56. [Google Scholar] [PubMed]
- P.Re.Val.E. Edition 2022 Web Site. Volume of Hospitalization for AMI from 2012 to 2021. Available online: https://www.dep.lazio.it/prevale2022/risultati/tipo5/home_tipo5.php?ind=122&tipo=5&area=1 (accessed on 15 September 2022).
- Angelici, L.; Sorge, C.; Di Martino, M.; Cappai, G.; Stafoggia, M.; Agabiti, N.; Girardi, E.; Lanini, S.; Nicastri, E.; Davoli, M.; et al. Incidence of SARS-CoV-2 Infection and Related Mortality by Education Level during Three Phases of the 2020 Pandemic: A Population-Based Cohort Study in Rome. J. Clin. Med. 2022, 11, 877. [Google Scholar] [CrossRef]
- Rete Emergenza Ospedaliera—Afferenze Rete Emergenza Ospedaliera Adulti. Available online: https://www.regione.lazio.it/enti/salute/sistemi-emergenza/rete-emergenza-ospedaliera (accessed on 15 September 2023).
- Rete ICTUS. Available online: https://www.regione.lazio.it/enti/salute/sistemi-emergenza/rete-ictus- (accessed on 15 September 2023).
- Amato, L.; Fusco, D.; Acampora, A.; Bontempi, K.; Rosa, A.C.; Colais, P.; Cruciani, F.; D’Ovidio, M.; Mataloni, F.; Minozzi, S.; et al. Volume and health outcomes: Evidence from systematic reviews and from evaluation of Italian hospital data. Epidemiol. Prev. 2017, 41 (Suppl. 2), 1–128. [Google Scholar] [CrossRef]
- Programmazione Della Rete Ospedaliera 2021–2023 in Conformità Agli Standard Previsti Nel DM 70/2015. Available online: https://www.regione.lazio.it/sites/default/files/documentazione/SAL_DD_G01328_10_02_2022_Allegato_1.pdf (accessed on 28 December 2023).
- P.Re.Val.E. (Programma Regionale Valutazione Esiti”—Regional Program for Outcomes and Processes Evaluation-Strumenti per Audit) Edition 2022 Web Sites. Available online: https://www.dep.lazio.it/prevale2022/audit/audit_qualita1.php?ind=1 (accessed on 16 September 2023).
- The BC Emergency Medicine Network: Evaluation Approach and Early Findings. British Columbia Medical Journal. Available online: https://bcmj.org/articles/bc-emergency-medicine-network-evaluation-approach-and-early-findings (accessed on 27 December 2023).
- Evans, J.M.; Commisso, E.; Grudniewicz, A.; Im, J.; Veillard, J.; Richards, G. Managing the performance of healthcare networks: A ‘dance’ between control and collaboration. Public Manag. Rev. 2023. [Google Scholar] [CrossRef]
- Vola, F.; Benedetto, V.; Vainieri, M.; Nuti, S. The Italian interregional performance evaluation system. Res. Health Serv. Reg. 2022, 1, 1–14. [Google Scholar] [CrossRef]
- Il Sistema di Monitoraggio. Available online: https://www.salute.gov.it/portale/lea/dettaglioContenutiLea.jsp?lingua=italiano&id=4744&area=Lea&menu=monitoraggioLea (accessed on 28 December 2023).



