
Topical Agents for Nonrestorative Management of Dental Erosion: A Narrative Review

 ,
,  , ,
, ,  and
and 
Abstract
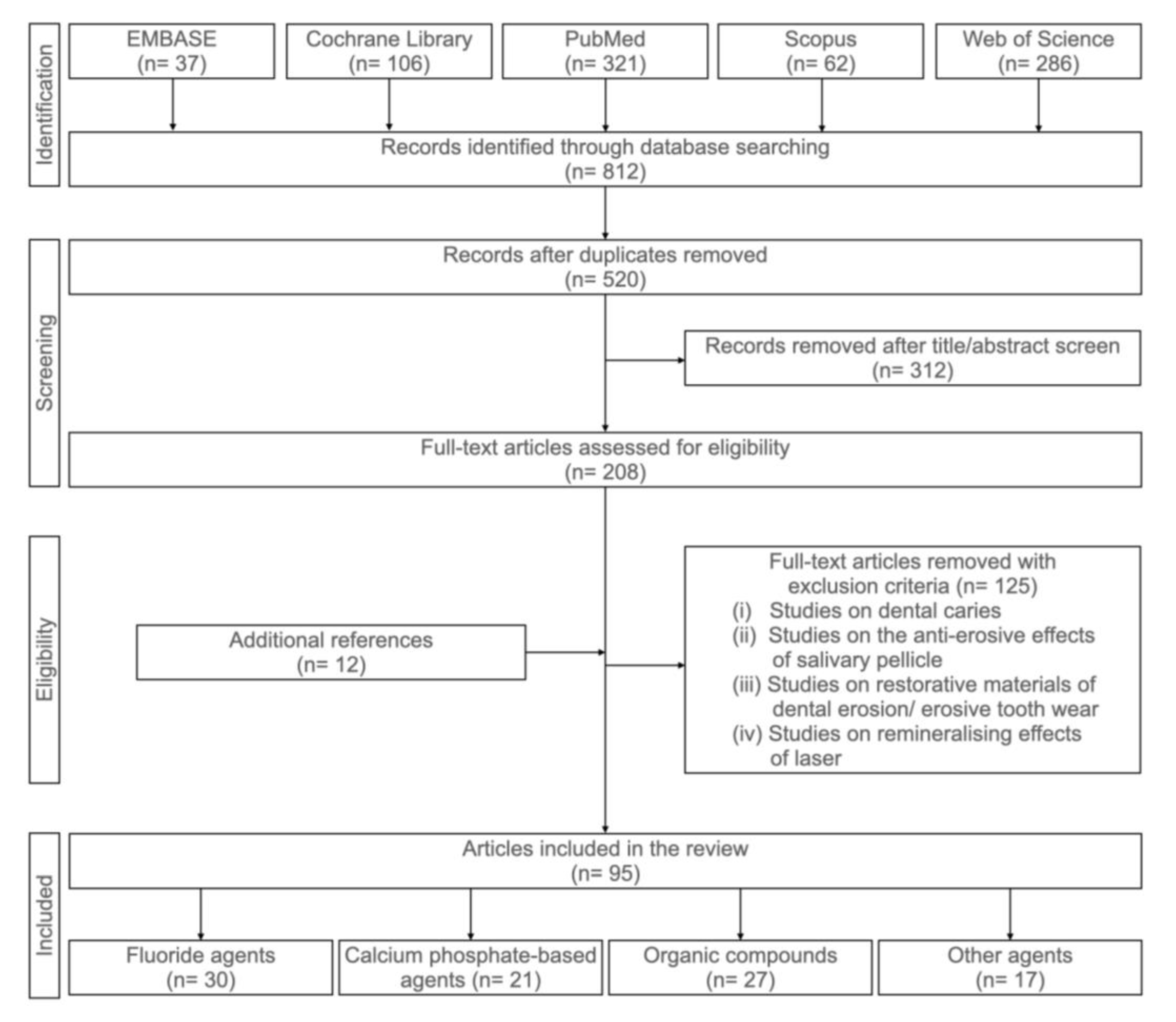
1. Introduction
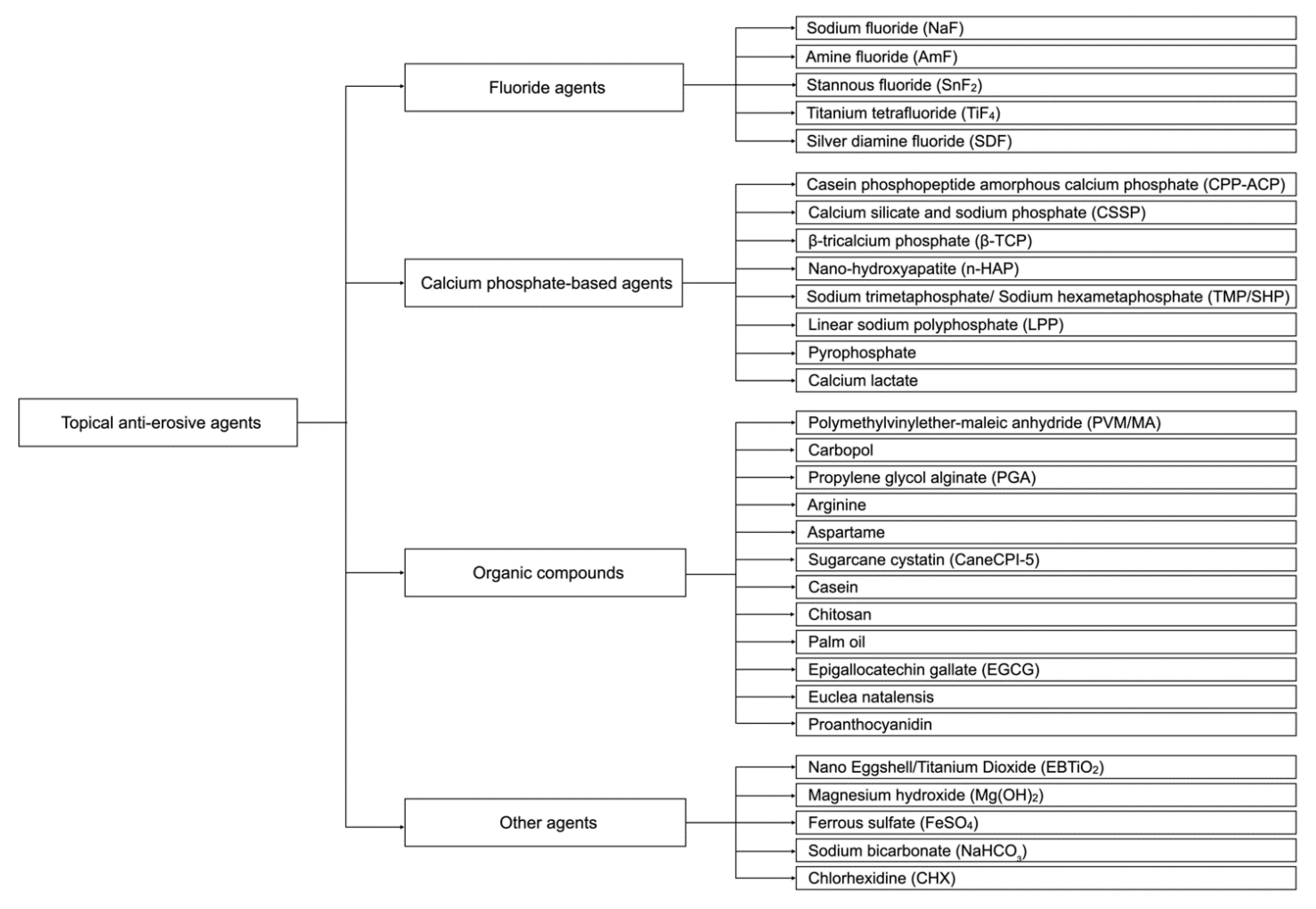
2. Anti-Erosive Agents in the Literature
2.1. Fluoride Agents
2.1.1. Sodium Fluoride (NaF)
2.1.2. Amine Fluoride Containing Agents (AmF)
2.1.3. Stannous Fluoride Containing Agents (SnF2)
2.1.4. Titanium Tetrafluoride (TiF4)
2.1.5. Silver Diamine Fluoride (SDF)
2.2. Calcium Phosphate-Based Agents
2.2.1. Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP)
2.2.2. Calcium Silicate and Sodium Phosphate (CSSP)
2.2.3. β-Tricalcium Phosphate (β-TCP)
2.2.4. Nano-Hydroxyapatite (n-HAP)
2.2.5. Sodium Trimetaphosphate/Sodium Hexametaphosphate (TMP/SHP)
2.2.6. Linear Sodium Polyphosphate (LPP)
2.2.7. Pyrophosphate
2.2.8. Calcium Lactate
2.3. Organic Compounds
2.3.1. Polymethylvinylether-Maleic Anhydride (PVM/MA)
2.3.2. Carbopol
2.3.3. Propylene Glycol Alginate (PGA)
2.3.4. Arginine
2.3.5. Aspartame
2.3.6. Sugarcane Cystatin (CaneCPI-5)
2.3.7. Casein
2.3.8. Chitosan
2.3.9. Palm Oil
2.3.10. Epigallocatechin Gallate (EGCG)
2.3.11. Euclea Natalensis Plant Extracts
2.3.12. Proanthocyanidin
2.4. Other Anti-Erosive Agents
2.4.1. Nano Eggshell/Titanium Dioxide (EBTiO2)
2.4.2. Magnesium Hydroxide (Mg(OH)2)
2.4.3. Ferrous Sulfate (FeSO4)
2.4.4. Sodium Bicarbonate (NaHCO3)
2.4.5. Chlorhexidine (CHX)
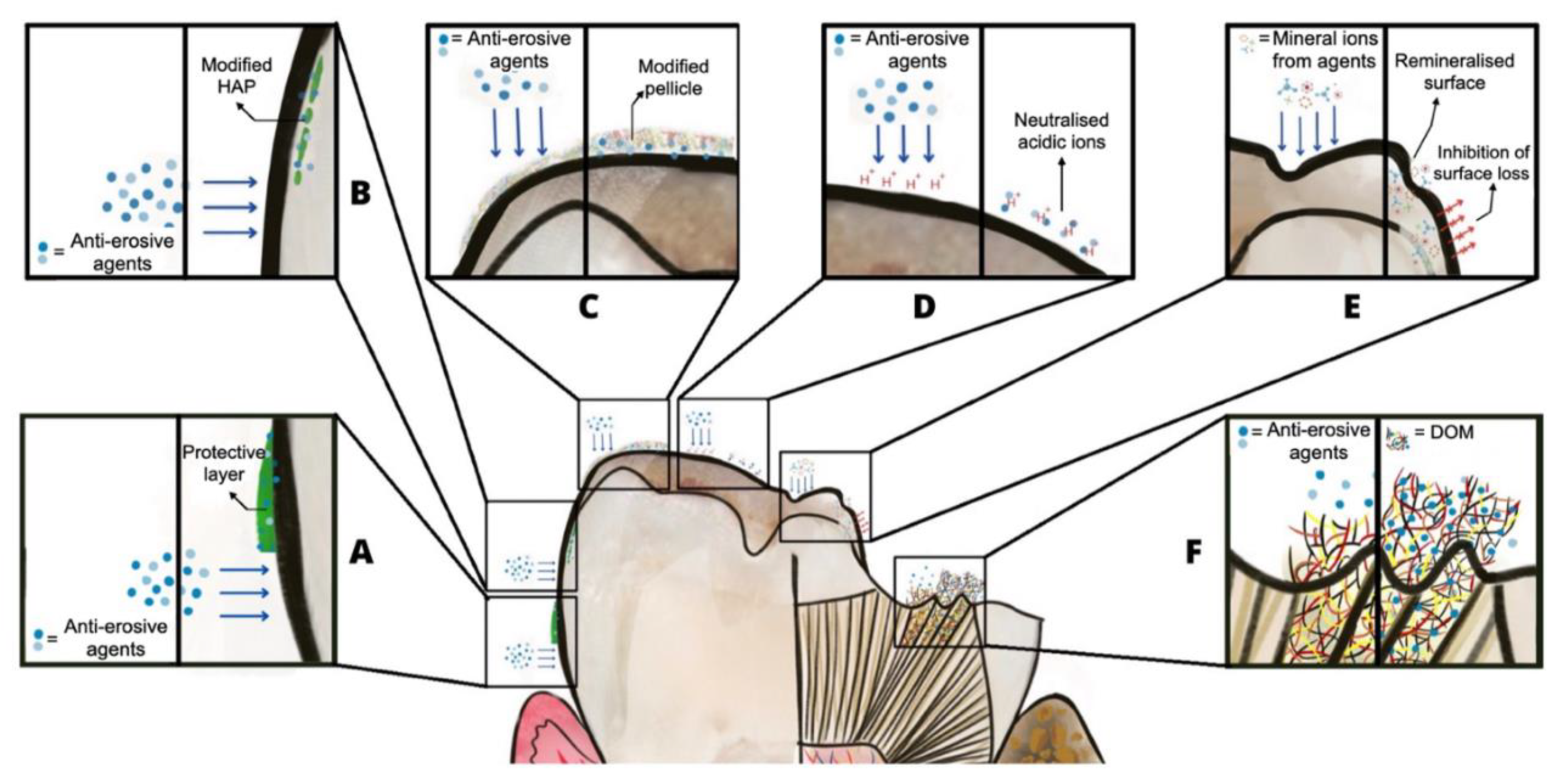
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schlueter, N.; Amaechi, B.T.; Bartlett, D.; Buzalaf, M.A.R.; Carvalho, T.S.; Ganss, C.; Hara, A.T.; Huysmans, M.C.D.; Lussi, A.; Moazzez, R.; et al. Terminology of erosive tooth wear: Consensus report of a workshop organized by the ORCA and the cariology research group of the IADR. Caries Res. 2020, 54, 2–6. [Google Scholar] [CrossRef]
- Seong, J.; Claydon, N.; Macdonald, E.; Garner, S.; Newcombe, R.G.; West, N. A randomised clinical trial to determine the abrasive effect of the tongue on human enamel loss with and without a prior erosive challenge. J. Dent. 2017, 58, 48–53. [Google Scholar] [CrossRef]
- Warreth, A.; Abuhijleh, E.; Almaghribi, M.A.; Mahwal, G.; Ashawish, A. Tooth surface loss: A review of literature. Saudi Dent. J. 2020, 32, 53–60. [Google Scholar] [CrossRef]
- Gupta, M.; Pandit, I.; Srivastava, N.; Gugnani, N. Dental erosion in children. J. Oral Health Comm. Dent. 2009, 3, 56–61. [Google Scholar]
- Lussi, A.; Buzalaf, M.A.R.; Duangthip, D.; Anttonen, V.; Ganss, C.; João-Souza, S.H.; Baumann, T.; Carvalho, T.S. The use of fluoride for the prevention of dental erosion and erosive tooth wear in children and adolescents. Eur. Arch. Paediatr. Dent. 2019, 20, 517–527. [Google Scholar] [CrossRef]
- Schlueter, N.; Luka, B. Erosive tooth wear—A review on global prevalence and on its prevalence in risk groups. Br. Dent. J. 2018, 224, 364–370. [Google Scholar] [CrossRef]
- Okunseri, C.; Wong, M.C.M.; Yau, D.T.W.; McGrath, C.; Szabo, A. The relationship between consumption of beverages and tooth wear among adults in the United States. J. Public Health Dent. 2015, 75, 274–281. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; Jaeggi, T.; Lussi, A. Restorative therapy of erosive lesions. Monogr. Oral Sci. 2014, 25, 253–261. [Google Scholar] [CrossRef]
- Belmar da Costa, M.; Delgado, A.H.S.; Pinheiro de Melo, T.; Amorim, T.; Mano Azul, A. Analysis of laboratory adhesion studies in eroded enamel and dentin: A scoping review. Biomater. Investig. Dent. 2021, 8, 24–38. [Google Scholar] [CrossRef]
- Taji, S.; Seow, W.K. A literature review of dental erosion in children. Aust. Dent. J. 2010, 55, 358–367. [Google Scholar] [CrossRef]
- Colombo, M.; Dagna, A.; Moroni, G.; Chiesa, M.; Poggio, C.; Pietrocola, G. Effect of different protective agents on enamel erosion: An in vitro investigation. J. Clin. Exp. Dent. 2019, 11, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, C.V.; Ramos-Oliveira, T.M.; Mantilla, T.F.; de Freitas, P.M. Frequency of application of AmF/NaF/SnCl2 solution and its potential in controlling human enamel erosion progression: An in situ study. Caries Res. 2017, 51, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, S.; Tuloglu, N.; Bicer, H.; Sen Tunc, E. Effect of fluoride varnish containing CPP-ACP on preventing enamel erosion. Scanning 2017, 2017, 1897825–1897827. [Google Scholar] [CrossRef]
- Buzalaf, M.A.R.; Magalhães, A.C.; Wiegand, A. Alternatives to fluoride in the prevention and treatment of dental erosion. Monogr. Oral Sci. 2014, 25, 244–252. [Google Scholar] [CrossRef]
