

The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Cranial Pain and Vital Signs
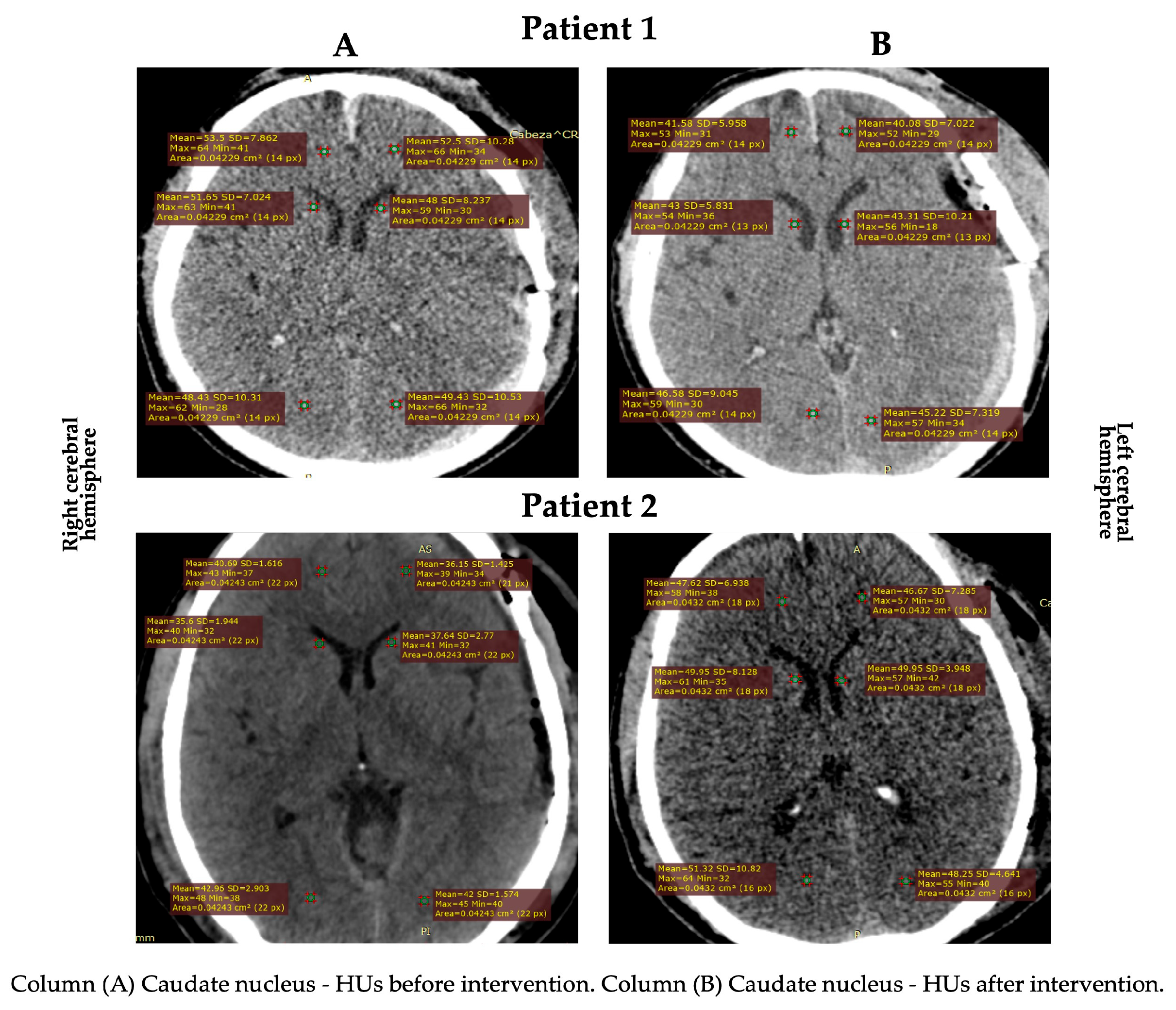
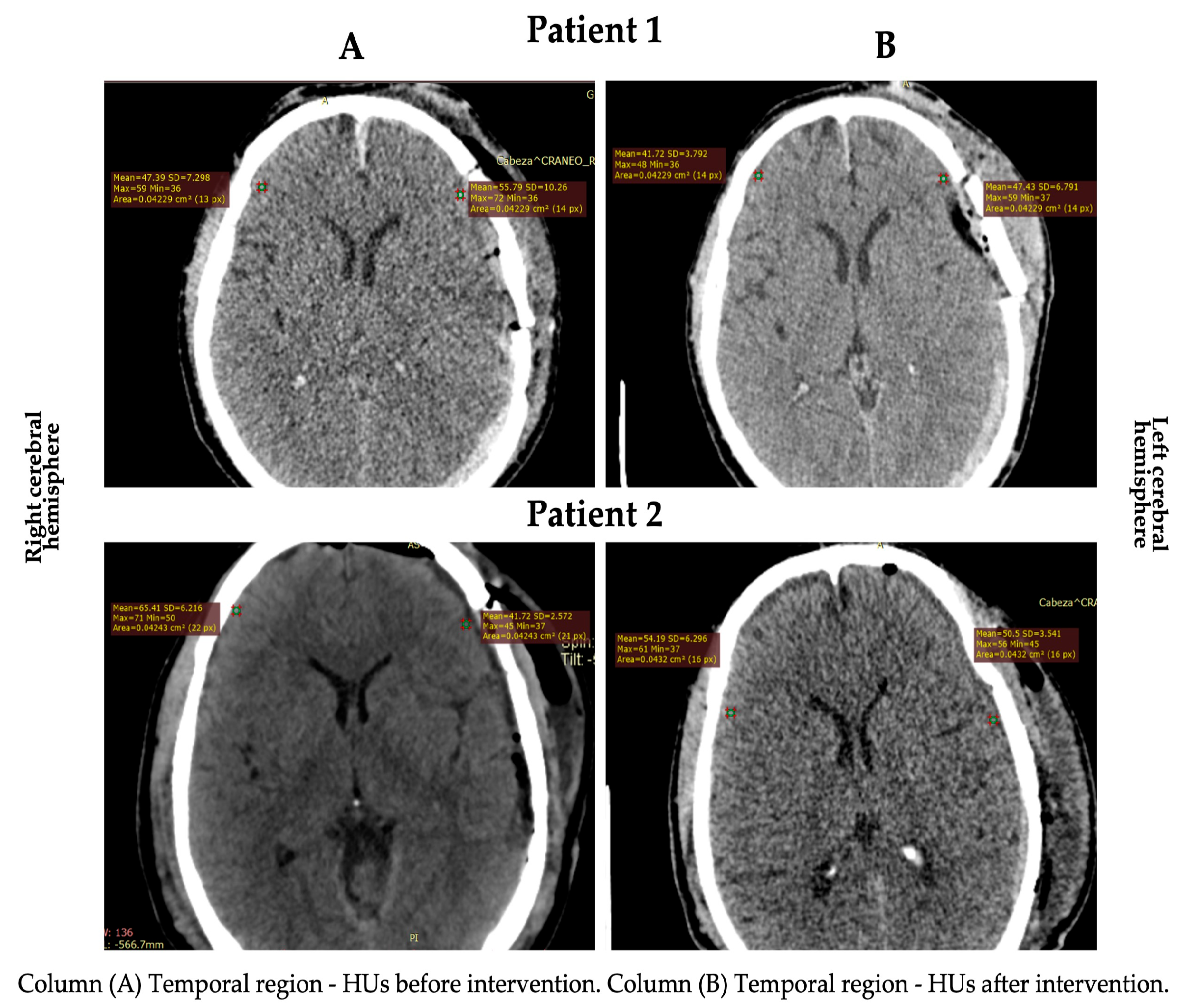
3.2. Cerebral Edema
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mckee, A.C.; Daneshvar, D.H. The Neuropathology of Traumatic Brain Injury. Handb. Clin. Neurol. 2015, 127, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.M.; Kochanek, P.M.; Simard, J.M. Pathophysiology and Treatment of Cerebral Edema in Traumatic Brain Injury. Neuropharmacology 2019, 145, 230–246. [Google Scholar] [CrossRef] [PubMed]
- Winkler, E.; Minter, D.; Yue, J.K.; Manley, G. Cerebral Edema in Traumatic Brain Injury: Pathophysiology and Prospective Therapeutic Targets. Neurosurg. Clin. N. Am. 2016, 27, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Hablitz, L.M.; Nedergaard, M. The Glymphatic System: A Novel Component of Fundamental Neurobiology. J. Neurosci. Off. J. Soc. Neurosci. 2021, 41, 7698–7711. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Cao, Y.; Tang, X.; Huang, J.; Cai, L.; Zhou, L. The Meningeal Lymphatic Vessels and the Glymphatic System: Potential Therapeutic Targets in Neurological Disorders. J. Cereb. Blood Flow Metab. 2022, 42, 1364–1382. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A Paravascular Pathway Facilitates CSF Flow through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef]
- Sun, B.-L.; Wang, L.-H.; Yang, T.; Sun, J.-Y.; Mao, L.-L.; Yang, M.-F.; Yuan, H.; Colvin, R.A.; Yang, X.-Y. Lymphatic Drainage System of the Brain: A Novel Target for Intervention of Neurological Diseases. Prog. Neurobiol. 2018, 163–164, 118–143. [Google Scholar] [CrossRef]
- Biswas, L.; Chen, J.; De Angelis, J.; Singh, A.; Owen-Woods, C.; Ding, Z.; Pujol, J.M.; Kumar, N.; Zeng, F.; Ramasamy, S.K.; et al. Lymphatic Vessels in Bone Support Regeneration after Injury. Cell 2023, 186, 382–397.e24. [Google Scholar] [CrossRef]
- Johnston, M.; Zakharov, A.; Papaiconomou, C.; Salmasi, G.; Armstrong, D. Evidence of Connections between Cerebrospinal Fluid and Nasal Lymphatic Vessels in Humans, Non-Human Primates and Other Mammalian Species. Cereb. Fluid Res. 2004, 1, 2. [Google Scholar] [CrossRef]