{kind=link}
{kind=link}
| Thirty-Day Mortality after First Hospital Admission in Patients with AMI | χ2 p-Value | |||||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| N | Row % | N | Row % | N | ||
| Total | 839 | 11,357 | 12,196 | |||
| A&F intervention | 0.011 | |||||
| Exposed Groups | 517 | 7.4 | 6485 | 92.6 | 7002 | |
| Control Groups | 322 | 6.2 | 4872 | 93.8 | 5194 | |
| Year | 0.842 | |||||
| 2021 | 409 | 6.8 | 5577 | 93.2 | 5986 | |
| 2022 | 430 | 6.9 | 5780 | 93.1 | 6210 | |
| Sex | <0.0001 | |||||
| Female | 354 | 9.8 | 3251 | 90.2 | 3605 | |
| Male | 485 | 5.6 | 8106 | 94.4 | 8591 | |
| Age (years) | <0.0001 | |||||
| 19–59 | 60 | 1.9 | 3033 | 98.1 | 3093 | |
| 60–69 | 92 | 3.0 | 2976 | 97.0 | 3068 | |
| 70–79 | 220 | 7.3 | 2795 | 92.7 | 3015 | |
| 80–100 | 467 | 15.5 | 2553 | 84.5 | 3020 | |
| Education level | <0.0001 | |||||
| Degree | 69 | 5.5 | 1175 | 94.5 | 1244 | |
| Lower-middle high school | 215 | 5.4 | 3731 | 94.6 | 3946 | |
| Middle high school | 176 | 5.1 | 3292 | 94.9 | 3468 | |
| None or elementary school | 340 | 11.2 | 2692 | 88.8 | 3032 | |
| Not stated | 39 | 7.7 | 467 | 92.3 | 506 | |
| Concomitant clinical conditions | ||||||
| Cancer | 97 | 14.4 | 577 | 85.6 | 674 | <0.0001 |
| Diabetes | 89 | 12.3 | 633 | 87.7 | 722 | <0.0001 |
| Lipid metabolism disorders | 25 | 7.1 | 329 | 92.9 | 354 | 0.890 |
| Obesity | 5 | 7.6 | 61 | 92.4 | 66 | 0.823 |
| Obesity at indexed admission | 13 | 2.4 | 525 | 97.6 | 538 | <0.0001 |
| Anemia | 62 | 19.0 | 264 | 81.0 | 326 | <0.0001 |
| Anemia at indexed admission | 54 | 9.7 | 504 | 90.3 | 558 | 0.008 |
| Coagulation defects | 1 | 16.7 | 5 | 83.3 | 6 | 0.343 |
| Coagulation defects at indexed admission | _ | _ | 3 | 100.0 | 3 | 0.638 |
| Other hematological diseases | 2 | 6.5 | 29 | 93.5 | 31 | 0.925 |
| Other hematological diseases at indexed admission | 4 | 8.7 | 42 | 91.3 | 46 | 0.626 |
| Arterial hypertension | 112 | 9.1 | 1125 | 90.9 | 1237 | 0.001 |
| Previous myocardial infarction | 54 | 5.7 | 895 | 94.3 | 949 | 0.132 |
| Other forms of ischemic heart disease | 90 | 9.0 | 905 | 91.0 | 995 | 0.005 |
| Heart failure | 90 | 16.6 | 452 | 83.4 | 542 | <0.0001 |
| Not well-defined forms and complications of heart disease | 6 | 8.0 | 69 | 92.0 | 75 | 0.701 |
| Rheumatic heart disease | 6 | 14.0 | 37 | 86.0 | 43 | 0.066 |
| Rheumatic heart disease at indexed admission | 27 | 16.9 | 133 | 83.1 | 160 | <0.0001 |
| Cardiomyopathies | 8 | 14.5 | 47 | 85.5 | 55 | 0.024 |
| Cardiomyopathies at indexed admission | 8 | 5.8 | 131 | 94.2 | 139 | 0.599 |
| Acute endocarditis and myocarditis | _ | _ | 6 | 100.0 | 6 | 0.506 |
| Other cardiac conditions | 14 | 13.3 | 91 | 86.7 | 105 | 0.009 |
| Other cardiac conditions at indexed admission | 35 | 10.8 | 289 | 89.2 | 324 | 0.005 |
