
Physical Activity Levels and Predictors during COVID-19 Lockdown among Lebanese Adults: The Impacts of Sociodemographic Factors, Type of Physical Activity and Work Location



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Ethical Considerations
2.4. Statistical Analysis
2.5. Machine Learning Analysis
3. Results
3.1. Description of the Study Sample
3.2. PA Levels and Their Association with Participants’ Characteristics
3.2.1. PA and Sex
3.2.2. PA and Age
3.2.3. PA and Work Location
3.2.4. PA and BMI
3.2.5. PA Level and Type of PA
3.2.6. Multivariate Analysis
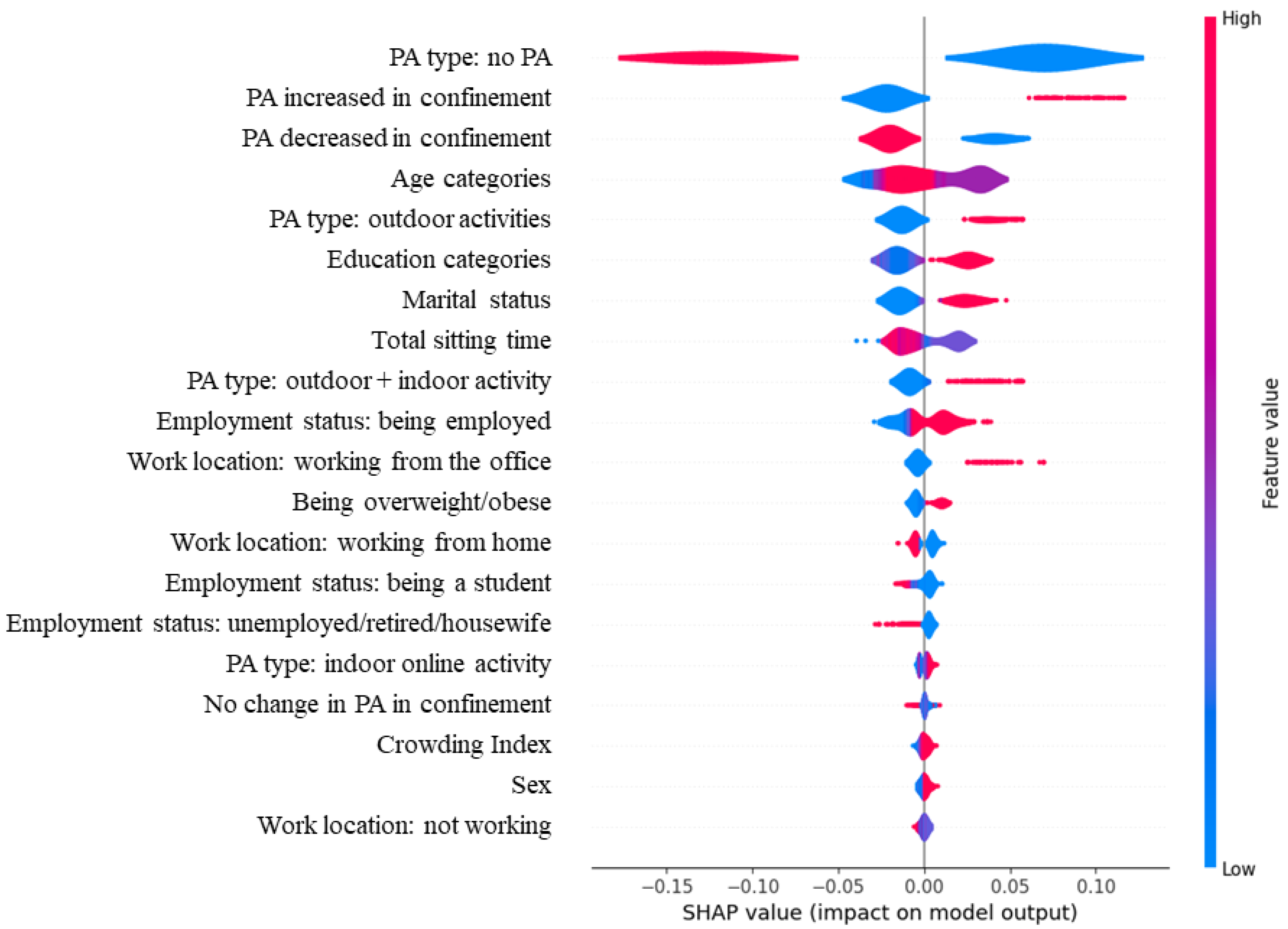
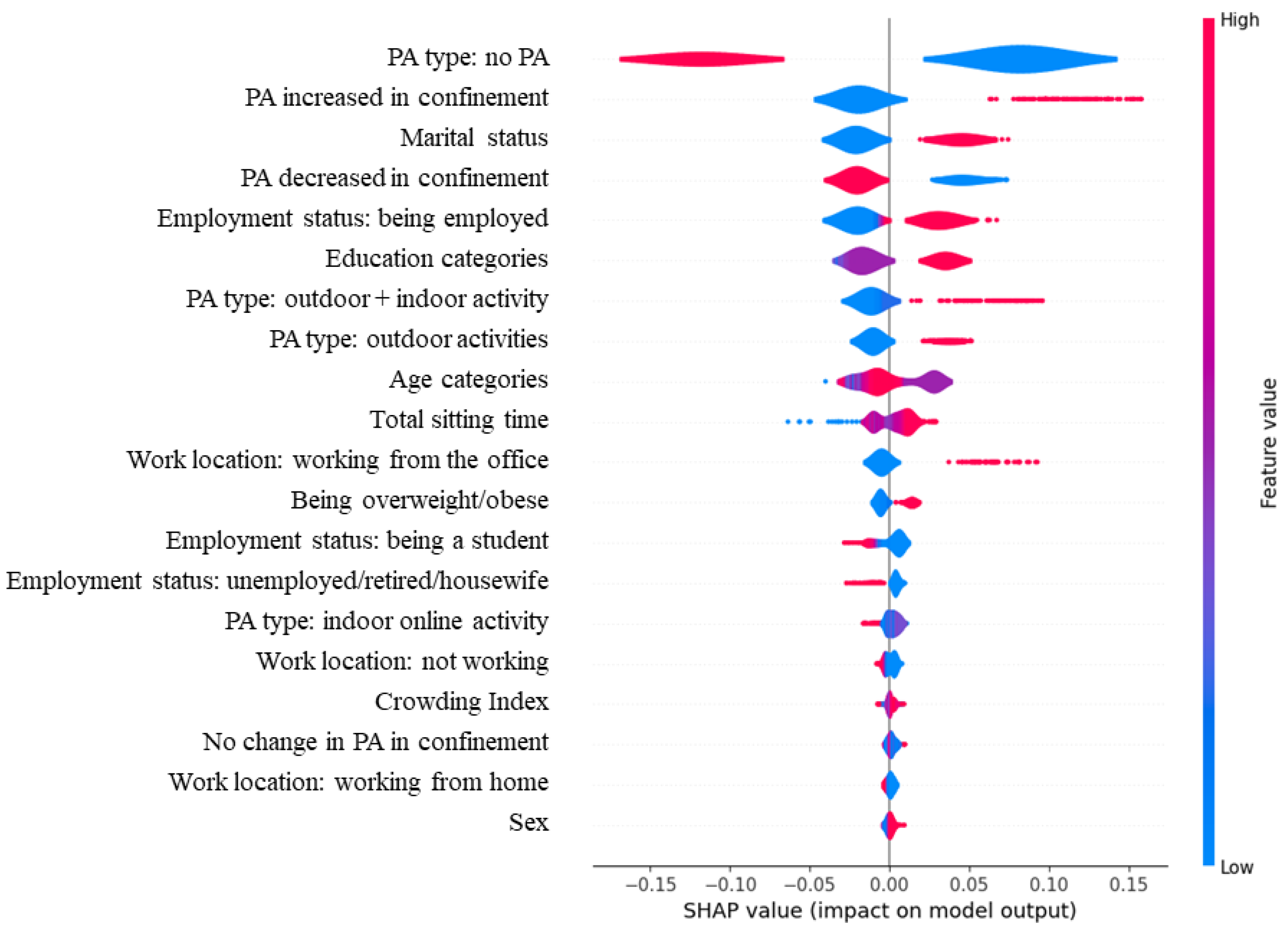
3.3. Analysis Using Machine Learning Algorithms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 12 April 2021).
- Bizri, A.R.; Khachfe, H.H.; Fares, M.Y.; Musharrafieh, U. COVID-19 Pandemic: An Insult over Injury for Lebanon. J. Community Health 2020, 46, 487–493. [Google Scholar] [CrossRef]
- Singh, D.; Mathioudakis, A.G.; Higham, A. Chronic Obstructive Pulmonary Disease and COVID-19: Interrelationships. Curr. Opin. Pulm. Med. 2022, 28, 76–83. [Google Scholar] [CrossRef]
- Bostancı, Ö.; Karaduman, E.; Çolak, Y.; Yılmaz, A.K.; Kabadayı, M.; Bilgiç, S. Respiratory Muscle Strength and Pulmonary Function in Unvaccinated Athletes before and after COVID-19 Infection: A Prospective Cohort Study. Respir. Physiol. Neurobiol. 2023, 308, 103983. [Google Scholar] [CrossRef]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical Activity during COVID-19 Induced Lockdown: Recommendations. J. Occup. Med. Toxicol. 2020, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical Inactivity Is Associated with a Higher Risk for Severe COVID-19 Outcomes: A Study in 48 440 Adult Patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Abate Daga, F.; Agostino, S.; Peretti, S.; Beratto, L. The Impact of