- Stokes, C.; White, E.F.; Toddes, S.; Bens, N.; Kulkarni, P.; Ferris, C.F. Whole CNS 3D Cryo-Fluorescence Tomography Shows CSF Clearance along Nasal Lymphatics, Spinal Nerves, and Lumbar/Sacral Lymph Nodes. J. Imaging 2023, 9, 45. [Google Scholar] [CrossRef]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. The Glymphatic Pathway in Neurological Disorders. Lancet Neurol. 2018, 17, 1016–1024. [Google Scholar] [CrossRef]
- Jacob, L.; de Brito Neto, J.; Lenck, S.; Corcy, C.; Benbelkacem, F.; Geraldo, L.H.; Xu, Y.; Thomas, J.-M.; El Kamouh, M.-R.; Spajer, M.; et al. Conserved Meningeal Lymphatic Drainage Circuits in Mice and Humans. J. Exp. Med. 2022, 219, e20220035. [Google Scholar] [CrossRef]
- Ferrara, M.; Bertozzi, G.; Volonnino, G.; Di Fazio, N.; Frati, P.; Cipolloni, L.; La Russa, R.; Fineschi, V. Glymphatic System a Window on TBI Pathophysiology: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 9138. [Google Scholar] [CrossRef]
- Ji, C.; Yu, X.; Xu, W.; Lenahan, C.; Tu, S.; Shao, A. The Role of Glymphatic System in the Cerebral Edema Formation after Ischemic Stroke. Exp. Neurol. 2021, 340, 113685. [Google Scholar] [CrossRef]
- Wang, M.; Ding, F.; Deng, S.; Guo, X.; Wang, W.; Iliff, J.J.; Nedergaard, M. Focal Solute Trapping and Global Glymphatic Pathway Impairment in a Murine Model of Multiple Microinfarcts. J. Neurosci. Off. J. Soc. Neurosci. 2017, 37, 2870–2877. [Google Scholar] [CrossRef]
- Ishida, K.; Yamada, K.; Nishiyama, R.; Hashimoto, T.; Nishida, I.; Abe, Y.; Yasui, M.; Iwatsubo, T. Glymphatic System Clears Extracellular Tau and Protects from Tau Aggregation and Neurodegeneration. J. Exp. Med. 2022, 219, e20211275. [Google Scholar] [CrossRef]
- Pettemeridou, E.; Kennedy, M.R.T.; Constantinidou, F. Executive Functions, Self-Awareness and Quality of Life in Chronic Moderate-to-Severe TBI. NeuroRehabilitation 2020, 46, 109–118. [Google Scholar] [CrossRef]
- Andriessen, T.M.J.C.; Jacobs, B.; Vos, P.E. Clinical Characteristics and Pathophysiological Mechanisms of Focal and Diffuse Traumatic Brain Injury. J. Cell. Mol. Med. 2010, 14, 2381–2392. [Google Scholar] [CrossRef]
