
Fast Saccadic Eye Movements Contribute to the Worsened Postural Sway in Older Adults Who Have Experienced Falls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
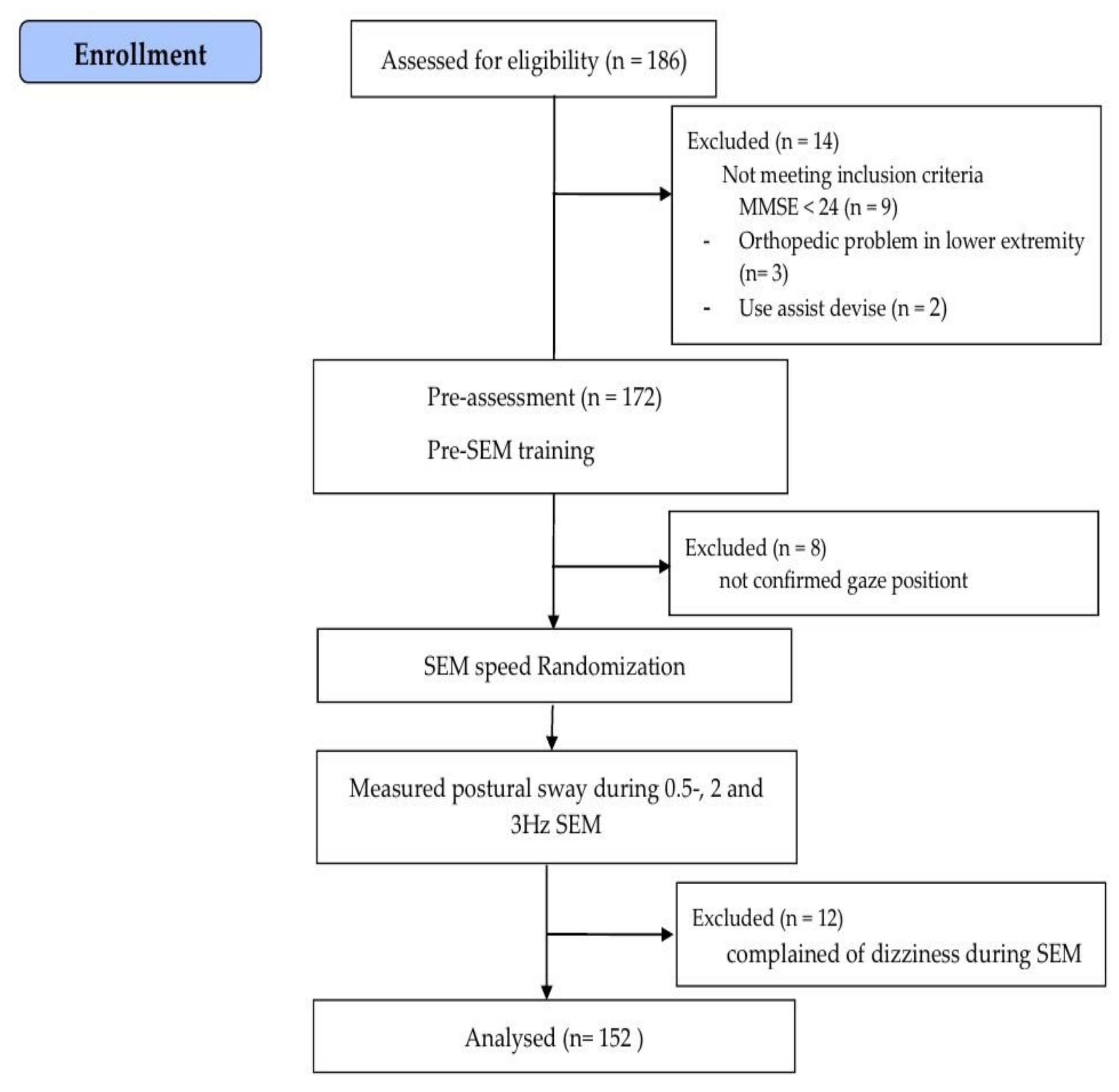
2.2. Participants and Procedures
2.3. SEM
2.4. Postural Sway Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, C.; Hallemans, A.; Verbecque, E.; De Vestel, C.; Herssens, N.; Vereeck, L. Aging and the Relationship between Balance Performance, Vestibular Function and Somatosensory Thresholds. J. Int. Adv. Otol. 2020, 16, 328. [Google Scholar] [CrossRef] [PubMed]
- Aartolahti, E.; Häkkinen, A.; Lönnroos, E.; Kautiainen, H.; Sulkava, R.; Hartikainen, S. Relationship between functional vision and balance and mobility performance in community-dwelling older adults. Aging Clin. Exp. Res. 2013, 25, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Bergland, A.; Wyller, T.B. Risk factors for serious fall related injury in elderly women living at home. Inj. Prev. 2004, 10, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Stel, V.S.; Smit, J.H.; Pluijm, S.M.; Lips, P. Balance and mobility performance as treatable risk factors for recurrent falling in older persons. J. Clin. Epidemiol. 2003, 56, 659–668. [Google Scholar] [CrossRef]
- Palmieri, R.M.; Ingersoll, C.D.; Stone, M.B.; Krause, B.A. Center-of-pressure parameters used in the assessment of postural control. J. Sport Rehabil. 2002, 11, 51–66. [Google Scholar] [CrossRef]
- Bae, Y. Comparison of Postural Sway, Plantar Cutaneous Sensation According to Saccadic Eye Movement Frequency in Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 7067. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, S.A.; Polastri, P.F.; Godoi, D.; Moraes, R.; Barela, J.A.; Rodrigues, S.T. Effects of saccadic eye movements on postural control in older adults. Psychol. Neurosci. 2015, 8, 19. [Google Scholar] [CrossRef]
