
Firefighter Health: A Narrative Review of Occupational Threats and Countermeasures

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
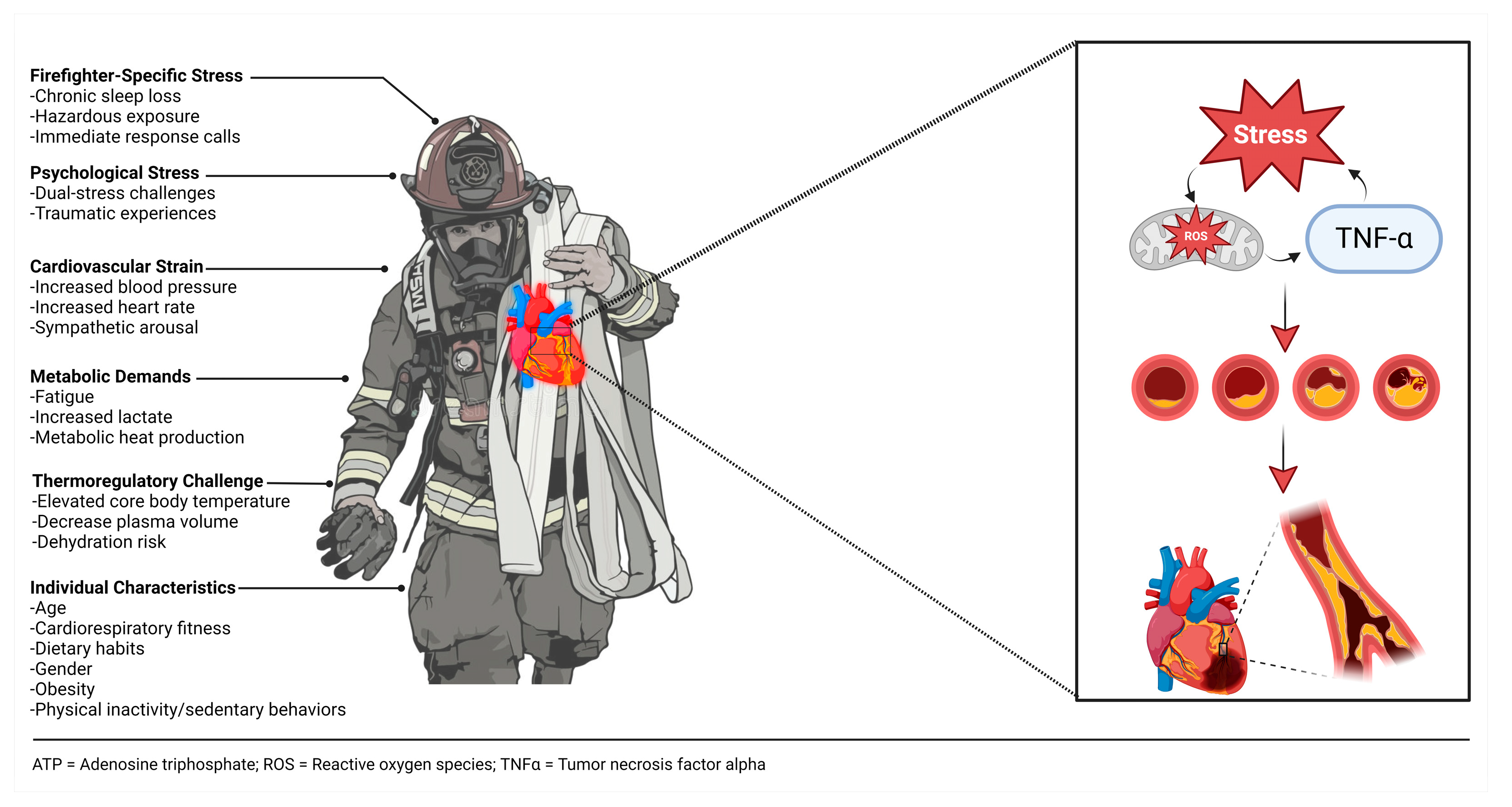
3.1. Physical Health Threat: Cardiovascular Disease
3.2. Physical Health Countermeasure: Clinical and Fitness Assessments
3.3. Physical Health Countermeasure: Exercise
3.4. Physical Health Countermeasure—Dietary Intake
3.5. Physical Health Countermeasure—Sleep
3.6. Physical Health Threat: Cancer
3.7. Physical Health Countermeasure: Cancer
3.8. Mental Health Threat: Traumatic Events
“Many firefighters spoke about the impact on their families. […] Reasons given were that they were concerned that their family member might change the way they viewed them as a person because of the kinds of things they were seeing at work. Concurrently, they also wanted their family members to have faith that their role as a firefighter was valuable and that their job was good and important, and they were worried that sharing some of their experiences might undermine their families’ valuation of the job. […] Firefighters acknowledged that the issues that impact their confidence in self and feelings of failure from bad outcomes at work carried over into their feelings within the family. Firefighters also acknowledged awareness and regret that mental health stressors from work carried over into their family life in terms of how they treated family members with less tolerance, irritability, or poor communication. […] They were concerned that taking time off work often compromised their family’s financial stability since sick benefits do not replace usual firefighter income. Many acknowledged the increased risk of divorce in the fire service or had personally experienced divorce and attributed work issues as a contributing factor” (p. 8, 2021) [155].
