
Association of Stool Frequency and Consistency with the Risk of All-Cause and Cause-Specific Mortality among U.S. Adults: Results from NHANES 2005–2010


Abstract
1. Introduction
2. Methods
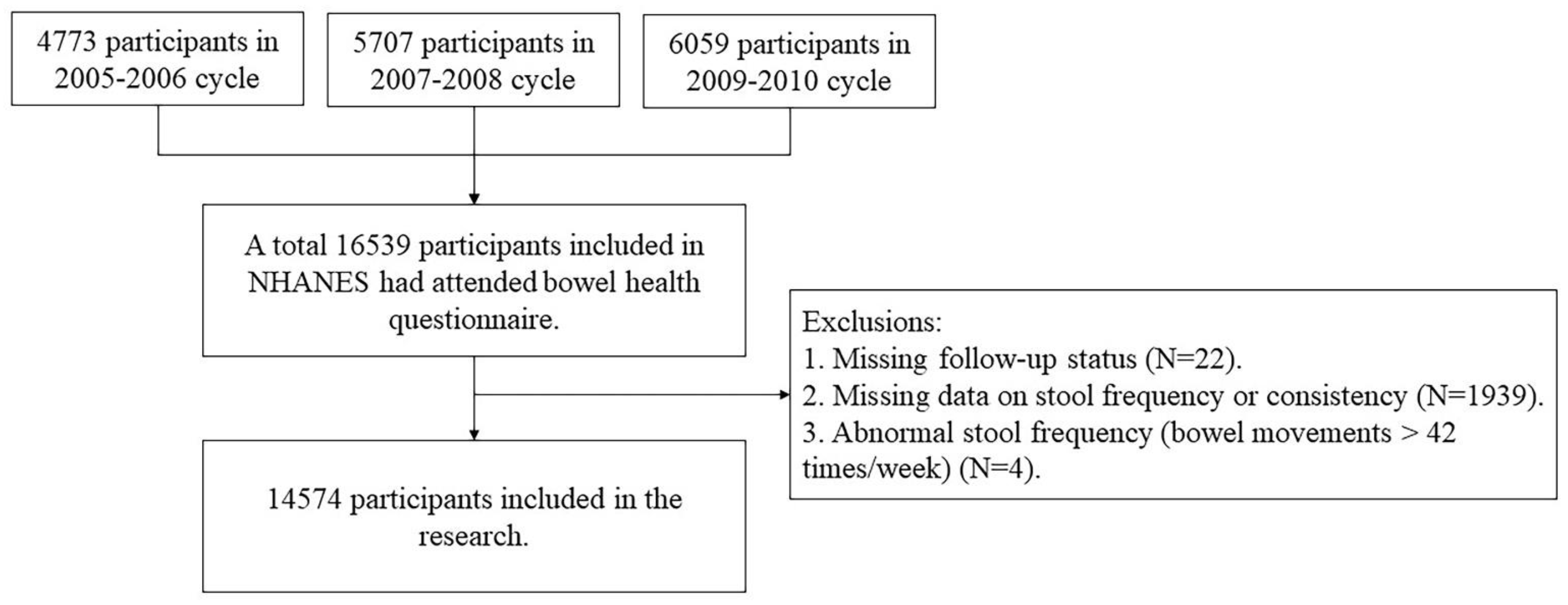
2.1. Study Design and Population
2.2. Definition of Exposure
2.3. Definition of Outcome
2.4. Definition of Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
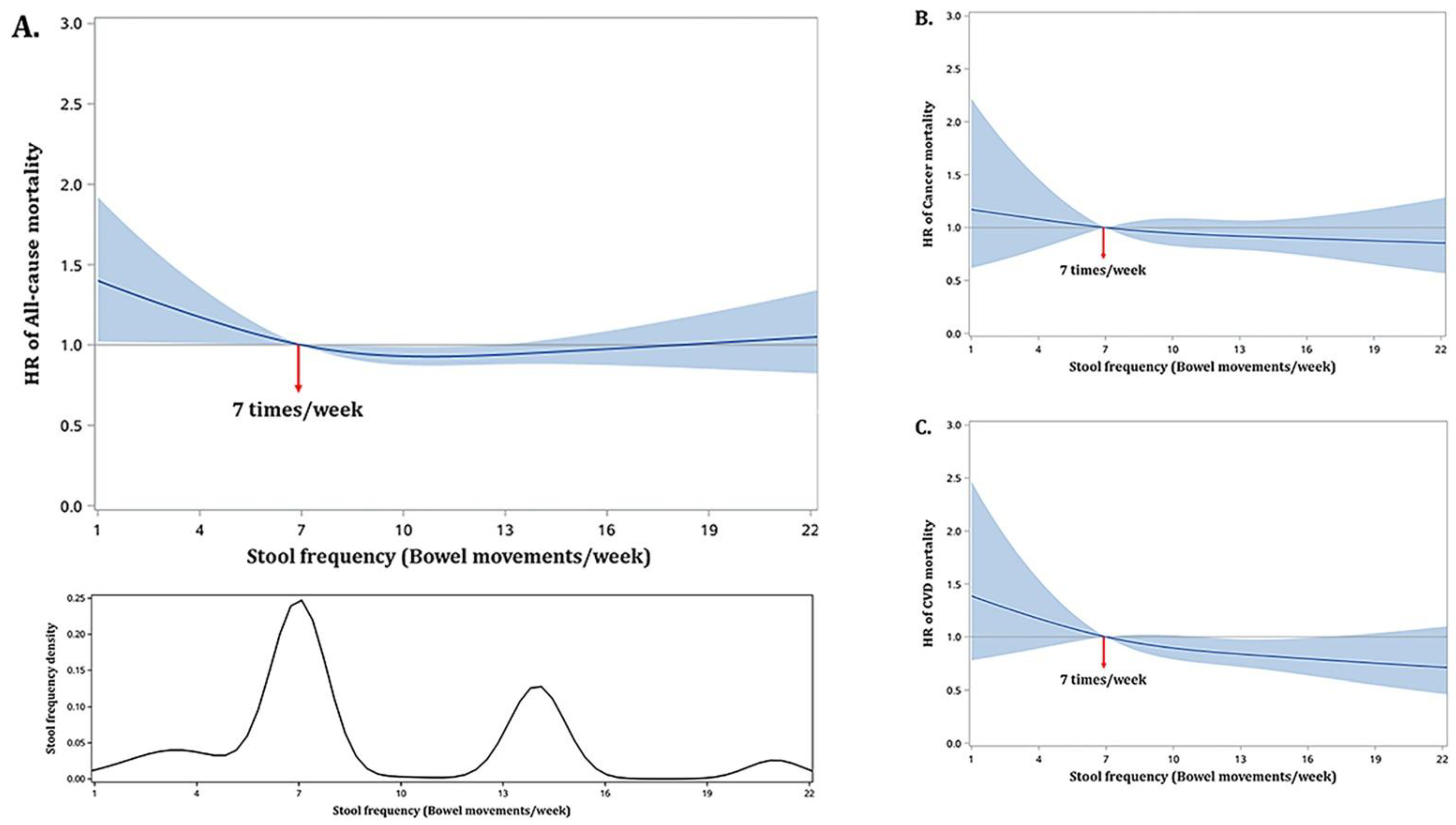
3.2. Stool Frequency and Mortality
3.3. Stool Consistency and Mortality
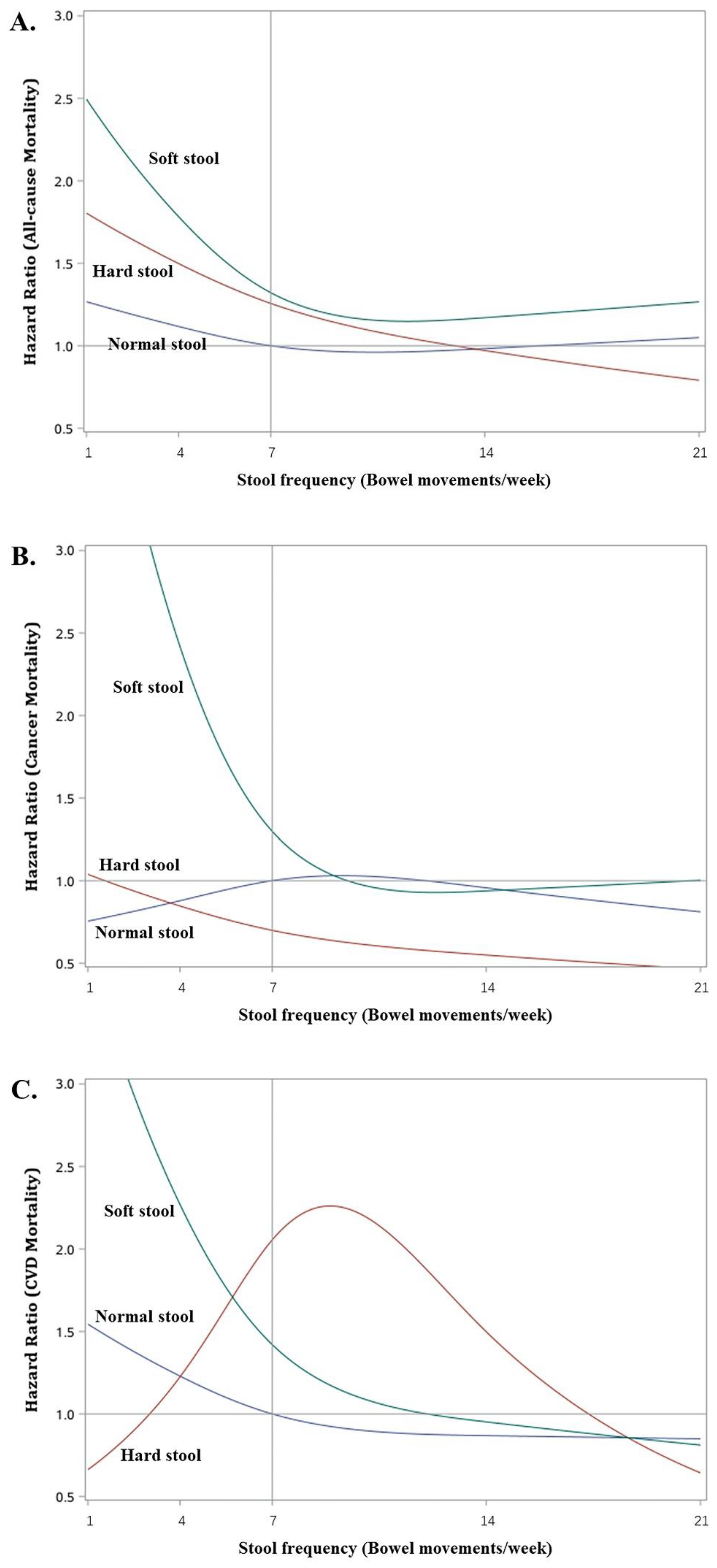
3.4. Joint Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NHANES | National Health and Nutrition Examination Survey |
| HR | hazard ratio |
| CVD | cardiovascular disease |
| ICD | international classification of disease |
| BMI | body mass index |
| ANOVA | analysis of variance |
| CI | confidence intervals |
References
- Barbara, G.; Feinle-Bisset, C.; Ghoshal, U.C.; Santos, J.; Vanner, S.J.; Vergnolle, N.; Zoetendal, E.G.; Quigley, E.M. The Intestinal Microenvironment and Functional Gastrointestinal Disorders. Gastroenterology 2016, 150, 1305–1318.e8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xie, Q.; Huo, X.; Liu, Z.; Da, M.; Yuan, M.; Zhao, Y.; Shen, G. Impact of intestinal dysbiosis on breast cancer metastasis and progression. Front. Oncol. 2022, 12, 1037831. [Google Scholar] [CrossRef] [PubMed]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 2021, 19, 55–71. [Google Scholar] [CrossRef]
- Qian, B.; Zhang, K.; Li, Y.; Sun, K. Update on gut microbiota in cardiovascular diseases. Front. Cell. Infect. Microbiol. 2022, 12, 1059349. [Google Scholar] [CrossRef]
- Shang, H.; Zhang, L.; Xiao, T.; Ruan, J.; Zhang, Q.; Liu, K.; Yu, Z.; Ni, Y.; Wang, B. Study on the differences of gut microbiota composition between phlegm-dampness syndrome and qi-yin deficiency syndrome in patients with metabolic syndrome. Front. Endocrinol. 2022, 13, 1063579. [Google Scholar] [CrossRef]
- Li, W.; Chen, T. An Insight into the Clinical Application of Gut Microbiota during Anticancer Therapy. Adv. Gut Microbiome Res. 2022, 2022, 8183993. [Google Scholar] [CrossRef]
- Ahluwalia, B.; Iribarren, C.; Magnusson, M.; Sundin, J.; Clevers, E.; Savolainen, O.; Ross, A.; Törnblom, H.; Simrén, M.; Öhman, L. A Distinct Faecal Microbiota and Metabolite Profile Linked to Bowel Habits in Patients with Irritable Bowel Syndrome. Cells 2021, 10, 1459. [Google Scholar] [CrossRef]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Vieira-Silva, S.; Falony, G.; Darzi, Y.; Lima-Mendez, G.; Yunta, R.G.; Okuda, S.; Vandeputte, D.; Valles-Colomer, M.; Hildebrand, F.; Chaffron, S.; et al. Species-function relationships shape ecological properties of the human gut microbiome. Nat. Microbiol. 2016, 1, 16088. [Google Scholar] [CrossRef]
