
Medical Students’ and Radiology Technician Trainees’ eHealth Literacy and Hygiene Awareness—Asynchronous and Synchronous Digital Hand Hygiene Training in a Single-Center Trial

 ,
,  , and
, and
Abstract
1. Introduction
- Carrying disinfectant on us.
- Wearing mouth-nose protection (MNP).
- Using our mobile phones as sources of information and digital identification tools.
- Analytical skills:
- ○ Information literacy (dealing with information).
- ○ Media literacy (handling new media).
- ○ Traditional literacy (education level, reading, spelling and everyday math skills).
- Context-specific skills:
- ○ General health literacy (biopsychosocial understanding of health).
- ○ Computer literacy (digital competence).
- ○ Use of scientific information sources (ability to understand, evaluate and interpret scientific findings).
2. Materials and Methods
2.1. Questionnaire
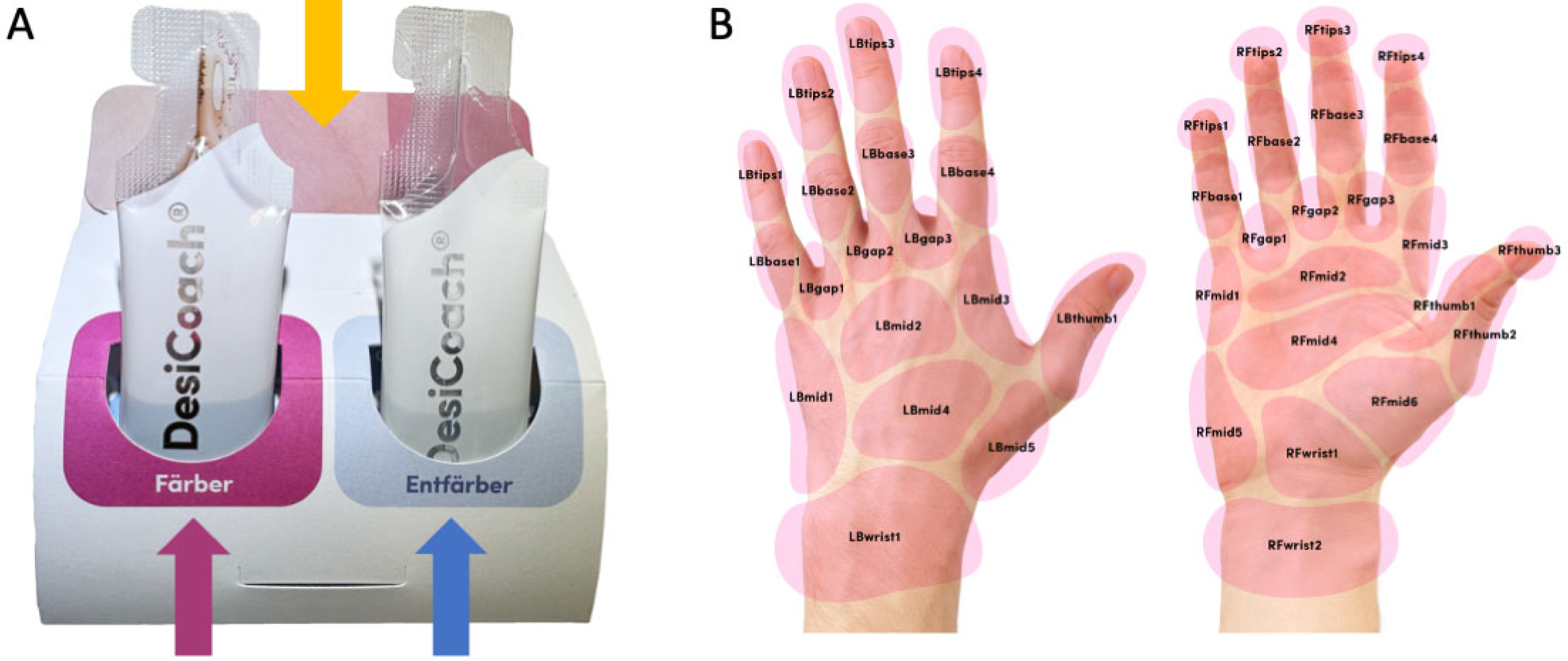
2.2. DesiCoach 2Go (Cohort A)
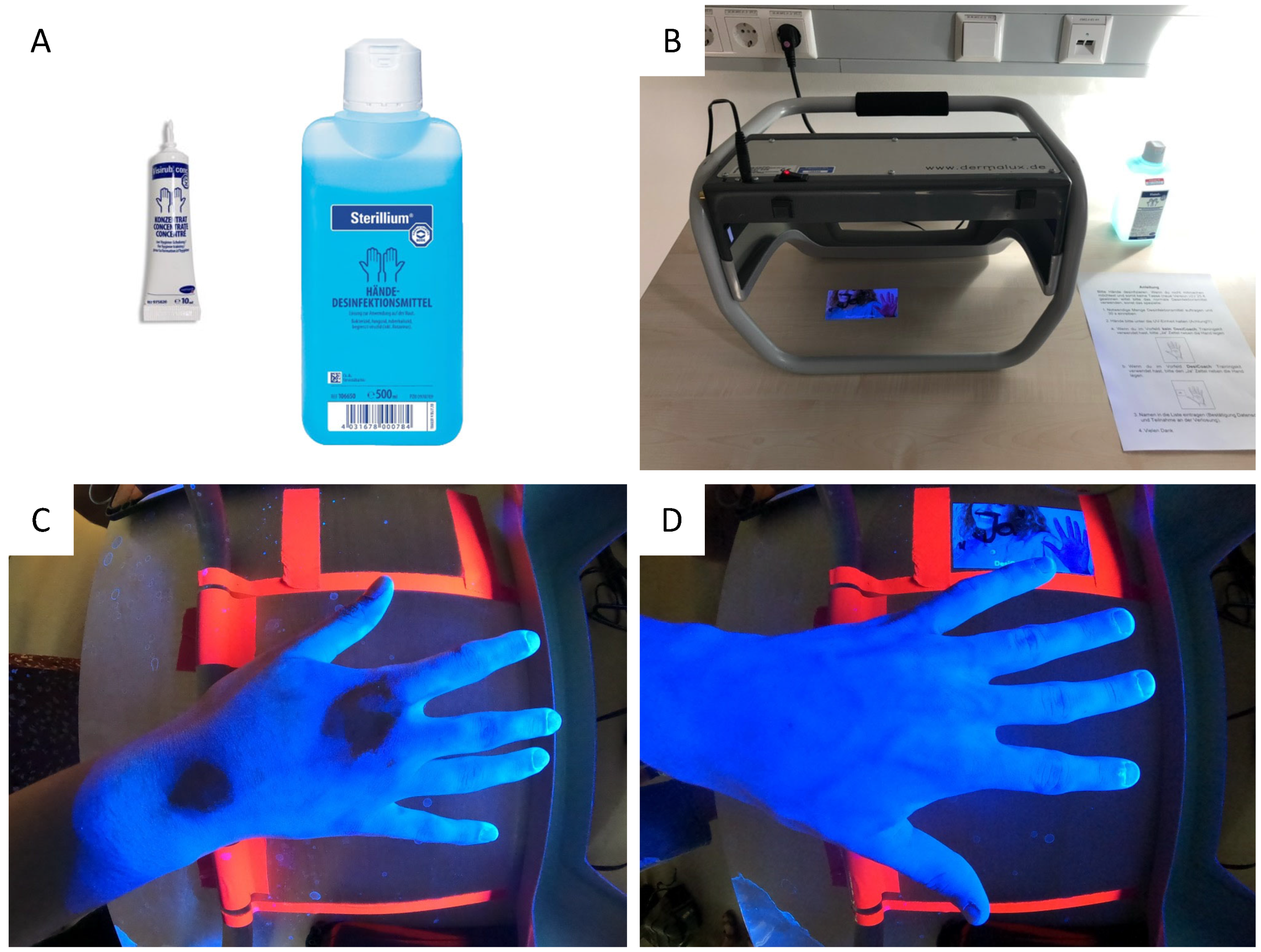
2.3. Visirub (Cohort B1 and B2)
2.4. Statistics
3. Results
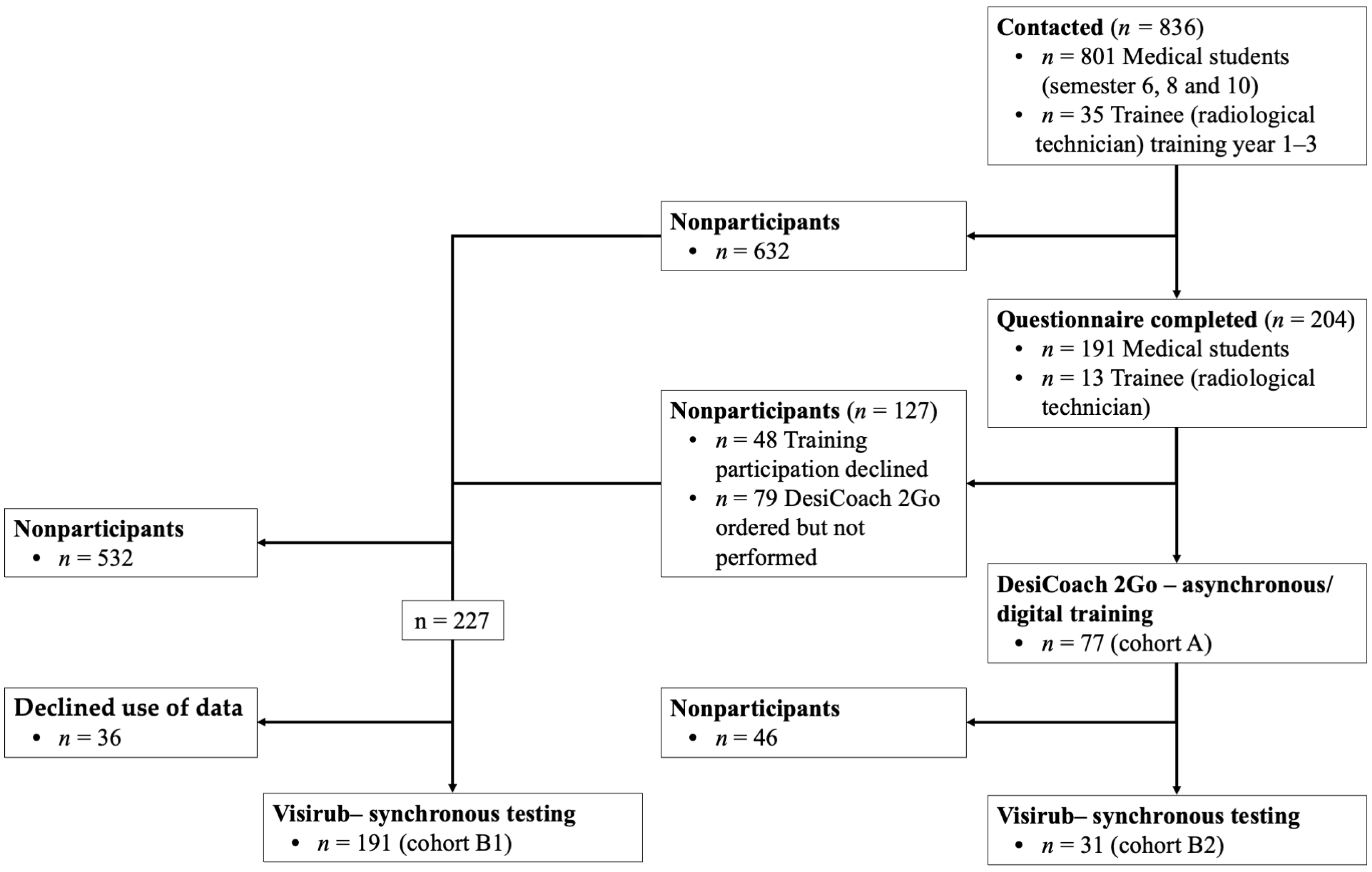
3.1. Survey and Participant
3.2. eHealth Literacy
3.3. Hygiene Awareness and Hand Hygiene
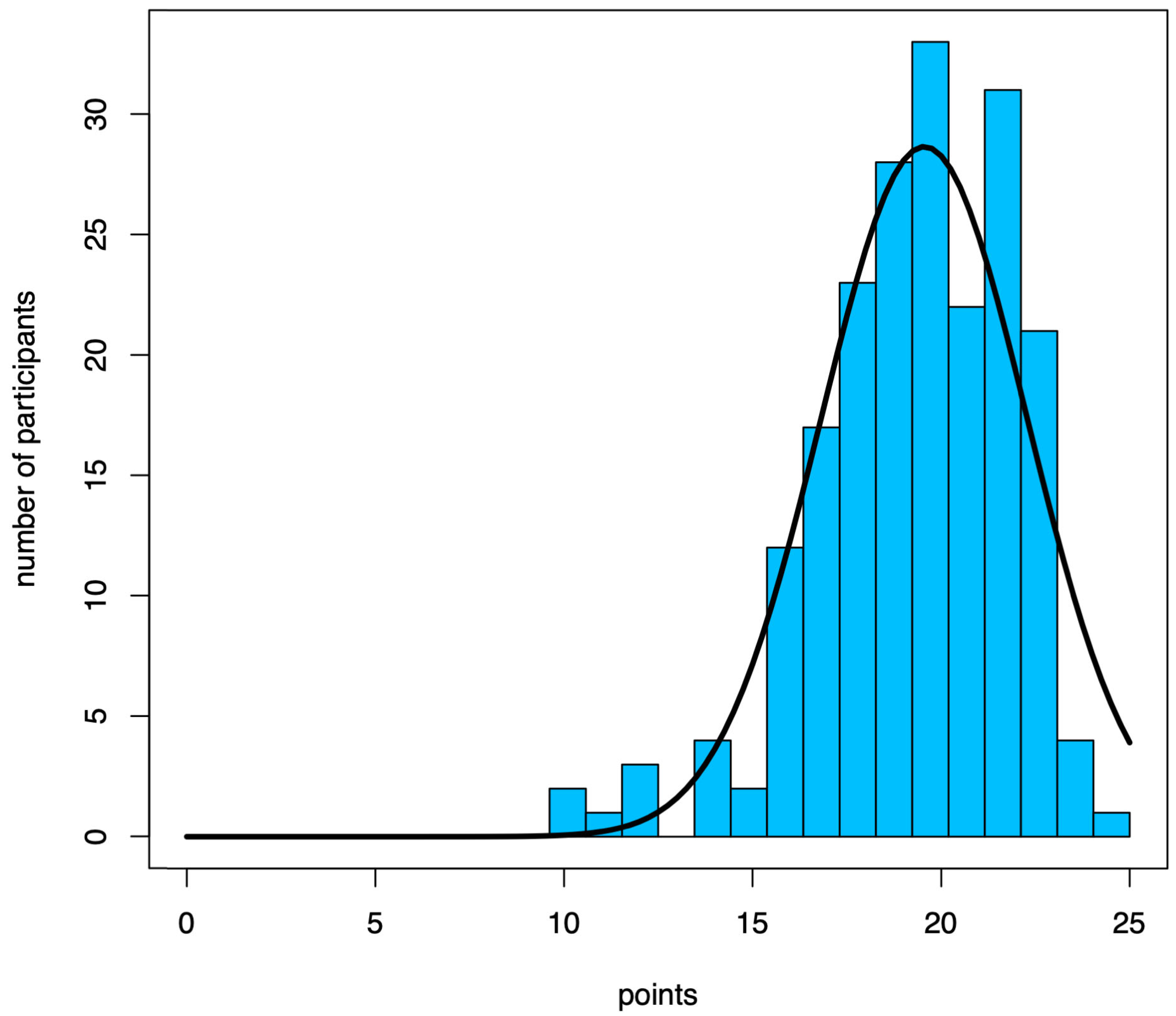
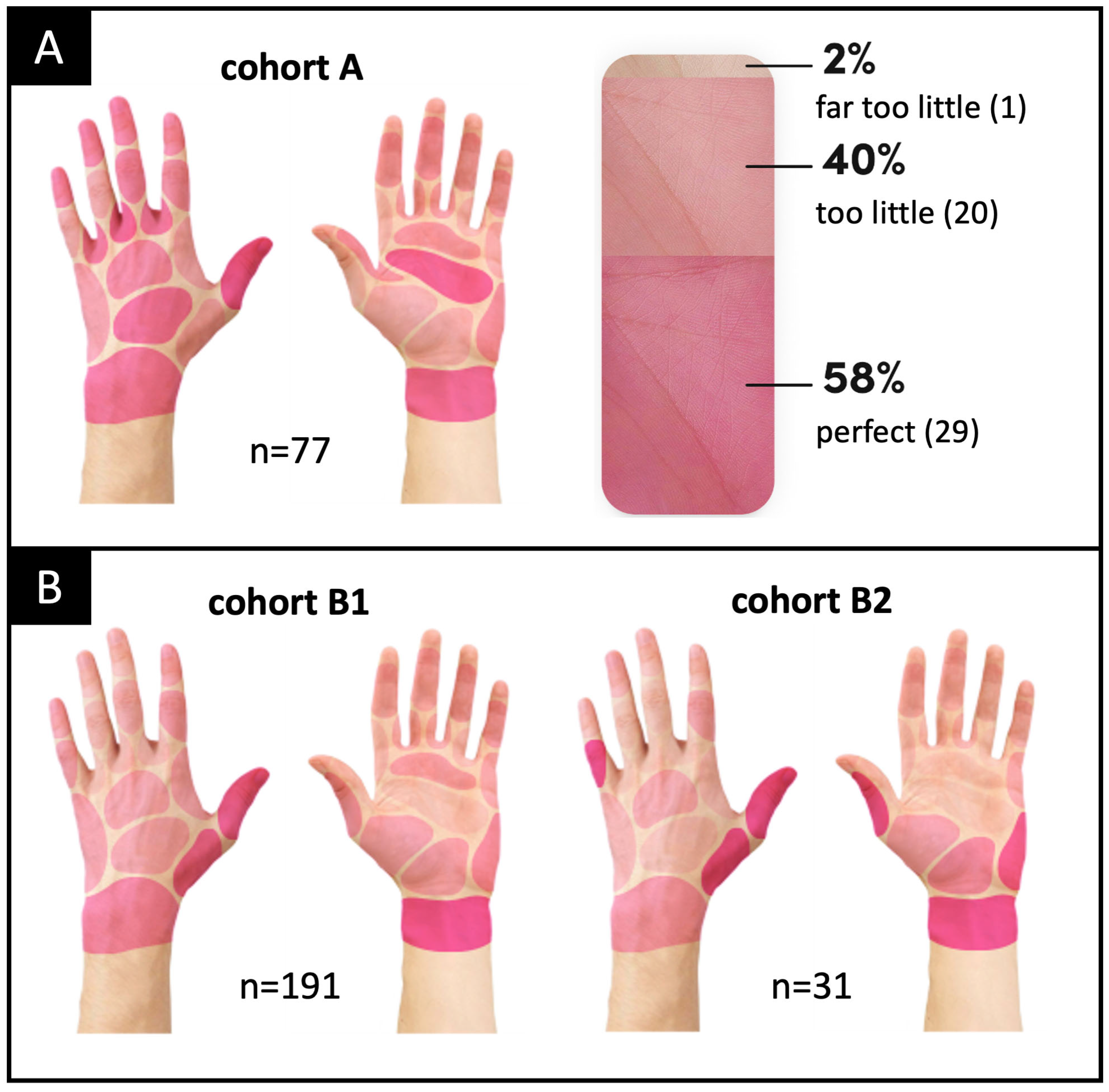
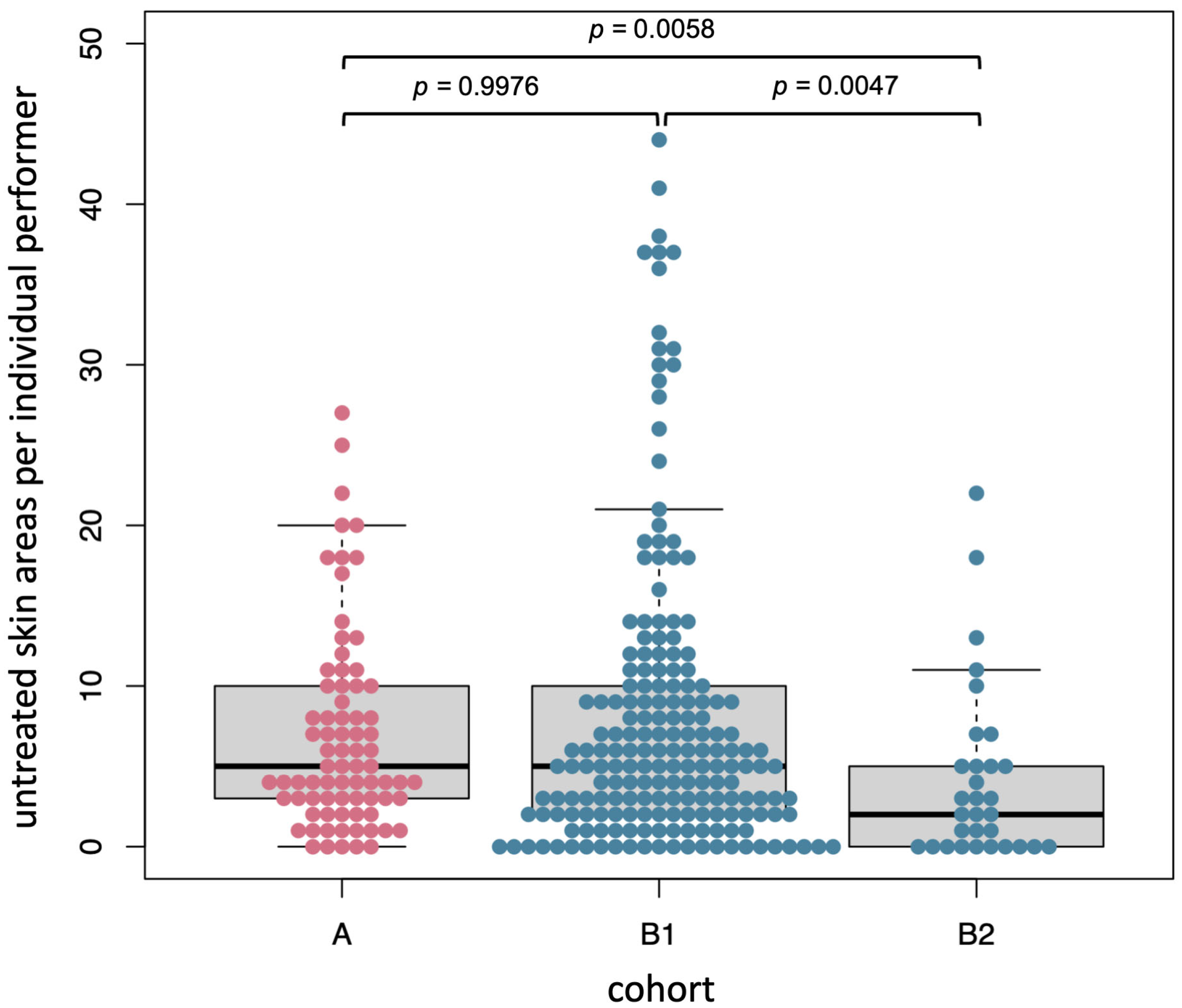
3.4. Hand Disinfection (Including Asynchronous Training)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kilgore, M.L.; Ghosh, K.; Beavers, C.M.; Wong, D.Y.; Hymel, P.A., Jr.; Brossette, S.E. The costs of nosocomial infections. Med. Care 2008, 46, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, W.R. Selected Aspects of the Socioeconomic Impact of Nosocomial Infections: Morbidity, Mortality, Cost, and Prevention. Infect. Control Hosp. Epidemiol. 2015, 17, 552–557. [Google Scholar] [CrossRef]
