
Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
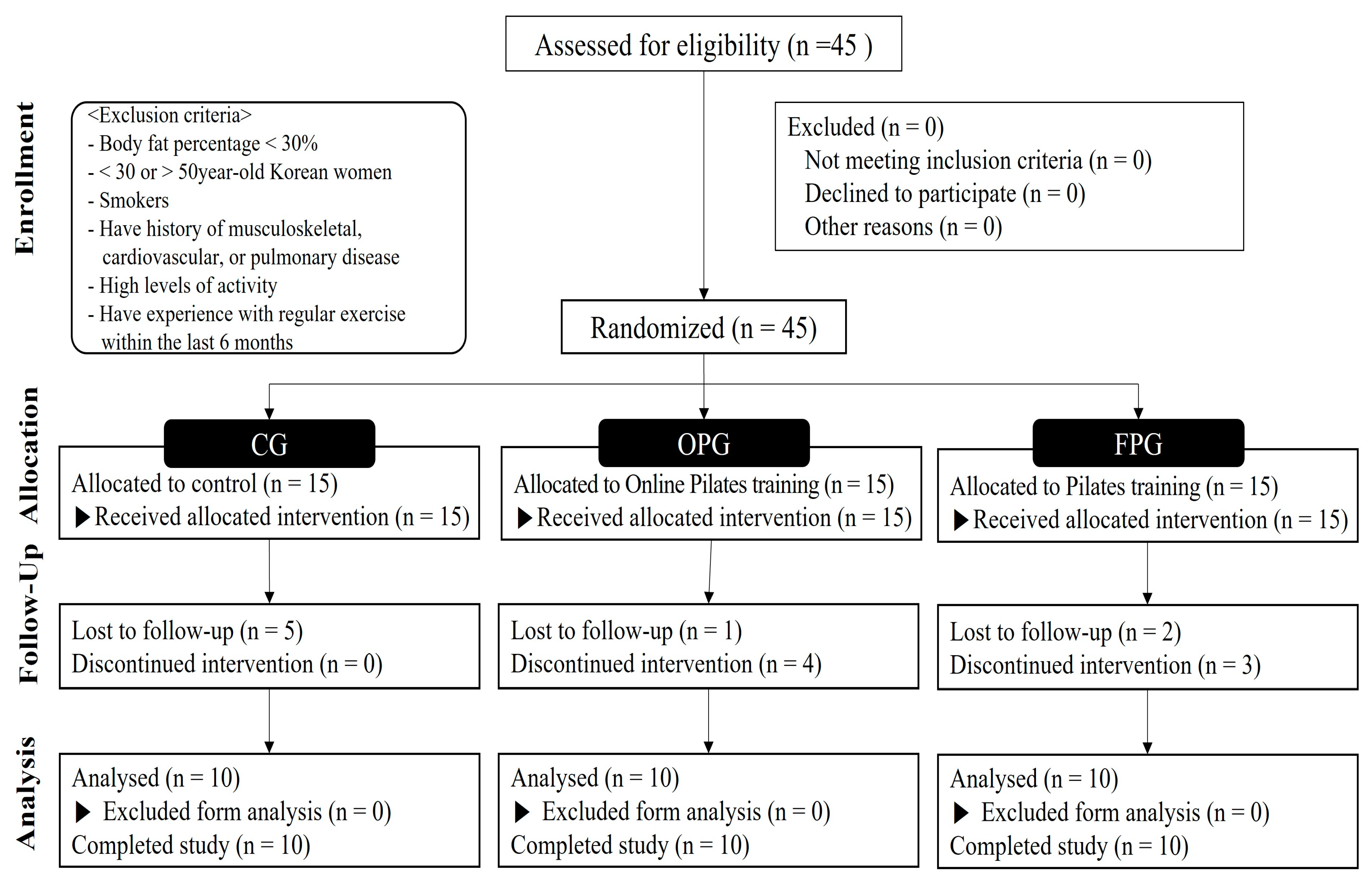
2.1. Participants
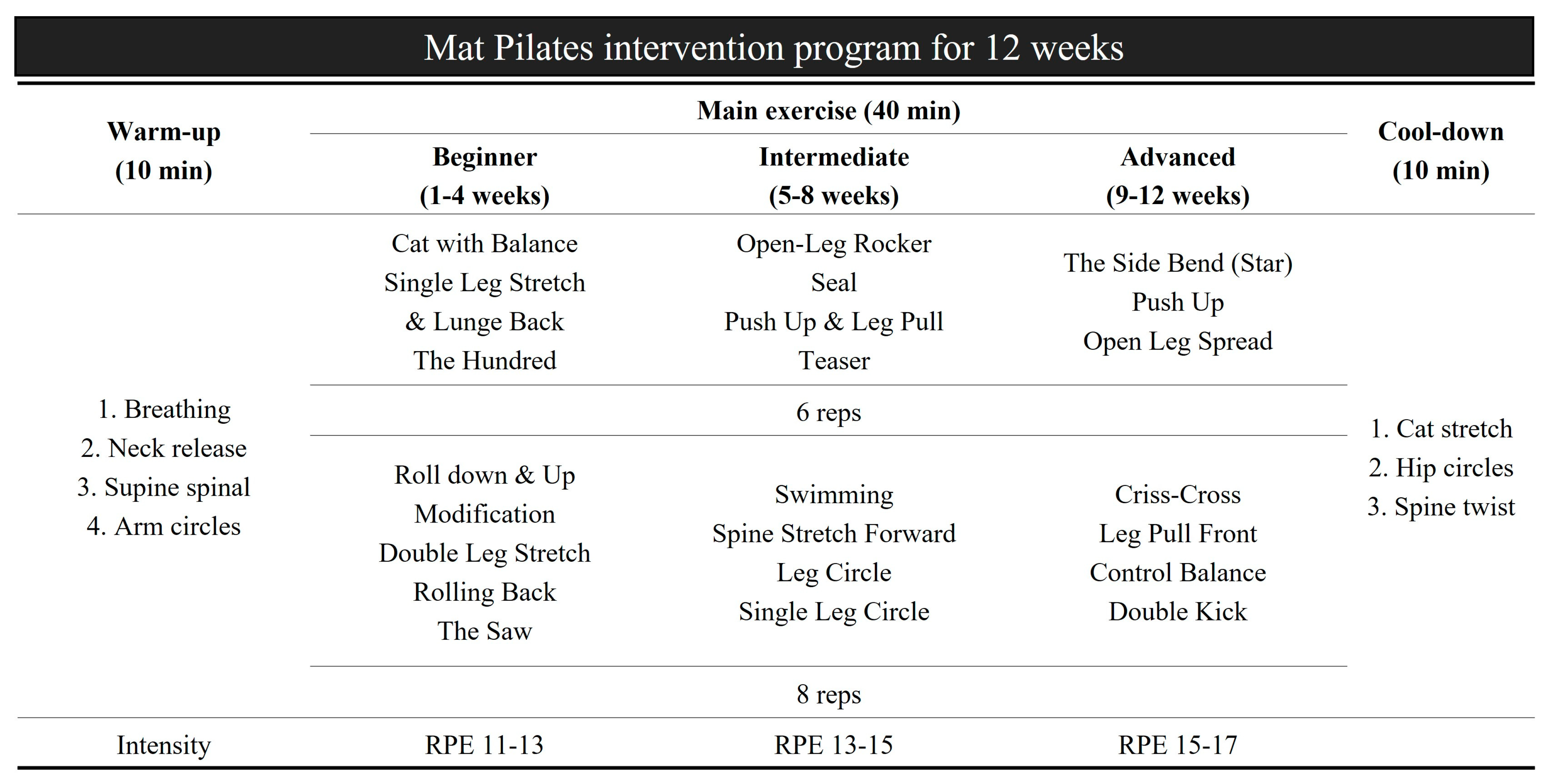
2.2. Study Design
2.3. Outcome Measurements
2.3.1. Anthropometry and Body Composition
2.3.2. Muscle Mechanical Property
2.3.3. Cardiometabolic Parameters
2.3.4. Mental Health
2.3.5. Physical Fitness
2.4. Statistical Analysis
3. Results
3.1. Anthropometry and Body Composition
3.2. Muscle Mechanical Property
3.3. Cardiometabolic Parameters
3.4. Mental Health
3.5. Physical Fitness
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Shahrbanian, S.; Alikhani, S.; Ahmadi Kakavandi, M.; Hackney, A.C. Physical Activity for Improving the Immune System of Older Adults During the COVID-19 Pandemic. Altern. Ther. Health Med. 2020, 26, 117–125. [Google Scholar] [PubMed]
- Wolf, S.; Seiffer, B.; Zeibig, J.M.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Is Physical Activity Associated with Less Depression and Anxiety During the COVID-19 Pandemic? A Rapid Systematic Review. Sports Med. 2021, 51, 1771–1783. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Jung, W.S.; Kim, J.; Lim, K. Twelve weeks of exercise modality in hypoxia enhances health-related function in obese older Korean men: A randomized controlled trial. Geriatr. Gerontol. Int. 2019, 19, 311–316. [Google Scholar] [CrossRef]
- Chin, S.H.; Kahathuduwa, C.N.; Binks, M. Physical activity and obesity: What we know and what we need to know. Obes. Rev. 2016, 17, 1226–1244. [Google Scholar] [CrossRef]
- Shook, R.P. Obesity and energy balance: What is the role of physical activity? Expert. Rev. Endocrinol. Metab. 2016, 11, 511–520. [Google Scholar] [CrossRef]
- Verheggen, R.J.; Maessen, M.F.; Green, D.J.; Hermus, A.R.; Hopman, M.T.; Thijssen, D.H. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef] [PubMed]
- Girard, O.; Malatesta, D.; Millet, G.P. Walking in Hypoxia: An Efficient Treatment to Lessen Mechanical Constraints and Improve Health in Obese Individuals? Front. Physiol. 2017, 8, 73. [Google Scholar] [CrossRef]
- Jung, K.; Kim, J.; Park, H.Y.; Jung, W.S.; Lim, K. Hypoxic Pilates Intervention for Obesity: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 7186. [Google Scholar] [CrossRef]
- Jung, K.; Seo, J.; Jung, W.S.; Kim, J.; Park, H.Y.; Lim, K. Effects of an Acute Pilates Program under Hypoxic Conditions on Vascular Endothelial Function in Pilates Participants: A Randomized Crossover Trial. Int. J. Environ. Res. Public Health 2020, 17, 2584. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Fischer, S.M.; Bagheri, R.; Park, S.Y. The Effects of Mat Pilates Training on Vascular Function and Body Fatness in Obese Young Women With Elevated Blood Pressure. Am. J. Hypertens. 2020, 33, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Bulguroglu, H.I.; Bulguroglu, M. The effects of online pilates and face-to-face pilates in healthy individuals during the COVID-19 pandemic: A randomized controlled study. BMC Sports Sci. Med. Rehabil. 2023, 15, 12. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide survey reveals fitness trends for 2010. ACSM’s Health Fit. J. 2009, 13, 9–16. [Google Scholar] [CrossRef]