- Irvine, K.-A.; Clark, J.D. Chronic Pain After Traumatic Brain Injury: Pathophysiology and Pain Mechanisms. Pain Med. 2018, 19, 1315–1333. [Google Scholar] [CrossRef]
- Leduc, O. Drenaje linfático manual con el método Leduc. EMC Kinesiterapia Med. Física 2014, 35, 1–10. [Google Scholar] [CrossRef]
- Lopera, C.; Worsley, P.R.; Bader, D.L.; Fenlon, D. Investigating the Short-Term Effects of Manual Lymphatic Drainage and Compression Garment Therapies on Lymphatic Function Using Near-Infrared Imaging. Lymphat. Res. Biol. 2017, 15, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Schingale, F.-J.; Esmer, M.; Küpeli, B.; Ünal, D. Investigation of the Less Known Effects of Manual Lymphatic Drainage: A Narrative Review. Lymphat. Res. Biol. 2022, 20, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.; Stitz, H.; Roth, C.; Ferbert, A.; Deinsberger, W.; Pahl, R.; Engel, H.; Kleffmann, J. Craniocervical Manual Lymphatic Drainage and Its Impact on Intracranial Pressure—A Pilot Study. Eur. J. Neurol. 2016, 23, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Wei, Y.; Zhang, X.; Huang, J.; Nie, M.; Liu, X.; Yuan, J.; Wang, D.; Tian, Y.; Jiang, W.; et al. Craniocervical Manual Lymphatic Drainage Increases the Efficiency of Atorvastatin-Based Treatment of Chronic Subdural Hematoma. Transl. Stroke Res. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Charlick, M.; Das, J.M. Anatomy, Head and Neck: Internal Carotid Arteries; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- DenOtter, T.D.; Schubert, J. Hounsfield Unit. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Oh, J.H.; Choi, S.P.; Wee, J.H.; Park, J.H. Inter-Scanner Variability in Hounsfield Unit Measured by CT of the Brain and Effect on Gray-to-White Matter Ratio. Am. J. Emerg. Med. 2019, 37, 680–684. [Google Scholar] [CrossRef]
- Río-González, Á.; Cerezo-Téllez, E.; Gala-Guirao, C.; González-Fernández, L.; Díaz-Meco Conde, R.; de la Cueva-Reguera, M.; Guitérrez-Ortega, C. Effects of Different Neck Manual Lymphatic Drainage Maneuvers on the Nervous, Cardiovascular, Respiratory and Musculoskeletal Systems in Healthy Students. J. Clin. Med. 2020, 9, 4062. [Google Scholar] [CrossRef]