- De Clercq, N.C.; Groen, A.K.; Romijn, J.A.; Nieuwdorp, M. Gut Microbiota in Obesity and Undernutrition. Adv. Nutr. Int. Rev. J. 2016, 7, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, K.E.; Lynch, S.V. Microbiota in Allergy and Asthma and the Emerging Relationship with the Gut Microbiome. Cell Host Microbe 2015, 17, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Carding, S.; Verbeke, K.; Vipond, D.T.; Corfe, B.M.; Owen, L.J. Dysbiosis of the gut microbiota in disease. Microb. Ecol. Health Dis. 2015, 26, 26191. [Google Scholar] [CrossRef] [PubMed]
- Törnblom, H.; Van Oudenhove, L.; Sadik, R.; Abrahamsson, H.; Tack, J.; Simrén, M. Colonic transit time and IBS symptoms: What’s the link? Am. J. Gastroenterol. 2012, 107, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Glia, A.; Lindberg, G.; Nilsson, L.H.; Mihocsa, L.; Åkerlund, J.E. Clinical value of symptom assessment in patients with constipation. Dis. Colon Rectum 1999, 42, 1401–1408; discussion 1408–1410. [Google Scholar] [CrossRef]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Tito, R.Y.; Joossens, M.; Raes, J. Stool consistency is strongly associated with gut microbiota richness and composition, enterotypes and bacterial growth rates. Gut 2016, 65, 57–62. [Google Scholar] [CrossRef]
- Vermorken, A.J.; Andrès, E.; Cui, Y. Bowel movement frequency, oxidative stress and disease prevention. Mol. Clin. Oncol. 2016, 5, 339–342. [Google Scholar] [CrossRef]
- Takagi, T.; Naito, Y.; Inoue, R.; Kashiwagi, S.; Uchiyama, K.; Mizushima, K.; Tsuchiya, S.; Dohi, O.; Yoshida, N.; Kamada, K.; et al. Differences in gut microbiota associated with age, sex, and stool consistency in healthy Japanese subjects. J. Gastroenterol. 2019, 54, 53–63. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Kubota, Y.; Iso, H.; Tamakoshi, A. Bowel Movement Frequency, Laxative Use, and Mortality from Coronary Heart Disease and Stroke Among Japanese Men and Women: The Japan Collaborative Cohort (JACC) Study. J. Epidemiol. 2016, 26, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Li, Y.; Heianza, Y.; Staller, K.; Chan, A.T.; Rimm, E.B.; Rexrode, K.; Qi, L. Associations of Bowel Movement Frequency with Risk of Cardiovascular Disease and Mortality among US Women. Sci. Rep. 2016, 6, 33005. [Google Scholar] [CrossRef] [PubMed]