- Luzi, L.; Radaelli, M.G. Influenza and obesity: Its odd relationship and the lessons for COVID-19 pandemic. Acta Diabetol. 2020, 57, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Campbell, J.P.; Gleeson, M.; Krüger, K.; Nieman, D.C.; Pyne, D.B.; Turner, J.E.; Walsh, N.P. Can exercise affect immune function to increase susceptibility to infection? Exerc. Immunol. Rev. 2020, 26, 8–22. [Google Scholar] [PubMed]
- da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende, E.S.D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2021, 21, 15–28. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, Z.; Wu, Z.; Ye, X.; Xu, X. Pilates for Overweight or Obesity: A Meta-Analysis. Front. Physiol. 2021, 12, 643455. [Google Scholar] [CrossRef]
- Dos Santos, A.N.; Serikawa, S.S.; Rocha, N.A. Pilates improves lower limbs strength and postural control during quite standing in a child with hemiparetic cerebral palsy: A case report study. Dev. Neurorehabil. 2016, 19, 226–230. [Google Scholar] [CrossRef]
- Curtis, R.G.; Ryan, J.C.; Edney, S.M.; Maher, C.A. Can Instagram be used to deliver an evidence-based exercise program for young women? A process evaluation. BMC Public Health 2020, 20, 1506. [Google Scholar] [CrossRef]
- Janjua, S.; Banchoff, E.; Threapleton, C.J.; Prigmore, S.; Fletcher, J.; Disler, R.T. Digital interventions for the management of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2021, 4, Cd013246. [Google Scholar] [CrossRef]
- Güngör, F.; Tarakci, E.; Özdemir-Acar, Z.; Soysal, A. The effects of supervised versus home Pilates-based core stability training on lower extremity muscle strength and postural sway in people with multiple sclerosis. Mult. Scler. 2022, 28, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Pérez de Villar, L.; Martínez-Olmos, F.J.; Pérez-Domínguez, F.B.; Benavent-Caballer, V.; Montañez-Aguilera, F.J.; Mercer, T.; Segura-Ortí, E. Comparison of intradialytic versus home-based exercise programs on physical functioning, physical activity level, adherence, and health-related quality of life: Pilot study. Sci. Rep. 2020, 10, 8302. [Google Scholar] [CrossRef]
- Suner-Keklik, S.; Numanoglu-Akbas, A.; Cobanoglu, G.; Kafa, N.; Guzel, N.A. An online pilates exercise program is effective on proprioception and core muscle endurance in a randomized controlled trial. Ir. J. Med. Sci. 2022, 191, 2133–2139. [Google Scholar] [CrossRef]
- Fleming, K.M.; Coote, S.B.; Herring, M.P. Home-based Pilates for symptoms of anxiety, depression and fatigue among persons with multiple sclerosis: An 8-week randomized controlled trial. Mult. Scler. 2021, 27, 2267–2279. [Google Scholar] [CrossRef] [PubMed]
- Nahm, J.-W.; Shin, Y.-J. Effects of mobile-based exercise intervention on health indices by the comparison of personal training time in male workers. Ethiop. J. Health Dev. 2020, 34, 10–17. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Siler, B. The Pilates Body: The Ultimate At-Home Guide to Strengthening, Lengthening and Toning Your Body-without Machines; Harmony: Singapore, 2000. [Google Scholar]
- Chuang, L.L.; Wu, C.Y.; Lin, K.C. Reliability, validity, and responsiveness of myotonometric measurement of muscle tone, elasticity, and stiffness in patients with stroke. Arch. Phys. Med. Rehabil. 2012, 93, 532–540. [Google Scholar] [CrossRef]