- O’Toole, S.; Mistry, M.; Mutahar, M.; Moazzez, R.; Bartlett, D. Sequence of stannous and sodium fluoride solutions to prevent enamel erosion. J. Dent. 2015, 43, 1498–1503. [Google Scholar] [CrossRef]
- Ainoosah, S.E.; Levon, J.; Eckert, G.J.; Hara, A.T.; Lippert, F. Effect of silver diamine fluoride on the prevention of erosive tooth wear in vitro. J. Dent. 2020, 103, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Ávila, D.M.; Zanatta, R.F.; Scaramucci, T.; Aoki, I.V.; Torres, C.R.G.; Borges, A.B. Randomized in situ trial on the efficacy of Carbopol in enhancing fluoride/stannous anti-erosive properties. J. Dent. 2020, 101, 1–6. [Google Scholar] [CrossRef]
- Nehme, M.; Jeffery, P.; Mason, S.; Lippert, F.; Zero, D.T.; Hara, A.T. Erosion remineralization efficacy of gel-to-foam fluoride toothpastes in situ: A randomized clinical trial. Caries Res. 2016, 50, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Nehme, M.; Parkinson, C.R.; Zero, D.T.; Hara, A.T. Randomised study of the effects of fluoride and time on in situ remineralisation of acid-softened enamel. Clin. Oral Investig. 2019, 23, 4455–4463. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.-F.; Liu, X.; Fadel, N.; Malmstrom, H.; Barnes, V.; Xu, T. Preventive effects of dentifrice containing 5000 ppm fluoride against dental erosion in situ. J. Dent. 2011, 39, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.; Seong, J.; Macdonald, E.; Claydon, N.; Hellin, N.; Barker, M.L.; He, T.; West, N.X. A randomised in situ trial, measuring the anti-erosive properties of a stannous-containing sodium fluoride dentifrice compared with a sodium fluoride/potassium nitrate dentifrice. Int. Dent. J. 2014, 64, 35–42. [Google Scholar] [CrossRef]
- Lussi, A.; Jaeggi, T.; Zero, D. The role of diet in the aetiology of dental erosion. Caries Res. 2004, 38, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Scaramucci, T.; Borges, A.B.; Lippert, F.; Frank, N.E.; Hara, A.T. Sodium fluoride effect on erosion–abrasion under hyposalivatory simulating conditions. Arch. Oral Biol. 2013, 58, 1457–1463. [Google Scholar] [CrossRef]
- Kensche, A.; Buschbeck, E.; König, B.; Koch, M.; Kirsch, J.; Hannig, C.; Hannig, M. Effect of fluoride mouthrinses and stannous ions on the erosion protective properties of the in situ pellicle. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Kato, M.T.; Bolanho, A.; Zarella, B.L.; Salo, T.; Tjäderhane, L.; Buzalaf, M.A.R. Sodium fluoride inhibits MMP-2 and MMP-9. J. Dent. Res. 2014, 93, 74–77. [Google Scholar] [CrossRef]
- Kato, M.T.; Leite, A.L.; Hannas, A.R.; Buzalaf, M.A.R. Gels containing MMP inhibitors prevent dental erosion in situ. J. Dent. Res. 2010, 89, 468–472. [Google Scholar] [CrossRef]
- Creeth, J.E.; Kelly, S.A.; Martinez-Mier, E.A.; Hara, A.T.; Bosma, M.L.; Butler, A.; Lynch, R.J.M.; Zero, D.T. Dose–response effect of fluoride dentifrice on remineralisation and further demineralisation of erosive lesions: A randomised in situ clinical study. J. Dent. 2015, 43, 823–831. [Google Scholar] [CrossRef]
- Turssi, C.P.; Hara, A.T.; Amaral, F.L.B.; França, F.M.G.; Basting, R.T. Calcium lactate pre-rinse increased fluoride protection against enamel erosion in a randomized controlled in situ trial. J. Dent. 2014, 42, 534–539. [Google Scholar] [CrossRef]
- Danelon, M.; Pessan, J.P.; Prado, K.M.; Ramos, J.P.; Emerenciano, N.G.; Moretto, M.J.; Martinhon, C.C.R.; Delbem, A.C.B. Protective effect of fluoride varnish containing trimetaphosphate against dentin erosion and erosion/abrasion: An in vitro study. Caries Res. 2020, 54, 292–296. [Google Scholar] [CrossRef]
- Ganss, C.; Lussi, A.; Schlueter, N. Dental erosion as oral disease. insights in etiological factors and pathomechanisms, and current strategies for prevention and therapy. Am. J. Dent. 2012, 25, 351–364. [Google Scholar]
- Frese, C.; Wohlrab, T.; Sheng, L.; Kieser, M.; Krisam, J.; Wolff, D. Clinical effect of stannous fluoride and amine fluoride containing oral hygiene products: A 4-year randomized controlled pilot study. Sci. Rep. 2019, 9, 7681. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho Leal, I.; Costa, W.K.D.F.; Passos, V.F. Fluoride dentifrice containing calcium silicate and sodium phosphate salts on dental erosion: In vitro study. Arch. Oral Biol. 2020, 118, 1–6. [Google Scholar] [CrossRef]