Physical Activity Rate on Subjective Well-Being among North-Western Italian Population during COVID-19 Nationwide Lockdown. J. Sports Med. Phys. Fit. 2022, 62, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Srivastav, A.K.; Sharma, N.; Samuel, A.J. Impact of Coronavirus Disease-19 (COVID-19) Lockdown on Physical Activity and Energy Expenditure among Physiotherapy Professionals and Students Using Web-Based Open E-Survey Sent through WhatsApp, Facebook and Instagram Messengers. Clin. Epidemiol. Glob. Health 2021, 9, 78–84. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Zacharakis, E.D. Impact of COVID-19 Lockdown on Physical Activity in a Sample of Greek Adults. Sports 2020, 8, 139. [Google Scholar] [CrossRef]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The Impact of Physical Activity on Psychological Health during COVID-19 Pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Zampelas, A.; Habib-Mourad, C.; Omar Abu Jamous, D.; Ali, H.I.; Al Sabbah, H.; et al. Assessment of Eating Habits and Lifestyle during the Coronavirus 2019 Pandemic in the Middle East and North Africa Region: A Cross-Sectional Study. Br. J. Nutr. 2020, 126, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Al Kitbi, M.; Hasan, H.; Al Hilali, M.; Abbas, N.; Hamadeh, R.; Saif, E.R.; Naja, F. Indirect Health Effects of COVID-19: Unhealthy Lifestyle Behaviors during the Lockdown in the United Arab Emirates. Int. J. Environ. Res. Public Health 2021, 18, 1964. [Google Scholar] [CrossRef] [PubMed]
- Abouzid, M.; El-Sherif, D.M.; Eltewacy, N.K.; Dahman, N.B.H.; Okasha, S.A.; Ghozy, S.; Islam, S.M.S.; EARG Collaborators. Influence of COVID-19 on Lifestyle Behaviors in the Middle East and North Africa Region: A Survey of 5896 Individuals. J. Transl. Med. 2021, 19, 129. [Google Scholar] [CrossRef]
