

Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
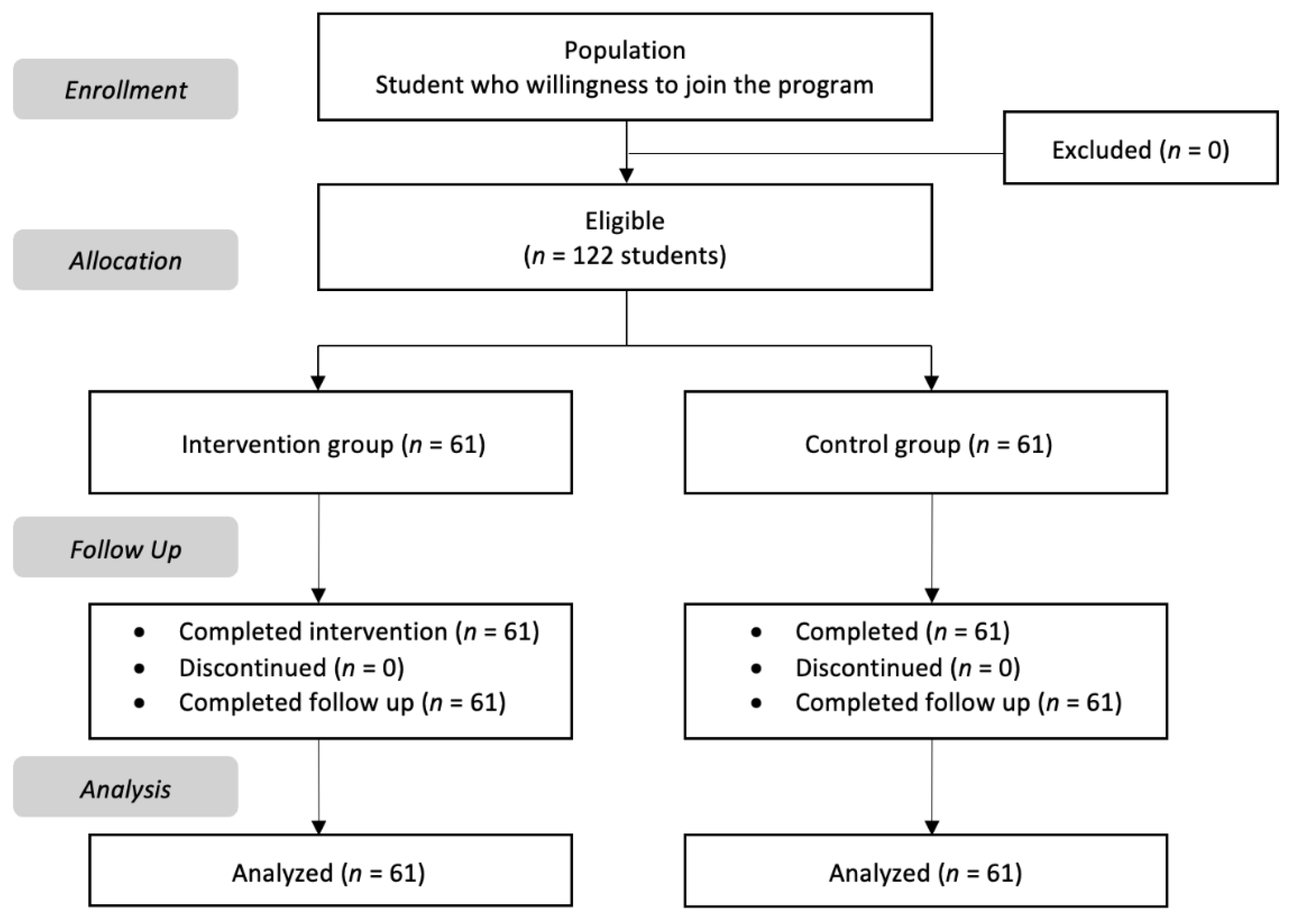
2.2. Recruiting and Sampling
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Clearance
3. Result
3.1. Characteristics of Participants
3.2. Baseline and Post-Intervention Stress, Anxiety, and Depression of Participants
3.3. Frequency Distribution of Participants’ Levels of Stress, Anxiety, and Depression
3.4. Age and Religion Factors on Participant’s Interventions
4. Discussion
4.1. Principal Finding
4.2. Limitations
4.3. Implications for Clinical Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martinez, P.J.; Aguilar, F.J.; Ortiz, M. Transitioning from face-to-face to blended and full online learning engineering master’s program. IEEE Trans. Educ. 2020, 63, 2–9. [Google Scholar] [CrossRef]
- Pelucio, L.; Simões, P.; Cristina, M.; Dourado, N.; Quagliato, L.A.; Nardi, A.E. Depression and anxiety among online learning students during the COVID-19 pandemic: A cross-sectional survey in Rio de Janeiro, Brazil. BMC 2022, 10, 192. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Ho, C. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.R.; Nihei, O.K. Depression, anxiety and stress symptoms in Brazilian university students during the COVID-19 pandemic: Predictors and association with life satisfaction, psychological well-being and coping strategies. PLoS ONE 2021, 61, e0258493. [Google Scholar] [CrossRef]
- Fawaz, M.; Samaha, A. E-learning: Depression, anxiety, and stress symptomatology among Lebanese university students during COVID-19 quarantine. Nurs. Forum 2021, 56, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Lindquist, R. Effects of mindfulness-based stress reduction on depression, anxiety, stress and mindfulness in Korean nursing students. Nurse Educ. Today 2015, 35, 86–90. [Google Scholar] [CrossRef]
- Buchanan, J.L. Prevention of depression in the college student population: A review of the literature. Arch. Psychiatr. Nurs. 2012, 26, 21–42. [Google Scholar] [CrossRef]
- Santoso, A.; Ardi, W.R.; Prasetya, R.L.; Dwidiyanti, M.; Wijayanti, D.Y.; Mu’in, M.; Aisah, N.A. Tingkat depresi mahasiswa keperawatan di tengah wabah COVID-19. Holist. Nurs. Health Sci. 2020, 3, 1–8. [Google Scholar] [CrossRef]
- Mahmoud, J.S.R.; Staten, R.T.; Hall, L.A.; Lennie, T.A. The relationship among young adult college students’ depression, anxiety, stress, demographics, life satisfaction, and coping styles. Issues Ment. Health Nurs. 2012, 33, 149–156. [Google Scholar] [CrossRef]
- García-González, J.; Ruqiong, W.; Alarcon-Rodriguez, R.; Requena-Mullor, M.; Ding, C.; Ventura-Miranda, M.I. Analysis of Anxiety Levels of Nursing Students Because of e-Learning during the COVID-19 Pandemic. Healthcare 2021, 9, 252. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Pandemic Has Worsened Pre-Existing Mental Health Conditions. News-Medical Net. 2020. Available online: https://www.news-medical.net/news/20200601/COVID-19-pandemic-has-worsened-pre-existing-mental-health-conditions.aspx (accessed on 14 April 2022).