- West, N.X.; He, T.; Hellin, N.; Claydon, N.; Seong, J.; Macdonald, E.; Farrell, S.; Eusebio, R.; Wilberg, A. Randomized in situ clinical trial evaluating erosion protection efficacy of a 0.454% stannous fluoride dentifrice. Int. J. Dent. Hyg. 2019, 17, 261–267. [Google Scholar] [CrossRef]
- Schlueter, N.; Klimek, J.; Ganss, C. Efficacy of tin-containing solutions on erosive mineral loss in enamel and dentine in situ. Clin. Oral Investig. 2011, 15, 361–367. [Google Scholar] [CrossRef]
- Huysmans, M.C.; Jager, D.H.; Ruben, J.L.; Unk, D.E.; Klijn, C.P.; Vieira, A.M. Reduction of erosive wear in situ by stannous fluoride-containing toothpaste. Caries Res. 2011, 45, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Olivan, S.R.G.; Sfalcin, R.A.; Fernandes, K.P.S.; Ferrari, R.A.M.; Horliana, A.C.R.T.; Motta, L.J.; Ortega, S.M.; Pinto, M.M.; Deana, A.M.; Bussadori, S.K. Preventive effect of remineralizing materials on dental erosion lesions by speckle technique: An in vitro analysis. Photodiagn. Photodyn. Ther. 2020, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Arnold, W.H.; Dorow, A.; Langenhorst, S.; Gintner, Z.; Bánóczy, J.; Gaengler, P. Effect of fluoride toothpastes on enamel demineralization. BMC Oral Health 2006, 6, 1–8. [Google Scholar] [CrossRef][Green Version]
- Ganss, C.; Neutard, L.; von Hinckeldey, J.; Klimek, J.; Schlueter, N. Efficacy of a Tin/Fluoride rinse: A randomized in situ trial on erosion. J. Dent. Res. 2010, 89, 1214–1218. [Google Scholar] [CrossRef]
- Wegehaupt, F.J.; Sener, B.; Attin, T.; Schmidlin, P.R. Anti-erosive potential of amine fluoride, cerium chloride and laser irradiation application on dentine. Arch. Oral Biol. 2011, 56, 1541–1547. [Google Scholar] [CrossRef]
- Da Silva Ávila, D.M.; Zanatta, R.F.; Scaramucci, T.; Aoki, I.V.; Torres, C.R.G.; Borges, A.B. Influence of bioadhesive polymers on the protective effect of fluoride against erosion. J. Dent. 2016, 56, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, P.G.; Harris, R.; Date, R.F.; Mussett, A.J.; Manly, A.; Barker, M.L.; Hellin, N.; West, N.X. In situ clinical evaluation of a stabilised, stannous fluoride dentifrice. Int. Dent. J. 2014, 64, 43–50. [Google Scholar] [CrossRef]
- West, N.X.; Hooper, S.M.; O’Sullivan, D.; Hughes, N.; North, M.; MacDonald, E.L.; Davies, M.; Claydon, N.C.A. In situ randomised trial investigating abrasive effects of two desensitising toothpastes on dentine with acidic challenge prior to brushing. J. Dent. 2012, 40, 77–85. [Google Scholar] [CrossRef]
- West, N.X.; Hellin, N.; Eusebio, R.; He, T. The erosion protection efficacy of a stabilized stannous fluoride dentifrice: An in situ randomized clinical trial. Am. J. Dent. 2019, 32, 138–142. [Google Scholar]
- Zhao, X.; He, T.; He, Y.; Chen, H. Efficacy of a stannous-containing dentifrice for protecting against combined erosive and abrasive tooth wear in situ. Oral Health Prev. Dent. 2020, 18, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Schlueter, N.; Neutard, L.; von Hinckeldey, J.; Klimek, J.; Ganss, C. Tin and fluoride as anti-erosive agents in enamel and dentine in vitro. Acta Odontol. Scand. 2010, 68, 180–184. [Google Scholar] [CrossRef] [PubMed]
- West, N.X.; Seong, J.; Hellin, N.; Eynon, H.; Barker, M.L.; He, T. A clinical study to measure anti-erosion properties of a stabilized stannous fluoride dentifrice relative to a sodium fluoride/triclosan dentifrice. Int. J. Dent. Hyg. 2017, 15, 113–119. [Google Scholar] [CrossRef]
- Machado, A.; Sakae, L.; Niemeyer, S.H.; Carvalho, T.S.; Amaechi, B.; Scaramucci, T. Anti-erosive effect of rinsing before or after toothbrushing with a fluoride/stannous ions solution: An in situ investigation: Application order of fluoride/tin products for erosive tooth wear. J. Dent. 2020, 101, 103450. [Google Scholar] [CrossRef] [PubMed]
- Körner, P.; Wiedemeier, D.B.; Attin, T.; Wegehaupt, F.J. Prevention of enamel softening by rinsing with a calcium solution before dental erosion. Caries Res. 2020, 54, 127–133. [Google Scholar] [CrossRef]
- Lussi, A.; Carvalho, T.S. The future of fluorides and other protective agents in erosion prevention. Caries Res. 2015, 49, 18–29. [Google Scholar] [CrossRef]
- De Souza, B.M.; Santi, L.R.P.; de Souza Silva, M.; Buzalaf, M.A.R.; Magalhães, A.C. Effect of an experimental mouth rinse containing NaF and TiF4 on tooth erosion and abrasion in situ. J. Dent. 2018, 73, 45–49. [Google Scholar] [CrossRef]