- Honkura, K.; Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Defecation frequency and cardiovascular disease mortality in Japan: The Ohsaki cohort study. Atherosclerosis 2016, 246, 251–256. [Google Scholar] [CrossRef]
- Sumida, K.; Molnar, M.Z.; Potukuchi, P.K.; Thomas, F.; Lu, J.L.; Yamagata, K.; Kalantar-Zadeh, K.; Kovesdy, C.P. Constipation and risk of death and cardiovascular events. Atherosclerosis 2019, 281, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Nagai, Y.; Oitate, M.; Shiozawa, H.; Ando, O. Comprehensive preclinical pharmacokinetic evaluations of trastuzumab deruxtecan (DS-8201a), a HER2-targeting antibody-drug conjugate, in cynomolgus monkeys. Xenobiotica 2019, 49, 1086–1096. [Google Scholar] [CrossRef]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef]
- Wilson, P.B. Associations between physical activity and constipation in adult Americans: Results from the National Health and Nutrition Examination Survey. Neurogastroenterol. Motil. 2020, 32, e13789. [Google Scholar] [CrossRef]
- Taba Taba Vakili, S.; Nezami, B.G.; Shetty, A.; Chetty, V.K.; Srinivasan, S. Association of high dietary saturated fat intake and uncontrolled diabetes with constipation: Evidence from the National Health and Nutrition Examination Survey. Neurogastroenterol. Motil. 2015, 27, 1389–1397. [Google Scholar] [CrossRef]
- Vermorken, A.J.; Cui, Y.; Kleerebezem, R.; Andrès, E. Bowel movement frequency and cardiovascular mortality, a matter of fibers and oxidative stress? Atherosclerosis 2016, 253, 278–280. [Google Scholar] [CrossRef]
- Burkitt, D.P.; Walker, A.R.; Painter, N.S. Effect of dietary fibre on stools and the transit-times, and its role in the causation of disease. Lancet 1972, 2, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Rong, S.; Snetselaar, L.G.; Xu, G.; Sun, Y.; Liu, B.; Wallace, R.B.; Bao, W. Association of Skipping Breakfast With Cardiovascular and All-Cause Mortality. J. Am. Coll. Cardiol. 2019, 73, 2025–2032. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, M.; Hyman, N.; Osler, T. Fecal incontinence severity index after fistulotomy: A predictor of quality of life. Dis. Colon Rectum 2002, 45, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Locke, G.R.; McNally, A.M.; Halder, S.L.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J. Impact of Functional Gastrointestinal Disorders on Survival in the Community. Am. J. Gastroenterol. 2010, 105, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Salmoirago-Blotcher, E.; Crawford, S.; Jackson, E.; Ockene, J.; Ockene, I. Constipation and Risk of Cardiovascular Disease among Postmenopausal Women. Am. J. Med. 2011, 124, 714–723. [Google Scholar] [CrossRef]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial ecology: Human gut microbes associated with obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef]
