
Dysbiosis: A Potential Precursor to the Development of a Depressive Disorder



Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
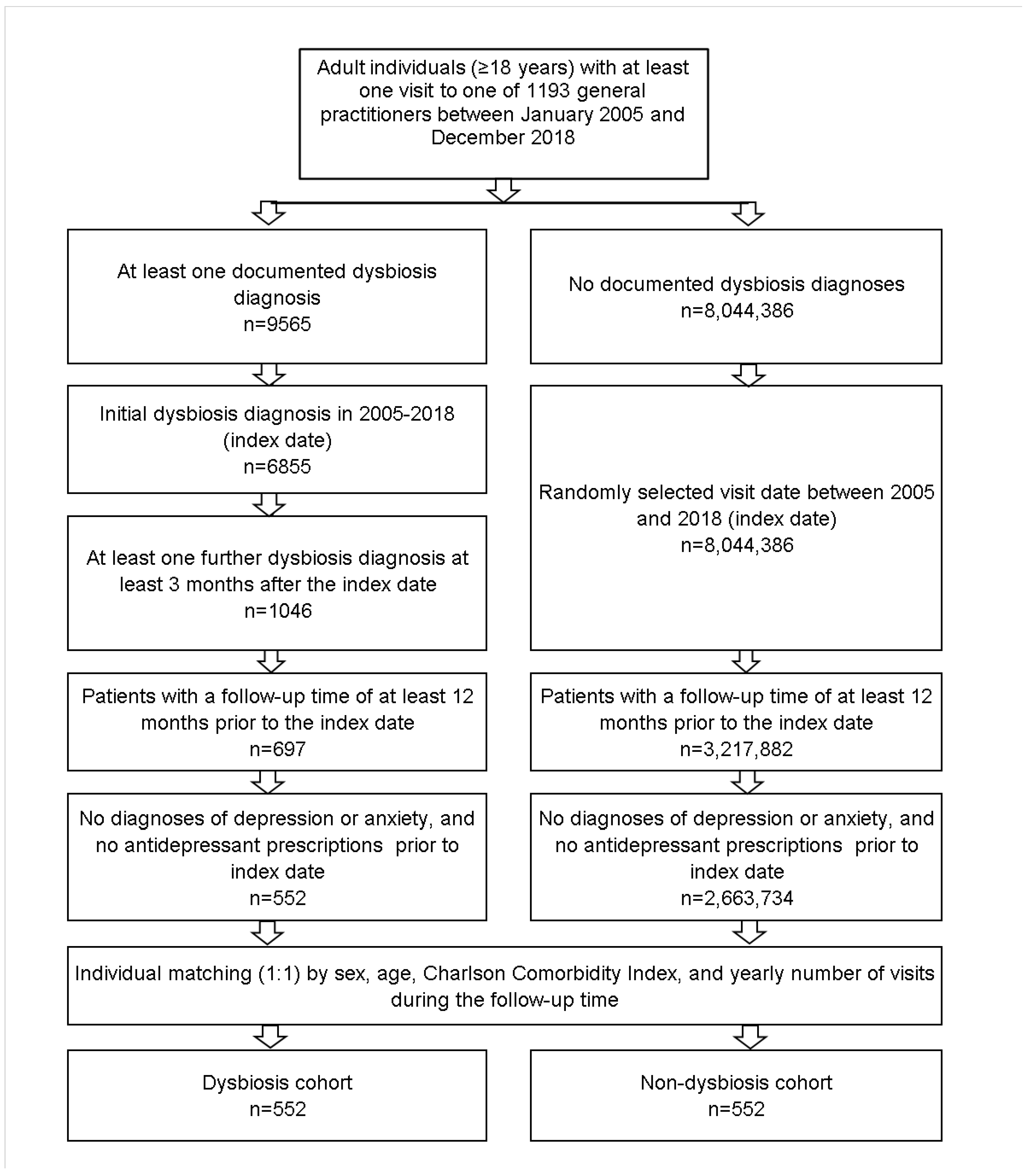
2.2. Study Population
2.3. Study Outcomes and Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
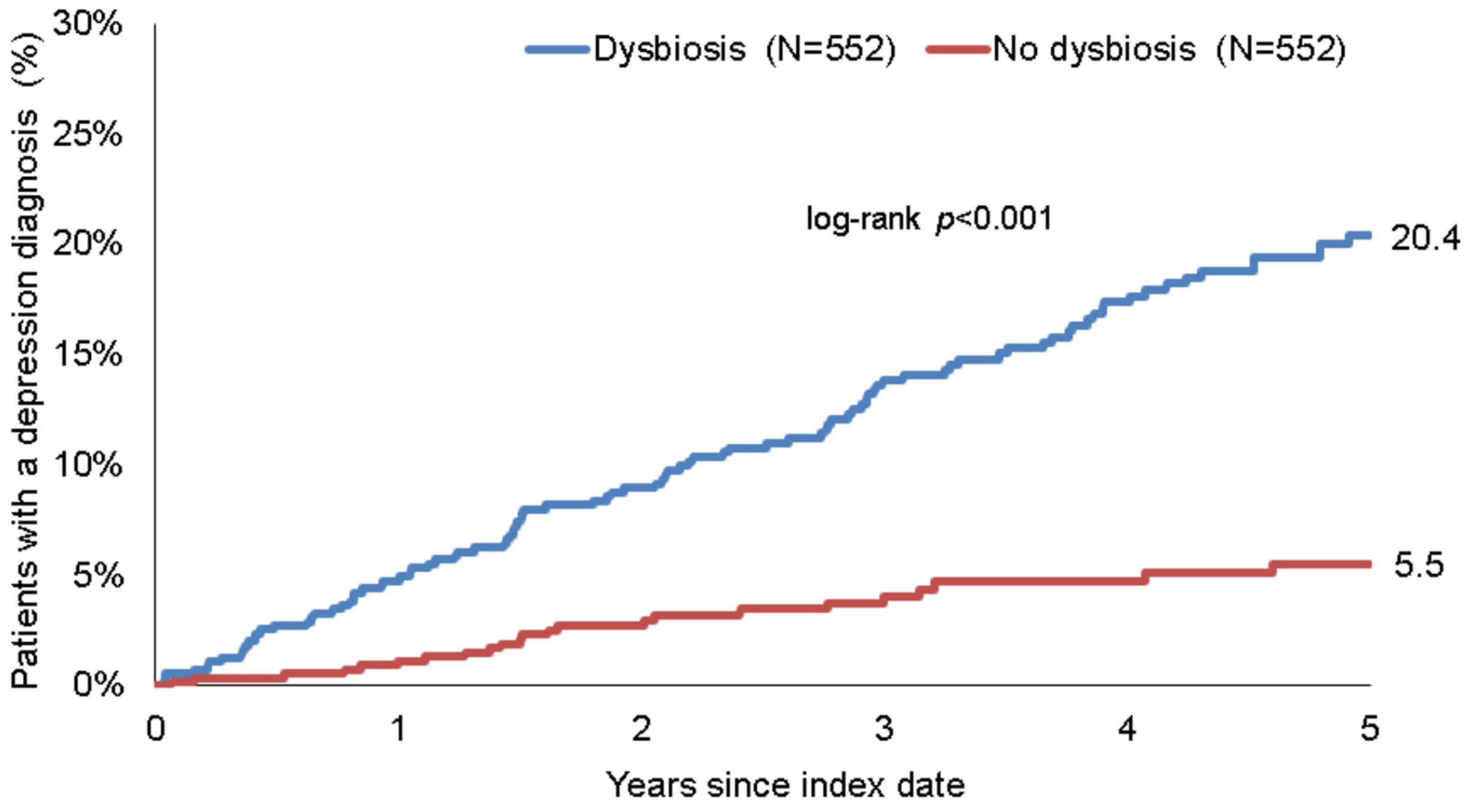
3.2. Association between Dysbiosis and Depression
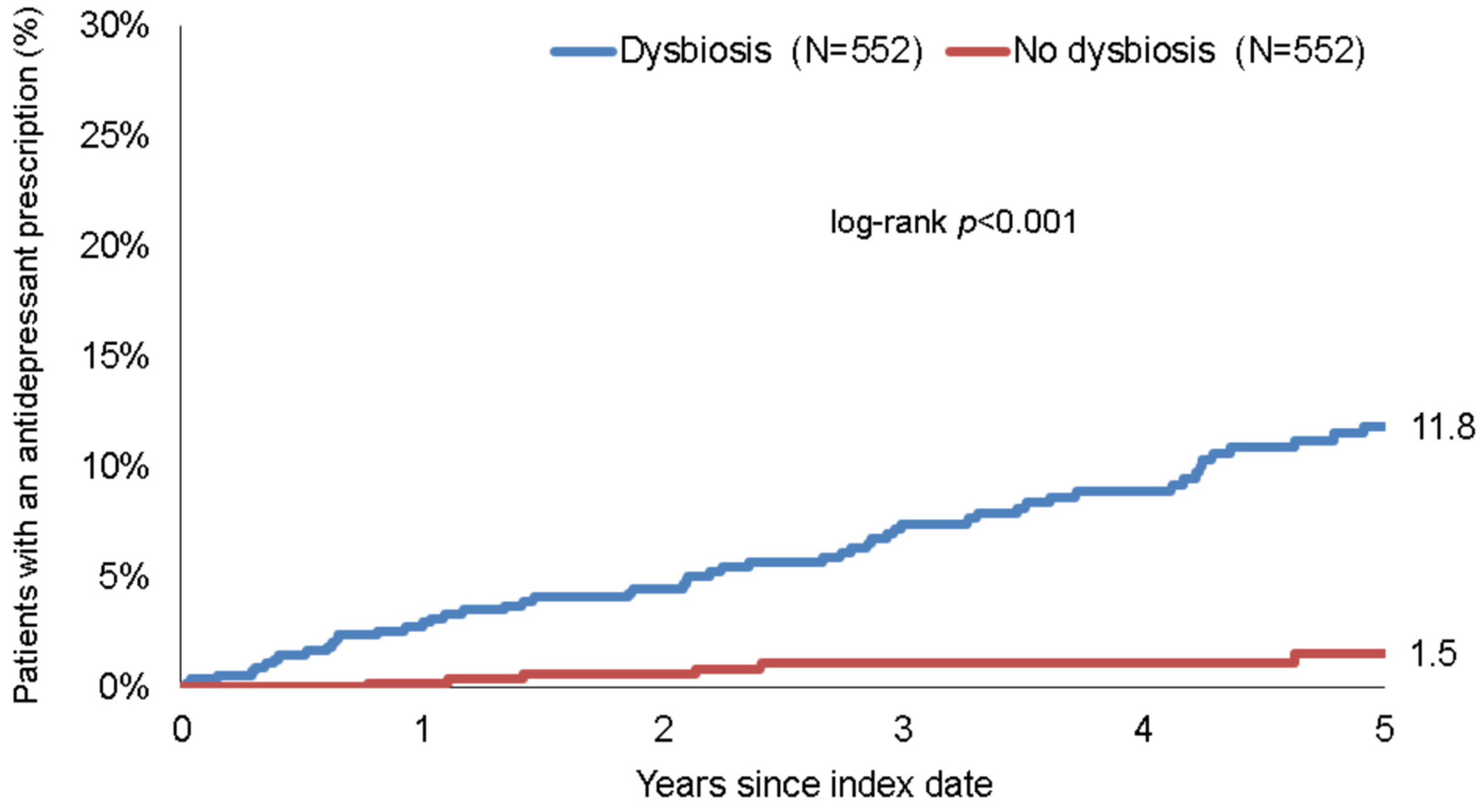
3.3. Association between Dysbiosis and Prescription of Antidepressant Drugs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, X.; Li, P.; Liu, M.; Zheng, H.; He, Y.; Chen, M.-X.; Tang, W.; Yue, X.; Huang, Y.; Zhuang, L.; et al. Gut dysbiosis induces the development of pre-eclampsia through bacterial translocation. Gut 2020, 69, 513–522. [Google Scholar] [CrossRef]
- Liu, S.; Gao, J.; Zhu, M.; Liu, K.; Zhang, H.-L. Gut Microbiota and Dysbiosis in Alzheimer’s Disease: Implications for Pathogenesis and Treatment. Mol. Neurobiol. 2020, 57, 5026–5043. [Google Scholar] [CrossRef]
- Yang, D.; Zhao, D.; Ali Shah, S.Z.; Wu, W.; Lai, M.; Zhang, X.; Li, J.; Guan, Z.; Zhao, H.; Li, W.; et al. The Role of the Gut Microbiota in the Pathogenesis of Parkinson’s Disease. Front. Neurol. 2019, 10, 1155. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Kim, H.J.; Cheong, H.K.; Kim, B.J.; Lee, K.H.; Kim, E.H.; Kim, E.A.; Kim, S.; Park, M.S.; Yoon, W.T.; et al. Prevalence of multiple sclerosis in Korea. Neurology 2010, 75, 1432–1438. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R. Diet, Gut Microbiota, and Vitamins D + A in Multiple Sclerosis. Neurotherapeutics 2018, 15, 75–91. [Google Scholar] [CrossRef] [Green Version]
- Han, R.; Ma, J.; Li, H. Mechanistic and therapeutic advances in non-alcoholic fatty liver disease by targeting the gut microbiota. Front. Med. 2018, 12, 645–657. [Google Scholar] [CrossRef]