- Greene, J.; Cohen, D.; Siskowski, C.; Toyinbo, P. The Relationship Between Family Caregiving and the Mental Health of Emerging Young Adult Caregivers. J. Behav. Health Serv. Res. 2017, 44, 551–563. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Segal, N.A.; Hein, J.; Basford, J.R. The effects of Pilates training on flexibility and body composition: An observational study. Arch. Phys. Med. Rehabil. 2004, 85, 1977–1981. [Google Scholar] [CrossRef]
- Cavina, A.P.S.; Pizzo Junior, E.; Machado, A.F.; Biral, T.M.; Lemos, L.K.; Rodrigues, C.R.D.; Pastre, C.M.; Vanderlei, F.M. Effects of the Mat Pilates Method on Body Composition: Systematic Review with Meta-Analysis. J. Phys. Act. Health 2020, 17, 673–681. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; Jesús de la Torre-Cruz, M.; Jiménez-García, J.D.; Zagalaz-Anula, N.; Redecillas-Peiró, M.T.; Mendoza-Ladrón de Guevara, N.; Hita-Contreras, F. The Influence of Pilates Exercises on Body Composition, Muscle Strength, and Gait Speed in Community-Dwelling Older Women: A Randomized Controlled Trial. J. Strength. Cond. Res. 2022, 36, 2298–2305. [Google Scholar] [CrossRef]
- Şavkin, R.; Aslan, U.B. The effect of Pilates exercise on body composition in sedentary overweight and obese women. J. Sports Med. Phys. Fit. 2017, 57, 1464–1470. [Google Scholar] [CrossRef]
- Nyenhuis, S.M.; Greiwe, J.; Zeiger, J.S.; Nanda, A.; Cooke, A. Exercise and Fitness in the Age of Social Distancing During the COVID-19 Pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 2152–2155. [Google Scholar] [CrossRef] [PubMed]
- Fleming, K.M.; Herring, M.P. The effects of pilates on mental health outcomes: A meta-analysis of controlled trials. Complement. Ther. Med. 2018, 37, 80–95. [Google Scholar] [CrossRef]
- Chen, Z.; Ye, X.; Xia, Y.; Song, H.; Wang, Y.; Guan, Y.; Shen, Z.; Chen, W.; Jiang, T.; Wu, H.; et al. Effect of Pilates on Glucose and Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Physiol. 2021, 12, 641968. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, J.; Kim, C.S. The effects of pilates exercise on lipid metabolism and inflammatory cytokines mRNA expression in female undergraduates. J. Exerc. Nutr. Biochem. 2014, 18, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Khajehlandi, M.; Mohammadi, R. The effect of Pilates training on body composition, lipid profile, and serum 25-hydroxy vitamin D levels in inactive overweight women. Zahedan J. Res. Med. Sci. 2021, 23, e100502. [Google Scholar] [CrossRef]
- Hagner-Derengowska, M.; Kałużny, K.; Kochański, B.; Hagner, W.; Borkowska, A.; Czamara, A.; Budzyński, J. Effects of Nordic Walking and Pilates exercise programs on blood glucose and lipid profile in overweight and obese postmenopausal women in an experimental, nonrandomized, open-label, prospective controlled trial. Menopause 2015, 22, 1215–1223. [Google Scholar] [CrossRef]
- Khairandish, R.; Ranjbar, R.; Habibi, A. Effects of pilates training on body composition, lipid profile and some physical fitness parameters in sedentary obese women. Jundishapur Sci. Med. J. 2018, 17, 49–61. [Google Scholar]