3.9. Mental Health Countermeasure: Mindfulness
3.10. Mental Health Countermeasure: Post-Trauma Debriefing
4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sterling, P.; Eyer, J. Handbook of Life Stress, Cognition and Health; Fisher, S., Reason, J., Eds.; J. Wiley Ltd.: Hoboken, NJ, USA, 1988; p. 631. [Google Scholar]
- McEwen, B.S.; Stellar, E. Stress and the individual. Mechanisms leading to disease. Arch. Intern. Med. 1993, 153, 2093–2101. [Google Scholar] [CrossRef] [PubMed]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocr. Rev. 2000, 21, 55–89. [Google Scholar] [CrossRef] [PubMed]
- Stults-Kolehmainen, M.A.; Bartholomew, J.B.; Sinha, R. Chronic psychological stress impairs recovery of muscular function and somatic sensations over a 96-hour period. J. Strength Cond. Res. 2014, 28, 2007–2017. [Google Scholar] [CrossRef] [PubMed]
- Lesniak, A.; Sell, K.; Morris, C.; Abel, M.G. Relationship between heart rate variability vs. occupational performance, physical activity, and fitness measures in structural firefighters. J. Sport Hum. Perform. 2022, 10, 56–72. [Google Scholar]
- Kales, S.N.; Smith, D.L. Firefighting and the heart: Implications for prevention. Circulation 2017, 135, 1296–1299. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Barr, D.A.; Kales, S.N. Extreme sacrifice: Sudden cardiac death in the US Fire Service. Extrem. Physiol. Med. 2013, 2, 6. [Google Scholar] [CrossRef]
- Soteriades, E.S.; Smith, D.L.; Tsismenakis, A.J.; Baur, D.M.; Kales, S.N. Cardiovascular disease in US firefighters: A systematic review. Cardiol. Rev. 2011, 19, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Fahy, R.F. US Firefighter Fatalities Due to Sudden Cardiac Death, 1995–2004; National Fire Protection Association: Quincy, MA, USA, 2005; pp. 1–9. [Google Scholar]
- Fahy, R.F.; LeBlanc, P.R.; Molis, J.L. Firefighter Fatalities in the United States—2005; National Fire Protection Association, Fire Analysis and Research Division: Quincy, MA, USA, 2006. [Google Scholar]
- Fahy, R.F.; LeBlanc, P.R.; Molis, J.L. Firefighter Fatalities in the United States–2011; National Fire Protection Association: Emmitsburg, MD, USA, 2012; Volume 1, pp. 1–36. [Google Scholar]
- Fahy, R.F.; LeBlanc, P.R.; Molis, J.L. Firefighter Fatalities in the United States: 2016; National Fire Protection Association, Fire Analysis and Research Division: Quincy, MA, USA, 2017. [Google Scholar]
- Fahy, R.F.; Petrillo, J.T.; Molis, J.L. Firefighter Fatalities in the US—2019; National Fire Protection Association: Quincy, MA, USA, 2020; pp. 1–26. [Google Scholar]
- Fahy, R.F.; Petrillo, J.T. Firefighter Fatalities in the US in 2021; National Fire Protection Association: Quincy, MA, USA, 2022. [Google Scholar]
- Kales, S.N.; Soteriades, E.S.; Christophi, C.A.; Christiani, D.C. Emergency duties and deaths from heart disease among firefighters in the United States. N. Engl. J. Med. 2007, 356, 1207–1215. [Google Scholar] [CrossRef]
- Hunter, A.L.; Shah, A.S.; Langrish, J.P.; Raftis, J.B.; Lucking, A.J.; Brittan, M.; Venkatasubramanian, S.; Stables, C.L.; Stelzle, D.; Marshall, J.; et al. Fire simulation and cardiovascular health in firefighters. Circulation 2017, 135, 1284–1295. [Google Scholar] [CrossRef]
- Wilson, T.E.; Crandall, C.G. Effect of thermal stress on cardiac function. Exerc. Sport Sci. Rev. 2011, 39, 12–17. [Google Scholar] [CrossRef]
- Santos, V.; Massuça, L.M.; Monteiro, L.; Angarten, V.; Abel, M.G.; Fernhall, B.; Santa-Clara, H. Comparison of acute arterial responses following a rescue simulation and maximal exercise in professional firefighters. Healthcare 2023, 11, 1032. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L. Firefighter fitness: Improving performance and preventing injuries and fatalities. Curr. Sports Med. Rep. 2011, 10, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Crandall, C.G.; Wilson, T.E. Human cardiovascular responses to passive heat stress. Compr. Physiol. 2015, 5, 17–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Manning, T.S.; Petruzzello, S.J. Effect of strenuous live-fire drills on cardiovascular and psychological responses of recruit firefighters. Ergonomics 2001, 44, 244–254. [Google Scholar] [CrossRef]
- Smith, D.L.; Petruzzello, S.J.; Chludzinski, M.A.; Chludzinski, M.A.; Reed, J.J.; Woods, J.A. Effects of strenuous live-fire drills on hematological, blood chemistry, and psychological measures. J. Therm. Biol. 2001, 26, 375–379. [Google Scholar] [CrossRef]
- Walker, A.; Keene, T.; Argus, C.; Driller, M.; Guy, J.H.; Rattray, B. Immune and inflammatory responses of Australian firefighters after repeated exposures to the heat. Ergonomics 2015, 58, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Wolkow, A.; Aisbett, B.; Jefferies, S.; Main, L.C. Effect of heat exposure and simulated physical firefighting work on acute inflammatory and cortisol responses. Ann. Work Expo. Health 2017, 61, 600–603. [Google Scholar] [CrossRef]
- Barbu, E.; Popescu, M.R.; Popescu, A.C.; Balanescu, S.M. Inflammation as a precursor of atherothrombosis, diabetes and early vascular aging. Int. J. Mol. Sci. 2022, 23, 963. [Google Scholar] [CrossRef]