- Fields, C.T.; Sampson, T.R.; Bruce-Keller, A.J.; Kiraly, D.D.; Hsiao, E.Y.; De Vries, G.J. Defining Dysbiosis in Disorders of Movement and Motivation. J. Neurosci. 2018, 38, 9414–9422. [Google Scholar] [CrossRef]
- Morshedi, M.; Hashemi, R.; Moazzen, S.; Sahebkar, A.; Hosseinifard, E.-S. Immunomodulatory and anti-inflammatory effects of probiotics in multiple sclerosis: A systematic review. J. Neuroinflamm. 2019, 16, 231. [Google Scholar] [CrossRef] [Green Version]
- Eustis, S.J.; McCall, M.W.; Murphy, E.A.; Wirth, M.D. Association Between Gastrointestinal Symptoms and Depression in a Representative Sample of Adults in the United States: Findings from National Health and Nutrition Examination Survey (2005–2016). J. Acad. Consult. Psychiatry 2021, 63, 268–279. [Google Scholar] [CrossRef]
- Chen, Y.; Meng, P.; Cheng, S.; Jia, Y.; Wen, Y.; Yang, X.; Yao, Y.; Pan, C.; Li, C.; Zhang, H.; et al. Assessing the effect of interaction between C-reactive protein and gut microbiome on the risks of anxiety and depression. Mol. Brain 2021, 14, 133. [Google Scholar] [CrossRef]
- Capuco, A.; Urits, I.; Hasoon, J.; Chun, R.; Gerald, B.; Wang, J.K.; Ngo, A.L.; Simopoulos, T.; Kaye, A.D.; Colontonio, M.M.; et al. Gut Microbiome Dysbiosis and Depression: A Comprehensive Review. Curr. Pain Headache Rep. 2020, 24, 36. [Google Scholar] [CrossRef]
- Zheng, P.; Zeng, B.; Zhou, C.; Liu, M.; Fang, Z.; Xu, X.; Zeng, L.; Chen, J.-J.; Fan, S.