- Shikai, N.; Shono, M.; Kitamura, T. Effects of coping styles and stressful life events on depression and anxiety in Japanese nursing students: A longitudinal study. Int. J. Nurs. Prac. 2009, 15, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Warnecke, E.; Quinn, S.; Ogden, K.; Towle, N.; Nelson, M.R. A randomised controlled trial of the effects of mindfulness practice on medical student stress levels. Med. Educ. 2011, 45, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, S.S.; Niles, B.L.; Park, C.L. A mindfulness model of affect regulation and depressive symptoms: Positive emotions, mood regulation expectancies, and self-acceptance as regulatory mechanisms. Personal. Individ. Differ. 2010, 49, 645–650. [Google Scholar] [CrossRef]
- Aristovnik, A.; Keržič, D.; Ravšelj, D.; Tomaževič, N.; Umek, L. Impacts of the covid-19 pandemic on life of higher education students. Sustainability 2020, 12, 8438. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of covid-19 on college students’ mental health in the united states: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Limcaoco, R.S.G.; Mateos, E.M.; Fernandez, J.M.; Roncero, C. Anxiety, worry and perceived stress in the world due to the COVID-19 pandemic, March 2020. Preliminary results. MedRiv 2020. [Google Scholar] [CrossRef]
- Baer, R.A. Self-focused attention and mechanisms of change in mindfulness-based treatment. Cogn. Behav. Ther. 2009, 38, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Crowley, C.; Kapitula, L.R.; Munk, D. Mindfulness, happiness, and anxiety in a sample of college students before and after taking a meditation course. J. Am. Coll. Health 2020, 70, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Hidayati, N.; Aryanti, P.I.; Salim, S.; Zuliani Erniyawati, Y.; Yusuf, A. Penggunaan mindfulness meditation dalam manajemen stres: Sebuah systematic review. J. Penelit. Kesehat. Suara Forikes 2018, 9, 95–100. [Google Scholar]
- Spears, C.A. Perceptions of mindfulness in a low-income, primarily african american treatment-seeking sample. Physiol. Behav. 2019, 176, 139–148. [Google Scholar] [CrossRef]
- Barnes, N.; Hattan, P.; Black, D.S.; Schuman-Olivier, Z. An examination of mindfulness-based programs in US medical schools. Mindfulness 2017, 8, 489–494. [Google Scholar] [CrossRef]
- Black, D.S. Mindfulness-based interventions: An antidote to suffering in the context of substance use, misuse, and addiction. Subst. Use Misuse 2014, 49, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Seppälä, E.M.; Bradley, C.; Moeller, J.; Harouni, L.; Nandamudi, D.; Brackett, M.A. Promoting mental health and psychological thriving in university students: A randomized controlled trial of three well-being interventions. Front. Psychiatry. 2020, 11, 590. [Google Scholar] [CrossRef] [PubMed]