- Gonzalez, D.E.; Waldman, H.S.; McAllister, M.J. The metabolic and physiological demands of a simulated fire ground test versus a live-fire training evolution in professional firefighters. Int. J. Exerc. Sci. 2023, 16, 230–241. [Google Scholar]
- Gonzalez, D.E.; Johnson, S.E.; Dillard, C.C.; Sowinski, R.J.; Martin, S.E.; Colvin, L.C.; McAllister, M.J. Physiological stress responses to a live-fire training evolution in career firefighters. Int. J. Exerc. Sci. Conf. Proc. 2023, 2, 9. [Google Scholar] [CrossRef]
- McAllister, M.J.; Gonzalez, A.E.; Waldman, H.S. Time restricted feeding reduces inflammation and cortisol response to a firegrounds test in professional firefighters. J. Occup. Environ. Med. 2021, 63, 441–447. [Google Scholar] [CrossRef]
- Richardson, A.; Terrazzini, N.; Gage, C.; Lee, B.J.; Bradley, R.; Watt, P.; Watkins, E.R. Inflammatory and psychological consequences of chronic high exposure firefighting. J. Therm. Biol. 2023, 111, 103399. [Google Scholar] [CrossRef]
- Huang, C.J.; Webb, H.E.; Zourdos, M.C.; Acevedo, E.O. Cardiovascular reactivity, stress, and physical activity. Front. Physiol. 2013, 4, 314. [Google Scholar] [CrossRef]
- Kales, S.N.; Soteriades, E.S.; Christoudias, S.G.; Christiani, D.C. Firefighters and on-duty deaths from coronary heart disease: A case control study. Environ. Health 2003, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Poston, W.S.C.; Haddock, C.K.; Jahnke, S.A.; Jitnarin, N.; Tuley, B.C.; Kales, S.N. The prevalence of overweight, obesity, and substandard fitness in a population-based firefighter cohort. J. Occup. Environ. Med. 2011, 53, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Tsismenakis, A.J.; Christophi, C.A.; Burress, J.W.; Kinney, A.M.; Kim, M.; Kales, S.N. The obesity epidemic and future emergency responders. Obesity 2009, 17, 1648–1650. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.L.; Franke, W.D. Prevalence of cardiovascular disease risk factors in volunteer firefighters. J. Occup. Environ. Med. 2009, 51, 958–962. [Google Scholar] [CrossRef] [PubMed]
- McAllister, M.J.; Gonzalez, D.E.; Leonard, M.; Martaindale, M.H.; Bloomer, R.J.; Pence, J.; Martin, S.E. Firefighters with higher cardiorespiratory fitness demonstrate lower markers of cardiovascular disease risk. J. Occup. Environ. Med. 2022, 64, 1036–1040. [Google Scholar] [CrossRef] [PubMed]
- McAllister, M.J.; Gonzalez, D.E.; Leonard, M.; Martaindale, M.H.; Bloomer, R.J.; Pence, J.; Martin, S.E. Risk factors for cardiometabolic disease in professional firefighters. J. Occup. Environ. Med. 2023, 65, 119–124. [Google Scholar] [CrossRef]
- Gonzalez, D.E.; McAllister, M.J.; Waldman, H.S.; Ferrando, A.A.; Joyce, J.; Barringer, N.D.; Dawes, J.J.; Kieffer, A.J.; Harvey, T.; Kerksick, C.M.; et al. International society of sports nutrition position stand: Tactical athlete nutrition. J. Int. Soc. Sports Nutr. 2022, 19, 267–315. [Google Scholar] [CrossRef]
- Mayer, J.M.; Nuzzo, J.L.; Chen, R.; Quillen, W.S.; Verna, J.L.; Miro, R.; Dagenais, S. The impact of obesity on back and core muscular endurance in firefighters. J. Obes. 2012, 2012, 729283. [Google Scholar] [CrossRef]
- Jahnke, S.A.; Poston, W.S.C.; Haddock, C.K.; Jitnarin, N. Obesity and incident injury among career firefighters in the central United States. Obesity 2013, 21, 1505–1508. [Google Scholar] [CrossRef] [PubMed]
- Farioli, A.; Yang, J.; Teehan, D.; Baur, D.M.; Smith, D.L.; Kales, S.N. Duty-related risk of sudden cardiac death among young US firefighters. Occup. Med. 2014, 64, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Teehan, D.; Farioli, A.; Baur, D.M.; Smith, D.; Kales, S.N. Sudden cardiac death among firefighters ≤ 45 years of age in the United States. Am. J. Cardiol. 2013, 112, 1962–1967. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Gibbons, L.W.; Kampert, J.B.; Nichaman, M.Z.; Blair, S.N. Low cardiorespiratory fitness and physical inactivity as predictors of mortality in men with type 2 diabetes. Ann. Intern. Med. 2000, 132, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Kampert, J.B.; Barlow, C.E.; Nichaman, M.Z.; Gibbons, L.W.; Paffenbarger, R.S., Jr.; Blair, S.N. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA 1999, 282, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Church, T.S.; Kampert, J.B.; Gibbons, L.W.; Barlow, C.E.; Blair, S.N. Usefulness of cardiorespiratory fitness as a predictor of all-cause and cardiovascular disease mortality in men with systemic hypertension. Am. J. Cardiol. 2001, 88, 651–656. [Google Scholar] [CrossRef]
- Löllgen, H.; Leyk, D. Exercise testing in sports medicine. Dtsch. Arztebl. 2018, 115, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Laveneziana, P.; Di Paolo, M.; Palange, P. The clinical value of cardiopulmonary exercise testing in the modern era. Eur. Respir. Rev. 2021, 30, 200187. [Google Scholar] [CrossRef]
- NFPA 1582; Standard on Comprehensive Occupational Medical Programs for Fire Departments. National Fire Protection Association: Quincy, MA, USA, 2018.