| Conduction disorders and arrhythmias | 75 | 13.1 | 499 | 86.9 | 574 | <0.0001 |
| Cerebrovascular diseases | 47 | 11.4 | 366 | 88.6 | 413 | 0.000 |
| Cerebrovascular diseases at indexed admission | 34 | 10.2 | 300 | 89.8 | 334 | 0.016 |
| Vascular diseases | 40 | 13.3 | 260 | 86.7 | 300 | <0.0001 |
| Vascular diseases at indexed admission | 24 | 6.5 | 348 | 93.5 | 372 | 0.741 |
| Chronic obstructive pulmonary disease (COPD) | 38 | 13.2 | 249 | 86.8 | 287 | <0.0001 |
| Chronic nephropathy | 68 | 15.7 | 364 | 84.3 | 432 | <0.0001 |
| Chronic kidney disease | 116 | 10.9 | 945 | 89.1 | 1061 | <0.0001 |
| Chronic diseases (liver, pancreas, intestines) | 9 | 13.2 | 59 | 86.8 | 68 | 0.038 |
| Chronic diseases (liver, pancreas, intestines) at indexed admission | 7 | 10.0 | 63 | 90.0 | 70 | 0.301 |
| Previous coronary artery bypass grafting | 31 | 9.7 | 287 | 90.3 | 318 | 0.041 |
| Previous coronary angioplasty | 65 | 5.3 | 1168 | 94.7 | 1233 | 0.019 |
| Cerebrovascular revascularization | 6 | 7.9 | 70 | 92.1 | 76 | 0.726 |
| Other heart surgery | 13 | 17.6 | 61 | 82.4 | 74 | 0.000 |
| Other vessel surgery | 30 | 11.4 | 233 | 88.6 | 263 | 0.003 |
| Type of hospital * | 0.120 | |||||
| EADI | 554 | 6.8 | 7575 | 93.2 | 8129 | |
| EADII | 262 | 7.3 | 3327 | 92.7 | 3589 | |
| ER | 23 | 4.8 | 455 | 95.2 | 478 | |
| % PTCA STEMI Patients within 90 min of Admission to the ER | χ2 p-Value | |||||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| N | Row % | N | Row % | N | ||
| Total | 3077 | 2007 | 5084 | |||
| A&F intervention | 0.069 | |||||
| Exposed Groups | 1950 | 59.6 | 1322 | 40.4 | 3272 | |
| Control Groups | 1127 | 62.2 | 685 | 37.8 | 1812 | |
| Year | 0.003 | |||||
| 2021 | 1420 | 58.4 | 1013 | 41.6 | 2433 | |
| 2022 | 1657 | 62.5 | 994 | 37.5 | 2651 | |
| Sex | <0.0001 | |||||
| Female | 701 | 54.5 | 586 | 45.5 | 1287 | |
| Male | 2376 | 62.6 | 1421 | 37.4 | 3797 | |
| Age (years) | <0.0001 | |||||
| 21–57 | 879 | 67.3 | 428 | 32.7 | 1307 | |
| 58–65 | 808 | 66.5 | 407 | 33.5 | 1215 | |
| 66–75 | 781 | 60.1 | 519 | 39.9 | 1300 | |
| 76–100 | 609 | 48.3 | 653 | 51.7 | 1262 | |
| Education level | <0.0001 | |||||
| Degree | 339 | 58.8 | 238 | 41.2 | 577 | |
| Lower-middle high school | 1031 | 62.2 | 626 | 37.8 | 1657 | |
| Middle high school | 988 | 63.0 | 581 | 37.0 | 1569 | |
| None or elementary school | 548 | 54.0 | 467 | 46.0 | 1015 | |
| Not stated | 171 | 64.3 | 95 | 35.7 | 266 | |
| Concomitant clinical conditions | ||||||
| Cancer | 109 | 44.9 | 134 | 55.1 | 243 | <0.0001 |
| Diabetes | 67 | 41.6 | 94 | 58.4 | 161 | <0.0001 |
| Lipid metabolism disorders | 36 | 45.0 | 44 | 55.0 | 80 | 0.004 |
| Obesity | 7 | 43.8 | 9 | 56.3 | 16 | 0.169 |
| Obesity at indexed admission | 126 | 56.8 | 96 | 43.2 | 222 | 0.240 |