- Burke, J.P. Infection control—A problem for patient safety. N. Engl. J. Med. 2003, 348, 651–656. [Google Scholar] [CrossRef]
- KRINKO. Personnel and organizational requirements for the prevention of nosocomial infections: Recommendations from the Commission for Hospital Hygiene and Infection Prevention. Bundesgesundheitsblatt Gesundh. Gesundh. 2009, 52, 951–962. [Google Scholar]
- Morii, D.; Miura, A.; Komori, M. The impact of television on-air time on hand hygiene compliance behaviors during COVID-19 outbreak. Am. J. Infect. Control 2023, S0196-6553(23)00102-5. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19). Situation Report—191. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200729-covid-19-sitrep-191.pdf?sfvrsn=2c327e9e_2 (accessed on 12 April 2023).
- Covino, M.; De Matteis, G.; Santoro, M.; Sabia, L.; Simeoni, B.; Candelli, M.; Ojetti, V.; Franceschi, F. Clinical characteristics and prognostic factors in COVID-19 patients aged ≥80 years. Geriatr. Gerontol. Int. 2020, 20, 704–708. [Google Scholar] [CrossRef]
- Fiore, V.; Beretta, R.; De Vito, A.; Barac, A.; Maida, I.; Joeseph Kelvin, D.D.; Piu, C.; Lai, V.; Madeddu, G.; Rubino, S.; et al. Emerging Clinical Features of COVID-19 Related Pancreatitis: Case Reports and Review of the Literature. Front. Med. 2021, 8, 779118. [Google Scholar] [CrossRef]
- Niu, S.; Tian, S.; Lou, J.; Kang, X.; Zhang, L.; Lian, H.; Zhang, J. Clinical characteristics of older patients infected with COVID-19: A descriptive study. Arch. Gerontol. Geriatr. 2020, 89, 104058. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Fois, S.S.; Zinellu, E.; Zinellu, A.; Merella, M.; Pau, M.C.; Carru, C.; Fois, A.G.; Pirina, P. Comparison of Clinical Features, Complete Blood Count Parameters, and Outcomes between Two Distinct Waves of COVID-19: A Monocentric Report from Italy. Healthcare 2022, 10, 2427. [Google Scholar] [CrossRef]