- Kilani, H.A.; Bataineh, M.F.; Al-Nawayseh, A.; Atiyat, K.; Obeid, O.; Abu-Hilal, M.M.; Mansi, T.; Al-Kilani, M.; Al-Kitani, M.; El-Saleh, M.; et al. Healthy Lifestyle Behaviors Are Major Predictors of Mental Wellbeing during COVID-19 Pandemic Confinement: A Study on Adult Arabs in Higher Educational Institutions. PLoS ONE 2020, 15, e0243524. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in Physical Activity and Sedentary Behaviours from before to during the COVID-19 Pandemic Lockdown: A Systematic Review. BMJ Open Sport. Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Abate Daga, F.; Agostino, S.; Peretti, S.; Beratto, L. COVID-19 Nationwide Lockdown and Physical Activity Profiles among North-Western Italian Population Using the International Physical Activity Questionnaire (IPAQ). Sport. Sci. Health 2021, 17, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Zakhour, M.; Bou kheir, M.; Haddad, R.; Al Hachach, M.; Sacre, H.; Salameh, P. Association between Eating Behavior and Quarantine/Confinement Stressors during the Coronavirus Disease 2019 Outbreak. J. Eat. Disord. 2020, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Cheikh Ismail, L.; Hashim, M.; Mohamad, M.N.; Hassan, H.; Ajab, A.; Stojanovska, L.; Jarrar, A.H.; Hasan, H.; Abu Jamous, D.O.; Saleh, S.T.; et al. Dietary Habits and Lifestyle during Coronavirus Pandemic Lockdown: Experience from Lebanon. Front. Nutr. 2021, 8, 606. [Google Scholar] [CrossRef]
- Hammoudi, S.F.; Mreydem, H.W.; Ali, B.T.A.; Saleh, N.O.; Chung, S.; Hallit, S.; Salameh, P. Smartphone Screen Time among University Students in Lebanon and Its Association with Insomnia, Bedtime Procrastination, and Body Mass Index during the COVID-19 Pandemic: A Cross-Sectional Study. Psychiatry Investig. 2021, 18, 871–878. [Google Scholar] [CrossRef]
