
Experiences, Perceptions, and Coping Patterns of Emergency Department Nurses with Occupational Stressors in Saudi Arabian Hospitals: Mixed-Method Study


Abstract
:1. Introduction
2. Materials and Methods
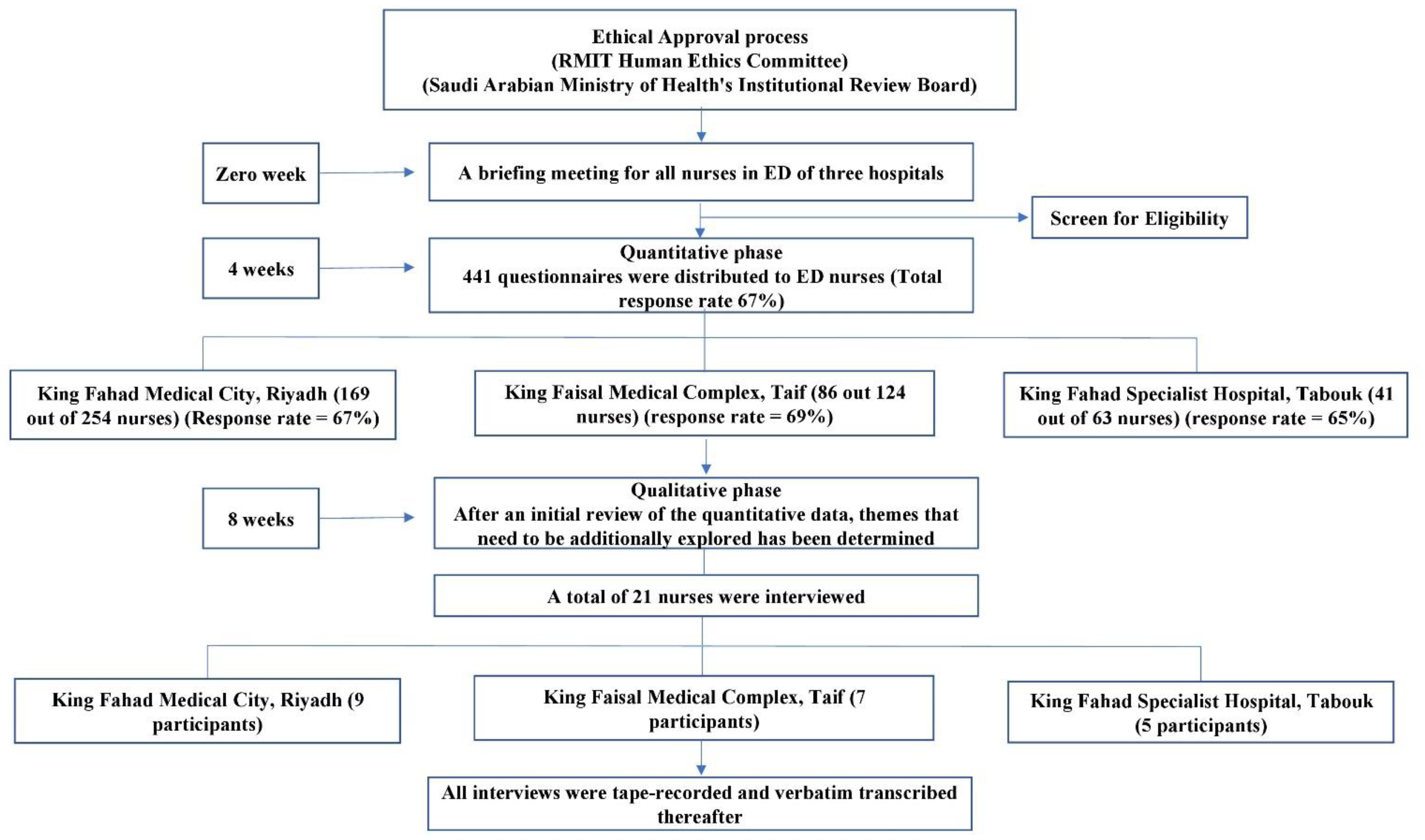
2.1. Study Design and Patients
2.2. Sampling and Setting
2.3. Instrument
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Quantitative Results
3.1.1. Socio-Demographic Attributes of Participants
3.1.2. Occupational Sources of Stress among Emergency Department Nurses
3.1.3. Perceptions and Experience of Stress
3.1.4. Coping with Stress
3.2. Qualitative Results
4. Discussion
4.1. Strengths and Limitations
4.2. Implications to Nursing Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van der Linden, M. The International Labour Organization, 1919–2019: An Appraisal. Labor 2019, 16, 11–41. [Google Scholar] [CrossRef]
- Stress, I.W. A Collective Challenge; International Labour Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- Brand, S.L.; Coon, J.T.; Fleming, L.E.; Carroll, L.; Bethel, A.; Wyatt, K. Whole-system approaches to improving the health and wellbeing of healthcare workers: A systematic review. PLoS ONE 2017, 12, e0188418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshaabani, A.; Hamza, K.A.; Rudnák, I. Impact of Diversity Management on Employees’ Engagement: The Role of Organizational Trust and Job Insecurity. Sustainability 2022, 14, 420. [Google Scholar] [CrossRef]
- Coetzee, S.K.; Klopper, H.C.; Ellis, S.M.; Aiken, L.H. A tale of two systems—Nurses practice environment, well being, perceived quality of care and patient safety in private and public hospitals in South Africa: A questionnaire survey. Int. J. Nurs. Stud. 2013, 50, 162–173. [Google Scholar] [CrossRef]
- Gonçalves, A.; Fontes, L.; Simães, C.; Gomes, A.R. Stress and burnout in health professionals. In Occupational and Environmental Safety and Health; Springer: Berlin/Heidelberg, Germany, 2019; pp. 563–571. [Google Scholar]
- Clark, P.F.; Stewart, J.B.; Clark, D.A. The globalization of the labour market for health-care professionals. Int. Labour Rev. 2006, 145, 37. [Google Scholar] [CrossRef]
- Chiang, Y.-M.; Chang, Y. Stress, depression, and intention to leave among nurses in different medical units: Implications for healthcare management/nursing practice. Health Policy 2012, 108, 149–157. [Google Scholar] [CrossRef]
- Chang, H.Y.; Shyu, Y.I.L.; Wong, M.K.; Friesner, D.; Chu, T.L.; Teng, C.I. Which aspects of professional commitment can effectively retain nurses in the nursing profession? J. Nurs. Scholarsh. 2015, 47, 468–476. [Google Scholar] [CrossRef]
- Kamal, S.M.; Al-Dhshan, M.; Abu-Salameh, K.; Abuadas, F.; Hassan, M. The effect of nurses’ perceived job related stressors on job satisfaction in Taif governmental hospitals in Kingdom of Saudi Arabia. J. Am. Sci. 2012, 8, 119–125. [Google Scholar]