- Senba, N.; Matsuo, H. Effect of a health education program on climacteric women. Climacteric 2010, 13, 561–569. [Google Scholar] [CrossRef]
- Dąbrowska-Galas, M.; Dąbrowska, J. Physical Activity Level and Self-Esteem in Middle-Aged Women. Int. J. Environ. Res. Public Health 2021, 18, 7293. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; Tan, A.L.; O’Connor, P.; Emery, P.; Wakefield, R.J. The effect of ageing on shear wave elastography muscle stiffness in adults. Aging Clin. Exp. Res. 2019, 31, 1755–1763. [Google Scholar] [CrossRef]
- Wells, C.; Kolt, G.S.; Bialocerkowski, A. Defining Pilates exercise: A systematic review. Complement. Ther. Med. 2012, 20, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Cronin, E.; Hickey, P.; Lynch, P.; Monaghan, K. Feasibility, safety and outcomes of an online, remotely supervised neuropilates class in a post stroke patient: A case study. Physiother. Pract. Res. 2022, 43, 113–124. [Google Scholar] [CrossRef]
- Dolgion, B.; Jeong, B.C.; Yoo, K.T. Effect of mat pilates and kinesio taping on shoulder posture and muscle characteristics of college students with round shoulder posture. J. Converg. Inf. Technol. 2021, 11, 254–264. [Google Scholar]
- Villanueva, A.; Rabal-Pelay, J.; Berzosa, C.; Gutiérrez, H.; Cimarras-Otal, C.; Lacarcel-Tejero, B.; Bataller-Cervero, A.V. Effect of a Long Exercise Program in the Reduction of Musculoskeletal Discomfort in Office Workers. Int. J. Environ. Res. Public Health 2020, 17, 9042. [Google Scholar] [CrossRef]
- Wijnhoven, H.A.; de Vet, H.C.; Picavet, H.S. Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin. J. Pain. 2006, 22, 717–724. [Google Scholar] [CrossRef]
- Marini, M.; Bendinelli, B.; Assedi, M.; Occhini, D.; Castaldo, M.; Fabiano, J.; Petranelli, M.; Migliolo, M.; Monaci, M.; Masala, G. Low back pain in healthy postmenopausal women and the effect of physical activity: A secondary analysis in a randomized trial. PLoS ONE 2017, 12, e0177370. [Google Scholar] [CrossRef]
- Bhavanani, A.B. Yoga and Mind Body Therapies in Health and Disease-A Brief Review. Ann. SBV 2019, 3, 29–41. [Google Scholar] [CrossRef]
- Burke, H.M.; Davis, M.C.; Otte, C.; Mohr, D.C. Depression and cortisol responses to psychological stress: A meta-analysis. Psychoneuroendocrinology 2005, 30, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Tafet, G.E.; Nemeroff, C.B. The Links Between Stress and Depression: Psychoneuroendocrinological, Genetic, and Environmental Interactions. J. Neuropsychiatry Clin. Neurosci. 2016, 28, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Pulopulos, M.M.; Baeken, C.; De Raedt, R. Cortisol response to stress: The role of expectancy and anticipatory stress regulation. Horm. Behav. 2020, 117, 104587. [Google Scholar] [CrossRef]
- Singla, S.; Jhamb, S.; Singh, K.D.; Kumar, A. Depression affects autonomic system of the body? Yes, it does! J. Educ. Health Promot. 2020, 9, 217. [Google Scholar] [CrossRef] [PubMed]
- Cavina, A.P.; Silva, N.M.; Biral, T.M.; Lemos, L.K.; Junior, E.P.; Pastre, C.M.; Vanderlei, L.C.; Vanderlei, F.M. Effects of 12-week Pilates training program on cardiac autonomic modulation: A randomized controlled clinical trial. J. Comp. Eff. Res. 2021, 10, 1363–1372. [Google Scholar] [CrossRef]