- De Vibe, M.; Solhaug, I.; Tyssen, R.; Friborg, O.; Rosenvinge, J.H.; Sørlie, T.; Bjørndal, A. Mindfulness training for stress management: A randomised controlled study of medical and psychology students. BMC Med. Educ. 2013, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Psychology Foundation of Australia. 2013. Available online: http://www.psychologyfoundation.org.au (accessed on 12 July 2022).
- Widyana, R.; Sumiharso; Safitri, R.M. Psychometric properties of internet-administered version of depression, anxiety and stress scales (dass-42) in sample Indonesian adult. J. Talent Dev. Excell. 2020, 12, 1422–1434. [Google Scholar]
- Damanik, E.D.; Rusli, E. Pengujian Reabilitas, Validitas, Analisis Item, dan Pembuatan Norma Depression Anxiety Scale (DASS): Berdasarkan Penelitian pada Kelompok Sampel Yogyakarta dan Bantul yang Mengalami Gempa Bumi dan Kelompok Sampel Jakarta dan Sekitarnya yang Tidak Mengalami Gempa Bumi. Thesis, Faculty of Psychology, Universitas Indonesia, Depok, Indonesia, 2006. [Google Scholar]
- Mutaqqin, D.; Ripa, S. Psychometric properties of the Indonesian version of the department anxiety stress scale: Factor structure, reability, gender and age measurements invariance. Psikohumaniora J. Penelit. Psikol. 2021, 6, 61–76. [Google Scholar] [CrossRef]
- Ibrahim, K.; Komariah, M.; Herliani, Y.K. The effect of mindfulness breathing meditation on psychological well-being: A quasi-experimental study among nurses working for COVID-19 patients. Holist. Nurs. Pract. 2022, 36, 46–51. [Google Scholar] [CrossRef]
- Nyklíček, I.; Dijksman, S.C.; Lenders, P.J.; Fonteijn, W.A.; Koolen, J.J. A brief mindfulness-based intervention for increase in emotional well-being and quality of life in percutaneous coronary intervention (pci) patients: The mindfulheart randomized controlled trial. J. Behav. Med. 2014, 37, 135–144. [Google Scholar] [CrossRef]
- Chiodelli, R.; Jesus SN, D.; Mello LT, N.D.; Andretta, I.; Oliveira, D.F.; Costa ME, S.; Russell, T. Effects of the Interculturality and Mindfulness Program (PIM) on University Students: A Quasi-Experimental Study. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1500–1515. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, X.; Wang, L.; Zhang, X. A randomized controlled trial of the effects of brief mindfulness meditation on anxiety symptoms and systolic blood pressure in Chinese nursing students. Nurse Educ. Today 2013, 33, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.S.; Choi, S.Y.; Ryu, E. The effectiveness of a stress coping program based on mindfulness meditation on the stress, anxiety, and depression experienced by nursing students in Korea. Nurse Educ. Today 2009, 29, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Dobkin, P.L.; Zhao, Q. Increased mindfulness–The active component of the mindfulness-based stress reduction program? Complement. Ther. Clin. Pract. 2011, 17, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Anālayo, B. In the seen just the seen: Mindfulness and the construction of experience. Mindfulness 2019, 10, 179–184. [Google Scholar] [CrossRef]