- Islam, M.I.; Alam, K.M.W.; Keramat, S.A.; Murshid, M.E.; Haque, R.; Kabir, E.; Khanam, R.; Khan, M.H. Working conditions and occupational stress among nurses in Bangladesh: A cross-sectional pilot study. J. Public Health 2021, 1–9. [Google Scholar] [CrossRef]
- Moustaka, E.; Constantinidis, T.C. Sources and effects of work-related stress in nursing. Health Sci. J. 2010, 4, 210. [Google Scholar]
- Banovcinova, L.; Baskova, M. Sources of work-related stress and their effect on burnout in midwifery. Procedia-Soc. Behav. Sci. 2014, 132, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Nagata, T.; Mori, K.; Ohtani, M.; Nagata, M.; Kajiki, S.; Fujino, Y.; Matsuda, S.; Loeppke, R. Total health-related costs due to absenteeism, presenteeism, and medical and pharmaceutical expenses in Japanese employers. J. Occup. Environ. Med. 2018, 60, e273. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.L.; White-Means, S.I.; Wicks, M.N.; Chang, C.F.; Gourley, D.; Rice, M. Cost burden of the presenteeism health outcome: Diverse workforce of nurses and pharmacists. J. Occup. Environ. Med. 2011, 53, 90–99. [Google Scholar] [CrossRef]
- Shan, G.; Wang, S.; Wang, W.; Guo, S.; Li, Y. Presenteeism in nurses: Prevalence, consequences, and causes from the perspectives of nurses and chief nurses. Front. Psychiatry 2021, 11, 584040. [Google Scholar] [CrossRef] [PubMed]
- Romppanen, J.; Häggman-Laitila, A. Interventions for nurses’ well-being at work: A quantitative systematic review. J. Adv. Nurs. 2017, 73, 1555–1569. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.; Irvine, F.; Wallymahmed, A. Personality, stress and coping in intensive care nurses: A descriptive exploratory study. Nurs. Crit. Care 2010, 15, 129–140. [Google Scholar] [CrossRef]
- Kennedy, B.; Curtis, K.; Waters, D. Is there a relationship between personality and choice of nursing specialty: An integrative literature review. BMC Nurs. 2014, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.; Bogossian, F.; Ahern, K. Stress and coping in Australian nurses: A systematic review. Int. Nurs. Rev. 2010, 57, 22–31. [Google Scholar] [CrossRef]
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work related stress, burnout, job satisfaction and general health of nurses. Int. J. Environ. Res. 2015, 12, 652–666. [Google Scholar] [CrossRef]
- Wang, W.; Kong, A.W.M.; Chair, S.Y. Relationship between job stress level and coping strategies used by Hong Kong nurses working in an acute surgical unit. Appl. Nurs. Res. 2011, 24, 238–243. [Google Scholar] [CrossRef]
- Lu, D.-M.; Sun, N.; Hong, S.; Fan, Y.-Y.; Kong, F.-Y.; Li, Q.-J. Occupational stress and coping strategies among emergency department nurses of China. Arch. Psychiatr. Nurs. 2015, 29, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Yuwanich, N.; Akhavan, S.; Nantsupawat, W.; Martin, L. Experiences of occupational stress among emergency nurses at private hospitals in Bangkok, Thailand. Open J. Nurs. 2017, 7, 657–670. [Google Scholar] [CrossRef] [Green Version]