- Drosos, I.; Tavridou, A.; Kolios, G. New aspects on the metabolic role of intestinal microbiota in the development of atherosclerosis. Metabolism 2015, 64, 476–481. [Google Scholar] [CrossRef]
- Harada, N.; Minami, Y.; Hanada, K.; Hanaoka, R.; Kobayashi, Y.; Izawa, T.; Sato, T.; Kato, S.; Inui, H.; Yamaji, R. Relationship between gut environment, feces-to-food ratio, and androgen deficiency-induced metabolic disorders. Gut Microbes 2020, 12, 1817719. [Google Scholar] [CrossRef]
- Musso, G.; Gambino, R.; Cassader, M. Interactions between gut microbiota and host metabolism predisposing to obesity and diabetes. Annu. Rev. Med. 2011, 62, 361–380. [Google Scholar] [CrossRef]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Hazen, S.L. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Investig. 2014, 124, 4204–4211. [Google Scholar] [CrossRef] [PubMed]
- Dacrema, M.; Ali, A.; Ullah, H.; Khan, A.; Di Minno, A.; Xiao, J.; Martins, A.M.C.; Daglia, M. Spice-Derived Bioactive Compounds Confer Colorectal Cancer Prevention via Modulation of Gut Microbiota. Cancers 2022, 14, 5682. [Google Scholar] [CrossRef] [PubMed]
- Caudet, J.; Trelis, M.; Cifre, S.; Soriano, J.M.; Rico, H.; Merino-Torres, J.F. Interplay between Intestinal Bacterial Communities and Unicellular Parasites in a Morbidly Obese Population: A Neglected Trinomial. Nutrients 2022, 14, 3211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, R.; Li, D.; Zhao, L.; Zhu, L. Role of gut microbiota in functional constipation. Gastroenterol. Rep. 2021, 9, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Pan, R.; Wang, L.; Xu, X.; Chen, Y.; Wang, H.; Wang, G.; Zhao, J.; Chen, W. Crosstalk between the Gut Microbiome and Colonic Motility in Chronic Constipation: Potential Mechanisms and Microbiota Modulation. Nutrients 2022, 14, 3704. [Google Scholar] [CrossRef]
- Tang, W.H.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N. Engl. J. Med. 2013, 368, 1575–1584. [Google Scholar] [CrossRef]
- Poon, W.Y.; Wang, H.B. Analysis of ordinal categorical data with misclassification. Br. J. Math. Stat. Psychol. 2010, 63, 17–42. [Google Scholar] [CrossRef]