- Kropp, A.; Sedlmeier, P. What makes mindfulness-based interventions effective? An examination of common components. Mindfulness 2019, 10, 2060–2072. [Google Scholar] [CrossRef]
- Mak, W.W.; Chio, F.H.; Chan, A.T.; Lui, W.W.; Wu, E.K. The efficacy of internet-based mindfulness training and cognitive-behavioral training with telephone support in the enhancement of mental health among college students and young working adults: Randomized controlled trial. J. Med. Internet Res. 2017, 19, e84. [Google Scholar] [CrossRef] [PubMed]
- Widiasih, R.; Ermiati; Jayanti, T.N.; Rais, Y. Psychosocial Interventions for Improving the Quality of Life in Breast Cancer Survivors: A Literature Review. IOP Conf. Ser. Earth Environ. Sci. 2019, 248, 12056. [Google Scholar] [CrossRef]
- Komariah, M.; Amirah, S.; Faisal, E.G.; Prayogo, S.A.; Maulana, S.; Platini, H.; Suryani, S.; Yosep, I.; Arifin, H. Efficacy of Internet-Based Cognitive Behavioral Therapy for Depression and Anxiety among Global Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis of a Randomized Controlled Trial Study. Healthcare 2022, 10, 1224. [Google Scholar] [CrossRef]
- Kurniawan, K.; Yosep, I.; Maulana, S.; Mulyana, A.M.; Amirah, S.; Abdurrahman, M.F.; Sugianti, A.; Putri, E.G.; Khoirunnisa, K.; Komariah, M.; et al. Efficacy of Online-Based Intervention for Anxiety during COVID-19: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sustainability 2022, 14, 2866. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Control Group | Intervention Group | p-Value |
|---|---|---|---|
| Gender | |||
| Female | 51 (83.60%) | 42 (68.90%) | 0.089 |
| Male | 10 (16.40%) | 19 (31.15%) | |
| Religion | |||
| Islam | 54 (49.1%) | 56 (50.9%) | 0.361 |
| Christian | 5 (50%) | 5 (50%) | |
| Buddhism | 2 (100%) | 0 (0%) | |
| Age | 20.30 ± 1.116 | 22.42 ± 3.672 | 0.000 |
| Variable | Intervention Group M (SD) | Control Group M (SD) | p-Value | |
|---|---|---|---|---|
| Stress | Baseline | 16.31 (9.807) | 16.00 (10.00) | 0.862 |
| Post | 10.07 (6.957) | 14.03 (8.77) | 0.007 | |
| Anxiety | Baseline | 14.08 (8.737) | 13.39 (8.74) | 0.664 |
| Post | 8.46 (5.448) | 10.66 (6.32) | 0.042 | |
| Depression | Baseline | 13.93 (9.631) | 12.36 (9.42) | 0.363 |
| Post | 7.54 (7.309) | 9.46 (7.70) | 0.161 | |
| Variable | Intervention Group | Control Group | ||
|---|---|---|---|---|
| Baseline | Post | Baseline | Post | |
| Stress | ||||
| Normal | 32 (51.6%) | 44 (55.7%) | 30 (48.4%) | 35 (44.3%) |
| Mild | 8 (50.0%) | 8 (42.1%) | 8 (50.0%) | 11 (57.9%) |
| Moderate | 8 (40.0%) | 7 (46.7%) | 12 (60.0%) | 8 (53.3%) |
| Severe | 10 (55.6%) | 0 (0.0%) | 8 (44.4%) | 6 (100.0%) |
|
Extremely severe | 3 (50.0%) | 2 (66.7%) | 3 (50.0%) | 1 (33.3%) |
| Anxiety | ||||
| Normal | 15 (50.0%) | 30 (57.7%) | 15 (50.0%) | 22 (42.3%) |
| Mild | 6 (50.0%) | 7 (46.7%) | 6 (50.0%) | 8 (53.3%) |
| Moderate | 15 (44.1%) | 17 (54.8%) | 19 (55.9%) | 14 (45.2%) |