| Anemia | 16 | 26.7 | 44 | 73.3 | 60 | <0.0001 |
| Anemia at indexed admission | 60 | 37.7 | 99 | 62.3 | 159 | <0.0001 |
| Coagulation defects | 1 | 100.0 | _ | _ | 1 | 0.419 |
| Coagulation defects at indexed admission | 1 | 100.0 | _ | _ | 1 | 0.419 |
| Other hematological diseases | 5 | 33.3 | 10 | 66.7 | 15 | 0.031 |
| Other hematological diseases at indexed admission | 11 | 64.7 | 6 | 35.3 | 17 | 0.724 |
| Arterial hypertension | 166 | 51.1 | 159 | 48.9 | 325 | 0.000 |
| Previous myocardial infarction | 81 | 38.4 | 130 | 61.6 | 211 | <0.0001 |
| Other forms of ischemic heart disease | 96 | 44.2 | 121 | 55.8 | 217 | <0.0001 |
| Heart failure | 27 | 32.5 | 56 | 67.5 | 83 | <0.0001 |
| Not well-defined forms and complications of heart disease | 4 | 30.8 | 9 | 69.2 | 13 | 0.028 |
| Rheumatic heart disease | 4 | 50.0 | 4 | 50.0 | 8 | 0.542 |
| Rheumatic heart disease at indexed admission | 18 | 41.9 | 25 | 58.1 | 43 | 0.012 |
| Cardiomyopathies | 3 | 18.8 | 13 | 81.3 | 16 | 0.001 |
| Cardiomyopathies at indexed admission | 23 | 39.7 | 35 | 60.3 | 58 | 0.001 |
| Acute endocarditis and myocarditis | _ | _ | 1 | 100.0 | 1 | 0.216 |
| Other cardiac conditions | 2 | 15.4 | 11 | 84.6 | 13 | 0.001 |
| Other cardiac conditions at indexed admission | 21 | 31.8 | 45 | 68.2 | 66 | <0.0001 |
| Conduction disorders and arrhythmias | 45 | 36.9 | 77 | 63.1 | 122 | <0.0001 |
| Cerebrovascular diseases | 54 | 45.0 | 66 | 55.0 | 120 | 0.000 |
| Cerebrovascular diseases at indexed admission | 42 | 34.4 | 80 | 65.6 | 122 | <0.0001 |
| Vascular diseases | 28 | 35.0 | 52 | 65.0 | 80 | <0.0001 |
| Vascular diseases at indexed admission | 42 | 39.6 | 64 | 60.4 | 106 | <0.0001 |
| Chronic obstructive pulmonary disease (COPD) | 23 | 38.3 | 37 | 61.7 | 60 | 0.000 |
| Chronic nephropathy | 37 | 38.1 | 60 | 61.9 | 97 | <0.0001 |
| Chronic kidney disease | 131 | 44.3 | 165 | 55.7 | 296 | <0.0001 |
| Chronic diseases (liver, pancreas, intestines) | 9 | 47.4 | 10 | 52.6 | 19 | 0.240 |
| Chronic diseases (liver, pancreas, intestines) at indexed admission | 13 | 48.1 | 14 | 51.9 | 27 | 0.187 |
| Previous coronary artery bypass grafting | 19 | 41.3 | 27 | 58.7 | 46 | 0.007 |
| Previous coronary angioplasty | 159 | 50.6 | 155 | 49.4 | 314 | 0.000 |
| Cerebrovascular revascularization | 10 | 62.5 | 6 | 37.5 | 16 | 0.871 |
| Other heart surgery | 6 | 28.6 | 15 | 71.4 | 21 | 0.003 |
| Other vessel surgery | 25 | 37.9 | 41 | 62.1 | 66 | 0.000 |
| Type of hospital * | 0.142 | |||||
| EADI | 1909 | 61.3 | 1204 | 38.7 | 3113 | |
| EADII | 1168 | 59.3 | 803 | 40.7 | 1971 | |
| Thirty-Day In-Hospital Mortality after Admission in Patients with Ischemic Stroke | χ2 p-Value | |||||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| N | Row % | N | Row % | N | ||
| Total | 432 | 5517 | 5949 | |||