- Al-Nuaimi, H.; ALBashtawy, M.; Qaddumi, J.; Baqir, M.; Suliman, M.; Abdalrahim, A.; Alkhawaldeh, A. Impact of Occupational Stress on Nurses’ Job Performance According to Nurses Perception. Med. Leg. Update 2021, 21, 252–255. [Google Scholar]
- Hogan, K.-A.; Fothergill-Bourbonnais, F.; Brajtman, S.; Phillips, S.; Wilson, K.G. When someone dies in the emergency department: Perspectives of emergency nurses. J. Emerg. Nurs. 2016, 42, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Alosaimi, F.D.; Kazim, S.N.; Almufleh, A.S.; Aladwani, B.S.; Alsubaie, A.S. Prevalence of stress and its determinants among residents in Saudi Arabia. Saudi Med. J. 2015, 36, 605–612. [Google Scholar] [CrossRef]
- Al Aseeri, M.R.M. Perceived Challenges of Working Environment Among Emergency Department Nurses in Saudi Arabia. J. Biol. Agric. Healthc. 2020, 10, 25–31. [Google Scholar]
- AlYami, M.S.; Watson, R. An overview of nursing in Saudi Arabia. J. Health Spec. 2014, 2, 10–12. [Google Scholar] [CrossRef]
- Lamadah, S.M.; Sayed, H.Y. Challenges facing nursing profession in Saudi Arabia. J. Biol. Agric. Healthc. 2014, 4, 20–25. [Google Scholar]
- Said, R.M.; El-Shafei, D.A. Occupational stress, job satisfaction, and intent to leave: Nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ. Sci. Pollut. Res. 2021, 28, 8791–8801. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Balducci, C.; Romeo, L.; Brondino, M.; Lazzarini, G.; Benedetti, F.; Toderi, S.; Fraccaroli, F.; Pasini, M. The validity of the short UK health and safety executive stress indicator tool for the assessment of the psychosocial work environment in Italy. Eur. J. Psychol. Assess. 2017, 33, 149–157. [Google Scholar] [CrossRef]
- McCoy, M.M. Sources of Stress and Coping Among Emergency Department Nurses; Gonzaga University: Spokane, WA, USA, 1997. [Google Scholar]
- Adriaenssens, J.; De Gucht, V.; Maes, S.J. Causes and consequences of occupational stress in emergency nurses, a longitudinal study. J. Nurs. Manag. 2015, 23, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Raeissi, P.; Raoofi, S.; Soltani, A.; Sokhanvar, M.; Visentin, D.C.; Cleary, M. Occupational stress and associated risk factors among nurses: A cross-sectional study. Contemp. Nurse 2019, 55, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Gong, Y.H. Relationship between occupational stress and coping strategy among operating theatre nurses in C hina: A questionnaire survey. J. Nurs. Manag. 2015, 23, 96–106. [Google Scholar] [CrossRef]
- Godwin, A.; Suuk, L.A.; Selorm, F.H. Occupational stress and its management among nurses at St. Dominic Hospital, Akwatia, Ghana. Health Sci. J. 2016, 10, 1. [Google Scholar] [CrossRef]