- Hove, L.H.; Stenhagen, K.R.; Holme, B.; Tveit, A.B. The protective effect of SnF2 containing toothpastes and solution on enamel surfaces subjected to erosion and abrasion in situ. Eur. Arch. Paediatr. Dent. 2014, 15, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Barlow, A.; Sufi, F.; Mason, S. Evaluation of different fluoridated dentifrice formulations using an in situ erosion remineralization model. J. Clin. Dent. 2009, 20, 192–198. [Google Scholar] [PubMed]
- Wang, X.; Lussi, A. Assessment and management of dental erosion. Dent. Clin. N. Am. 2010, 54, 565–578. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, A.C.; Levy, F.M.; Rizzante, F.A.; Rios, D.; Buzalaf, M.A.R. Effect of NaF and TiF4 varnish and solution on bovine dentin erosion plus abrasion in vitro. Acta Odontol. Scand. 2012, 70, 160–164. [Google Scholar] [CrossRef]
- De Souza, B.M.; Santi, L.R.P.; João-Souza, S.H.; Carvalho, T.S.; Magalhães, A.C. Effect of titanium tetrafluoride/sodium fluoride solutions containing chitosan at different viscosities on the protection of enamel erosion in vitro. Arch. Oral Biol. 2020, 120, 1–5. [Google Scholar] [CrossRef]
- Yamashita, J.M.; Torres, N.M.; Moura-Grec, P.G.; Marsicano, J.A.; Sales-Peres, A.; Sales-Peres, S.H.C. Role of arginine and fluoride in the prevention of eroded enamel: An in vitro model. Aust. Dent. J. 2013, 58, 478–482. [Google Scholar] [CrossRef]
- Mantilla, T.F.; Turssi, C.P.; Ramos-Oliveira, T.M.; Silva, C.V.D.; Suzuki, L.C.; Freitas, P.M.D. The in situ effect of titanium tetrafluoride gel on erosion/abrasion progression in human dentin. Braz. Dent. J. 2017, 28, 337–345. [Google Scholar] [CrossRef][Green Version]
- Mantilla, T.F.; Silva, C.V.D.; Ramos-Oliveira, T.M.; Turssi, C.P.; Ribeiro, M.S.; Freitas, P.M.D. TiF4 gel effects on tubular occlusion of eroded/abraded human dentin. Microsc. Res. Tech. 2017, 80, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, A.C.; Rios, D.; Honório, H.M.; Delbem, A.C.B.; Buzalaf, M.A.R. Effect of 4% titanium tetrafluoride solution on the erosion of permanent and deciduous human enamel: An in situ/ex vivo study. J. Appl. Oral Sci. 2009, 17, 56–60. [Google Scholar] [CrossRef]
- Wiegand, A.; Waldheim, E.; Sener, B.; Magalhães, A.C.; Attin, T. Comparison of the effects of TiF4 and NaF solutions at pH 1.2 and 3.5 on enamel erosion in vitro. Caries Res. 2009, 43, 269–277. [Google Scholar] [CrossRef]
- Yu, H.; Attin, T.; Wiegand, A.; Buchalla, W. Effects of various fluoride solutions on enamel erosion in vitro. Caries Res. 2010, 44, 390–401. [Google Scholar] [CrossRef] [PubMed]
- Hove, L.H.; Holme, B.; Stenhagen, K.R.; Tveit, A.B. Protective effect of TiF4 solutions with different concentrations and pH on development of erosion-like lesions. Caries Res. 2011, 45, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, A.; Hiestand, B.; Sener, B.; Magalhães, A.C.; Roos, M.; Attin, T. Effect of TiF4, ZrF4, HfF4 and AmF on erosion and erosion/abrasion of enamel and dentin in situ. Arch. Oral Biol. 2009, 55, 223–228. [Google Scholar] [CrossRef][Green Version]
- Hove, L.H.; Holme, B.; Young, A.; Tveit, A.B. The protective effect of TiF4, SnF2 and NaF against erosion-like lesions in situ. Caries Res. 2008, 42, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Nudelman, F.; Marzec, B.; Walker, J.M.; Lo, E.C.M.; Walls, A.W.; Chu, C.H. Formation of fluorohydroxyapatite with silver diamine fluoride. J. Dent. Res. 2017, 96, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Zhao, I.S.; Mei, M.L.; Burrow, M.F.; Lo, E.C.-M.; Chu, C.-H. Effect of silver diamine fluoride and potassium iodide treatment on secondary caries prevention and tooth discolouration in cervical glass ionomer cement restoration. Int. J. Mol. Sci. 2017, 18, 340. [Google Scholar] [CrossRef] [PubMed]
- Soares-Yoshikawa, A.L.; Cury, J.A.; Tabchoury, C.P.M. Fluoride concentration in SDF commercial products and their bioavailability with demineralized dentine. Braz. Dent. J. 2020, 31, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.-H.; Kim, J.-W.; Yoon, Y.-M.; Lee, N.-Y.; Lee, S.-H.; Jih, M.-K. Time-dependent anti-demineralization effect of silver diamine fluoride. Children 2020, 7, 251. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, A.F.M.; Siqueira, F.S.F.; Morales, L.A.R.; Araujo, L.C.R.; Campos, V.S.; Bauer, J.R.; Reis, A.; Loguercio, A.D. Influence of silver diamine fluoride on the adhesive properties of interface resin-eroded dentin. Int. J. Adhes. Adhes. 2021, 106, 1–9. [Google Scholar] [CrossRef]