- Rodriguez-Guerra, M.; Jadhav, P.; Vittorio, T.J. Current treatment in COVID-19 disease: A rapid review. Drugs Context 2021, 10, 2020-10-3. [Google Scholar] [CrossRef]
- Fiore, V.; De Vito, A.; Fanelli, C.; Geremia, N.; Princic, E.; Nivoli, A.; Maida, I.; Lorettu, L.; Madeddu, G.; Babudieri, S. Mood Reactive Disorders among COVID-19 Inpatients: Experience from a Monocentric Cohort. Med. Princ. Pract. 2021, 30, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Danet Danet, A. Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Med. Clin. 2021, 156, 449–458. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Depression and anxiety during COVID-19. Lancet 2022, 399, 518. [Google Scholar] [CrossRef] [PubMed]
- Macaraan, W.E.R. The COVID-19 pandemic and its concomitant benefits: Improved hygiene habits. J. Public Health 2022, 44, e407–e408. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Loffler, H.; Gastmeier, P. Hand hygiene for the prevention of nosocomial infections. Dtsch. Arztebl. Int. 2009, 106, 649–655. [Google Scholar] [CrossRef]
- Almalki, M.; Giannicchi, A. Health Apps for Combating COVID-19: Descriptive Review and Taxonomy. JMIR Mhealth Uhealth 2021, 9, e24322. [Google Scholar] [CrossRef]
- Hemmer, C.J.; Hufert, F.; Siewert, S.; Reisinger, E. Protection from COVID-19: The Efficacy of Face Masks. Dtsch. Ärztebl. Int. 2021, 118, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Olanrewaju, A.; AbdulAziz, A.; Preece, C.N.; Shobowale, K. Evaluation of measures to prevent the spread of COVID-19 on the construction sites. Clean. Eng. Technol. 2021, 5, 100277. [Google Scholar] [CrossRef] [PubMed]
- Mojtahedzadeh, N.; Rohwer, E.; Lengen, J.; Harth, V.; Mache, S. Health-promoting work design for telework in the context of the COVID-19 pandemic. Zent. Arb. Arb. Erg. 2021, 71, 69–74. [Google Scholar]