- Javelle, F.; Laborde, S.; Hosang, T.J.; Metcalfe, A.J.; Zimmer, P. The Importance of Nature Exposure and Physical Activity for Psychological Health and Stress Perception: Evidence from the First Lockdown Period during the Coronavirus Pandemic 2020 in France and Germany. Front. Psychol. 2021, 12, 623946. [Google Scholar] [CrossRef]
- Thayyib, P.V.; Mamilla, R.; Khan, M.; Fatima, H.; Asim, M.; Anwar, I.; Shamsudheen, M.K.; Khan, M.A. State-of-the-Art of Artificial Intelligence and Big Data Analytics Reviews in Five Different Domains: A Bibliometric Summary. Sustainability 2023, 15, 4026. [Google Scholar] [CrossRef]
- Alsareii, S.A.; Awais, M.; Alamri, A.M.; AlAsmari, M.Y.; Irfan, M.; Aslam, N.; Raza, M. Physical Activity Monitoring and Classification Using Machine Learning Techniques. Life 2022, 12, 1103. [Google Scholar] [CrossRef]
- Arvidsson, D.; Fridolfsson, J.; Börjesson, M. Measurement of Physical Activity in Clinical Practice Using Accelerometers. J. Intern. Med. 2019, 286, 137–153. [Google Scholar] [CrossRef]
- The IPAQ Group. Downloadable Questionnaires—International Physical Activity Questionnaire. Available online: https://sites.google.com/site/theipaq/questionnaire_links (accessed on 5 December 2016).
- Helou, K.; El Helou, N.; Mahfouz, M.; Mahfouz, Y.; Salameh, P.; Harmouche-Karaki, M. Validity and Reliability of an Adapted Arabic Version of the Long International Physical Activity Questionnaire. BMC Public. Health 2017, 18, 49. [Google Scholar] [CrossRef]
- The IPAQ Group. IPAQ Scoring Protocol—International Physical Activity Questionnaire. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 17 February 2017).
- Lundberg, S.M.; Lee, S.-I.; A Unified Approach to Interpreting Model Predictions. In Advances in Neural Information Processing Systems; 2017; Volume 30. Available online: https://proceedings.neurips.cc/paper_files/paper/2017/hash/8a20a8621978632d76c43dfd28b67767-Abstract.html (accessed on 16 June 2023).