- Chaussade, S.; Khyari, A.; Garret, M.; Gaudric, M.; Couturier, D.; Guerre, J. Determination of total and segmental colonic transit time in constipated patients. Results in 91 patients with a new simplified method. Dig. Dis. Sci. 1989, 34, 1168–1172. [Google Scholar] [CrossRef]
- Manning, A.P.; Wyman, J.B.; Heaton, K.W. How trustworthy are bowel histories? Comparison of recalled and recorded information. Br. Med. J. 1976, 2, 213–214. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Seide, B.M.; Zinsmeister, A.R.; Melton, L.J. Insights into normal and disordered bowel habits from bowel diaries. Am. J. Gastroenterol. 2008, 103, 692–698. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Stool Consistency Types | p-Value | ||
|---|---|---|---|---|---|
| Hard 1 | Normal 2 | Soft 3 | |||
| No. of participants | 14,574 | 1128 | 11,152 | 2294 | |
| Bowel movements, % | <0.0001 | ||||
| 1–2 times/week | 516 (3.3) | 123 (11.0) | 327 (2.7) | 66 (2.8) | |
| 3–6 times/week | 1664 (12.1) | 217 (21.1) | 1272 (12.1) | 175 (7.2) | |
| 7 times/week | 7386 (53.0) | 487 (43.8) | 5942 (55.6) | 957 (42.7) | |
| 8–21 times/week | 4807 (30.4) | 291 (23.4) | 3519 (28.8) | 997 (43.2) | |
| >21 times/week | 201 (1.2) | 10 (0.6) | 92 (0.8) | 99 (4.1) | |
| Age, years | 46.7 ± 0.3 | 45.7 ± 0.5 | 46.5 ± 0.4 | 48.3 ± 0.5 | <0.0001 |
| Females% | 7402 (51.1) | 777 (71.7) | 5353 (48.6) | 1272 (55.0) | <0.0001 |
| Race/Ethnicity% | <0.0001 | ||||
| non-Hispanic Black | 2890 (10.9) | 257 (14.6) | 2175 (10.4) | 458 (12.0) | |
| non-Hispanic White | 7184 (71.1) | 488 (64.8) | 5700 (72.6) | 996 (65.6) | |
| Mexican American | 2677 (8.2) | 216 (9.2) | 1948 (7.6) | 513 (10.9) | |
| Others | 1823 (9.8) | 167 (11.4) | 1329 (9.4) | 327 (11.5) | |
| Smoking status% | 0.0001 | ||||
| Never | 7651 (52.8) | 670 (59.1) | 5846 (52.9) | 1135 (48.8) | |
| Former smoker | 3703 (24.9) | 242 (20.9) | 2859 (25.1) | 602 (25.8) | |
| Current smoker | 3215 (22.3) | 216 (20.0) | 2443 (21.9) | 556 (25.4) | |
| Current drinker% | 10,414 (75.9) | 678 (65.1) | 8164 (77.3) | 1572 (73.7) | |
| Recreational physical activity% | <0.0001 | ||||
| Low or never | 5720 (47.8) | 495 (53.1) | 4130 (45.6) | 1095 (56.2) | |
| Moderate | 2657 (28.4) | 183 (26.5) | 2069 (29.3) | 405 (24.4) | |
| Vigorous | 1965 (23.8) | 131 (20.4) | 1582 (25.1) | 252 (19.3) | |
| BMI kg/m2 | 28.7 ± 0.1 | 27.8 ± 0.3 | 28.5 ± 0.1 | 30.2 ± 0.2 | <0.0001 |
| Underweight | 219 (1.6) | 24 (1.9) | 167 (1.7) | 28 (1.1) | <0.0001 |
| Normal weight | 3919 (29.8) | 361 (36.0) | 3075 (30.2) | 483 (24.6) | |