- Ashton, R.E.; Tew, G.A.; Aning, J.J.; Gilbert, S.E.; Lewis, L.; Saxton, J.M. Effects of short-term, medium-term and long-term resistance exercise training on cardiometabolic health outcomes in adults: Systematic review with meta-analysis. Br. J. Sports Med. 2020, 54, 341–348. [Google Scholar] [CrossRef]
- Nagel, T.; Melton, B.; Grosicki, G.J. Fighting arterial stiffness: A case for the importance of cardiorespiratory fitness in firefighters. Med. Hypotheses 2022, 162, 110831. [Google Scholar] [CrossRef]
- Baur, D.M.; Christophi, C.A.; Tsismenakis, A.J.; Cook, E.F.; Kales, S.N. Cardiorespiratory fitness predicts cardiovascular risk profiles in career firefighters. J. Occup. Environ. Med. 2011, 53, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Wedell-Neergaard, A.S.; Krogh-Madsen, R.; Petersen, G.L.; Hansen, Å.M.; Pedersen, B.K.; Lund, R.; Bruunsgaard, H. Cardiorespiratory fitness and the metabolic syndrome: Roles of inflammation and abdominal obesity. PLoS ONE 2018, 13, e0194991. [Google Scholar] [CrossRef] [PubMed]
- Ras, J.; Kengne, A.P.; Smith, D.L.; Soteriades, E.S.; Leach, L. Association between cardiovascular disease risk factors and cardiorespiratory fitness in firefighters: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2023, 20, 2816. [Google Scholar] [CrossRef]
- Strauss, M.; Foshag, P.; Jehn, U.; Brzęk, A.; Littwitz, H.; Leischik, R. Higher cardiorespiratory fitness is strongly associated with lower cardiovascular risk factors in firefighters: A cross-sectional study in a German fire brigade. Sci. Rep. 2021, 11, 2445. [Google Scholar] [CrossRef] [PubMed]
- McKinney, Z.J.; Bovard, R.S.; Starchook-Moore, M.N.; Ronneberg, K.; Xi, M.; Bredeson, D.M.; Schwartz, E.C.; Thelen, S.L.; Nash, T.L.; Dickinson, M.; et al. Cardiorespiratory fitness of firefighters: Initial results of a multi-phased study. J. Occup. Environ. Med. 2021, 63, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.M.; Christophi, C.A.; Cook, E.F.; Kales, S.N. Age-related decline in cardiorespiratory fitness among career firefighters: Modification by physical activity and adiposity. J. Obes. 2012, 2012, 710903. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Barr, D.; Boland, D.M.; Smith, D.L.; Cooper, C.B. Validation of the firefighter WFI treadmill protocol for predicting VO2 max. Occup. Med. 2015, 65, 143–146. [Google Scholar] [CrossRef]
- Delisle, A.T.; Piazza-Gardner, A.K.; Cowen, T.L.; Huq, M.B.; Delisle, A.D.; Stopka, C.B.; Tillman, M.D. Validation of a cardiorespiratory fitness assessment for firefighters. J. Strength Cond. Res. 2014, 28, 2717–2723. [Google Scholar] [CrossRef]
- Hale, D.; Kollock, R.; Thomas, J.; Sanders, G.; Peveler, W.; Mangan, A.; Landon, B. A submaximal field test of aerobic capacity does not accurately reflect VO2max in career firefighters. Int. J. Exerc. Sci. 2022, 15, 221–230. [Google Scholar]
- Yang, J.; Christophi, C.A.; Farioli, A.; Baur, D.M.; Moffatt, S.; Zollinger, T.W.; Kales, S.N. Association between push-up exercise capacity and future cardiovascular events among active adult men. JAMA 2019, 2, e188341. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Durand, G.; Tsismenakis, A.J.; Jahnke, S.A.; Baur, D.M.; Christophi, C.A.; Kales, S.N. Firefighters’ physical activity: Relation to fitness and cardiovascular disease risk. Med. Sci. Sports Exerc. 2011, 43, 1752–1759. [Google Scholar] [CrossRef]
- NFPA 1583; Standard on Health-Related Fitness Programs for Firefighters. National Fire Protection Association: Quincy, MA, USA, 2015.
- National Fire Protection Association. The Fifth Needs Assessment of the United States Fire Service; National Fire Protection Association: Quincy, MA, USA, 2021. [Google Scholar]
- Melton, B.F.; Ryan, G.; Snarr, R.L.; Weeks, M.; Langford, E.; Villafuerte, M. Fitness policies within the fire service: A pilot investigation of exercise adherence on fitness outcomes among rural firefighters. Am. J. Lifestyle Med. 2021, 17, 437–442. [Google Scholar] [CrossRef] [PubMed]
- NFPA 1582; Standard on Comprehensive Occupational Medical Programs for Fire Departments. National Fire Protection Association: Quincy, MA, USA, 2007.
- Williford, H.N.; Duey, W.J.; Olson, M.S.; Howard, R.; Wang, N. Relationship between fire fighting suppression tasks and physical fitness. Ergonomics 1999, 42, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Albert, C.M.; Mittleman, M.A.; Chae, C.U.; Lee, I.M.; Hennekens, C.H.; Manson, J.E. Triggering of sudden death from cardiac causes by vigorous exertion. N. Engl. J. Med. 2000, 343, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Getty, A.K.; Wisdo, T.R.; Chavis, L.N.; Derella, C.C.; McLaughlin, K.C.; Perez, A.N.; DiCiurcio, W.T., 3rd; Corbin, M.; Feairheller, D.L. Effects of circuit exercise training on vascular health and blood pressure. Prev. Med. Rep. 2018, 10, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Martin, Z.T.; Schlaff, R.A.; Hemenway, J.K.; Coulter, J.R.; Knous, J.L.; Lowry, J.E.; Ode, J.J. Cardiovascular disease risk factors and physical fitness in volunteer firefighters. Int. J. Exerc. Sci. 2019, 12, 764–776. [Google Scholar] [PubMed]
- McLaughlin, K.C.; Perez, A.N.; Donahue, S.; Feairheller, D.L. Tactical circuit training improves blood pressure and vascular health more than resistance training. Int. J. Exerc. Sci. 2021, 14, 1320–1333. [Google Scholar]
- Pawlak, R.; Clasey, J.L.; Palmer, T.; Symons, T.B.; Abel, M.G. The effect of a novel tactical training program on physical fitness and occupational performance in firefighters. J. Strength Cond. Res. 2015, 29, 578–588. [Google Scholar] [CrossRef]