- Crystal, Y.O.; Niederman, R. Evidence-based dentistry update on silver diamine fluoride. Dent. Clin. N. Am. 2018, 63, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Viana, Í.E.L.; Lopes, R.M.; Silva, F.R.O.; Lima, N.B.; Aranha, A.C.C.; Feitosa, S.; Scaramucci, T. Novel fluoride and stannous-functionalized β-tricalcium phosphate nanoparticles for the management of dental erosion. J. Dent. 2020, 92, 1–6. [Google Scholar] [CrossRef]
- Somani, R.; Jaidka, S.; Singh, D.J.; Arora, V. Remineralizing potential of various agents on dental erosion. J. Oral Biol. Craniofac. Res. 2014, 4, 104–108. [Google Scholar] [CrossRef]
- Yu, H.; Jiang, N.-W.; Ye, X.-Y.; Zheng, H.-Y.; Attin, T.; Cheng, H. In situ effect of tooth mousse containing CPP-ACP on human enamel subjected to in vivo acid attacks. J. Dent. 2018, 76, 40–45. [Google Scholar] [CrossRef]
- Jordão, M.C.; Alencar, C.R.B.; Mesquita, I.M.; Buzalaf, M.A.R.; Magalhães, A.C.; Machado, M.A.A.M.; Honório, H.M.; Rios, D. In situ effect of chewing gum with and without CPP-ACP on enamel surface hardness subsequent to ex vivo acid challenge. Caries Res. 2016, 50, 325–330. [Google Scholar] [CrossRef]
- Wiegand, A.; Attin, T. Randomised in situ trial on the effect of milk and CPP-ACP on dental erosion. J. Dent. 2014, 42, 1210–1215. [Google Scholar] [CrossRef]
- Agrawal, N.; Shashikiran, N.D.; Singla, S.; Ravi, K.S.; Kulkarni, V.K. Effect of remineralizing agents on surface microhardness of primary and permanent teeth after erosion. J. Dent. Child. 2014, 81, 117–121. [Google Scholar]
- Grewal, N.; Kudupudi, V.; Grewal, S. Surface remineralization potential of casein phosphopeptide-amorphous calcium phosphate on enamel eroded by cola-drinks: An in-situ model study. Contemp. Clin. Dent. 2013, 4, 331–337. [Google Scholar] [CrossRef]
- De Alencar, C.R.B.; Magalhães, A.C.; de Andrade Moreira Machado, M.A.; de Oliveira, T.M.; Honório, H.M.; Rios, D. In situ effect of a commercial CPP-ACP chewing gum on the human enamel initial erosion. J. Dent. 2014, 42, 1502–1507. [Google Scholar] [CrossRef]
- Zawaideh, F.I.; Owais, A.I.; Mushtaha, S. Effect of CPP-ACP or a potassium nitrate sodium fluoride dentifrice on enamel erosion prevention. J. Clin. Pediatr. Dent. 2017, 41, 135–140. [Google Scholar] [CrossRef]
- Fernandes, L.H.F.; Alencar, C.R.B.D.; Melo, J.B.D.C.A.D.; Rios, D.; Honório, H.M.; Cavalcanti, A.L. In situ effect of intra-oral application of pastes containing CPP-ACP or CPP-ACPF against initial enamel erosion. Pesqui. Bras. Odontopediatria Clín. Integr. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Srinivasan, N.; Kavitha, M.; Loganathan, S.C. Comparison of the remineralization potential of CPP–ACP and CPP–ACP with 900 ppm fluoride on eroded human enamel: An in situ study. Arch. Oral Biol. 2010, 55, 541–544. [Google Scholar] [CrossRef]
- Fanfoni, L.; Costantinides, F.; Berton, F.; Marchesi, G.; Polo, L.; di Lenarda, R.; Nicolin, V. From erosion to remineralization: The possible role of two topic home devices used as combined treatment. Appl. Sci. 2020, 10, 4093. [Google Scholar] [CrossRef]
- Ionta, F.Q.; dos Santos, N.M.; Mesquita, I.M.; Dionísio, E.J.; Cruvinel, T.; Honório, H.M.; Rios, D. Is the dentifrice containing calcium silicate, sodium phosphate, and fluoride able to protect enamel against chemical mechanical wear? An in situ/ex vivo study. Clin. Oral Investig. 2019, 23, 3713–3720. [Google Scholar] [CrossRef]
- João-Souza, S.H.; Scaramucci, T.; Bühler Borges, A.; Lussi, A.; Saads Carvalho, T.; Corrêa Aranha, A.C. Influence of desensitizing and anti-erosive toothpastes on dentine permeability: An in vitro study. J. Dent. 2019, 89, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Joiner, A.; Schäfer, F.; Naeeni, M.M.; Gupta, A.K.; Zero, D.T. Remineralisation effect of a dual-phase calcium silicate/phosphate gel combined with calcium silicate/phosphate toothpaste on acid-challenged enamel in situ. J. Dent. 2014, 42, 53–59. [Google Scholar] [CrossRef]
- Marianna Lopes, R.; Scaramucci, T.; Walker, C.L.; Feitosa, S.A.; Aranha, A.C.C. In situ evaluation of desensitizing toothpastes for protecting against erosive tooth wear and its characterization. Clin. Oral Investig. 2021, 25, 6857–6870. [Google Scholar] [CrossRef]
- De Oliveira, A.F.B.; Mathews, S.M.; Ramalingam, K.; Amaechi, B. The effectiveness of an NaF rinse containing fTCP on eroded enamel remineralization. J. Public Health 2016, 24, 147–152. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Karthikeyan, R.; Mensinkai, P.K.; Najibfard, K.; Mackey, A.C.; Karlinsey, R.L. Remineralization of eroded enamel by a NaF rinse containing a novel calcium phosphate agent in an in situ model: A pilot study. Clin. Cosmet. Investig. Dent. 2010, 2, 93–100. [Google Scholar] [CrossRef][Green Version]