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.-I. From Local Explanations to Global Understanding with Explainable AI for Trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Ou, C.; Liu, J.; Qian, Y.; Chong, W.; Zhang, X.; Liu, W.; Su, H.; Zhang, N.; Zhang, J.; Duan, C.-Z.; et al. Rupture Risk Assessment for Cerebral Aneurysm Using Interpretable Machine Learning on Multidimensional Data. Front. Neurol. 2020, 11, 570181. [Google Scholar] [CrossRef] [PubMed]
- Barwais, F.A. Physical Activity at Home during the COVID-19 Pandemic in the Two Most-Affected Cities in Saudi Arabia. TOPHJ 2020, 13, 470–476. [Google Scholar] [CrossRef]
- Park, A.H.; Zhong, S.; Yang, H.; Jeong, J.; Lee, C. Impact of COVID-19 on Physical Activity: A Rapid Review. J. Glob. Health 2022, 12, 05003. [Google Scholar] [CrossRef]
- Dunton, G.F.; Wang, S.D.; Do, B.; Courtney, J. Early Effects of the COVID-19 Pandemic on Physical Activity Locations and Behaviors in Adults Living in the United States. Prev. Med. Rep. 2020, 20, 101241. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, Eating Behavior and Physical Activity during COVID-19 Lockdown: A Study of UK Adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention How to Be Physically Active While Social Distancing|Physical Activity|CDC. Available online: https://www.cdc.gov/physicalactivity/how-to-be-physically-active-while-social-distancing.html (accessed on 19 April 2021).
- World Health Organization. Stay Physically Active during Self-Quarantine. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/publications-and-technical-guidance/noncommunicable-diseases/stay-physically-active-during-self-quarantine (accessed on 20 April 2021).
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of Working from Home with Occupational Physical Activity and Sedentary Behavior under the COVID-19 Pandemic. J. Occup. Health 2021, 63, e12212. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too Much Sitting—A Health Hazard. Diabetes Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Pears, M.; Kola-Palmer, S.; De Azevedo, L.B. The Impact of Sitting Time and Physical Activity on Mental Health during COVID-19 Lockdown. Sport. Sci. Health 2021, 18, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Rüth, M.; Kaspar, K. Educational and Social Exergaming: A Perspective on Physical, Social, and Educational Benefits and Pitfalls of Exergaming at Home during the COVID-19 Pandemic and Afterwards. Front. Psychol. 2021, 12, 644036. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample (n = 795) | Men (n = 218) | Women (n = 577) | p-Value * | |
|---|---|---|---|---|
| Age (mean ± SD) | 33.13 ± 14.39 | 33.24 ± 16.0 | 33.07 ± 13.71 | 0.891 † |
| Age n (%) | 0.096 * | |||
| <23 years | 302 (38.0) | 95 (43.6) | 207 (35.9) | |
| 24–39 years | 241 (30.3) | 56 (25.7) | 185 (32.1) | |
| ≥40 years | 252 (31.7) | 67 (30.7) | 185 (32.1) | |