- Bae, Y. Saccadic eye movement improves plantar sensation and postural balance in elderly women. Tohoku J. Exp. Med. 2016, 239, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerraz, M.; Bronstein, A. Ocular versus extraocular control of posture and equilibrium. Neurophysiol. Clin./Clin. Neurophysiol. 2008, 38, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y. Decreased Saccadic Eye Movement Speed Correlates with Dynamic Balance in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 7842. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.T.; Polastri, P.F.; Carvalho, J.C.; Barela, J.A.; Moraes, R.; Barbieri, F.A. Saccadic and smooth pursuit eye movements attenuate postural sway similarly. Neurosci. Lett. 2015, 584, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liang, Y.-Y.; Wang, L.; Sheng, J.; Ma, S.-J. Reliability and validity of center of pressure measures for balance assessment in older adults. J. Phys. Ther. Sci. 2016, 28, 1364–1367. [Google Scholar] [CrossRef] [PubMed]
- Kalron, A.; Achiron, A. Postural control, falls and fear of falling in people with multiple sclerosis without mobility aids. J. Neurol. Sci. 2013, 335, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A. When to use the B onferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Bakeman, R. Recommended effect size statistics for repeated measures designs. Behav. Res. Methods 2005, 37, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Kumar, C. The patient who falls:“It’s always a trade-off”. JAMA 2010, 303, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.-H.; Ong, P.-H.; Clark, R.A.; Matcher, D.B.; Lim, E.C.-W. Falls efficacy, postural balance, and risk for falls in older adults with falls-related emergency department visits: Prospective cohort study. BMC Geriatr. 2017, 17, 1–7. [Google Scholar] [CrossRef]
- Muir, J.W.; Kiel, D.P.; Hannan, M.; Magaziner, J.; Rubin, C.T. Dynamic parameters of balance which correlate to elderly persons with a history of falls. PLoS ONE 2013, 8, e70566. [Google Scholar] [CrossRef] [PubMed]
- Colledge, N.; Cantley, P.; Peaston, I.; Brash, H.; Lewis, S.; Wilson, J. Ageing and balance: The measurement of spontaneous sway by posturography. Gerontology 1994, 40, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E.; Holliday, P.J.; Fernie, G.R. Aging and postural control: A comparison of spontaneous-and induced-sway balance tests. J. Am. Geriatr. Soc. 1990, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Visser, J.E.; Carpenter, M.G.; van der Kooij, H.; Bloem, B.R. The clinical utility of posturography. Clin. Neurophysiol. 