- Eng, T.R. The eHealth Landscape: A Terrain Map of Emerging Information and Communication Technologies in Health and Heath Care; Robert Wood Johnson Foundation: Princeton, NJ, USA, 2001. [Google Scholar]
- Jadad, A.; Oh, H.; Rizo, C.; Enkin, M.; Powell, J.; Pagliari, C. What Is eHealth (3): A Systematic Review of Published Definitions. J. Med. Internet Res. 2005, 7, e1. [Google Scholar]
- Norman, C.D.; Skinner, H.A. eHealth Literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef]
- Kotecha, S.; Sanghera, R. A medical student’s perspective on the impact of the COVID-19 pandemic in altering student and trainee perceptions of a ‘good’ doctor. Med. Teach. 2023, 45, 445–446. [Google Scholar] [CrossRef]
- Sadiku, M.N.O.; Chukwu, U.C.; Ajayi-Majebi, A.; Musa, S.M. Digital Natives in Healthcare. Int. J. Trend Sci. Res. Dev. 2022, 6, 939–945. [Google Scholar]
- Lee, J.; Lee, E.H.; Chae, D. eHealth Literacy Instruments: Systematic Review of Measurement Properties. J. Med. Internet Res. 2021, 23, e30644. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines Approved by the Guidelines Review Committee. In WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Marsall, M.; Engelmann, G.; Skoda, E.M.; Teufel, M.; Bauerle, A. Measuring Electronic Health Literacy: Development, Validation, and Test of Measurement Invariance of a Revised German Version of the eHealth Literacy Scale. J. Med. Internet Res. 2022, 24, e28252. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef]
- World Health Organization. Hand Hygiene Knowledge Questionnaire for Health-Care Workers. Patient Safety, a World Alliance for Safer Health Care, Save Lives, Cleans Your Hands. A Questionnaire Developed by Infection Control Programme; Hôpitaux Universitaires de Genève English Version; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1992; 430p. [Google Scholar]