- Mathews, M.S.; Amaechi, B.T.; Ramalingam, K.; Ccahuana-Vasquez, R.A.; Chedjieu, I.P.; Mackey, A.C.; Karlinsey, R.L. In situ remineralisation of eroded enamel lesions by NaF rinses. Arch. Oral Biol. 2012, 57, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Ince, S.G.; Banu Ermis, R. The in situ potential of synthetic nano-hydroxyapatite for tooth enamel repair. Bioinspired Biomim. Nanobiomater. 2021, 10, 78–86. [Google Scholar] [CrossRef]
- Esteves-Oliveira, M.; Santos, N.M.; Meyer-Lueckel, H.; Wierichs, R.J.; Rodrigues, J.A. Caries-preventive effect of anti-erosive and nano-hydroxyapatite-containing toothpastes in vitro. Clin. Oral Investig. 2016, 21, 291–300. [Google Scholar] [CrossRef]
- Tschoppe, P.; Zandim, D.L.; Martus, P.; Kielbassa, A.M. Enamel and dentine remineralization by nano-hydroxyapatite toothpastes. J. Dent. 2011, 39, 430–437. [Google Scholar] [CrossRef]
- Bordea, I.R.; Candrea, S.; Alexescu, G.T.; Bran, S.; Băciuț, M.; Băciuț, G.; Lucaciu, O.; Dinu, C.M.; Todea, D.A. Nano-hydroxyapatite use in dentistry: A systematic review. Drug Metab. Rev. 2020, 52, 319–332. [Google Scholar] [CrossRef]
- Shellis, R.P.; Featherstone, J.D.B.; Lussi, A. Understanding the chemistry of dental erosion. Monogr. Oral Sci. 2014, 25, 163–179. [Google Scholar] [CrossRef] [PubMed]
- Abou Neel, E.A.; Bakhsh, T.A. An eggshell-based toothpaste as a cost-effective treatment of dentin hypersensitivity. Eur. J. Dent. 2021, 15, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Missel, E.M.C.; Cunha, R.F.; Vieira, A.E.M.; Cruz, N.V.S.; Castilho, F.C.N.; Delbem, A.C.B. Sodium trimetaphosphate enhances the effect of 250 ppm. fluoride toothpaste against enamel demineralization in vitro. Eur. J. Oral Sci. 2016, 124, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Lussi, A. Dental erosion—Novel remineralizing agents in prevention or repair. Adv. Dent. Res. 2009, 21, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Pancote, L.P.; Manarelli, M.M.; Danelon, M.; Delbem, A.C.B. Effect of fluoride gels supplemented with sodium trimetaphosphate on enamel erosion and abrasion: In vitro study. Arch. Oral Biol. 2013, 59, 336–340. [Google Scholar] [CrossRef]
- Danelon, M.; Pessan, J.P.; Santos, V.R.d.; Chiba, E.K.; Garcia, L.S.G.; de Camargo, E.R.; Delbem, A.C.B. Fluoride toothpastes containing micrometric or nano-sized sodium trimetaphosphate reduce enamel erosion in vitro. Acta Odontol. Scand. 2018, 76, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Moretto, M.J.; Delbem, A.C.B.; Manarelli, M.M.; Pessan, J.P.; Martinhon, C.C.R. Effect of fluoride varnish supplemented with sodium trimetaphosphate on enamel erosion and abrasion: An in situ/ex vivo study. J. Dent. 2013, 41, 1302–1306. [Google Scholar] [CrossRef]
- Manarelli, M.M.; Vieira, A.E.M.; Matheus, A.A.; Sassaki, K.T.; Delbem, A.C.B. Effect of mouth rinses with fluoride and trimetaphosphate on enamel erosion: An in vitro study. Caries Res. 2011, 45, 506–509. [Google Scholar] [CrossRef]
- Scaramucci, T.; João-Souza, S.H.; Lippert, F.; Eckert, G.J.; Aoki, I.V.; Hara, A.T. Influence of toothbrushing on the antierosive effect of film-forming agents. Caries Res. 2016, 50, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Scaramucci, T.; Borges, A.B.; Lippert, F.; Zero, D.T.; Aoki, I.V.; Hara, A.T. Anti-erosive properties of solutions containing fluoride and different film-forming agents. J. Dent. 2015, 43, 458–465. [Google Scholar] [CrossRef]
- João-Souza, S.H.; Bezerra, S.J.C.; de Freitas, P.M.; de Lima, N.B.; Aranha, A.C.C.; Hara, A.T.; Scaramucci, T. In situ evaluation of fluoride-, stannous- and polyphosphate-containing solutions against enamel erosion. J. Dent. 2017, 63, 30–35. [Google Scholar] [CrossRef]
- Creeth, J.E.; Parkinson, C.R.; Burnett, G.R.; Sanyal, S.; Lippert, F.; Zero, D.T.; Hara, A.T. Effects of a sodium fluoride- and phytate-containing dentifrice on remineralisation of enamel erosive lesions—An in situ randomised clinical study. Clin. Oral Investig. 2018, 22, 2543–2552. [Google Scholar] [CrossRef]
- Parkinson, C.R.; Burnett, G.R.; Creeth, J.E.; Lynch, R.J.M.; Budhawant, C.; Lippert, F.; Hara, A.T.; Zero, D.T. Effect of phytate and zinc ions on fluoride toothpaste efficacy using an in situ caries model. J. Dent. 2018, 73, 24–31. [Google Scholar] [CrossRef]