- Joe, M.J.; Hatsu, I.E.; Tefft, A.; Mok, S.; Adetona, O. Dietary behavior and diet interventions among structural firefighters: A narrative review. Nutrients 2022, 14, 4662. [Google Scholar] [CrossRef]
- Burris, J.C.; Werner, C.M.; Woolf, K. The relationship between dietary intake and dietary-focused lifestyle interventions on risk factors associated with cardiovascular disease in firefighters. Curr. Nutr. Rep. 2022, 11, 206–224. [Google Scholar] [CrossRef]
- Kadiwar, P.; Shah, N.; Black, T.; Caban-Martinez, A.J.; Steinberg, M.; Black, K.; Sackey, J.; Graber, J. Dietary intake among members of a volunteer fire department compared with us daily dietary recommendations. J. Occup. Environ. Med. 2021, 63, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.; Mayer, J.M. Evaluating nutrient intake of career firefighters compared to military dietary reference intakes. Nutrients 2020, 12, 1876. [Google Scholar] [CrossRef] [PubMed]
- Aragon, A.A.; Schoenfeld, B.J.; Wildman, R.; Kleiner, S.; VanDusseldorp, T.; Taylor, L.; Earnest, C.P.; Arciero, P.J.; Wilborn, C.; Kalman, D.S.; et al. International society of sports nutrition position stand: Diets and body composition. J. Int. Soc. Sports Nutr. 2017, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Yang, J.; Farioli, A.; Korre, M.; Kales, S.N. Dietary preferences and nutritional information needs among career firefighters in the United States. Glob. Adv. Health Med. 2015, 4, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Mertens, E.; Mullie, P.; Deforche, B.; Lefevre, J.; Charlier, R.; Huybrechts, I.; Clarys, P. Cross-sectional study on the relationship between the Mediterranean Diet Score and blood lipids. Nutr. J. 2014, 13, 88. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Farioli, A.; Korre, M.; Kales, S.N. Modified Mediterranean diet score and cardiovascular risk in a North American working population. PLoS ONE 2014, 9, e87539. [Google Scholar] [CrossRef]
- McAllister, M.J.; Gonzalez, A.E.; Waldman, H.S. Impact of time restricted feeding on markers of cardiometabolic health and oxidative stress in resistance-trained firefighters. J. Strength Cond. Res. 2022, 36, 2515–2522. [Google Scholar] [CrossRef]
- Gonzalez, A.E.; Waldman, H.S.; Abel, M.G.; McCurdy, K.W.; McAllister, M.J. Impact of time restricted feeding on fitness variables in professional resistance trained firefighters. J. Occup. Environ. Med. 2021, 63, 343–349. [Google Scholar] [CrossRef]
- Almeida, A.A.; Reeve, E.H.; Dickinson, R.L.; Carty, M.; Gilpin, J.; Feairheller, D.L. Civilians have higher adherence and more improvements in health with a mediterranean diet and circuit training program compared with firefighters. J. Occup. Environ. Med. 2022, 64, 488–494. [Google Scholar] [CrossRef]
- Patterson, R.E.; Sears, D.D. Metabolic effects of intermittent fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef] [PubMed]
- Kellawan, J.M.; Stuart-Hill, L.A.; Petersen, S.R. The effects of caffeine during exercise in fire protective ensemble. Ergonomics 2009, 52, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Wassell, S.D.; Edwards, E.S.; Saunders, M.J.; Womack, C.J. Effect of caffeine on the hemostatic response to firefighting drills. J. Caffeine Adenosine Res. 2020, 10, 117–123. [Google Scholar] [CrossRef]
- McAllister, M.J.; Basham, S.A.; Smith, J.W.; Waldman, H.S.; Krings, B.M.; Mettler, J.A.; Butawan, M.B.; Bloomer, R.J. Effects of environmental heat and antioxidant ingestion on blood markers of oxidative stress in professional firefighters performing structural fire exercises. J. Occup. Environ. Med. 2018, 60, e595–e601. [Google Scholar] [CrossRef] [PubMed]
- Barros, B.; Oliveira, M.; Morais, S. Firefighters’ occupational exposure: Contribution from biomarkers of effect to assess health risks. Environ. Int. 2021, 156, 106704. [Google Scholar] [CrossRef] [PubMed]
- Horn, G.P.; Kesler, R.M.; Motl, R.W.; Hsiao-Wecksler, E.T.; Klaren, R.E.; Ensari, I.; Petrucci, M.N.; Fernhall, B.; Rosengren, K.S. Physiological responses to simulated firefighter exercise protocols in varying environments. Ergonomics 2015, 58, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Waldman, H.S.; Bryant, A.R.; Shepherd, B.D.; Egan, B.; McAllister, M.J. No effect of a ketone monoester on markers of stress and performance in a live-burn search and rescue in firefighters. J. Strength Cond. Res. 2022, 36, 763–771. [Google Scholar] [CrossRef]
- Smolander, J.; Louhevaara, V.; Tuomi, T.; Korhonen, O.; Jaakkola, J. Cardiorespiratory and thermal effects of wearing gas protective clothing. Int. Arch. Occup. Environ. Health 1984, 54, 261–270. [Google Scholar] [CrossRef]
- Larsen, B.; Snow, R.; Williams-Bell, M.; Aisbett, B. Simulated firefighting task performance and physiology under very hot conditions. Front. Physiol. 2015, 6, 322. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.S.; McLellan, T.M.; Tenaglia, S. The thermophysiology of uncompensable heat stress physiological manipulations and individual characteristics. Sports Med. 2000, 29, 329–359. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the academy of nutrition and dietetics, dietitians of Canada, and the American college of sports medicine: Nutrition and athletic performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef] [PubMed]
- Edgar, D.; Dement, W.; Fuller, C. Effect of SCN lesions on sleep in squirrel monkeys: Evidence for opponent processes in sleep-wake regulation. J. Neurosci. 1993, 13, 1065–1079. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2015, 66, 143–172. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.R.; Roth, T. Shift work sleep disorder: Burden of illness and approaches to management. Drugs 2006, 66, 2357–2370. [Google Scholar] [CrossRef]