- Akbas, E.; Ünver, B. A six-week Pilates exercise protocol for improving physical and mental health-related parameters. Malays. J. Mov. Health Exerc. 2018, 7, 65–79. [Google Scholar] [CrossRef]
- Choi, Y.-J.; Cho, G.-S.; Kim, I.-G. The relationship between the coaching knowledge of the taekwondo instructors and satisfaction and loyalty of the trainees. Indian J. Sci. Technol. 2016, 9, 46. [Google Scholar] [CrossRef]
- Lambert, T.E.; Harvey, L.A.; Avdalis, C.; Chen, L.W.; Jeyalingam, S.; Pratt, C.A.; Tatum, H.J.; Bowden, J.L.; Lucas, B.R. An app with remote support achieves better adherence to home exercise programs than paper handouts in people with musculoskeletal conditions: A randomised trial. J. Physiother. 2017, 63, 161–167. [Google Scholar] [CrossRef]
- Moreno, M.A.; Catai, A.M.; Teodori, R.M.; Borges, B.L.; Cesar Mde, C.; Silva, E. Effect of a muscle stretching program using the Global Postural Reeducation method on respiratory muscle strength and thoracoabdominal mobility of sedentary young males. J. Bras. Pneumol. 2007, 33, 679–686. [Google Scholar] [CrossRef]
- Critchley, D.J.; Pierson, Z.; Battersby, G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Man. Ther. 2011, 16, 183–189. [Google Scholar] [CrossRef]
- Castagnoli, C.; Cecchi, F.; Del Canto, A.; Paperini, A.; Boni, R.; Pasquini, G.; Vannetti, F.; Macchi, C. Effects in Short and Long Term of Global Postural Reeducation (GPR) on Chronic Low Back Pain: A Controlled Study with One-Year Follow-Up. Sci. World J. 2015, 2015, 271436. [Google Scholar] [CrossRef]
- Park, J.M.; Hyun, G.S.; Jee, Y.S. Effects of Pilates core stability exercises on the balance abilities of archers. J. Exerc. Rehabil. 2016, 12, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Campos de Oliveira, L.; Gonçalves de Oliveira, R.; Pires-Oliveira, D.A. Effects of Pilates on muscle strength, postural balance and quality of life of older adults: A randomized, controlled, clinical trial. J. Phys. Ther. Sci. 2015, 27, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Bullo, V.; Bergamin, M.; Gobbo, S.; Sieverdes, J.C.; Zaccaria, M.; Neunhaeuserer, D.; Ermolao, A. The effects of Pilates exercise training on physical fitness and wellbeing in the elderly: A systematic review for future exercise prescription. Prev. Med. 2015, 75, 1–11. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | FPG | OPG | CG | p-Value |
|---|---|---|---|---|
| Age (year) | 43.00 ± 5.56 | 42.20 ± 5.45 | 44.60 ± 5.50 | 0.616 |
| Height (cm) | 161.52 ± 5.39 | 159.43 ± 4.50 | 160.04 ± 6.00 | 0.670 |
| Weight (kg) | 63.85 ± 9.86 | 66.05 ± 8.96 | 68.97 ± 7.60 | 0.442 |
| BMI (kg/m2) | 24.47 ± 3.48 | 25.97 ± 3.15 | 26.99 ± 3.55 | 0.266 |
| Free fat mass (kg) | 40.55 ± 4.56 | 40.50 ± 4.17 | 42.64 ± 3.41 | 0.419 |
| Body fat mass (kg) | 23.33 ± 6.63 | 25.55 ± 5.60 | 26.35 ± 5.96 | 0.524 |
| Percent body fat (%) | 36.08 ± 5.31 | 38.38 ± 3.91 | 37.80 ± 5.07 | 0.545 |
| Parameters | Groups | Test | ∆% | p (η2) | ||
|---|---|---|---|---|---|---|
| Pre | Post | |||||
| Weight (kg) | FPG | 63.85 ± 9.86 | 63.34 ± 8.79 | −0.80 | G | 0.319 (0.081) |
| OPG | 66.05 ± 8.96 | 65.54 ± 7.22 | −0.77 | T | 0.661 (0.007) | |