2008, 119, 2424–2436. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.M.; Bampouras, T.M.; Donovan, T.; Dewhurst, S. Eye movements affect postural control in young and older females. Front. Aging Neurosci. 2016, 8, 216. [Google Scholar] [CrossRef] [PubMed]
- Raffi, M.; Piras, A.; Persiani, M.; Perazzolo, M.; Squatrito, S. Angle of gaze and optic flow direction modulate body sway. J. Electromyogr. Kinesiol. 2017, 35, 61–68. [Google Scholar] [CrossRef]
- Aoki, M.; Nishihori, T.; Jiang, Y.; Nagasaki, S.; Wakaoka, T.; Ito, Y. Damping control of balance in the medial/lateral direction and the risk of falling in the elderly. Geriatr. Gerontol. Int. 2013, 13, 182–189. [Google Scholar] [CrossRef]
- Park, J.W.; Jung, M.; Kweon, M. The mediolateral CoP parameters can differentiate the fallers among the community-dwelling elderly population. J. Phys. Ther. Sci. 2014, 26, 381–384. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Faller (n = 58) | Non-Faller (n = 94) | t | p | 95% CI |
|---|---|---|---|---|---|
| Age (years) | 77.10 ± 6.11 a | 75.71 ± 5.84 | 1.400 | 0.142 | 1.391 (−0.573~3.354) |
| Height (cm) | 151.76 ± 6.17 | 152.98 ± 16.34 | −0.547 | 0.585 | −1.224 (−5.652~3.203) |
| Weight (Kg) | 58.75 ± 9.19 | 61.60 ± 10.79 | −1.668 | 0.097 | −2.846 (−6.217~0.524) |
| Sex (male/female) | 10/48 | 19/75 | |||
| K-MMSE b (score) | 25.91 ± 3.01 | 26.35 ± 2.50 | −0.944 | 0.347 | −0.441 (−1.364~0.482) |
| Number of falls | 1.78 ± 1.09 | 0 | 14.434 | <0.001 | 1.778 (1.534~2.022) |
| Postural sway of baseline | |||||
| CoP c path length (mm) | 244.42 ± 188.59 | 241.81 ± 188.35 | |||
| CoPvelocity (mm/s) | 16.20 ± 11.71 | 16.32 ± 13.18 | |||
| CoPmedlateral length (mm) | 10.56 ± 11.61 | 10.44 ± 9.79 | |||
| CoPanteroposteiror length (mm) | 21.68 ± 12.56 | 21.89 ± 10.71 | |||
| Variable | SEM Speed | Faller (n = 58) | Non-Faller (n = 94) | Group * Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | F | p a | Mean ± SD | F | p a | F | p b | η2 | ||