| Overweight | 4965 (33.7) | 371 (33.2) | 3857 (34.4) | 737 (29.9) | |
| Obesity | 5336 (34.9) | 360 (28.8) | 3958 (33.8) | 1018 (44.4) | |
| Dietary fiber g * | 16.3 ± 0.2 | 14.1 ± 0.3 | 16.6 ± 0.2 | 16.8 ± 0.2 | <0.0001 |
| Annual family income% | <0.0001 | ||||
| ≤$19,999 | 3491 (17.3) | 322 (22.4) | 2529 (16.4) | 640 (19.8) | |
| $20,000–$34,999 | 3442 (20.2) | 289 (24.3) | 2578 (19.6) | 575 (21.9) | |
| $35,000–$74,999 | 4069 (31.5) | 288 (29.8) | 3173 (31.7) | 608 (30.9) | |
| ≥$75000 | 3051 (31.0) | 176 (23.5) | 2487 (32.2) | 388 (27.4) | |
| History of chronic disease% | 6509 (40.6) | 462 (40.3) | 4860 (39.4) | 1187 (47.4) | <0.0001 |
| Characteristics | Stool Frequency | p-Value | ||||
|---|---|---|---|---|---|---|
| 1–2 Times/Week | 3–6 Times /Week | 7 Times/Week | 8–21 Times/Week | >21 Times/Week | ||
| Number of participants | 516 | 1664 | 7386 | 4807 | 201 | |
| Age, years | 43.0 ± 0.9 | 44.6 ± 0.5 | 47.6 ± 0.4 | 46.3 ± 0.4 | 49.7 ± 1.2 | <0.0001 |
| Female, n (%) | 401 (83.4) | 1081 (67.7) | 3826 (52.1) | 1997 (39.5) | 97 (44.7) | <0.0001 |
| Ethnicity, n (%) | <0.0001 | |||||
| non-Hispanic Black | 172 (21.5) | 383 (12.8) | 1224 (8.4) | 1076 (13.5) | 35 (10.9) | |
| non-Hispanic White | 235 (65.3) | 895 (73.8) | 4038 (75.1) | 1921 (63.7) | 95 (67.8) | |
| Mexican American | 57 (5.6) | 197 (5.0) | 1186 (6.7) | 1186 (12.3) | 51 (10.9) | |
| Others | 52 (7.6) | 189 (8.6) | 938 (9.8) | 624 (10.5) | 20 (10.4) | |
| Smoking status, n (%) | 0.0001 | |||||
| Never | 273 (52.5) | 935 (56.8) | 3830 (52.1) | 2508 (52.4) | 105 (52.6) | |
| Former smoker | 100 (19.0) | 367 (21.0) | 1972 (26.1) | 1211 (25.1) | 53 (25.7) | |
| Current smoker | 143 (28.5) | 362 (22.2) | 1582 (21.8) | 1085 (22.5) | 43 (21.7) | |
| Current drinker, n (%) | 319 (64.0) | 1159 (74.3) | 5260 (75.8) | 3536 (78.2) | 140 (70.5) | <0.0001 |
| Recreational physical activity, n (%) | 0.0034 | |||||
| Low or never | 226 (57.2) | 674 (48.7) | 2826 (47.0) | 1915 (47.8) | 79 (45.8) | |
| Moderate | 87 (29.1) | 287 (29.1) | 1391 (29.3) | 849 (26.3) | 43 (30.0) | |
| Vigorous | 47 (13.7) | 198 (22.2) | 960 (23.7) | 740 (25.9) | 20 (24.2) | |
| BMI, kg/m2 | 28.0 ± 0.3 | 27.7 ± 0.2 | 28.3 ± 0.1 | 29.8 ± 0.2 | 30.7 ± 0.5 | <0.0001 |
| Underweight, n (%) | 8 (1.7) | 35 (2.3) | 126 (1.8) | 47 (0.9) | 3 (1.4) | <0.0001 |
| Normal weight, n (%) | 170 (35.7) | 551 (36.4) | 2118 (31.3) | 1047 (24.3) | 33 (18.5) | |
| Overweight, n (%) | 162 (31.3) | 538 (31.9) | 2574 (34.2) | 1624 (33.7) | 67 (35.2) | |