| CON | 68.97 ± 7.60 | 69.42 ± 6.64 | 0.65 | G × T | 0.579 (0.040) | |
| BMI (kg/m2) | FPG | 24.47 ± 3.48 | 24.30 ± 3.31 | −0.72 | G | 0.194 (0.114) |
| OPG | 25.97 ± 3.15 | 25.81 ± 2.86 | −0.62 | T | 0.777 (0.003) | |
| CON | 26.99 ± 3.55 | 27.18 ± 3.27 | 0.72 | G × T | 0.600 (0.037) | |
| Free fat mass (kg) | FPG | 40.55 ± 4.56 | 40.84 ± 4.21 | 0.72 | G | 0.461 (0.056) |
| OPG | 40.50 ± 4.17 | 40.67 ± 4.09 | 0.42 | T | 0.546 (0.014) | |
| CON | 42.64 ± 3.41 | 42.49 ± 3.23 | −0.35 | G × T | 0.553 (0.043) | |
| SMM (kg) | FPG | 21.92 ± 2.71 | 22.07 ± 2.46 | 0.68 | G | 0.442 (0.059) |
| OPG | 21.98 ± 2.47 | 22.10 ± 2.43 | 0.55 | T | 0.443 (0.022) | |
| CON | 23.21 ± 2.00 | 23.18 ± 2.02 | −0.13 | G × T | 0.748 (0.021) | |
| Body fat mass (kg) | FPG | 23.33 ± 6.63 | 22.64 ± 6.02 | −2.96 | G | 0.378 (0.070) |
| OPG | 25.55 ± 5.60 | 25.07 ± 4.75 | −1.88 | T | 0.428 (0.023) | |
| CON | 26.35 ± 5.96 | 26.70 ± 5.29 | 1.33 | G × T | 0.429 (0.061) | |
| Percent body fat (%) | FPG | 36.08 ± 5.31 | 35.14 ± 4.99 | −2.61 | G | 0.398 (0.066) |
| OPG | 38.38 ± 3.91 | 37.77 ± 3.72 | −1.59 | T | 0.187 (0.063) | |
| CON | 37.80 ± 5.07 | 38.29 ± 4.60 | 1.30 | G × T | 0.083 (0.169) | |
| WHR | FPG | 0.870 ± 0.043 | 0.866 ± 0.037 | −0.51 | G | 0.947 (0.004) |
| OPG | 0.869 ± 0.059 | 0.867 ± 0.051 | −0.22 | T | 0.815 (0.002) | |
| CON | 0.875 ± 0.083 | 0.876 ± 0.064 | 0.13 | G × T | 0.954 (0.003) | |
| Parameters | Groups | Test | ∆% | p (η2) | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | |||||||
| Rectus abdominis | Tone (Hz) | FPG | 11.68 ± 1.67 | 9.88 ± 0.80 | −15.41 ** | G | 0.301 (0.085) | |
| OPG | 11.02 ± 1.30 | 10.05 ± 0.45 | −8.80 * | T | 0.002 (0.304) | ++ | ||
| CON | 11.08 ± 1.41 | 11.35 ± 1.01 | 2.44 | G × T | 0.006 (0.313) | ++ | ||
| Stiffness (N/m) | FPG | 172.95 ± 10.40 | 157.25 ± 16.55 | −9.08 * | G | 0.340 (0.077) | ||
| OPG | 170.40 ± 15.05 | 162.10 ± 13.29 | −4.87 * | T | 0.009 (0.228) | ++ | ||
| CON | 170.90 ± 10.61 | 172.90 ± 10.62 | 1.17 | G × T | 0.032 (0.225) | + | ||
| External oblique | Tone (Hz) | FPG | 12.50 ± 1.45 | 11.07 ± 0.97 | −11.44 *** | G | 0.474 (0.054) | |
| OPG | 12.41 ± 1.07 | 11.76 ± 1.01 | −5.24 * | T | 0.000 (0.421) | +++ | ||
| CON | 12.22 ± 0.91 | 12.46 ± 0.94 | 1.96 | G × T | 0.000 (0.473) | +++ | ||
| Stiffness (N/m) | FPG | 186.80 ± 16.28 | 167.35 ± 19.05 | −10.41 ** | G | 0.507 (0.049) | ||
| OPG | 186.20 ± 18.65 | 176.10 ± 13.40 | −5.42 * | T | 0.004 (0.275) | ++ | ||
| CON | 183.95 ± 19.02 | 186.50 ± 16.39 | 1.39 | G × T | 0.013 (0.276) | + | ||
| Erector spinae | Tone (Hz) | FPG | 16.34 ± 1.69 | 15.05 ± 1.54 | −7.89 ** | G | 0.687 (0.027) | |
| OPG | 16.57 ± 1.79 | 15.89 ± 1.91 | −4.10 * | T | 0.002 (0.305) | ++ | ||
| CON | 16.10 ± 1.66 | 16.43 ± 1.54 | 2.05 | G × T | 0.001 (0.396) | ++ | ||
| Stiffness (N/m) | FPG | 329.65 ± 57.14 | 297.45 ± 50.71 | −9.77 ** | G | 0.790 (0.017) | ||
| OPG | 333.85 ± 49.02 | 312.45 ± 51.01 | −6.41 * | T | 0.003 (0.289) | ++ | ||
| CON | 323.45 ± 46.59 | 331.75 ± 30.68 | 2.57 | G × T | 0.003 (0.334) | ++ | ||
| Parameters | Groups | Test | ∆% | p (η2) | ||
|---|---|---|---|---|---|---|
| Pre | Post | |||||
| SBP (mmHg) | FPG | 118.60 ± 10.25 | 114.05 ± 10.56 | −3.84 | G | 0.560 (0.042) |