- Do, B.N.; Tran, T.V.; Phan, D.T.; Nguyen, H.C.; Nguyen, T.T.P.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Trinh, M.V.; Do, T.V.; et al. Health Literacy, eHealth Literacy, Adherence to Infection Prevention and Control Procedures, Lifestyle Changes, and Suspected COVID-19 Symptoms Among Health Care Workers During Lockdown: Online Survey. J. Med. Internet Res. 2020, 22, e22894. [Google Scholar] [CrossRef]
- Paramio Pérez, G.; Almagro, B.J.; Hernando Gómez, Á.; Aguaded Gómez, J.I. Validación de la escala eHealth Literacy (eHEALS) en población universitaria española. Rev. Esp. Salud Públ. 2015, 89, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Mitsutake, S.; Shibata, A.; Ishii, K.; Okazaki, K.; Oka, K. Developing Japanese version of the eHealth Literacy Scale (eHEALS). Nihon Koshu Eisei Zasshi 2011, 58, 361–371. [Google Scholar]
- Sudbury-Riley, L.; FitzPatrick, M.; Schulz, P.J. Exploring the Measurement Properties of the eHealth Literacy Scale (eHEALS) Among Baby Boomers: A Multinational Test of Measurement Invariance. J. Med. Internet Res. 2017, 19, e53. [Google Scholar] [CrossRef]
- Shiferaw, K.B.; Mehari, E.A. Internet use and eHealth literacy among health-care professionals in a resource limited setting: A cross-sectional survey. Adv. Med. Educ. Pract. 2019, 10, 563–570. [Google Scholar] [CrossRef]
- Holt, K.A.; Overgaard, D.; Engel, L.V.; Kayser, L. Health literacy, digital literacy and eHealth literacy in Danish nursing students at entry and graduate level: A cross sectional study. BMC Nurs. 2020, 19, 22. [Google Scholar] [CrossRef]
- Soellner, R.; Huber, S.; Reder, M. The Concept of eHealth Literacy and Its Measurement. J. Media Psychol. 2014, 26, 29–38. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. 3.63 Million Healthcare Workers Have Direct Patient Contact, Press Release No. N085 of 23 December 2020; Statistisches Bundesamt: Wiesbaden, Germany, 2020. [Google Scholar]