- Borges, A.B.; Scaramucci, T.; Lippert, F.; Zero, D.T.; Hara, A.T. Erosion protection by calcium lactate/sodium fluoride rinses under different salivary flows in vitro. Caries Res. 2014, 48, 193–199. [Google Scholar] [CrossRef]
- Bezerra, S.J.; João-Souza, S.H.; Aoki, I.V.; Borges, A.B.; Hara, A.T.; Scaramucci, T. Anti-erosive effect of solutions containing sodium fluoride, stannous chloride, and selected film-forming polymers. Caries Res. 2019, 53, 305–313. [Google Scholar] [CrossRef]
- Beyer, M.; Reichert, J.; Sigusch, B.W.; Watts, D.C.; Jandt, K.D. Morphology and structure of polymer layers protecting dental enamel against erosion. Dent. Mater. 2012, 28, 1089–1097. [Google Scholar] [CrossRef]
- Wang, W.; Xie, Q.; Xu, T.; Wang, Q.; Malmstrom, H.S.; Ren, Y.-F. Fluoride release and anti-erosive effects of dentifrices containing PVM/MA copolymers. J. Dent. 2012, 41, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Creeth, J.E.; Burnett, G.R.; Souverain, A.; Gomez-Pereira, P.; Zero, D.T.; Lippert, F.; Hara, A.T. In situ efficacy of an experimental toothpaste on enamel rehardening and prevention of demineralisation: A randomised, controlled trial. BMC Oral Health 2020, 20, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Ávila, D.M.; Augusto, M.G.; Zanatta, R.F.; Scaramucci, T.; Aoki, I.V.; Torres, C.R.G.; Borges, A.B. Enhancing the anti-erosive properties of fluoride and stannous with the polymer carbopol. Caries Res. 2020, 54, 250–257. [Google Scholar] [CrossRef]
- Sakae, L.O.; Niemeyer, S.H.; Bezerra, S.J.C.; Borges, A.B.; Turssi, C.P.; Scaramucci, T. The addition of propylene glycol alginate to a fluoride solution to control enamel wear: An in situ study. Caries Res. 2020, 54, 517–523. [Google Scholar] [CrossRef]
- Olley, R.C.; Pilecki, P.; Hughes, N.; Jeffery, P.; Austin, R.S.; Moazzez, R.; Bartlett, D. An in situ study investigating dentine tubule occlusion of dentifrices following acid challenge. J. Dent. 2012, 40, 585–593. [Google Scholar] [CrossRef]
- West, N.X.; He, T.; Macdonald, E.L.; Seong, J.; Hellin, N.; Barker, M.L.; Eversole, S.L. Erosion protection benefits of stabilized SnF2 dentifrice versus an arginine–sodium monofluorophosphate dentifrice: Results from in vitro and in situ clinical studies. Clin. Oral Investig. 2017, 21, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.C.S.; Bandéca, M.C.; Pinheiro, M.C.; Cavassim, R.; Tonetto, M.R.; Borges, A.H.; Sampaio, J.E.C. Preventive effect of a high fluoride toothpaste and arginine-carbonate toothpaste on dentinal tubules exposure followed by acid challenge: A dentine permeability evaluation. BMC Res. Notes 2014, 7, 385. [Google Scholar] [CrossRef] [PubMed]
- West, N.; He, T.; Hellin, N.; Claydon, N.; Seong, J.; Macdonald, E.; Eusebio, R. Erosion protection efficacy of a 0.454% stannous fluoride dentifrice versus an arginine-containing dentifrice. Am. J. Dent. 2018, 31, 63–66. [Google Scholar]
- Seong, J.; Macdonald, E.; Newcombe, R.G.; Davies, M.; Jones, S.B.; Johnson, S.; West, N.X. In situ randomised trial to investigate the occluding properties of two desensitising toothpastes on dentine after subsequent acid challenge. Clin. Oral Investig. 2013, 17, 195–203. [Google Scholar] [CrossRef]
- Ionta, F.; Bassoto, M.A.; dos Santos, N.; di Campli, F.; Honório, H.; Cruvinel, T.; Buzalaf, M.; Rios, D. Effect of in situ aspartame mouthwash to prevent intrinsic and extrinsic erosive tooth wear. J. Clin. Exp. Dent. 2020, 12, 638–643. [Google Scholar] [CrossRef]
- Rios, D.; Ionta, F.-Q.; Rebelato, R.; Jordão, M.-C.; Wang, L.; Magalhães, A.-C.; Honório, H.-M. The effect of aspartame and pH changes on the erosive potential of cola drinks in bovine enamel: An in vitro study. J. Clin. Exp. Dent. 2018, 10, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Pelá, V.T.; Lunardelli, J.G.Q.; Tokuhara, C.K.; Gironda, C.C.; Silva, N.D.G.; Carvalho, T.S.; Santiago, A.C.; Souza, B.M.; Moraes, S.M.; Henrique-Silva, F.; et al. Safety and in situ antierosive effect of CaneCPI-5 on dental enamel. J. Dent. Res. 2021, 100, 1344–1350. [Google Scholar] [CrossRef]