-H.; Du, X.; et al. Gut microbiome remodeling induces depressive-like behaviors through a pathway mediated by the host’s metabolism. Mol. Psychiatry 2016, 21, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Capuco, A.; Urits, I.; Hasoon, J.; Chun, R.; Gerald, B.; Wang, J.K.; Kassem, H.; Ngo, A.L.; Abd-Elsayed, A.; Simopoulos, T.; et al. Current Perspectives on Gut Microbiome Dysbiosis and Depression. Adv. Ther. 2020, 37, 1328–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.-H.; Xue, F.; Yu, S.-F.; Li, X.-S.; Liu, L.; Jia, Y.-Y.; Yan, W.-J.; Tan, Q.-R.; Wang, H.-N.; Peng, Z.-W. Gut microbiota dysbiosis in depressed women: The association of symptom severity and microbiota function. J. Affect. Disord. 2021, 282, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Han, S.K.; Kim, J.K.; Park, H.S.; Shin, Y.J.; Kim, D.H. Chaihu-Shugan-San (Shihosogansan) alleviates restraint stress-generated anxiety and depression in mice by regulating NF-κB-mediated BDNF expression through the modulation of gut microbiota. Chin. Med. 2021, 16, 77. [Google Scholar] [CrossRef] [PubMed]
- Le Morvan de Sequeira, C.; Kaeber, M.; Cekin, S.E.; Enck, P.; Mack, I. The Effect of Probiotics on Quality of Life, Depression and Anxiety in Patients with Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3497. [Google Scholar] [CrossRef]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, Y.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Seitz, J.; Dahmen, B.; Keller, L.; Herpertz-Dahlmann, B. Gut Feelings: How Microbiota Might Impact the Development and Course of Anorexia Nervosa. Nutrients 2020, 12, 3295. [Google Scholar] [CrossRef]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids from Gut Microbiota in Gut-Brain Communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef] [Green Version]