| Crowding index n (%) | 0.563 * | |||
| <1 | 461 (58.0) | 130 (59.6) | 331 (57.4) | |
| ≥1 | 334 (42.0) | 88 (40.4) | 246 (42.6) | |
| Marital status n (%) | 0.727 * | |||
| Single | 489 (61.5) | 138 (63.3) | 351 (60.8) | |
| Engaged/Married | 279 (35.1) | 74 (33.9) | 205 (35.5) | |
| Divorced/Widowed | 27 (3.4) | 6 (2.8) | 21 (3.6) | |
| Education n (%) | 0.237 * | |||
| High school or less | 248 (31.2) | 77 (35.3) | 171 (29.6) | |
| Bachelor | 247 (31.1) | 60 (27.5) | 187 (32.4) | |
| Master’s degree or above | 300 (37.7) | 81 (37.2) | 219 (38.0) | |
| BMI (kg/m2) (n = 793) n (%) | <0.001 * | |||
| <18.5 | 62 (7.8) | 9 (4.1) | 53 (9.2) | |
| 18.5–24.9 | 462 (58.1) | 95 (43.8) | 367 (63.7) | |
| 25–29.9 | 208 (26.2) | 91 (41.9) | 117 (20.3) | |
| ≥30 | 61 (7.7) | 22 (10.1) | 39 (6.8) | |
| Employment category n (%) | 0.001 * | |||
| Employed | 370 (46.5) | 108 (49.5) | 262 (45.4) | |
| Student | 268 (33.7) | 85 (39.0) | 183 (31.7) | |
| Unemployed/Retired/Housewife | 157 (19.7) | 25 (11.5) | 132 (22.9) | |
| Job location during lockdown n (%) | 0.006 * | |||
| Home | 360 (45.3) | 94 (43.1) | 266 (46.1) | |
| Office | 74 (9.3) | 32 (14.7) | 42 (7.3) | |
| Student/Unemployed | 361 (45.4) | 92 (42.2) | 269 (46.6) | |
| Auto-declared PA change during lockdown n (%) | 0.405 * | |||
| Did not change | 130 (16.4) | 38 (17.4) | 92 (15.9) | |
| Decreased | 537 (67.5) | 151 (69.3) | 386 (66.9) | |
| Increased | 128 (16.1) | 29 (13.3) | 99 (17.2) | |
| Type of PA during lockdown n (%) | 0.542 * | |||
| At-home workouts | 193 (24.3) | 48 (22.0) | 145 (25.1) | |
| Outdoor activities (walking, jogging, hiking) | 191 (24.0) | 51 (23.4) | 140 (24.3) | |
| At-home and outdoor activities | 139 (17.5) | 36 (16.5) | 103 (17.9) | |
| No PA | 272 (34.2) | 83 (38.1) | 189 (32.8) |
| Home (n = 360) | Office (n = 74) | Student/Unemployed (n = 361) | p-Value | |
|---|---|---|---|---|
| Total PA level n (%) | <0.001 | |||
| <600 MET·min/week | 131 (36.4) | 10 (13.5) | 147 (40.7) | |
| ≥600 MET·min/week | 229 (63.6) | 64 (86.5) | 214 (59.3) | |
| Job-related PA n (%) | <0.001 | |||
| <600 MET·min/week | 327 (90.8) | 29 (39.2) | 354 (98.1) | |
| ≥600 MET·min/week | 33 (9.2) | 45 (60.8) | 7 (1.9) | |
| Transportation-related PA n (%) | 0.093 | |||
| <600 MET·min/week | 322 (89.4) | 64 (86.5) | 303 (83.9) | |
| ≥600 MET·min/week | 38 (10.6) | 10 (13.5) | 58 (16.1) | |
| Housework-related PA n (%) | 0.936 | |||
| <600 MET·min/week | 234 (65.0) | 48 (64.9) | 239 (66.2) | |
| ≥600 MET·min/week | 126 (35.0) | 26 (35.1) | 122 (33.8) | |
| Leisure-related PA n (%) | 0.061 | |||
| <600 MET·min/week | 237 (65.8) | 42 (56.8) | 254 (70.4) | |
| ≥600 MET·min/week | 123 (34.2) | 32 (43.2) | 107 (29.6) | |
| Walking n (%) | <0.001 | |||
| <600 MET·min/week | 259 (71.9) | 32 (43.2) | 257 (71.2) | |
| ≥600 MET·min/week | 101 (28.1) | 42 (56.8) | 104 (28.8) | |