| OPG | 122.85 ± 12.89 | 119.40 ± 13.96 | −2.81 | T | 0.059 (0.126) | |
| CON | 118.70 ± 7.48 | 118.15 ± 6.92 | −0.46 | G × T | 0.514 (0.048) | |
| DBP (mmHg) | FPG | 75.80 ± 9.01 | 74.30 ± 7.97 | −1.98 | G | 0.988 (0.001) |
| OPG | 76.00 ± 11.03 | 74.60 ± 10.60 | −1.84 | T | 0.293 (0.041) | |
| CON | 74.85 ± 5.53 | 74.60 ± 5.91 | −0.33 | G × T | 0.847 (0.012) | |
| MAP (mmHg) | FPG | 90.06 ± 8.89 | 87.57 ± 8.45 | −2.76 | G | 0.889 (0.009) |
| OPG | 91.62 ± 11.25 | 89.52 ± 10.94 | −2.29 | T | 0.123 (0.086) | |
| CON | 89.46 ± 5.84 | 89.12 ± 5.99 | −0.38 | G × T | 0.668 (0.029) | |
| TG (mg/dL) | FPG | 120.20 ± 66.75 | 101.10 ± 62.03 | −15.89 | G | 0.730 (0.023) |
| OPG | 126.60 ± 72.12 | 113.10 ± 68.35 | −10.66 | T | 0.121 (0.087) | |
| CON | 132.00 ± 50.73 | 130.80 ± 43.16 | −0.91 | G × T | 0.575 (0.040) | |
| TC (mg/dL) | FPG | 194.70 ± 22.42 | 185.80 ± 24.52 | −4.57 | G | 0.738 (0.022) |
| OPG | 189.50 ± 56.50 | 183.30 ± 41.20 | −3.27 | T | 0.438 (0.022) | |
| CON | 197.40 ± 23.01 | 194.36 ± 24.14 | −1.54 | G × T | 0.953 (0.004) | |
| HDL-C (mg/dL) | FPG | 58.50 ± 10.28 | 65.70 ± 15.46 | 12.31 | G | 0.183 (0.118) |
| OPG | 52.60 ± 13.48 | 57.30 ± 12.84 | 8.94 | T | 0.066 (0.120) | |
| CON | 53.30 ± 8.25 | 53.60 ± 12.29 | 0.56 | G × T | 0.416 (0.063) | |
| LDL-C (mg/dL) | FPG | 119.96 ± 34.65 | 103.06 ± 25.26 | −14.09 | G | 0.921 (0.006) |
| OPG | 118.28 ± 56.96 | 105.98 ± 35.23 | −10.40 | T | 0.266 (0.046) | |
| CON | 117.94 ± 25.42 | 116.35 ± 60.43 | −1.35 | G × T | 0.779 (0.018) | |
| Glucose (mg/dL) | FPG | 102.20 ± 6.00 | 97.88 ± 5.29 | −4.22 | G | 0.113 (0.149) |
| OPG | 105.72 ± 5.15 | 103.30 ± 8.31 | −2.29 | T | 0.103 (0.095) | |
| CON | 101.74 ± 5.82 | 101.30 ± 5.33 | −0.44 | G × T | 0.545 (0.044) | |
| Parameters | Groups | Test | ∆% | p (η2) | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | |||||||
| HRV | Mean RR (msec) | FPG | 741.65 ± 92.26 | 821.53 ± 84.60 | 10.77 * | G | 0.315 (0.082) | |
| OPG | 798.64 ± 91.62 | 850.04 ± 76.97 | 6.44 | T | 0.024 (0.174) | + | ||
| CON | 837.61 ± 97.36 | 824.07 ± 91.33 | −1.62 | G × T | 0.077 (0.173) | |||
| SDNN (ms) | FPG | 27.23 ± 10.03 | 34.78 ± 9.64 | 27.73 *** | G | 0.541 (0.044) | ||
| OPG | 25.41 ± 8.98 | 30.07 ± 10.94 | 18.34 | T | 0.004 (0.269) | ++ | ||
| CON | 33.21 ± 9.73 | 31.34 ± 9.38 | −5.65 | G × T | 0.005 (0.326) | ++ | ||
| RMSSD (ms) | FPG | 34.58 ± 14.48 | 41.33 ± 11.67 | 19.50 * | G | 0.771 (0.019) | ||
| OPG | 32.04 ± 18.42 | 35.75 ± 16.53 | 11.58 * | T | 0.008 (0.233) | ++ | ||
| CON | 39.20 ± 18.43 | 37.93 ± 15.07 | −3.24 | G × T | 0.017 (0.261) | + | ||
| LF (ms2) | FPG | 197.12 ± 63.57 | 164.33 ± 44.10 | −16.64 | G | 0.549 (0.043) | ||
| OPG | 185.26 ± 32.50 | 166.08 ± 26.18 | −10.35 | T | 0.082 (0.108) | |||
| CON | 192.56 ± 59.25 | 196.86 ± 42.05 | 2.23 | G × T | 0.238 (0.101) | |||
| HF (ms2) | FPG | 191.58 ± 48.35 | 212.52 ± 51.91 | 10.93 | G | 0.936 (0.005) | ||
| OPG | 189.71 ± 50.08 | 201.51 ± 37.92 | 6.22 | T | 0.118 (0.088) | |||
| CON | 196.26 ± 42.32 | 197.56 ± 44.54 | 0.67 | G × T | 0.529 (0.046) | |||
| LF/HF ratio | FPG | 1.05 ± 0.26 | 0.78 ± 0.14 | −25.17 * | G | 0.421 (0.062) | ||
| OPG | 1.02 ± 0.24 | 0.84 ± 0.12 | −18.38 * | T | 0.007 (0.242) | ++ | ||