- Lim-Hing, K.; Rincon, F. Secondary Hematoma Expansion and Perihemorrhagic Edema after Intracerebral Hemorrhage: From Bench Work to Practical Aspects. Front. Neurol. 2017, 8, 74. [Google Scholar] [CrossRef]
- Korosec, B.J. Manual Lymphatic Drainage Therapy. Home Health Care Manag. Pract. 2004, 16, 499–511. [Google Scholar] [CrossRef]
- Esmer, M.; Keser, I.; Erer, D.; Kupeli, B. Acute Cardiovascular Responses to the Application of Manual Lymphatic Drainage in Different Body Regions. Lymphat. Res. Biol. 2019, 17, 362–367. [Google Scholar] [CrossRef]
- Shibahashi, K.; Sugiyama, K.; Okura, Y.; Tomio, J.; Hoda, H.; Hamabe, Y. Defining Hypotension in Patients with Severe Traumatic Brain Injury. World Neurosurg. 2018, 120, e667–e674. [Google Scholar] [CrossRef]
- Lorente-Aznar, T.; Perez-Aguilar, G.; García-Espot, A.; Benabarre-Ciria, S.; Mendia-Gorostidi, J.L.; Dols-Alonso, D.; Blasco-Romero, J. Estimation of arterial oxygen saturation in relation to altitude. Med. Clin. 2016, 147, 435–440. [Google Scholar] [CrossRef]
- Urday, S.; Beslow, L.A.; Dai, F.; Zhang, F.; Battey, T.W.; Vashkevich, A.; Ayres, A.; Leasure, A.; Selim, M.; Simard, J.M.; et al. Rate of Perihematomal Edema Expansion Predicts Outcome After Intracerebral Hemorrhage. Crit. Care Med. 2016, 44, 790–797. [Google Scholar] [CrossRef]
- Tong, L.; Guo, Z.; Ou, Y.; Yu, Y.; Zhang, X.; Tang, J.; Zhang, J.H.; Lou, Q.A. Cerebral Venous Collaterals: A New Fort for Fighting Ischemic Stroke? Prog. Neurobiol. 2018, 163–164, 172–193. [Google Scholar] [CrossRef]
- De Vlieger, G.; Meyfroidt, G. Kidney Dysfunction After Traumatic Brain Injury: Pathophysiology and General Management. Neurocrit. Care 2022, 38, 504–516. [Google Scholar] [CrossRef]
- Rauchman, S.H.; Albert, J.; Pinkhasov, A.; Reiss, A.B. Mild-to-Moderate Traumatic Brain Injury: A Review with Focus on the Visual System. Neurol. Int. 2022, 14, 453–470. [Google Scholar] [CrossRef]