| Obesity, n (%) | 170 (31.3) | 517 (29.4) | 2498 (32.7) | 2056 (41.1) | 95 (44.9) | |
| Dietary fiber, g * | 12.4 ± 0.4 | 14.7 ± 0.3 | 16.1 ± 0.2 | 17.6 ± 0.3 | 16.9 ± 0.8 | <0.0001 |
| Annual family income, n (%) | <0.0001 | |||||
| ≤$19,999 | 181 (29.8) | 389 (17.7) | 1690 (16.1) | 1166 (17.7) | 65 (24.2) | |
| $20,000–$34,999 | 117 (21.7) | 393 (19.0) | 1723 (20.1) | 1167 (21.1) | 42 (17.6) | |
| $35,000–$74,999 | 123 (27.6) | 486 (32.9) | 2089 (31.7) | 1320 (31.0) | 51 (29.2) | |
| ≥$75,000 | 73 (20.8) | 354 (30.3) | 1638 (32.1) | 949 (30.3) | 37 (28.9) | |
| History of chronic disease, n (%) | 223 (41.5) | 695 (37.0) | 3266 (39.8) | 2200 (42.6) | 125 (59.3) | <0.0001 |
| Stool Consistency | Proportion of Deaths | Mortality Rate (per 100,000 Person Years) | HR (95% CI) |
|---|---|---|---|
| All mortality | |||
| Separate hard lumps, like nuts | 40/319 | 1302 | 1.36 (0.99, 1.88) |
| Like a sausage but lumpy | 93/809 | 990 | 1.23 (0.98, 1.56) |
| A sausage shape with cracks in the surface | 313/3607 | 762 | 1.13 (0.94, 1.36) |
| Like a sausage or snake, smooth and soft | 769/7545 | 922 | Ref. |
| Soft blobs with clear-cut edges | 128/1162 | 1189 | 1.48 ** (1.17, 1.86) |
| Fluffy pieces with ragged edges, a mushy stool | 131/983 | 1323 | 1.20 (0.88, 1.64) |
| Watery, no solid pieces | 28/149 | 2452 | 1.41 (0.86, 2.33) |
| Cancer mortality | |||
| Separate hard lumps, like nuts | 6/319 | 252 | 1.25 (0.39, 3.95) |
| Like a sausage but lumpy | 13/809 | 106 | 0.57 (0.30, 1.07) |
| A sausage shape with cracks in the surface | 78/3607 | 191 | 1.21 (0.88, 1.66) |
| Like a sausage or snake, smooth and soft | 187/7545 | 219 | Ref. |
| Soft blobs with clear-cut edges | 31/1162 | 310 | 1.60 * (1.02,2.50) |
| Mushy stool, or watery | 42/1132 | 333 | 1.25 (0.69, 2.29) |
| CVD mortality | |||
| Separate hard lumps, like nuts | 9/319 | 283 | 1.80 (0.84, 3.88) |
| Like a sausage but lumpy | 19/809 | 191 | 1.45 (0.87, 2.41) |
| A sausage shape with cracks in the surface | 62/3607 | 136 | 1.04 (0.76, 1.43) |
| Like a sausage or snake, smooth and soft | 145/7545 | 171 | Ref. |
| Soft blobs with clear-cut edges | 26/1162 | 218 | 1.48 (0.86, 2.56) |
| Mushy stool, or watery | 23/1132 | 241 | 1.19 (0.70, 2.00) |
| Outcome | Joint Association/Type and Frequency | HR * | p-Value |
|---|---|---|---|
| All-cause | Hard stool at 4 times/week | 1.50 (1.19, 1.89) | 0.0006 |
| Hard stool at 7 times/week | 1.26 (1.00, 1.57) | 0.0456 | |
| Hard stool at 14 times/week | 0.97 (0.75, 1.26) | 0.8249 | |