- Gottschall, S. Gesundheits-Apps: Wer Nutzt Sie? Und Was Denken Die Bürger? Available online: https://blog.der-digitale-patient.de/gesundheits-apps-buerger/ (accessed on 1 May 2023).
- Epstein, N.; Huber, J.; Gartmeier, M.; Berberat, P.O.; Reimer, M.; Fischer, M.R. Investigation on the acquisition of scientific competences during medical studies and the medical doctoral thesis. GMS J. Med. Educ. 2018, 35, Doc20. [Google Scholar] [PubMed]
- Ballantine, J.A.; McCourt Larres, P.; Oyelere, P. Computer usage and the validity of self-assessed computer competence among first-year business students. Comput. Educ. 2007, 49, 976–990. [Google Scholar] [CrossRef]
- Ihme, J.M.; Senkbeil, M. Warum können Jugendliche ihre eigenen computerbezogenen Kompetenzen nicht realistisch einschätzen? Z. Entwickl. Pädagog. Psychol. 2017, 49, 24–37. [Google Scholar] [CrossRef]
- Sinopidis, X.; Tsekoura, E.; Plotas, P.; Gkentzi, D.; Roupakias, S.; Fouzas, S.; Karatza, A.; Skaperda, M.; Panagiotopoulou, O.; Spyridakis, I.; et al. Healthcare workers’ hand hygiene knowledge and compliance evaluation, in a Greek university hospital. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5667–5675. [Google Scholar]
- Zakeri, H.; Ahmadi, F.; Rafeemanesh, E.; Saleh, L.A. The knowledge of hand hygiene among the healthcare workers of two teaching hospitals in Mashhad. Electron Physician 2017, 9, 5159–5165. [Google Scholar] [CrossRef]
- Zia, I.; Cheema, S.S.; Sheikh, N.S.; Ashraf, H. Hand Hygiene Knowledge, Attitudes, and Self-Reported Practices among Medical and Nursing Staff of a Tertiary-Care Military Hospital: A Cross-Sectional Study. Available online: https://ijic.info/article/view/21469 (accessed on 13 May 2022).