- Rauchman, S.H.; Zubair, A.; Jacob, B.; Rauchman, D.; Pinkhasov, A.; Placantonakis, D.G.; Reiss, A.B. Traumatic Brain Injury: Mechanisms, Manifestations, and Visual Sequelae. Front. Neurosci. 2023, 17, 1090672. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; Baril, A.-A.; Charlebois-Plante, C.; Jodoin, M.; Sanchez, E.; De Baets, L.; Arbour, C.; Lavigne, G.J.; Gosselin, N.; De Beaumont, L. The Putative Role of Neuroinflammation in the Interaction between Traumatic Brain Injuries, Sleep, Pain and Other Neuropsychiatric Outcomes: A State-of-the-Art Review. J. Clin. Med. 2023, 12, 1793. [Google Scholar] [CrossRef]
- Shim, J.-M.; Kim, S.-J. Effects of Manual Lymph Drainage of the Neck on EEG in Subjects with Psychological Stress. J. Phys. Ther. Sci. 2014, 26, 127–129. [Google Scholar] [CrossRef]
- Honguten, A.; Mekhora, K.; Pichaiyongwongdee, S.; Somprasong, S. Effects of Lymphatic Drainage Therapy on Autonomic Nervous System Responses in Healthy Subjects: A Single Blind Randomized Controlled Trial. J. Bodyw. Mov. Ther. 2021, 27, 169–175. [Google Scholar] [CrossRef]
- Kim, S.-J.; Kwon, O.-Y.; Yi, C.-H. Effects of Manual Lymph Drainage on Cardiac Autonomic Tone in Healthy Subjects. Int. J. Neurosci. 2009, 119, 1105–1117. [Google Scholar] [CrossRef]
- Mavroudis, I.; Chatzikonstantinou, S.; Ciobica, A.; Balmus, I.-M.; Iordache, A.; Kazis, D.; Chowdhury, R.; Luca, A.-C. A Systematic Review and Meta-Analysis of the Grey Matter Volumetric Changes in Mild Traumatic Brain Injuries. Appl. Sci. 2022, 12, 9954. [Google Scholar] [CrossRef]
- Kim, H.; Kim, G.; Yoon, B.C.; K, K.; Kim, B.-J.; Choi, Y.H.; Czosnyka, M.; Oh, B.-M.; Kim, D.-J. Quantitative Analysis of Computed Tomography Images and Early Detection of Cerebral Edema for Pediatric Traumatic Brain Injury Patients: Retrospective Study. BMC Med. 2014, 12, 186. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before | After | Difference (%) | |
|---|---|---|---|
| Cranial pain (cm) | |||
| Patient 1 | 5 | 5 | 0 (=00.00) |
| Patient 2 | 6 | 2 | 4 (↓ 66.66) |
| Heart rate (lpm) | |||
| Patient 1 | 88 | 75 | 13 (↓ 14.77) |
| Patient 2 | 59 | 60 | 1 (↑ 01.66) |