| Hard stool at 21 times/week | 0.79 (0.44, 1.43) | 0.4348 | |
| Soft stool at 4 times/week | 1.78 (1.17, 2.73) | 0.0076 | |
| Soft stool at 7 times/week | 1.32 (1.06, 1.64) | 0.0120 | |
| Soft stool at 14 times/week | 1.17 (0.94, 1.46) | 0.1567 | |
| Soft stool at 21 times/week | 1.27 (0.98, 1.64) | 0.0696 | |
| Cancer | Hard stool at 4 times/week | 0.85 (0.48, 1.51) | 0.5709 |
| Hard stool at 7 times/week | 0.70 (0.38, 1.28) | 0.2478 | |
| Hard stool at 14 times/week | 0.55 (0.17, 1.74) | 0.3086 | |
| Hard stool at 21 times/week | 0.46 (0.05, 4.27) | 0.4972 | |
| Soft stool at 4 times/week | 2.42 (1.31, 4.47) | 0.0048 | |
| Soft stool at 7 times/week | 1.30 (0.86, 1.95) | 0.2078 | |
| Soft stool at 14 times/week | 0.94 (0.59, 1.48) | 0.7846 | |
| Soft stool at 21 times/week | 1.00 (0.62, 1.61) | 0.9911 | |
| CVD | Hard stool at 4 times/week | 1.23 (0.56, 2.69) | 0.6123 |
| Hard stool at 7 times/week | 2.05 (1.16, 3.64) | 0.0137 | |
| Hard stool at 14 times/week | 1.50 (0.77, 2.90) | 0.2296 | |
| Hard stool at 21 times/week | 0.64 (0.19, 2.19) | 0.4794 | |
| Soft stool at 4 times/week | 2.27 (1.12, 4.60) | 0.0231 | |
| Soft stool at 7 times/week | 1.42 (0.91, 2.21) | 0.1194 | |
| Soft stool at 14 times/week | 0.95 (0.54, 1.67) | 0.8630 | |
| Soft stool at 21 times/week | 0.81 (0.41, 1.62) | 0.5528 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, X.; Li, J.; Wu, Y.; Dai, H.; Lynn, H.S.; Zhang, X. Association of Stool Frequency and Consistency with the Risk of All-Cause and Cause-Specific Mortality among U.S. Adults: Results from NHANES 2005–2010. Healthcare 2023, 11, 29. https://doi.org/10.3390/healthcare11010029
Peng X, Li J, Wu Y, Dai H, Lynn HS, Zhang X. Association of Stool Frequency and Consistency with the Risk of All-Cause and Cause-Specific Mortality among U.S. Adults: Results from NHANES 2005–2010. Healthcare. 2023; 11(1):29. https://doi.org/10.3390/healthcare11010029
Chicago/Turabian StylePeng, Xinwei, Jibin Li, Yuwan Wu, Hongji Dai, Henry S. Lynn, and Xi Zhang. 2023. "Association of Stool Frequency and Consistency with the Risk of All-Cause and Cause-Specific Mortality among U.S. Adults: Results from NHANES 2005–2010" Healthcare 11, no. 1: 29. https://doi.org/10.3390/healthcare11010029
APA StylePeng, X., Li, J., Wu, Y., Dai, H., Lynn, H. S., & Zhang, X. (2023). Association of Stool Frequency and Consistency with the Risk of All-Cause and Cause-Specific Mortality among U.S. Adults: Results from NHANES 2005–2010. Healthcare, 11(1), 29. https://doi.org/10.3390/healthcare11010029