- Glazer, S.; Gyurak, A. Sources of occupational stress among nurses in five countries. Int. J. Intercult. Relat. 2008, 32, 49–66. [Google Scholar] [CrossRef]
- Jones, G.; Hocine, M.; Salomon, J.; Dab, W.; Temime, L. Demographic and occupational predictors of stress and fatigue in French intensive-care registered nurses and nurses’ aides: A cross-sectional study. Int. J. Nurs. Stud. 2015, 52, 250–259. [Google Scholar] [CrossRef]
- Stimpfel, A.W.; Brewer, C.S.; Kovner, C.T. Scheduling and shift work characteristics associated with risk for occupational injury in newly licensed registered nurses: An observational study. Int. J. Nurs. Stud. 2015, 52, 1686–1693. [Google Scholar] [CrossRef]
- Almajwal, A.M. Stress, shift duty, and eating behavior among nurses in Central Saudi Arabia. Saudi Med. J. 2016, 37, 191–198. [Google Scholar] [CrossRef]
- Al-Makhaita, H.M.; Sabra, A.A.; Hafez, A.S. Predictors of work-related stress among nurses working in primary and secondary health care levels in Dammam, Eastern Saudi Arabia. J. Fam. Community Med. 2014, 21, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Almalki, M.J.; FitzGerald, G.; Clark, M. The relationship between quality of work life and turnover intention of primary health care nurses in Saudi Arabia. BMC Health Serv. Res. 2012, 12, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connor, J.B.; Miller, A.M. Occupational stress and adaptation of immigrant nurses from the Philippines. J. Res. Nurs. 2014, 19, 504–515. [Google Scholar] [CrossRef]
- Yim, H.-Y.; Seo, H.-J.; Cho, Y.; Kim, J. Mediating role of psychological capital in relationship between occupational stress and turnover intention among nurses at veterans administration hospitals in Korea. Asian Nurs. Res. 2017, 11, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ríos-Risquez, M.I.; García-Izquierdo, M. Patient satisfaction, stress and burnout in nursing personnel in emergency departments: A cross-sectional study. Int. J. Nurs. Stud. 2016, 59, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Wu, Q.; Zhu, X.; Shi, Y. Improving sleep quality relieves occupational stress in nurses of cardiac surgical intensive care unit. Biomed. Res. Tokyo 2017, 28, 3934–3940. [Google Scholar]
- Khammar, A.; Amjad, R.; Rohani, M.; Yari, A.; Noroozi, M.; Poursadeghian, A.; Hami, M.; Poursadeghiyan, M. Survey of shift work disorders and occupational stress among nurses: A cross-sectional study. Ann. Trop. Med. Public Health 2017, 10, 978–984. [Google Scholar]
- Nielsen, K.J.; Pedersen, A.H.; Rasmussen, K.; Pape, L.; Mikkelsen, K.L. Work-related stressors and occurrence of adverse events in an ED. Am. J. Emerg. Med. 2013, 31, 504–508. [Google Scholar] [CrossRef]