| Respiratory rate (rpm) | |||
| Patient 1 | 14 | 15 | 1 (↑ 06.66) |
| Patient 2 | 13 | 17 | 4 (↑ 23.52) |
| Oxygen saturation SpO₂ (%) | |||
| Patient 1 | 85 | 93 | 8 (↑ 08.60) |
| Patient 2 | 89 | 94 | 5 (↑ 07.44) |
| Systolic blood pressure (mmHg) | |||
| Patient 1 | 118 | 122 | 4 (↑ 03.27) |
| Patient 2 | 144 | 128 | 16 (↓ 11.11) |
| Diastolic blood pressure (mmHg) | |||
| Patient 1 | 70 | 66 | 4 (↓ 05.71) |
| Patient 2 | 66 | 80 | 14 (↑ 17.50) |
| Body temperature (°C) | |||
| Patient 1 | 36.2 | 37 | 0.8 (↑ 02.16) |
| Patient 2 | 37.1 | 37.2 | 0.1 (↑ 00.26) |
| Before | After | Difference (%) | |
|---|---|---|---|
| RCH | |||
| TR (HU) | |||
| Patient 1 | 47.39 | 41.72 | 05.67 (↓ 11.96) |
| Patient 2 | 65.41 | 54.19 | 11.22 (↓ 17.15) |
| CN (HU) | |||
| Patient 1 | 51.65 | 43.00 | 08.65 (↓ 16.74) |
| Patient 2 | 35.60 | 49.95 | 14.35 (↑ 28.72) |
| LCH | |||
| TR (HU) | |||
| Patient 1 | 55.79 | 47.43 | 08.36 (↓ 14.98) |
| Patient 2 | 41.72 | 50.50 | 08.78 (↑ 17.38) |
| CN (HU) | |||
| Patient 1 | 48.00 | 43.31 | 04.90 (↓ 09.77) |
| Patient 2 | 37.64 | 49.95 | 12.31 (↑ 24.64) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esparza, W.D.; Aladro-Gonzalvo, A.R.; Ruíz-Hontangas, A.; Celi, D.; Aguirre, M.B. The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury. Healthcare 2023, 11, 1474. https://doi.org/10.3390/healthcare11101474
Esparza WD, Aladro-Gonzalvo AR, Ruíz-Hontangas A, Celi D, Aguirre MB. The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury. Healthcare. 2023; 11(10):1474. https://doi.org/10.3390/healthcare11101474
Chicago/Turabian StyleEsparza, Wilmer Danilo, Arian Ramón Aladro-Gonzalvo, Antonio Ruíz-Hontangas, Daniela Celi, and María Belén Aguirre. 2023. "The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury" Healthcare 11, no. 10: 1474. https://doi.org/10.3390/healthcare11101474
APA StyleEsparza, W. D., Aladro-Gonzalvo, A. R., Ruíz-Hontangas, A., Celi, D., & Aguirre, M. B. (2023). The Effect of Craniofacial Manual Lymphatic Drainage after Moderate Traumatic Brain Injury. Healthcare, 11(10), 1474. https://doi.org/10.3390/healthcare11101474