| A&F intervention | 0.006 | |||||
| Exposed Groups | 249 | 8.2 | 2803 | 91.8 | 3052 | |
| Control Groups | 183 | 6.3 | 2714 | 93.7 | 2897 | |
| Year | 0.081 | |||||
| 2021 | 232 | 7.9 | 2722 | 92.1 | 2954 | |
| 2022 | 200 | 6.7 | 2795 | 93.3 | 2995 | |
| Sex | <0.0001 | |||||
| Female | 243 | 8.8 | 2512 | 91.2 | 2755 | |
| Male | 189 | 5.9 | 3005 | 94.1 | 3194 | |
| Age (years) | <0.0001 | |||||
| 35–66 | 26 | 1.7 | 1482 | 98.3 | 1508 | |
| 67–76 | 71 | 4.8 | 1401 | 95.2 | 1472 | |
| 77–83 | 111 | 7.8 | 1318 | 92.2 | 1429 | |
| 84–100 | 224 | 14.5 | 1316 | 85.5 | 1540 | |
| Education level | <0.0001 | |||||
| Degree | 24 | 4.2 | 543 | 95.8 | 567 | |
| Lower-middle high school | 107 | 6.7 | 1492 | 93.3 | 1599 | |
| Middle high school | 76 | 5.5 | 1304 | 94.5 | 1380 | |
| None or elementary | 211 | 10.0 | 1901 | 90.0 | 2112 | |
| Not stated | 14 | 4.8 | 277 | 95.2 | 291 | |
| Concomitant clinical conditions | ||||||
| Cancer | 21 | 9.9 | 192 | 90.1 | 213 | 0.137 |
| Diabetes | 34 | 11.8 | 254 | 88.2 | 288 | 0.002 |
| Lipid metabolism disorders | 7 | 6.4 | 103 | 93.6 | 110 | 0.714 |
| Obesity | 4 | 11.1 | 32 | 88.9 | 36 | 0.372 |
| Obesity at indexed admission | 9 | 6.5 | 130 | 93.5 | 139 | 0.718 |
| Anemia | 23 | 13.5 | 147 | 86.5 | 170 | 0.001 |
| Anemia at indexed admission | 11 | 6.1 | 169 | 93.9 | 180 | 0.546 |
| Coagulation defects | _ | _ | 3 | 100.0 | 3 | 0.628 |
| Coagulation defects at indexed admission | 1 | 8.3 | 11 | 91.7 | 12 | 0.886 |
| Other hematological diseases | 1 | 6.7 | 14 | 93.3 | 15 | 0.929 |
| Other hematological diseases at indexed admission | 4 | 9.3 | 39 | 90.7 | 43 | 0.605 |
| Arterial hypertension | 71 | 12.0 | 520 | 88.0 | 591 | <0.0001 |
| Previous myocardial infarction | 14 | 11.1 | 112 | 88.9 | 126 | 0.092 |
| Other forms of ischemic heart disease | 27 | 10.7 | 226 | 89.3 | 253 | 0.033 |
| Heart failure | 50 | 17.4 | 237 | 82.6 | 287 | <0.0001 |
| Not well-defined forms and complications of heart disease | 4 | 9.8 | 37 | 90.2 | 41 | 0.537 |
| Rheumatic heart disease | 8 | 17.8 | 37 | 82.2 | 45 | 0.006 |
| Rheumatic heart disease at indexed admission | 2 | 3.3 | 58 | 96.7 | 60 | 0.239 |
| Cardiomyopathies | 3 | 10.0 | 27 | 90.0 | 30 | 0.562 |
| Cardiomyopathies at indexed admission | 3 | 8.3 | 33 | 91.7 | 36 | 0.804 |
| Acute endocarditis and myocarditis | _ | _ | 3 | 100.0 | 3 | 0.628 |
| Other cardiac conditions | 12 | 14.6 | 70 | 85.4 | 82 | 0.010 |
| Other cardiac conditions at indexed admission | 8 | 3.5 | 220 | 96.5 | 228 | 0.026 |
| Conduction disorders and arrhythmias | 55 | 14.6 | 321 | 85.4 | 376 | <0.0001 |
| Cerebrovascular diseases | 40 | 9.6 | 378 | 90.4 | 418 | 0.059 |
| Vascular diseases | 11 | 8.0 | 126 | 92.0 | 137 | 0.726 |
| Vascular diseases at indexed admission | 15 | 6.0 | 233 | 94.0 | 248 | 0.452 |