- McCarthy, V.J.; Power, S.; Greiner, B.A. Perceived occupational stress in nurses working in Ireland. Occup. Med. 2010, 60, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Mark, G.; Smith, A.P. Occupational stress, job characteristics, coping, and the mental health of nurses. Br. J. Health Psychol. 2012, 17, 505–521. [Google Scholar] [CrossRef]
- Tajvar, A.; Saraji, G.N.; Ghanbarnejad, A.; Omidi, L.; Hosseini, S.S.S.; Abadi, A.S.S. Occupational stress and mental health among nurses in a medical intensive care unit of a general hospital in Bandar Abbas in 2013. Electron. Physician 2015, 7, 1108–1113. [Google Scholar]
- Wu, H.; Sun, W.; Wang, L. Factors associated with occupational stress among Chinese female emergency nurses. Emerg. Med. J. 2012, 29, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Crilly, J.; Greenslade, J.; Lincoln, C.; Timms, J.; Fisher, A. Measuring the impact of the working environment on emergency department nurses: A cross-sectional pilot study. Int. Emerg. Nurs. 2017, 31, 9–14. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Section | Domain | Author | Description | Items |
|---|---|---|---|---|
| 1 | Sociodemographic characteristics | Developed by researcher | Close-ended multiple-choice and Yes/No questions | 9 |
| 2 | Sources of Stress | Adapted from Lu, Sun, Hong, Fan, Kong and Li [23], and Moustaka and Constantinidis [12] | 57 items were measured on a 7-point Likert scale, subdivided into five domains: | 57 |
| a. specialty and work (13 items) | ||||
| b. workload (8 items) | ||||
| c. working conditions and resources (12 items) | ||||
| d. patient care (12 items) | ||||
| e. management and interpersonal relationships (12 items) | ||||
| 3 | Perception of stress | Adapted from Perceived Stress Scale by Cohen, et al. [33] | 10 items measured on a 5-point Likert scale (4 = very often, 3 = fairly often, 2 = sometimes, 1 = amost never, and 0 = never) | 10 |
| 4 | Coping methods | Adapted from Balducci, et al. [34] and McCoy [35] | Open-ended, fill in the blanks, close-ended multiple choice questions | 9 |
| Variables | n | % |
|---|---|---|
| Age | ||
| 20–29 | 151 | 51 |
| 30–39 | 114 | 38.5 |
| >40 | 31 | 10.5 |
| Gender | ||
| Female | 265 | 89.5 |
| Male | 22 | 7.4 |
| Prefer not to say | 9 | 3.1 |
| Educational level | ||
| Diploma | 43 | 14.5 |
| Bachelor’s degree | 245 | 82.8 |
| Master’s degree | 8 | 2.7 |
| Nationality | ||
| Saudis | 50 | 16.9 |
| Filipino | 118 | 39.8 |
| Indian | 122 | 41.2 |
| Pakistani | 2 | 0.7 |
| others | 4 | 1.4 |
| Marital Status | ||
| Single/Divorced | 151 | 51 |
| Married | 145 | 49 |
| Do you have children | ||
| Yes | 121 | 40.9 |
| No | 175 | 59.1 |
| General Nursing Work Experience | ||
| Less than 2 years | 24 | 8.1 |
| 2–6 years | 135 | 45.6 |
| 7–10 years | 95 | 32.1 |
| >11 years | 42 | 14.2 |
| ED Work Experience | ||
| Less than 2 years | 124 | 41.9 |
| 2–6 years | 108 | 36.5 |
| 7–10 years | 50 | 16.9 |
| >11 years | 14 | 4.7 |
| Items | Total Rating | Mean | Rank |