- Jordi, S.B.U.; Botte, F.; Lang, B.M.; Greuter, T.; Krupka, N.; Auschra, B.; Schreiner, P.; Sulz, M.C.; Biedermann, L.; von Känel, R.; et al. Type D personality is associated with depressive symptoms and clinical activity in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2021, 54, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.; Barrett, K.; Nijher, M.; de Lusignan, S. Prevalence of depression and anxiety in people with inflammatory bowel disease and associated healthcare use: Population-based cohort study. Évid. Based Ment. Health 2021, 24, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.; Mukewar, S.V.; Jagtap, S.; Khaliq, A.; Nijhawan, S.; Patil, M.; Basu, I.; Srivastav, A.P.; Kalita, P.P.; Manonmani, M.M.; et al. Sociodemographic and Clinical Profiles of Patients with Irritable Bowel Syndrome: A Cross-sectional, Multi-centric, Epidemiological Study in India. J. Assoc. Physicians India 2021, 69, 11–12. [Google Scholar] [PubMed]
- Snigdha, S.; Ha, K.; Tsai, P.; Dinan, T.G.; Bartos, J.D.; Shahid, M. Probiotics: Potential novel therapeutics for microbiota-gut-brain axis dysfunction across gender and lifespan. Pharmacol. Ther. 2021, 231, 107978. [Google Scholar] [CrossRef] [PubMed]
- Thackray, V.G. Sex, Microbes, and Polycystic Ovary Syndrome. Trends Endocrinol. Metab. 2019, 30, 54–65. [Google Scholar] [CrossRef]
- Pinto-Meza, A.; Usall, J.; Serrano-Blanco, A.; Suárez, D.; Haro, J.M. Gender differences in response to antidepressant treatment prescribed in primary care. Does menopause make a difference? J. Affect. Disord. 2006, 93, 53–60. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Proportion Affected among Patients with Dysbiosis (%) n = 552 | Proportion Affected among Patients without Dysbiosis (%) n = 552 | p-Value |
|---|---|---|---|
| Age (Mean, SD) | 49.6 (18.2) | 49.6 (18.2) | 0.990 |
| Age 18–40 | 32.8 | 33.7 | 0.808 |
| Age 41–50 | 19.3 | 17.4 | |