| Moderate PA n (%) | <0.001 | |||
| <600 MET·min/week | 256 (71.1) | 36 (48.6) | 273 (75.6) | |
| ≥600 MET·min/week | 104 (28.9) | 38 (51.4) | 88 (24.4) | |
| Vigorous PA n (%) | 0.093 | |||
| <600 MET·min/week | 225 (62.5) | 38 (51.4) | 234 (64.8) | |
| ≥600 MET·min/week | 135 (37.5) | 36 (48.6) | 127 (35.2) | |
| Sitting time (hours/day) | <0.001 | |||
| Tertile 1 = ≤6.29 h | 101 (29.7) | 35 (52.2) | 109 (33.7) | |
| Tertile 2 = 6.29–10 h | 127 (37.4) | 27 (40.3) | 107 (33.1) | |
| Tertile 3 = >10 h | 112 (32.9) | 5 (7.5) | 107 (33.1) |
| ≥600 vs. <600 MET·min/week ORs a (95% CI) | |
|---|---|
| Total PA | |
| Age 23–40 vs. <23 y | 1.220 (0.847–1.756) |
| Age ≥ 40 vs. <23 y | 3.033 † (2.002–4.593) |
| Women vs. Men | 1.078 (0.762–1.527) |
| Office vs. Home | 3.688 † (1.802–7.547) |
| Job-related PA | |
| Age 23–40 vs. <23 y | 5.252 † (2.099–13.138) |
| Age ≥ 40 vs. <23 y | 3.977 † (1.531–10.332) |
| Women vs. Men | 0.853 (0.460–1.581) |
| Office vs. Home | 13.445 † (7.269–24.865) |
| Transportation-related PA | |
| Age 23–40 vs. <23 y | 0.983(0.552–1.752) |
| Age ≥ 40 vs. <23 y | 2.430 † (1.423–4.149) |
| Women vs. Men | 0.691 (0.433–1.103) |
| Office vs. Home | 1.223 (0.568–2.632) |
| Housework-related PA | |
| Age 23–40 vs. <23 y | 0.923 (0.624–1.365) |
| Age ≥ 40 vs. <23 y | 1.928 † (1.305–2.848) |
| Women vs. Men | 1.745 (1.215–2.505) |
| Office vs. Home | 1.085 (0.630–1.868) |
| Leisure-related PA | |
| Age 23–40 vs. <23 y | 1.040 (0.704–1.538) |
| Age ≥ 40 vs. <23 y | 1.798 * (1.209–2.675) |
| Women vs. Men | 0.783 (0.555–1.105) |
| Office vs. Home | 1.417 (0.841–2.390) |
| Walking | |
| Age 23–40 vs. <23 y | 1.591 * (1.057–2.395) |
| Age ≥ 40 vs. <23 y | 2.733 † (1.800–4.149) |
| Women vs. Men | 0.943 (0.657–1.355) |
| Office vs. Home | 3.236 † (1.904–5.500) |
| Moderate PA | |
| Age 23–40 vs. <23 y | 1.107 (0.738–1.660) |
| Age ≥ 40 vs. <23 y | 1.424 (0.941–2.154) |
| Women vs. Men | 0.835 (0.585–1.193) |
| Office vs. Home | 2.452 † (1.457–4.126) |
| Vigorous PA | |
| Age 23–40 vs.<23 y | 1.235 (0.843–1.809) |
| Age ≥ 40 vs.<23 y | 2.470 † (1.672–3.649) |
| Women vs. Men | 1.286 (0.909–1.820) |
| Office vs. Home | 1.592 (0.945–2.681) |
| Sitting time | Tertile 3 vs. Tertile 1 |
| Age 23–40 vs.<23 y | 0.615 (0.376–1.007) |
| Age ≥ 40 vs.<23 y | 0.220 † (0.132–0.367) |
| Women vs. Men | 0.612 * (0.388–0.967) |
| Office vs. Home | 0.120 † (0.044–0.327) |
| Sitting time | Tertile 2 vs. Tertile 1 |
| Age 23–40 vs.<23 y | 0.701 (0.434–1.134) |
| Age ≥ 40 vs.<23 y | 0.334 † (0.206–0.541) |
| Women vs. Men | 0.570 * (0.371–0.877) |
| Office vs. Home | 0.564 (0.310–1.024) |
| Accuracy | Precision | Recall | F1-Score | |
|---|---|---|---|---|
| Train set | ||||
| Random Forest | 0.74 | 0.82 | 0.74 | 0.76 |
| XGBoost | 0.73 | 0.76 | 0.73 | 0.74 |
| SVM | 0.76 | 0.79 | 0.76 | 0.77 |