- Baier, C.; Albrecht, U.-V.; Ebadi, E.; Vonberg, R.-P.; Schilke, R. Knowledge about hand hygiene in the Generation Z: A questionnaire-based survey among dental students, trainee nurses and medical technical assistants in training. Am. J. Infect. Control 2020, 48, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Exner, M.; Gebel, J. Verkürzung der Einwirkzeit der hygienischen Händedesinfektion auf 15 Sekunden—Mitteilung der Desinfektionsmittel-Kommission im VAH. Hyg. Med. 2019, 44, 121–123. [Google Scholar]
- Fuchs, E.; Niehaus, I.; Stoletzki, A. Das Schulbuch in der Forschung—Analyse und Empfehlung für die Bildungspraxis, 4th ed.; V&R Unipress: Göttingen, Germany, 2014. [Google Scholar]
- Segarra, V.A.; Tanner, S. Comparing outdated and updated textbook figures helps introduce undergraduates to primary literature. J. Microbiol. Biol. Educ. 2015, 16, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Stambaugh, J.E.; Trank, C.Q. Not So Simple: Integrating New Research Into Textbooks. Acad. Manag. Learn. Educ. 2010, 9, 663–681. [Google Scholar]
- KRINKO. Händehygiene in Einrichtungen des Gesundheitswesens—Empfehlung der Kommission für Krankenhaushygiene und Infektionspraävention (KRINKO) beim Robert Koch-Institut (RKI). Bundesgesundheitsblatt Gesundh. Gesundh. 2016, 59, 1189–1220. [Google Scholar] [CrossRef] [PubMed]
- Gniadek, A.; Ogorek-Tecza, B.; Inglot, A.; Nowacka, A.; Micek, A. Hand Areas Which Are Commonly Missed during Hand Disinfection by Nursing Students Who Completed a Basic Educational Course in Hand Hygiene. Int. J. Environ. Res. Public Health 2021, 18, 2590. [Google Scholar] [CrossRef]
- Kampf, G.; Ruselack, S.; Eggerstedt, S.; Nowak, N.; Bashir, M. Less and less-influence of volume on hand coverage and bactericidal efficacy in hand disinfection. BMC Infect. Dis. 2013, 13, 472. [Google Scholar] [CrossRef]
- Hitchings, A.W.; Wood, D.M.; Warren-Gash, C.; Gil Rivas, S.; Dargan, P.I. Determining the volume of toxic liquid ingestions in adults: Accuracy of estimates by healthcare professionals and members of the public. Clin. Toxicol. 2013, 51, 77–82. [Google Scholar] [CrossRef]
- Schuld, J.; Kollmar, O.; Seidel, R.; Black, C.; Schilling, M.K.; Richter, S. Estimate or calculate? How surgeons rate volumes and surfaces. Langenbeck’s Arch. Surg. 2012, 397, 763–769. [Google Scholar] [CrossRef]
- Szumska, E.; Czajkowski, P.; Zablocki, M.; Rozkiewicz, D. The Association between Hand Disinfection Techniques and Their Barriers, as Well as the “Bare below the Elbows” Concept, among Healthcare Professionals—A Study Based on a Polish Population. Int. J. Environ. Res. Public Health 2022, 19, 11781. [Google Scholar] [CrossRef]
- Fichtner, A.; Haupt, E.; Karwath, T.; Wullenk, K.; Pöhlmann, C.; Jatzwauk, L. A single standardized practical training for surgical scrubbing according to EN1500: Effect quantification, value of the standardized method and comparison with clinical reference groups. GMS Z. Med. Ausbild. 2013, 30, Doc24. [Google Scholar] [PubMed]
- Kampf, G.; Reichel, M.; Feil, Y.; Eggerstedt, S.; Kaulfers, P.M. Influence of rub-in technique on required application time and hand coverage in hygienic hand disinfection. BMC Infect. Dis. 2008, 8, 149. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Result |
|---|---|
| Age [mean ± SD (median; range: min–max)] | 24 ± 3.59 (23; 18–44) |
| Gender | |
| Female | 152 (74.5%) |
| Male | 52 (25.5%); |
| Place of residence | |
| Large city (>100,000 inhabitants) | 146 (71.6%) |
| Medium-size city (>20,000 inhabitants) | 20 (9.8%) |
| Small town (>5000 inhabitants) | 18 (8.8%) |
| Rural area (<5000 inhabitants) | 20 (9.8%) |
| Last educational qualification | |
| Intermediate school leaving certificate | 9 (4.4%) |
| Qualification for university entrance | 148 (72.5%) |
| University degree | 36 (17.6%) |
| Completed vocational training | 11 (5.4%) |
| Current status | |
| In training for radiology technician | 13 (6.4%) |
| In medical studies (university) | 191 (93.6%) |
| Item | Mean ± SD | Factor Loading | Mean Item-Total Correlation |
|---|---|---|---|
| I know what health resources are available on the internet | 3.35 ± 0.98 | 0.71 | 0.72 |
| I know where to find helpful health resources on the internet | 3.69 ± 0.92 | 0.79 | 0.76 |
| I know how to find helpful health resources on the internet | 3.76 ± 0.92 | 0.68 | 0.69 |
| I know how to use the internet to answer my questions about health | 3.84 ± 0.91 | 0.76 | 0.73 |
| I know how to use the health information I find on the internet to help me | 3.86 ± 0.95 | 0.65 | 0.72 |
| I have the skills I need to evaluate the health resources I find on the internet | 3.90 ± 0.93 | 0.73 | 0.58 |
| I can tell high-quality health resources from low-quality health resources on the internet | 3.82 ± 0.92 | 0.77 | 0.60 |