|---|---|---|---|
| Excessive amount of paper work | 1155 | 3.90 | 1st |
| Staff shortage | 1134 | 3.83 | 2nd |
| Feeling tired on shift | 1060 | 3.58 | 3rd |
| Providing Care for many patients | 1049 | 3.54 | 4th |
| Adequate Payment and reward | 1029 | 3.48 | 5th |
| Last five items | |||
| Worry about any nursing procedures that may cause the pain | 576 | 1.95 | |
| Accomplishment of my job-related goals | 549 | 1.85 | |
| relationship with other nurses in this department is adversely affected my job | 548 | 1.85 | |
| I like the people I work with | 511 | 1.73 | |
| lack the skills/knowledge to provide effective patients education | 509 | 1.72 |
| Nurse Specialty and Work | Workload and Time Assignment | Working Conditions and Resources | Patient Care | Management and Interpersonal Relationships | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants Attributes | L | M | H | L | M | H | L | M | H | L | M | H | L | M | H | |
| Gender | Male | 5 | 15 | 2 | 4 | 11 | 7 | 5 | 12 | 5 | 3 | 13 | 6 | 9 | 10 | 3 |
| Female | 78 | 146 | 41 | 59 | 100 | 106 | 86 | 136 | 43 | 107 | 123 | 35 | 142 | 98 | 25 | |
| ρ (rs) = 0.04 | ρ (rs) = 0.02 | ρ (rs) = 0.057 | ρ (rs) = 0.11 | ρ (rs) = 0.11 | ||||||||||||
| Marital Status | Single/divorced | 37 | 88 | 26 | 29 | 60 | 62 | 38 | 87 | 26 | 48 | 82 | 21 | 75 | 63 | 13 |
| Married | 47 | 79 | 19 | 34 | 57 | 54 | 55 | 66 | 24 | 65 | 59 | 21 | 80 | 50 | 15 | |
| ρ (rs) = −0.08 | ρ (rs) = −0.078 | ρ (rs) = −0.13 * | ρ (rs)= −0.09 | ρ (rs) = −0.02 | ||||||||||||
| Age | 20–29 | 39 | 86 | 26 | 27 | 58 | 66 | 44 | 82 | 25 | 57 | 72 | 22 | 76 | 60 | 15 |
| 30–39 | 35 | 65 | 14 | 30 | 47 | 37 | 40 | 56 | 18 | 47 | 54 | 13 | 60 | 44 | 10 | |
| >40 | 10 | 16 | 5 | 6 | 12 | 13 | 9 | 15 | 7 | 9 | 15 | 7 | 19 | 9 | 3 | |
| ρ (rs) = −0.05 | ρ (rs) = −0.06 | ρ (rs) = 0.001 | ρ (rs) = 0.04 | ρ (rs) = 0.05 | ||||||||||||
| Level of education | Diploma | 22 | 19 | 2 | 19 | 12 | 12 | 25 | 14 | 4 | 27 | 12 | 4 | 32 | 9 | 2 |
| Bachelor | 61 | 141 | 43 | 43 | 102 | 100 | 67 | 132 | 46 | 82 | 126 | 37 | 117 | 102 | 26 | |
| Master | 1 | 7 | 0 | 1 | 3 | 4 | 1 | 7 | 0 | 4 | 3 | 1 | 6 | 2 | 0 | |
| ρ (rs) = 0.19 ** | ρ (rs) = 0.18 ** | ρ (rs) = 0.19 ** | ρ (rs) = 0.14 * | ρ (rs) = 0.12 * | ||||||||||||
| General Nursing Work Experience | ˂2 years | 11 | 6 | 7 | 6 | 12 | 6 | 8 | 13 | 3 | 8 | 12 | 4 | 12 | 10 | 2 |
| 2–6 years | 34 | 82 | 19 | 23 | 50 | 62 | 38 | 74 | 23 | 50 | 65 | 20 | 69 | 49 | 17 | |
| 7–10 years | 26 | 54 | 15 | 21 | 40 | 34 | 29 | 47 | 19 | 33 | 49 | 13 | 45 | 42 | 8 | |
| >11 years | 13 | 25 | 4 | 13 | 15 | 14 | 18 | 19 | 5 | 22 | 15 | 5 | 29 | 12 | 1 | |
| ρ (rs) = −0.03 | ρ (rs) = −0.07 | ρ (rs) = −0.05 | ρ (rs) = −0.08 | ρ (rs) = −0.10 | ||||||||||||
| ED Work Experience | ˂2 years | 44 | 64 | 16 | 29 | 48 | 47 | 64 | 63 | 15 | 58 | 53 | 13 | 71 | 44 | 9 |