| Chronic obstructive pulmonary disease (COPD) | 21 | 16.9 | 103 | 83.1 | 124 | <0.0001 |
| Chronic nephropathy | 26 | 16.4 | 133 | 83.6 | 159 | <0.0001 |
| Chronic nephropathy at indexed admission | 29 | 13.2 | 191 | 86.8 | 220 | 0.001 |
| Chronic kidney disease | 3 | 8.6 | 32 | 91.4 | 35 | 0.765 |
| Diseases chronic diseases (liver, pancreas, intestines) | 2 | 4.8 | 40 | 95.2 | 42 | 0.531 |
| Diseases chronic diseases (liver, pancreas, intestines) at indexed admission | 9 | 6.3 | 135 | 93.8 | 144 | 0.636 |
| Cerebrovascular revascularization | _ | _ | 27 | 100.0 | 27 | 0.145 |
| Other heart surgery | 13 | 19.4 | 54 | 80.6 | 67 | <0.0001 |
| Other vessel surgery | 11 | 8.5 | 119 | 91.5 | 130 | 0.594 |
| Type of hospital * | 0.207 | |||||
| noNVT | 15 | 12.0 | 110 | 88.0 | 125 | |
| NVT | 11 | 6.3 | 164 | 93.7 | 175 | |
| NTUI | 209 | 7.1 | 2742 | 92.9 | 2951 | |
| NTUII | 197 | 7.3 | 2501 | 92.7 | 2698 | |
| % of Hospital Readmissions within 30 days of Discharge for Ischemic Stroke | χ2 p-Value | |||||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| N | Row % | N | Row % | N | ||
| Total | 392 | 5061 | 5453 | |||
| A&F intervention | 0.910 | |||||
| Exposed Groups | 201 | 7.8 | 2580 | 92.8 | 2781 | |
| Control Groups | 191 | 7.7 | 2481 | 92.9 | 2672 | |
| Year | 0.248 | |||||
| 2021 | 182 | 7.3 | 2503 | 93.2 | 2685 | |
| 2022 | 210 | 8.2 | 2558 | 92.4 | 2768 | |
| Sex | 0.062 | |||||
| Female | 159 | 6.9 | 2321 | 93.6 | 2480 | |
| Male | 233 | 8.5 | 2740 | 92.2 | 2973 | |
| Age (years) | 0.005 | |||||
| 35–66 | 71 | 5.5 | 1296 | 94.8 | 1367 | |
| 67–76 | 101 | 8.1 | 1240 | 92.5 | 1341 | |
| 77–83 | 125 | 9.4 | 1323 | 91.4 | 1448 | |
| 84–100 | 95 | 7.9 | 1202 | 92.7 | 1297 | |
| Education level | 0.432 | |||||
| Degree | 41 | 8.2 | 498 | 92.4 | 539 | |
| Lower-middle high school | 96 | 6.9 | 1384 | 93.5 | 1480 | |
| Middle high school | 90 | 7.5 | 1202 | 93.0 | 1292 | |
| None or elementary school | 149 | 8.7 | 1719 | 92.0 | 1868 | |
| Not stated | 16 | 6.2 | 258 | 94.2 | 274 | |
| Concomitant clinical conditions | ||||||
| Cancer | 16 | 9.1 | 175 | 91.6 | 191 | 0.518 |
| Diabetes | 18 | 7.8 | 232 | 92.8 | 250 | 0.994 |
| Lipid metabolism disorders | 7 | 7.5 | 93 | 93.0 | 100 | 0.941 |
| Obesity | 4 | 14.3 | 28 | 87.5 | 32 | 0.243 |
| Obesity at indexed admission | 4 | 3.2 | 125 | 96.9 | 129 | 0.069 |
| Anemia | 12 | 9.0 | 133 | 91.7 | 145 | 0.608 |
| Anemia at indexed admission | 12 | 8.1 | 149 | 92.5 | 161 | 0.895 |
| Coagulation defects | 1 | 50.0 | 2 | 66.7 | 3 | 0.080 |
| Coagulation defects at indexed admission | 1 | 11.1 | 9 | 90.0 | 10 | 0.731 |
| Other hematological diseases | 1 | 7.7 | 13 | 92.9 | 14 | 0.995 |
| Other hematological diseases at indexed admission | 2 | 5.6 | 36 | 94.7 | 38 | 0.645 |