| Age 51–60 | 18.3 | 20.7 | |
| Age >60 | 28.3 | 29.5 | |
| Sex | |||
| Female | 61.4 | 61.4 | 1.000 |
| Male | 38.6 | 38.6 | |
| Yearly number of visits during the follow-up | 1.5 (1.8) | 1.5 (1.8) | 1.000 |
| Charlson Comorbidity Index (Mean, SD) | 5.0 (4.9) | 5.0 (4.9) | 0.970 |
| Depression | Prescription of Antidepressants | |||
|---|---|---|---|---|
| Variable | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Total | 2.85 (2.00–4.04) | <0.001 | 4.12 (2.35–7.21) | <0.001 |
| Age 18–40 | 3.77 (1.88–7.56) | <0.001 | 4.61 (1.57–13.50) | 0.005 |
| Age 41–50 | 2.04 (0.94–4.42) | 0.073 | 2.08 (0.65–6.67) | 0.218 |
| Age 51–60 | 1.93 (1.01–3.66) | 0.045 | 2.80 (1.00–7.83) | 0.049 |
| Age >60 | 4.43 (2.06–9.53) | <0.001 | 10.59 (2.49–44.98) | 0.001 |
| Sex | ||||
| Female | 2.61 (1.74–3.92) | <0.001 | 4.55 (2.31–8.99) | <0.001 |
| Male | 3.54 (1.75–7.14) | <0.001 | 3.09 (1.14–8.40) | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, S.-Y.; Kostev, K.; Tanislav, C. Dysbiosis: A Potential Precursor to the Development of a Depressive Disorder. Healthcare 2022, 10, 1503. https://doi.org/10.3390/healthcare10081503
Chung S-Y, Kostev K, Tanislav C. Dysbiosis: A Potential Precursor to the Development of a Depressive Disorder. Healthcare. 2022; 10(8):1503. https://doi.org/10.3390/healthcare10081503
Chicago/Turabian StyleChung, Seung-Young, Karel Kostev, and Christian Tanislav. 2022. "Dysbiosis: A Potential Precursor to the Development of a Depressive Disorder" Healthcare 10, no. 8: 1503. https://doi.org/10.3390/healthcare10081503
APA StyleChung, S.-Y., Kostev, K., & Tanislav, C. (2022). Dysbiosis: A Potential Precursor to the Development of a Depressive Disorder. Healthcare, 10(8), 1503. https://doi.org/10.3390/healthcare10081503