- Roth, T. Characteristics and determinants of normal sleep. J. Clin. Psychiatry 2004, S16, 8–11. [Google Scholar]
- Rosekind, M.R.; Gander, P.H.; Gregory, K.B.; Smith, R.M.; Miller, D.L.; Oyung, R.; Webbon, L.L.; Johnson, J.M. Managing fatigue in operational settings 1: Physiological considerations and counter-measures. Hosp. Top. 1997, 75, 23–30. [Google Scholar] [CrossRef]
- Stout, J.W.; Beidel, D.C.; Brush, D.; Bowers, C. Sleep disturbance and cognitive functioning among firefighters. J. Health Psychol. 2020, 26, 2248–2259. [Google Scholar] [CrossRef]
- Christoforou, T.; Cvirn, M.; Ferguson, S.; Armstrong, T.; Smith, B. The effect of sleep restriction and exposure to physical activity on the cognitive ability of volunteer firefighters across a 3-day simulated fire-ground tour. In Sleep, Performance and Wellbeing in Adults and Adolescents; Sargent, C., Zhou, X., Eds.; Australasian Chronobiology Society: Adelaide, Australia, 2013; pp. 13–17. [Google Scholar]
- Banks, S.; Dinges, D.F. Behavioral and physiological consequences of sleep restriction. J. Clin. Sleep Med. 2007, 3, 519–528. [Google Scholar] [CrossRef]
- Liu, Y.; Tanaka, H. Overtime work, insufficient sleep, and risk of non-fatal acute myocardial infarction in Japanese men. Occup. Environ. Med. 2002, 59, 447–451. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- Reaven, G.M.; Lithell, H.; Landsberg, L. Hypertension and associated metabolic abnormalities—The role of insulin resistance and the sympathoadrenal system. N. Engl. J. Med. 1996, 334, 374–382. [Google Scholar] [CrossRef]
- Carey, M.G.; Al-Zaiti, S.S.; Dean, G.E.; Sessanna, L.; Finnell, D.S. Sleep problems, depression, substance use, social bonding, and quality of life in professional firefighters. J. Occup. Environ. Med. 2011, 53, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Mullington, J.M.; Haack, M.; Toth, M.; Serrador, J.M.; Meier-Ewert, H.K. Cardiovascular, inflammatory, and metabolic consequences of sleep deprivation. Prog. Cardiovasc. Dis. 2009, 51, 294–302. [Google Scholar] [CrossRef]
- Palagini, L.; Bruno, R.M.; Gemignani, A.; Baglioni, C.; Ghiadoni, L.; Riemann, D. Sleep loss and hypertension: A systematic review. Curr. Pharm. Des. 2013, 19, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Deboer, T. Long-term effect of a single dose of caffeine on sleep, the sleep EEG and neuronal activity in the peduncular part of the lateral hypothalamus under constant dark conditions. Clocks Sleep 2022, 4, 260–276. [Google Scholar] [CrossRef] [PubMed]
- Brachtel, D.; Richter, E. Absolute bioavailability of caffeine from a tablet formulation. J. Hepatol. 1992, 16, 385. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Military Nutrition Research. Caffeine for the Sustainment of Mental Task Performance: Formulations for Military Operations; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Arnaud, M.J. The pharmacology of caffeine. In Progress in Drug Research/Fortschritte der Arzneimittelforschung/Progrès des Recherches Pharmaceutiques; Birkhäuser: Basel, Switzerland, 1987; Volume 31, pp. 273–313. [Google Scholar] [CrossRef]
- Roehrs, T.; Roth, T. Caffeine: Sleep and daytime sleepiness. Sleep Med. Rev. 2008, 12, 153–162. [Google Scholar] [CrossRef]
- Thakkar, M.M.; Sharma, R.; Sahota, P. Alcohol disrupts sleep homeostasis. Alcohol 2015, 49, 299–310. [Google Scholar] [CrossRef]
- Smith, L.J.; Gallagher, M.W.; Tran, J.K.; Vujanovic, A.A. Posttraumatic stress, alcohol use, and alcohol use reasons in firefighters: The role of sleep disturbance. Compr. Psychiatry 2018, 87, 64–71. [Google Scholar] [CrossRef]
- Jaehne, A.; Unbehaun, T.; Feige, B.; Lutz, U.C.; Batra, A.; Riemann, D. How smoking affects sleep: A polysomnographical analysis. Sleep Med. 2012, 13, 1286–1292. [Google Scholar] [CrossRef]
- Zhang, L.; Samet, J.; Caffo, B.; Punjabi, N.M. Cigarette smoking and nocturnal sleep architecture. Am. J. Epidemiol. 2006, 164, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Sabanayagam, C.; Shankar, A. The association between active smoking, smokeless tobacco, second-hand smoke exposure and insufficient sleep. Sleep Med. 2011, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- McGillis, Z.; Dorman, S.C.; Robertson, A.; Larivière, M.; Leduc, C.; Eger, T.; Oddson, B.E.; Larivière, C. Sleep quantity and quality of ontario wildland firefighters across a low-hazard fire season. J. Occup. Environ. Med. 2017, 59, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Lee, C.T.; Yeung, W.F.; Chan, M.S.; Chung, E.W.; Lin, W.L. Sleep hygiene education as a treatment of insomnia: A systematic review and meta-analysis. Fam. Pract. 2018, 35, 365–375. [Google Scholar] [CrossRef]
- Billings, J.; Focht, W. Firefighter shift schedules affect sleep quality. J. Occup. Environ. Med. 2016, 58, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Haddock, C.K.; Poston, W.S.C.; Jitnarin, N.; Jahnke, S.A. Excessive daytime sleepiness in firefighters in the central United States. J. Occup. Environ. Med. 2013, 55, 416–423. [Google Scholar] [CrossRef]
- Daniels, R.D.; Kubale, T.L.; Yiin, J.H.; Dahm, M.M.; Hales, T.R.; Baris, D.; Zahm, S.H.; Beaumont, J.J.; Waters, K.M.; Pinkerton, L.E. Mortality and cancer incidence in a pooled cohort of US firefighters from San Francisco, Chicago and Philadelphia (1950–2009). Occup. Environ. Med. 2014, 71, 388–397. [Google Scholar] [CrossRef]