| Arterial hypertension | 35 | 7.3 | 481 | 93.2 | 516 | 0.708 |
| Previous myocardial infarction | 7 | 6.7 | 104 | 93.7 | 111 | 0.716 |
| Other forms of ischemic heart disease | 17 | 8.3 | 205 | 92.3 | 222 | 0.782 |
| Heart failure | 27 | 13.0 | 207 | 88.5 | 234 | 0.009 |
| Not well-defined forms and complications of heart disease | 4 | 12.1 | 33 | 89.2 | 37 | 0.392 |
| Rheumatic heart disease | 5 | 16.1 | 31 | 86.1 | 36 | 0.118 |
| Rheumatic heart disease at indexed admission | 10 | 21.3 | 47 | 82.5 | 57 | 0.002 |
| Cardiomyopathies | 1 | 3.8 | 26 | 96.3 | 27 | 0.482 |
| Cardiomyopathies at indexed admission | 3 | 10.0 | 30 | 90.9 | 33 | 0.671 |
| Acute endocarditis and myocarditis | _ | _ | 3 | 100.0 | 3 | 0.630 |
| Other cardiac conditions | 8 | 13.3 | 60 | 88.2 | 68 | 0.142 |
| Other cardiac conditions at indexed admission | 16 | 7.9 | 203 | 92.7 | 219 | 0.945 |
| Conduction disorders and arrhythmias | 30 | 10.5 | 286 | 90.5 | 316 | 0.102 |
| Cerebrovascular diseases | 32 | 9.4 | 340 | 91.4 | 372 | 0.274 |
| Vascular diseases | 11 | 9.6 | 114 | 91.2 | 125 | 0.481 |
| Vascular diseases at indexed admission | 11 | 5.0 | 221 | 95.3 | 232 | 0.140 |
| Chronic obstructive pulmonary disease (COPD) | 10 | 10.8 | 93 | 90.3 | 103 | 0.318 |
| Chronic nephropathy | 18 | 15.9 | 113 | 86.3 | 131 | 0.003 |
| Chronic nephropathy at indexed admission | 23 | 13.9 | 166 | 87.8 | 189 | 0.007 |
| Chronic kidney disease | 6 | 23.1 | 26 | 81.3 | 32 | 0.011 |
| Diseases chronic diseases (liver, pancreas, intestines) | 3 | 8.3 | 36 | 92.3 | 39 | 0.903 |
| Diseases chronic diseases (liver, pancreas, intestines) at indexed admission | 9 | 7.3 | 123 | 93.2 | 132 | 0.868 |
| Cerebrovascular revascularization | _ | _ | 27 | 100.0 | 27 | 0.147 |
| Other heart surgery | 7 | 15.2 | 46 | 86.8 | 53 | 0.088 |
| Other vessel surgery | 11 | 10.5 | 105 | 90.5 | 116 | 0.334 |
| Type of hospital * | 0.551 | |||||
| noNVT | 8 | 7.8 | 102 | 92.7 | 110 | |
| NVT | 16 | 11.0 | 146 | 90.1 | 162 | |
| NTUI | 197 | 7.9 | 2506 | 92.7 | 2703 | |
| NTUII | 171 | 7.4 | 2307 | 93.1 | 2478 | |
| AMI/STEMI Pathway | ||||||
|---|---|---|---|---|---|---|
| Indicators | Facilities (Patients) | 30-Day Mortality after First Hospital Admission in Patients with AMI | Facilities (Patients) | % PTCA-STEMI Patients within 90 min of Admission to the ER | ||
| Unadjusted | Adjusted * | Unadjusted | Adjusted ** | |||
| Exposed Group | ||||||
| “Pre-”—2021 (%) | 12 (3393) | 7.40 | 10.51 | 12 (1541) | 58.66 | 58.12 |
| “Post-”—2022 (%) | 15 (3609) | 7.37 | 10.29 | 12 (1731) | 60.43 | 59.43 |
| Difference Post-/Pre- (PP) | −0.03 | −0.22 | 1.77 | 1.31 | ||
| Control Group | ||||||
| “Pre-”—2021 (%) | 15 (2593) | 6.09 | 9.48 | 8 (892) | 57.85 | 56.79 |
| “Post”—2022 (%) | 16 (2601) | 6.31 | 9.34 | 8 (920) | 66.41 | 65.42 |