| CON | 0.98 ± 0.20 | 1.01 ± 0.17 | 3.58 | G × T | 0.041 (0.210) | + | ||
| STAI (score) | FPG | 41.80 ± 8.75 | 33.40 ± 4.74 | −20.10 ** | G | 0.634 (0.033) | ||
| OPG | 39.40 ± 9.58 | 35.50 ± 10.38 | −9.90 * | T | 0.031 (0.162) | + | ||
| CON | 39.20 ± 9.27 | 41.50 ± 7.55 | 5.87 | G × T | 0.020 (0.250) | + | ||
| BDI (score) | FPG | 12.20 ± 4.64 | 8.00 ± 5.50 | −34.43 * | G | 0.376 (0.070) | ||
| OPG | 11.10 ± 5.13 | 9.10 ± 4.61 | −18.02 | T | 0.058 (0.127) | |||
| CON | 11.80 ± 4.92 | 13.00 ± 3.59 | 10.17 | G × T | 0.046 (0.204) | + | ||
| Parameters | Groups | Test | ∆% | p (η2) | |||
|---|---|---|---|---|---|---|---|
| Pre | Post | ||||||
| Dominant grip strength (kg) | FPG | 23.56 ± 3.35 | 25.97 ± 3.93 | 10.23 | G | 0.270 (0.092) | |
| OPG | 26.55 ± 5.50 | 28.88 ± 4.76 | 8.78 | T | 0.079 (0.110) | ||
| CON | 24.96 ± 7.00 | 24.17 ± 5.54 | −3.17 | G × T | 0.138 (0.136) | ||
| Non-dominant grip strength (kg) | FPG | 21.17 ± 4.67 | 23.25 ± 5.53 | 9.83 | G | 0.111 (0.150) | |
| OPG | 26.12 ± 5.16 | 27.79 ± 5.12 | 6.39 | T | 0.309 (0.038) | ||
| CON | 24.46 ± 7.58 | 23.60 ± 4.47 | −3.53 | G × T | 0.386 (0.068) | ||
| Sit-up (number) | FPG | 15.60 ± 6.83 | 17.90 ± 6.66 | 14.74 ** | G | 0.666 (0.030) | |
| OPG | 16.10 ± 7.89 | 17.50 ± 8.28 | 8.70 * | T | 0.001 (0.360) | ++ | |
| CON | 14.30 ± 5.81 | 14.50 ± 4.74 | 1.40 | G × T | 0.051 (0.198) | ||
| Sit-and-Reach (cm) | FPG | 8.92 ± 8.82 | 15.49 ± 9.16 | 73.65 ** | G | 0.683 (0.028) | |
| OPG | 9.40 ± 6.18 | 14.16 ± 8.40 | 50.64 * | T | 0.000 (0.548) | +++ | |
| CON | 8.73 ± 10.20 | 9.35 ± 10.24 | 7.10 | G × T | 0.005 (0.322) | ++ | |
| Right Balance (sec) | FPG | 9.09 ± 8.32 | 18.15 ± 13.14 | 99.78 * | G | 0.249 (0.098) | |
| OPG | 9.79 ± 8.05 | 16.02 ± 13.67 | 63.74 | T | 0.008 (0.235) | ++ | |
| CON | 7.62 ± 5.91 | 7.98 ± 5.75 | 4.71 | G × T | 0.155 (0.129) | ||
| Left Balance (sec) | FPG | 8.66 ± 8.30 | 18.15 ± 15.47 | 109.51 * | G | 0.164 (0.125) | |
| OPG | 9.29 ± 7.06 | 16.57 ± 16.44 | 78.40 | T | 0.014 (0.203) | + | |
| CON | 6.47 ± 5.38 | 6.63 ± 2.37 | 2.39 | G × T | 0.199 (0.113) | ||
| VO2max (ml/kg/min) | FPG | 25.01 ± 5.06 | 27.13 ± 7.22 | 8.48 | G | 0.316 (0.082) | |
| OPG | 23.11 ± 4.46 | 24.18 ± 3.90 | 4.63 | T | 0.338 (0.034) | ||
| CON | 23.48 ± 5.30 | 22.81 ± 3.81 | −2.85 | G × T | 0.422 (0.062) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-Y.; Jung, K.; Jung, W.-S.; Kim, S.-W.; Kim, J.; Lim, K. Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity. Healthcare 2023, 11, 2768. https://doi.org/10.3390/healthcare11202768
Park H-Y, Jung K, Jung W-S, Kim S-W, Kim J, Lim K. Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity. Healthcare. 2023; 11(20):2768. https://doi.org/10.3390/healthcare11202768
Chicago/Turabian StylePark, Hun-Young, Kyounghwa Jung, Won-Sang Jung, Sung-Woo Kim, Jisu Kim, and Kiwon Lim. 2023. "Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity" Healthcare 11, no. 20: 2768. https://doi.org/10.3390/healthcare11202768
APA StylePark, H.-Y., Jung, K., Jung, W.-S., Kim, S.-W., Kim, J., & Lim, K. (2023). Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity. Healthcare, 11(20), 2768. https://doi.org/10.3390/healthcare11202768