- Demers, P.A.; DeMarini, D.M.; Fent, K.W.; Glass, D.C.; Hansen, J.; Adetona, O.; Andersen, M.H.; Freeman, L.E.B.; Caban-Martinez, A.J.; Daniels, R.D.; et al. Carcinogenicity of occupational exposure as a firefighter. Lancet Oncol. 2022, 23, 985–986. [Google Scholar] [CrossRef]
- Jalilian, H.; Ziaei, M.; Weiderpass, E.; Rueegg, C.S.; Khosravi, Y.; Kjaerheim, K. Cancer incidence and mortality among firefighters. Int. J. Cancer 2019, 145, 2639–2646. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; Kim, J.; Christophi, C.A.; Kales, S.N. Cancer incidence and mortality in firefighters: A state-of-the-art review and meta-َanalysis. Asian Pac. J. Cancer Prev. 2019, 20, 3221–3231. [Google Scholar] [CrossRef] [PubMed]
- Fent, K.W.; Siegel, M.R.; Mayer, A.C.; Wilkinson, A.; Wepsala, W. Charting new territory: Understanding cancer in firefighters. Int. Fire Serv. J. Leadersh. Manag. 2020, 16, 7–15. [Google Scholar]
- Young, A.S.; Sparer-Fine, E.H.; Pickard, H.M.; Sunderland, E.M.; Peaslee, G.F.; Allen, J.G. Per- and polyfluoroalkyl substances (PFAS) and total fluorine in fire station dust. J. Expo. Sci. Environ. Epidemiol. 2021, 31, 930–942. [Google Scholar] [CrossRef]
- Engelsman, M.; Toms, L.L.; Banks, A.P.W.; Wang, X.; Mueller, J.F. Biomonitoring in firefighters for volatile organic compounds, semivolatile organic compounds, persistent organic pollutants, and metals: A systematic review. Environ. Res. 2020, 188, 109562. [Google Scholar] [CrossRef]
- Baxter, C.S.; Hoffman, J.D.; Knipp, M.J.; Reponen, T.; Haynes, E.N. Exposure of firefighters to particulates and polycyclic aromatic hydrocarbons. J. Occup. Environ. Hyg. 2014, 11, D85–D91. [Google Scholar] [CrossRef] [PubMed]
- Fent, K.W.; Eisenberg, J.; Snawder, J.; Sammons, D.; Pleil, J.D.; Stiegel, M.A.; Mueller, C.; Horn, G.P.; Dalton, J. Systemic exposure to PAHs and benzene in firefighters suppressing controlled structure fires. Ann. Occup. Hyg. 2014, 58, 830–845. [Google Scholar] [CrossRef]
- Fent, K.W.; Toennis, C.; Sammons, D.; Robertson, S.; Bertke, S.; Calafat, A.M.; Pleil, J.D.; Geer Wallace, M.A.; Kerber, S.; Smith, D.L.; et al. Firefighters’ and instructors’ absorption of PAHs and benzene during training exercises. Int. J. Hyg. Environ. Health 2019, 222, 991–1000. [Google Scholar] [CrossRef]
- Horn, G.P.; Fent, K.W.; Kerber, S.; Smith, D.L. Hierarchy of contamination control in the fire service: Review of exposure control options to reduce cancer risk. J. Occup. Environ. Hyg. 2022, 19, 538–557. [Google Scholar] [CrossRef]
- Peaslee, G.F.; Wilkinson, J.T.; McGuinness, S.R.; Tighe, M.; Caterisano, N.; Lee, S.; Gonzales, A.; Roddy, M.; Mills, S.; Mitchell, K. Another pathway for firefighter exposure to per- and polyfluoroalkyl substances: Firefighter textiles. Environ. Sci. Technol. Lett. 2020, 7, 594–599. [Google Scholar] [CrossRef]
- Lesniak, A.Y.; Bergstrom, H.C.; Clasey, J.L.; Stromberg, A.J.; Abel, M.G. The effect of personal protective equipment on firefighter occupational performance. J. Strength Cond. Res. 2020, 34, 2165–2172. [Google Scholar] [CrossRef]
- Dempsey, J.A.; Neder, J.A.; Phillips, D.B.; O’Donnell, D.E. The physiology and pathophysiology of exercise hyperpnea. Handb. Clin. Neurol. 2022, 188, 201–232. [Google Scholar] [CrossRef] [PubMed]
- Jaques, P.A.; Kim, C.S. Measurement of total lung deposition of inhaled ultrafine particles in healthy men and women. Inhal. Toxicol. 2000, 12, 715–731. [Google Scholar] [CrossRef]
- Wilson, T.E.; Cui, J.; Zhang, R.; Crandall, C.G. Heat stress reduces cerebral blood velocity and markedly impairs orthostatic tolerance in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 291, R1443–R1448. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, M.; Wilson, T.E.; Crandall, C.G. Neural control and mechanisms of eccrine sweating during heat stress and exercise. J. Appl. Physiol. 2006, 100, 1692–1701. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.E. Cardiovascular and metabolic responses to thermal insults. In Theory and Applications of Heat Transfer in Cells and Organs; Shrivastava, D., Ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2018. [Google Scholar]
- Dąbrowska, A.K.; Spano, F.; Derler, S.; Adlhart, C.; Spencer, N.D.; Rossi, R.M. The relationship between skin function, barrier properties, and body-dependent factors. Skin. Res. Technol. 2018, 24, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Lademann, J.; Otberg, N.; Richter, H.; Meyer, L.; Audring, H.; Teichmann, A.; Thomas, S.; Knüttel, A.; Sterry, W. Application of optical non-invasive methods in skin physiology: A comparison of laser scanning microscopy and optical coherent tomography with histological analysis. Skin. Res. Technol. 2007, 13, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Firefighter-Cancer-Support-Network, “Taking Action Against Cancer in the Fire Service”. 2013. Available online: https://firefightercancersupport.org/wp-content/uploads/2017/11/taking-action-against-cancer-in-the-fire-service-pdf.pdf (accessed on 1 November 2023).
- Federal Emergency Management Agency. Safety and Health Considerations for the Design of Fire and Emergency Medical Services Stations; April–May 2018 Report; U.S. Fire Administration: Emmitsburg, MD, USA, 2018.
- Song, G.; Wang, F. (Eds.) Firefighters’ Clothing and Equipment: Performance, Protection, and Comfort, 1st ed.; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Ruderman Family Foundation. The Ruderman White Paper on Mental Health and Suicide of First Responders. Report by Primary Contributor Heyman, M. Prepared April 2018. Available online: https://rudermanfoundation.org/white_papers/police-officers-and-firefighters-are-more-likely-to-die-by-suicide-than-in-line-of-duty/ (accessed on 11 October 2023).