| 2–6 years | 27 | 65 | 16 | 26 | 40 | 42 | 31 | 53 | 24 | 40 | 51 | 17 | 56 | 39 | 13 | |
| 7–10 years | 10 | 29 | 11 | 7 | 23 | 20 | 12 | 30 | 8 | 10 | 31 | 9 | 20 | 24 | 6 | |
| >11 years | 3 | 9 | 2 | 1 | 6 | 7 | 4 | 7 | 3 | 5 | 6 | 3 | 8 | 6 | 0 | |
| ρ (rs) = 0.13 * | ρ (rs) = 0.08 | ρ (rs) = 0.10 | ρ (rs) = 0.17 ** | ρ (rs) = 0.07 | ||||||||||||
| In the Last Month, How Often Have You | Never, % (n) | Almost Never, % (n) | Sometimes, % (n) | Fairly Often, % (n) | Very Often, % (n) |
| been upset because of something that happened unexpectedly | 41(13.9) | 62(20.9) | 95(32.1) | 60(20.3) | 38(12.8) |
| felt that you were unable to control the important things in your life? | 43(14.5) | 68(23.0) | 108(36.5) | 50(16.9) | 27(9.1) |
| felt nervous and “stressed”? | 27(9.1) | 36(12.2) | 104(35.1) | 74(25.0) | 55(18.5) |
| felt confident about your ability to handle your personal problems? | 36(12.2) | 47(15.9) | 103(34.8) | 70(23.6) | 40(13.5) |
| felt that things were not going your way? | 35(11.8) | 44(14.9) | 134(45.3) | 60(20.3) | 23(7.7) |
| found that you could not cope with all the things that you had to do? | 52(17.6) | 56(18.9) | 117(39.5) | 50(16.9) | 21(7.1) |
| been able to control irritations in your life? | 28(9.5) | 49(16.6) | 125(42.2) | 72(24.3) | 22(7.4) |
| felt that you were on top of things? | 54(18.2) | 54(18.2) | 124(41.9) | 49(16.9) | 15(5.1) |
| been angered because of things that were outside of your control? | 41(13.9) | 58(19.6) | 104(35.1) | 64(21.6) | 29(9.8) |
| felt difficulties were piling up so high that you could not overcome them? | 39(13.2) | 64(21.6) | 112(37.8) | 55(18.6) | 26(8.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alruwaili, M.M.; Abuadas, F.H.; Maude, P.; Ross, A. Experiences, Perceptions, and Coping Patterns of Emergency Department Nurses with Occupational Stressors in Saudi Arabian Hospitals: Mixed-Method Study. Healthcare 2022, 10, 1504. https://doi.org/10.3390/healthcare10081504
Alruwaili MM, Abuadas FH, Maude P, Ross A. Experiences, Perceptions, and Coping Patterns of Emergency Department Nurses with Occupational Stressors in Saudi Arabian Hospitals: Mixed-Method Study. Healthcare. 2022; 10(8):1504. https://doi.org/10.3390/healthcare10081504
Chicago/Turabian StyleAlruwaili, Majed M., Fuad H. Abuadas, Phillip Maude, and Alistair Ross. 2022. "Experiences, Perceptions, and Coping Patterns of Emergency Department Nurses with Occupational Stressors in Saudi Arabian Hospitals: Mixed-Method Study" Healthcare 10, no. 8: 1504. https://doi.org/10.3390/healthcare10081504
APA StyleAlruwaili, M. M., Abuadas, F. H., Maude, P., & Ross, A. (2022). Experiences, Perceptions, and Coping Patterns of Emergency Department Nurses with Occupational Stressors in Saudi Arabian Hospitals: Mixed-Method Study. Healthcare, 10(8), 1504. https://doi.org/10.3390/healthcare10081504