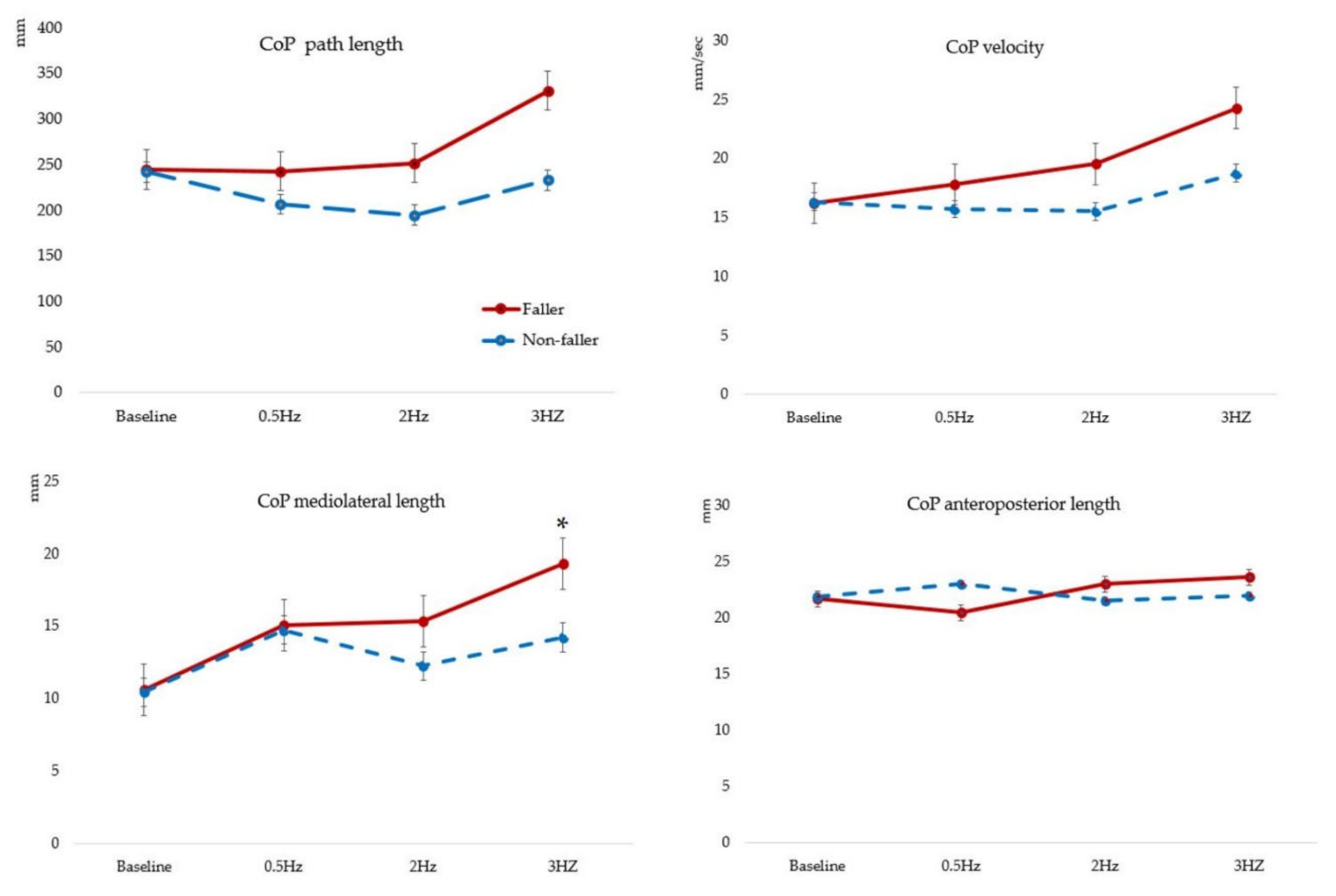
| CoPpath length (mm) | Baseline | 244.42 ± 188.59 | 3.389 | 0.019 | 241.81 ± 188.35 | 0.308 | 0.580 | 2.096 | 0.104 | 0.014 |
| 0.5 Hz | 242.38 ± 177.47 | 206.29 ± 138.37 | ||||||||
| 2 Hz | 251.50 ± 227.14 | 194.64 ± 138.37 †† | ||||||||
| 3 HZ | 331.03 ± 225.81 *†‡ | 232.93 ± 185.66 | ||||||||
| CoPvelocity (mm/sec) | Baseline | 16.20 ± 11.71 | 2.736 | 0.045 | 16.32 ± 13.18 | 0.884 | 0.450 | 0.883 | 0.433 | 0.006 |
| 0.5 Hz | 17.79 ± 12.70 | 15.69 ± 15.56 | ||||||||
| 2 Hz | 19.53 ± 16.49 | 15.51 ± 14.69 | ||||||||
| 3 HZ | 24.27 ± 27.33 ‡ | 18.73 ± 22.45 | ||||||||
| CoPmedlateral length (mm) | Baseline | 10.56 ± 11.61 | 6.821 | <0.001 | 10.44 ± 9.79 | 3.387 | 0.019 | 3.108 | 0.026 | 0.020 |
| 0.5 Hz | 15.04 ± 12.53 ** | 14.71 ± 16.00 ** | ||||||||
| 2 Hz | 15.31 ± 13.40 †† | 12.23 ± 11.89 | ||||||||
| 3 HZ | 19.28 ± 14.75 ‡ | 14.21 ± 12.14 * | ||||||||
| CoPanteroposteiror length (mm) | Baseline | 21.68 ± 12.56 | 1.514 | 0.213 | 21.89 ± 10.71 | 0.311 | 0.817 | 1.287 | 0.278 | 0.009 |
| 0.5 Hz | 20.46 ± 11.72 | 22.99 ± 15.34 | ||||||||
| 2 Hz | 23.00 ± 11.75 | 21.48 ± 11.10 | ||||||||
| 3 HZ | 23.59 ± 15.26 | 21.93 ± 15.46 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.; Lee, S.; Bae, Y. Fast Saccadic Eye Movements Contribute to the Worsened Postural Sway in Older Adults Who Have Experienced Falls. Healthcare 2022, 10, 1708. https://doi.org/10.3390/healthcare10091708
Lee C, Lee S, Bae Y. Fast Saccadic Eye Movements Contribute to the Worsened Postural Sway in Older Adults Who Have Experienced Falls. Healthcare. 2022; 10(9):1708. https://doi.org/10.3390/healthcare10091708
Chicago/Turabian StyleLee, Changjoon, Subin Lee, and Youngsook Bae. 2022. "Fast Saccadic Eye Movements Contribute to the Worsened Postural Sway in Older Adults Who Have Experienced Falls" Healthcare 10, no. 9: 1708. https://doi.org/10.3390/healthcare10091708
APA StyleLee, C., Lee, S., & Bae, Y. (2022). Fast Saccadic Eye Movements Contribute to the Worsened Postural Sway in Older Adults Who Have Experienced Falls. Healthcare, 10(9), 1708. https://doi.org/10.3390/healthcare10091708