| Neural Network | 0.76 | 0.76 | 0.76 | 0.75 |
| Test set | ||||
| Random Forest | 0.75 | 0.82 | 0.75 | 0.77 |
| XGBoost | 0.75 | 0.76 | 0.75 | 0.76 |
| SVM | 0.68 | 0.69 | 0.68 | 0.69 |
| Neural Network | 0.71 | 0.71 | 0.71 | 0.70 |
| Accuracy | Precision | Recall | F1-Score | |
|---|---|---|---|---|
| Train set | ||||
| Random Forest | 0.74 | 0.93 | 0.73 | 0.82 |
| XGBoost | 0.73 | 0.86 | 0.75 | 0.80 |
| SVM | 0.75 | 0.85 | 0.78 | 0.81 |
| Neural Network | 0.76 | 0.78 | 0.90 | 0.83 |
| Test set | ||||
| Random Forest | 0.75 | 0.92 | 0.76 | 0.83 |
| XGBoost | 0.75 | 0.84 | 0.81 | 0.82 |
| SVM | 0.68 | 0.78 | 0.74 | 0.76 |
| Neural Network | 0.71 | 0.72 | 0.84 | 0.77 |
| Accuracy | Precision | Recall | F1-Score | |
|---|---|---|---|---|
| Train set | ||||
| Random Forest | 0.76 | 0.77 | 0.77 | 0.76 |
| XGBoost | 0.73 | 0.73 | 0.73 | 0.73 |
| SVM | 0.778 | 0.78 | 0.78 | 0.77 |
| Neural Network | 0.73 | 0.72 | 0.73 | 0.70 |
| Test set | ||||
| Random Forest | 0.76 | 0.76 | 0.76 | 0.76 |
| XGBoost | 0.67 | 0.67 | 0.67 | 0.67 |
| SVM | 0.69 | 0.69 | 0.69 | 0.69 |
| Neural Network | 0.65 | 0.64 | 0.65 | 0.62 |
| Accuracy | Precision | Recall | F1-Score | |
|---|---|---|---|---|
| Train set | ||||
| Random Forest | 0.76 | 0.76 | 0.81 | 0.81 |
| XGBoost | 0.73 | 0.76 | 0.82 | 0.79 |
| SVM | 0.74 | 0.82 | 0.78 | 0.80 |
| Neural Network | 0.73 | 0.73 | 0.92 | 0.81 |
| Test set | ||||
| Random Forest | 0.76 | 0.81 | 0.80 | 0.80 |
| XGBoost | 0.67 | 0.68 | 0.74 | 0.71 |
| SVM | 0.66 | 0.74 | 0.74 | 0.74 |
| Neural Network | 0.65 | 0.65 | 0.86 | 0.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harmouche-Karaki, M.; Mahfouz, M.; Salameh, P.; El Helou, N. Physical Activity Levels and Predictors during COVID-19 Lockdown among Lebanese Adults: The Impacts of Sociodemographic Factors, Type of Physical Activity and Work Location. Healthcare 2023, 11, 2080. https://doi.org/10.3390/healthcare11142080
Harmouche-Karaki M, Mahfouz M, Salameh P, El Helou N. Physical Activity Levels and Predictors during COVID-19 Lockdown among Lebanese Adults: The Impacts of Sociodemographic Factors, Type of Physical Activity and Work Location. Healthcare. 2023; 11(14):2080. https://doi.org/10.3390/healthcare11142080
Chicago/Turabian StyleHarmouche-Karaki, Mireille, Maya Mahfouz, Pascale Salameh, and Nour El Helou. 2023. "Physical Activity Levels and Predictors during COVID-19 Lockdown among Lebanese Adults: The Impacts of Sociodemographic Factors, Type of Physical Activity and Work Location" Healthcare 11, no. 14: 2080. https://doi.org/10.3390/healthcare11142080
APA StyleHarmouche-Karaki, M., Mahfouz, M., Salameh, P., & El Helou, N. (2023). Physical Activity Levels and Predictors during COVID-19 Lockdown among Lebanese Adults: The Impacts of Sociodemographic Factors, Type of Physical Activity and Work Location. Healthcare, 11(14), 2080. https://doi.org/10.3390/healthcare11142080