- Stanley, I.H.; Hom, M.A.; Hagan, C.R.; Joiner, T.E. Career prevalence and correlates of suicidal thoughts and behaviors among firefighters. J. Affect. Disord. 2015, 187, 163–171. [Google Scholar] [CrossRef]
- Carson, L.M.; Marsh, S.M.; Brown, M.M.; Elins, K.L.; Tiesman, H.M. An analysis of suicides among first responders—Findings from the National Violent Death Reporting System, 2015–2017. J. Safety Res. 2023, 85, 361–370. [Google Scholar] [CrossRef]
- Vigil, N.H.; Beger, S.; Gochenour, K.S.; Frazier, W.H.; Vadeboncoeur, T.F.; Bobrow, B.J. Suicide among the EMS occupation in the United States. West. J. Emerg. Med. 2021, 22, 326–332. [Google Scholar] [CrossRef]
- Mumford, E.A.; Liu, W.; Taylor, B.G. Profiles of U.S. law enforcement officers’ physical, psychological, and behavioral health: Results from a nationally representative survey of officers. Police Q. 2021, 24, 357–381. [Google Scholar] [CrossRef]
- Rudofossi, D.M. Working with Traumatized Police Officer Patients: A Clinician’s Guide to Complex PTSD Syndromes in Public Safety Professionals; Routledge: London, UK, 2007. [Google Scholar]
- DeMoulin, D.; Jacobs, S.; Nam, Y.; Harding, A.B.; Moskowitz, A.F.; Shi, Y.; Kim, H. Mental health among firefighters. J. Occup. Environ. Med. 2022, 64, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Stelnicki, A.M.; Jamshidi, L.; Taillieu, T.L.; Carleton, R.N.; Afifi, T.O. Mental health and well-being among children of public safety personnel in Canada. Int. J. Environ. Res. Public Health 2022, 19, 14030. [Google Scholar] [CrossRef] [PubMed]
- MacDermid, J.C.; Lomotan, M.; Hu, M.A. Canadian career firefighters’ mental health impacts and priorities. Int. J. Environ. Res. Public Health 2021, 18, 12666. [Google Scholar] [CrossRef]
- Giessing, L.; Oudejans, R.R.; Hutter, V.; Plessner, H.; Strahler, J.; Frenkel, M.O. Acute and chronic stress in daily police service: A three-week N-of-1 study. Psychoneuroendocrinology 2020, 112, 104865. [Google Scholar] [CrossRef] [PubMed]
- Guidi, J.; Lucente, M.; Sonino, N.; Fava, G.A. Allostatic load and its impact on health: A systematic review. Psychother. Psychosom. 2021, 90, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World through Mindfulness; Hachett Books: New York, NY, USA, 2005. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living; Delta: New York, NY, USA, 1990. [Google Scholar]
- McCown, D.; Reibel, D.; Micozzi, M.S. Teaching Mindfulness: A Practical Guide for Clinicians and Educators; Springer: New York, NY, USA, 2011. [Google Scholar]
- Counson, I.; Hosemans, D.; Lai, T.J.; Mott, B.; Harvey, S.B.; Joyce, S. Mental health and mindfulness among Australian firefighters. BMC Psychol. 2019, 7, 34. [Google Scholar] [CrossRef]
- Stanley, I.H.; Boffa, J.W.; Tran, J.K.; Schmit, N.B.; Joiner, T.E.; Vujanovic, A.A. Posttraumatic stress disorder symptoms and mindfulness facets in relation to suicide risk among firefighters. J. Clin. Psychol. 2019, 75, 696–709. [Google Scholar] [CrossRef]
- Smith, B.W.; Ortiz, J.A.; Steffen, L.E.; Tooley, E.M.; Wiggins, K.T.; Yeater, E.A.; Montoya, J.D. Mindfulness is associated with fewer PTSD symptoms, depressive symptoms, physical symptoms, and alcohol problems in urban firefighters. J. Consult. Clin. Psychol. 2011, 79, 613–617. [Google Scholar] [CrossRef]
- Denkova, E.; Zanesco, A.P.; Rogers, S.L.; Jha, A.P. Is resilience trainable? An initial study comparing mindfulness and relaxation training in firefighters. Psychiatry Res. 2020, 285, 112794. [Google Scholar] [CrossRef]
- Mitchell, J.T.; Bray, G. Emergency Services Stress: Guidelines for Preserving the Health and Careers of Emergency Services Personnel; Prentice Hall: Englewood Cliffs, NJ, USA, 1990. [Google Scholar]
- Jeannette, J.M.; Scoboria, A. Firefighter preferences regarding post-incident intervention. Work Stress 2008, 22, 314–326. [Google Scholar] [CrossRef]
- Brewin, C.R.; Andrews, B.; Valentine, J.D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J. Consult. Clin. Psychol. 2000, 68, 748–766. [Google Scholar] [CrossRef]


{kind=link}
| Morbidity | Cardiovascular Disease | Psychological Disorders | Cancer |
|---|---|---|---|
| Countermeasure |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez, D.E.; Lanham, S.N.; Martin, S.E.; Cleveland, R.E.; Wilson, T.E.; Langford, E.L.; Abel, M.G. Firefighter Health: A Narrative Review of Occupational Threats and Countermeasures. Healthcare 2024, 12, 440. https://doi.org/10.3390/healthcare12040440
Gonzalez DE, Lanham SN, Martin SE, Cleveland RE, Wilson TE, Langford EL, Abel MG. Firefighter Health: A Narrative Review of Occupational Threats and Countermeasures. Healthcare. 2024; 12(4):440. https://doi.org/10.3390/healthcare12040440
Chicago/Turabian StyleGonzalez, Drew E., Sarah N. Lanham, Steven E. Martin, Richard E. Cleveland, Thad E. Wilson, Emily L. Langford, and Mark G. Abel. 2024. "Firefighter Health: A Narrative Review of Occupational Threats and Countermeasures" Healthcare 12, no. 4: 440. https://doi.org/10.3390/healthcare12040440
APA StyleGonzalez, D. E., Lanham, S. N., Martin, S. E., Cleveland, R. E., Wilson, T. E., Langford, E. L., & Abel, M. G. (2024). Firefighter Health: A Narrative Review of Occupational Threats and Countermeasures. Healthcare, 12(4), 440. https://doi.org/10.3390/healthcare12040440