| Difference Post-/Pre- (PP) | 0.22 | −0.14 | 8.56 | 8.63 | ||
| DID PP | −0.24 | −0.08 | −6.80 | −7.29 | ||
| (95% CI) | (−2.03; 1.56) | (−2.80; 2.65) | (−12.38; −1.22) | (−12.75; −1.83) | ||
| p-value for interaction | 0.794 | 0.956 | 0.017 | 0.009 | ||
| Ischemic Stroke Pathway | ||||||
|---|---|---|---|---|---|---|
| Indicators | Facilities (Patients) | Thirty-Day In-Hospital Mortality after Admission in Patients with Ischemic Stroke | Facilities (Patients) | % of Hospital Readmissions within 30 days of Discharge for Ischemic Stroke | ||
| Unadjusted | Adjusted * | Unadjusted | Adjusted ** | |||
| Exposed Group | ||||||
| “Pre-”—2021 (%) | 8 (1885) | 8.54 | 7.89 | 8 (1711) | 7.36 | 7.33 |
| “Post-”—2022 (%) | 8 (1908) | 6.87 | 7.15 | 8 (1760) | 6.88 | 6.79 |
| Difference Post-/Pre- (PP) | −1.67 | −0.74 | −0.48 | −0.54 | ||
| Control Group | ||||||
| “Pre-”—2021 (%) | 8 (1069) | 6.64 | 6.65 | 8 (974) | 5.75 | 5.51 |
| “Post-”—2022 (%) | 9 (1087) | 6.35 | 6.91 | 9 (1008) | 8.83 | 8.76 |
| Difference Post-/Pre- (PP) | −0.29 | 0.26 | 3.08 | 3.25 | ||
| DID PP | −1.38 | −0.99 | −3.57 | −3.80 | ||
| (95% CI) | (−4.07; 1.30) | (−2.93; 0.95) | (−6.42; −0.72) | (−6.57; −1.03) | ||
| p-value for interaction | 0.313 | 0.315 | 0.014 | 0.007 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelici, L.; Angioletti, C.; Pinnarelli, L.; Colais, P.; de Belvis, A.G.; Melnyk, A.; La Gatta, E.; Farchi, S.; Davoli, M.; Agabiti, N.; et al. EASY-NET Program: Effectiveness of an Audit and Feedback Intervention in the Emergency Care for Acute Conditions in the Lazio Region. Healthcare 2024, 12, 733. https://doi.org/10.3390/healthcare12070733
Angelici L, Angioletti C, Pinnarelli L, Colais P, de Belvis AG, Melnyk A, La Gatta E, Farchi S, Davoli M, Agabiti N, et al. EASY-NET Program: Effectiveness of an Audit and Feedback Intervention in the Emergency Care for Acute Conditions in the Lazio Region. Healthcare. 2024; 12(7):733. https://doi.org/10.3390/healthcare12070733
Chicago/Turabian StyleAngelici, Laura, Carmen Angioletti, Luigi Pinnarelli, Paola Colais, Antonio Giulio de Belvis, Andriy Melnyk, Emanuele La Gatta, Sara Farchi, Marina Davoli, Nera Agabiti, and et al. 2024. "EASY-NET Program: Effectiveness of an Audit and Feedback Intervention in the Emergency Care for Acute Conditions in the Lazio Region" Healthcare 12, no. 7: 733. https://doi.org/10.3390/healthcare12070733
APA StyleAngelici, L., Angioletti, C., Pinnarelli, L., Colais, P., de Belvis, A. G., Melnyk, A., La Gatta, E., Farchi, S., Davoli, M., Agabiti, N., & Acampora, A. (2024). EASY-NET Program: Effectiveness of an Audit and Feedback Intervention in the Emergency Care for Acute Conditions in the Lazio Region. Healthcare, 12(7), 733. https://doi.org/10.3390/healthcare12070733