| I feel confident in using information from the internet to make health decisions | 3.54 ± 0.92 | 0.58 | 0.60 |
| Variance accounted for = 31.9% | |||
| Coefficient alpha = 0.89 | |||
| Knowledge Statements (Correct Responses) | RT, n (%) | MS, n (%) | Total, n (%) |
|---|---|---|---|
| Which of the following is the main route of the transmission of potentially harmful germs between patients? (Healthcare workers hands when not clean) | 5 (38.5) | 173 (90.6) | 178 (87.3) |
| What is the most frequent source of germs responsible for healthcare associated infections? (Germs already present on or within the patient) | 10 (76.9) | 117 (61.3) | 127 (62.3) |
| Which of the following hand hygiene actions prevents the transmission of germs to a patient? | |||
| Before touching the patient (yes) | 13 (100) | 189 (99) | 202 (99) |
| Immediately after a risk of body fluid exposure (no) | 1 (7.7) | 62 (32.5) | 63 (30.9) |
| After exposure to the immediate surroundings of a patient (no) | 7 (53.8) | 70 (36.6) | 77 (37.7) |
| Immediately before a clean/aseptic procedure (yes) | 11 (84.6) | 188 (98.4) | 199 (97.5) |
| Which of the following hand hygiene actions prevents the transmission of germs to healthcare workers? | |||
| After touching a patient (yes) | 13 (100) | 189 (99) | 202 (99) |
| Immediately after a risk of body fluid exposure (yes) | 13 (100) | 190 (99.5) | 203 (99.5) |
| Immediately before a clean/aseptic procedure (no) | 3 (23.1) | 116 (60.7) | 119 (58.3) |
| After exposure to the immediate surroundings of a patient (yes) | 11 (84.6) | 186 (97.4) | 197 (96.6) |
| Which of the following statements on alcohol-based handrubbing and handwashing with soap and water are true? | |||
| Handrubbing is more rapid for hand cleansing than handwashing (true) | 4 (30.8) | 115 (60.2) | 119 (58.3) |
| Handrubbing causes skin dryness more than handwashing (false) | 3 (23.1) | 162 (84.8) | 165 (80.9) |
| Handrubbing is more effective against germs than handwashing (true) | 11 (84.6) | 149 (78) | 160 (78.4) |
| Handwashing and handrubbing are recommended to be performed in sequence (false) | 3 (23.1) | 102 (53.4) | 105 (51.5) |
| What is the minimal time needed for alcohol-based handrub to kill most germs on your hands? (20 s) | 3 (23.1) | 106 (55.5) | 109 (53.4) |
| Which type of hand hygiene method is required in the following situations? | |||
| Before palpation of the abdomen (rubbing) | 10 (76.9) | 176 (92.1) | 186 (91.2) |
| Before giving an injection (rubbing) | 10 (76.9) | 187 (97.9) | 197 (96.6) |
| After emptying a bedpan (rubbing) | 8 (61.5) | 124 (64.9) | 132 (64.7) |
| After removing examination gloves (rubbing) | 6 (46.2) | 171 (89.5) | 177 (86.8) |
| After making a patient’s bed (rubbing) | 9 (69.2) | 165 (86.4) | 174 (85.3) |
| After visible exposure to blood (washing) | 6 (46.2) | 103 (53.9) | 109 (53.4) |
| Which of the following should be avoided, as it is associated with an increased likelihood that harmful germs will colonize on hands? | |||
| Jewelry (yes) | 9 (69.2) | 190 (99.5) | 199 (97.5) |
| Damaged skin (yes) | 10 (76.9) | 187 (97.9) | 197 (96.6) |
| Artificial fingernails (yes) | 9 (69.2) | 189 (99) | 198 (97.1) |
| Regular use of a hand cream (no) | 9 (69.2) | 184 (96.3) | 193 (94.6) |
| A Back | B1 Back | B2 Back | |
|---|---|---|---|
| A front | <0.001 | <0.001 | <0.001 |
| B1 front | 0.5037 | <0.001 | <0.001 |
| B2 front | <0.001 | <0.001 | 0.8168 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kühnel, C.; Salomo, S.; Pagiatakis, H.; Hübner, J.; Seifert, P.; Freesmeyer, M.; Gühne, F. Medical Students’ and Radiology Technician Trainees’ eHealth Literacy and Hygiene Awareness—Asynchronous and Synchronous Digital Hand Hygiene Training in a Single-Center Trial. Healthcare 2023, 11, 1475. https://doi.org/10.3390/healthcare11101475
Kühnel C, Salomo S, Pagiatakis H, Hübner J, Seifert P, Freesmeyer M, Gühne F. Medical Students’ and Radiology Technician Trainees’ eHealth Literacy and Hygiene Awareness—Asynchronous and Synchronous Digital Hand Hygiene Training in a Single-Center Trial. Healthcare. 2023; 11(10):1475. https://doi.org/10.3390/healthcare11101475
Chicago/Turabian StyleKühnel, Christian, Sarah Salomo, Helena Pagiatakis, Jutta Hübner, Philipp Seifert, Martin Freesmeyer, and Falk Gühne. 2023. "Medical Students’ and Radiology Technician Trainees’ eHealth Literacy and Hygiene Awareness—Asynchronous and Synchronous Digital Hand Hygiene Training in a Single-Center Trial" Healthcare 11, no. 10: 1475. https://doi.org/10.3390/healthcare11101475
APA StyleKühnel, C., Salomo, S., Pagiatakis, H., Hübner, J., Seifert, P., Freesmeyer, M., & Gühne, F. (2023). Medical Students’ and Radiology Technician Trainees’ eHealth Literacy and Hygiene Awareness—Asynchronous and Synchronous Digital Hand Hygiene Training in a Single-Center Trial. Healthcare, 11(10), 1475. https://doi.org/10.3390/healthcare11101475