| Severe | 9 (60.0%) | 4 (28.6%) | 6 (40.0%) | 10 (71.4%) |
|
Extremely severe | 16 (51.6%) | 3 (30.0%) | 15 (48.4%) | 7 (70.0%) |
| Depression | ||||
| Normal | 21 (43.8%) | 29 (58.0%) | 27 (56.2%) | 21 (42.0%) |
| Mild | 13 (52.0%) | 18 (62.1%) | 12 (48.0%) | 11 (37.9%) |
| Moderate | 14 (53.8%) | 10 (37.0%) | 12 (46.2%) | 17 (63.0%) |
| Severe | 6 (60.0%) | 2 (22.2%) | 4 (40.0%) | 7 (77.8%) |
|
Extremely severe | 7 (53.8%) | 2 (28.6%) | 6 (46.2%) | 5 (71.4%) |
| Variable | Baseline | Post | p-Value * | ||
|---|---|---|---|---|---|
| IG (M, SD) | CG (M, SD) | IG (M, SD) | CG (M, SD) | ||
| Age (years) | |||||
| Stress | |||||
| <21 | 14.66 (9.152) | 21.83 (7.627) | 10.00 (6.958) | 14.83 (9.827) | 0.63 |
| 21 | 18.82 (11.775) | 15.19 (6.322) | 11.12 (7.960) | 13.05 (8.851) | |
| >21 | 18.00 (7.714) | 15.47 (11.909) | 8.33 (4.975) | 14.50 (8.760) | |
| Anxiety | |||||
| <21 | 12.60 (8.388) | 17.33 (5.007) | 8.23 (5.180) | 13.50 (6.504) | 0.457 |
| 21 | 15.59 (10.381) | 13.10 (6.503) | 9.71 (6.659) | 11.05 (7.619) | |
| >21 | 17.00 (5.831) | 12.88 (10.304) | 7.00 (3.742) | 9.91 (5.384) | |
| Depression | |||||
| <21 | 12.66 (9.434) | 16.67 (8.335) | 7.74 (6.423) | 11.83 (6.969) | 0.573 |
| 21 | 16.76 (11.306) | 11.67 (6.102) | 8.35 (10.000) | 11.10 (9.633) | |
| >21 | 13.56 (6.126) | 12.03 (11.156) | 5.22 (4.206) | 8.03 (6.264) | |
| Religion | |||||
| Stress | |||||
| Islam | 17.20 (9.727) | 16.11 (10.101) | 10.69 (7.012) | 14.41 (8.891) | 0.568 |
| Christian | 10.00 (8.337) | 14.80 (9.731) | 4.80 (2.683) | 9.80 (6.496) | |
| Buddhism | 8.00 (9.899) | - | 6.50 (9.192) | - | |
| Anxiety | |||||
| Islam | 14.89 (8.801) | 13.43 (8.932) | 9.00 (5.425) | 10.71 (6.387) | 0.505 |
| Christian | 8.20 (4.868) | 13.00 (6.892) | 3.80 (2.168) | 10.00 (6.205) | |
| Buddhism | 7.00 (8.485) | - | 5.50 (7.778) | - | |
| Depression | |||||
| Islam | 14.50 (9.743) | 12.63 (9.680) | 7.93 (7.581) | 9.55 (7.865) | 0.534 |
| Christian | 9.40 (7.436) | 9.40 (5.550) | 3.40 (1.140) | 8.40 (6.025) | |
| Buddhism | 10.00 (12.728) | - | 7.50 (7.778) | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komariah, M.; Ibrahim, K.; Pahria, T.; Rahayuwati, L.; Somantri, I. Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students. Healthcare 2023, 11, 26. https://doi.org/10.3390/healthcare11010026
Komariah M, Ibrahim K, Pahria T, Rahayuwati L, Somantri I. Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students. Healthcare. 2023; 11(1):26. https://doi.org/10.3390/healthcare11010026
Chicago/Turabian StyleKomariah, Maria, Kusman Ibrahim, Tuti Pahria, Laili Rahayuwati, and Irman Somantri. 2023. "Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students" Healthcare 11, no. 1: 26. https://doi.org/10.3390/healthcare11010026
APA StyleKomariah, M., Ibrahim, K., Pahria, T., Rahayuwati, L., & Somantri, I. (2023). Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students. Healthcare, 11(1), 26. https://doi.org/10.3390/healthcare11010026