- Santos, L.A.; Martini, T.; Câmara, J.V.F.; Reis, F.N.; Cassia Ortiz, A.D.; Camiloti, G.D.; Levy, F.M.; Shibao, P.Y.T.; Honorio, H.M.; Henrique-Silva, F.; et al. Solutions and gels containing a sugarcane-derived cystatin (CaneCPI-5) reduce enamel and dentin erosion in vitro. Caries Res. 2021, 55, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Santiago, A.C.; Khan, Z.N.; Miguel, M.C.; Gironda, C.C.; Soares-Costa, A.; Pelá, V.T.; Leite, A.L.; Edwardson, J.M.; Buzalaf, M.A.R.; Henrique-Silva, F. A new sugarcane cystatin strongly binds to dental enamel and reduces erosion. J. Dent. Res. 2017, 96, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Chawhuaveang, D.D.; Yu, O.Y.; Yin, I.X.; Lam, W.Y.-H.; Mei, M.L.; Chu, C.-H. Acquired salivary pellicle and oral diseases: A literature review. J. Dent. Sci. 2021, 16, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Jager, D.H.J.; Vissink, A.; Timmer, C.J.; Bronkhorst, E.; Vieira, A.M.; Huysmans, M.C.D.N.J.M. Reduction of erosion by protein-containing toothpastes. Caries Res. 2013, 47, 135–140. [Google Scholar] [CrossRef]
- White, A.J.; Gracia, L.H.; Barbour, M.E. Inhibition of dental erosion by casein and casein-derived proteins. Caries Res. 2011, 45, 13–20. [Google Scholar] [CrossRef]
- Beltrame, A.P.C.; Suchyta, D.; Abd Alraheam, I.; Mohammed, A.; Schoenfisch, M.; Walter, R.; Almeida, I.C.; Souza, L.C.; Miguez, P.A. Effect of phosphorylated chitosan on dentin erosion: An in vitro study. Caries Res. 2018, 52, 378–386. [Google Scholar] [CrossRef]
- Schlueter, N.; Klimek, J.; Ganss, C. Randomised in situ study on the efficacy of a Tin/Chitosan toothpaste on erosive-abrasive enamel loss. Caries Res. 2013, 47, 574–581. [Google Scholar] [CrossRef]
- Schlueter, N.; Klimek, J.; Ganss, C. Effect of a chitosan additive to a Sn2+-containing toothpaste on its anti-erosive/anti-abrasive efficacy—A controlled randomised in situ trial. Clin. Oral Investig. 2014, 18, 107–115. [Google Scholar] [CrossRef]
- Souza, B.M.; Machado, P.F.; Vecchia, L.R.P.; Magalhães, A.C. Effect of chitosan solutions with or without fluoride on the protection against dentin erosion in vitro. Eur. J. Oral Sci. 2020, 128, 495–500. [Google Scholar] [CrossRef]
- Aykut-Yetkiner, A.; Attin, T.; Wiegand, A. Prevention of dentine erosion by brushing with anti-erosive toothpastes. J. Dent. 2014, 42, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Ionta, F.Q.; Alencar, C.R.B.D.; Santos, N.M.D.; Bergantin, B.T.P.; Val, P.P.; Honório, H.M.; Oliveira, T.M.D.; Rios, D. Effect of palm oil alone or associated to stannous solution on enamel erosive-abrasive wear: A randomized in situ/ex vivo study. Arch. Oral Biol. 2018, 95, 68–73. [Google Scholar] [CrossRef]
- Ionta, F.Q.; Alencar, C.R.B.D.; Val, P.P.; Boteon, A.P.; Jordão, M.C.; Honório, H.M.; Buzalaf, M.A.R.; Rios, D. Effect of vegetable oils applied over acquired enamel pellicle on initial erosion. J. Appl. Oral Sci. 2017, 25, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-L.; Chang, H.-H.; Chiang, Y.-C.; Lu, Y.-C.; Lin, C.-P. Effects of fluoride and epigallocatechin gallate on soft-drink-induced dental erosion of enamel and root dentin. J. Formos. Med. Assoc. 2018, 117, 276–282. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, M.D.R.; Carneiro, J.R.M.; Passos, V.F.; Santiago, S.L. Effect of green tea as a protective measure against dental erosion in coronary dentine. Braz. Oral Res. 2016, 30, 1–6. [Google Scholar] [CrossRef]
- Kato, M.T.; Magalhães, A.C.; Rios, D.; Hannas, A.R.; Attin, T.; Buzalaf, M.A.R. Protective effect of green tea on dentin erosion and abrasion. J. Appl. Oral Sci. 2009, 17, 560–564. [Google Scholar] [CrossRef]
- De Souza-E-Silva, C.M.; da Silva Ventura, T.M.; de Paila Silva Cassiano, L.; de Lima Leite, A.; Buzalaf, M.A.R. Effect of gels containing chlorhexidine or epigallocatechin-3-gallate on the protein composition of the acquired enamel pellicle. Arch. Oral Biol. 2017, 82, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.T.; Hannas, A.R.; Cardoso, C.D.A.B.; Cassiano, L.D.P.S.; Naves, P.A.; Magalhães, A.C.; Tjäderhane, L.; Buzalaf, M.A.R. Dentifrices or gels containing MMP inhibitors prevent dentine loss: In situ studies. Clin. Oral Investig. 2021, 25, 2183–2190. [Google Scholar] [CrossRef] [PubMed]
- Sales-Peres, S.H.D.C.; Xavier, C.N.H.; Mapengo, M.A.A.; Forim, M.R.; Silva, M.D.F.; Sales-Peres, A. Erosion and abrasion-inhibiting in situ effect of the Euclea natalensis plant of African regions. Braz. Oral Res. 2016, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sales-Peres, S.H.D.C.; Brianezzi, L.F.D.F.; Marsicano, J.A.; Forim, M.R.; da Silva, M.F.D.G.F.; Sales-Peres, A. Evaluation of an experimental gel containing Euclea natalensis: An in vitro study. Evid. Based Complementary Altern. Med. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- Cardoso, F.; Boteon, A.P.; Silva, T.A.P.D.; Prakki, A.; Wang, L.; HonÓrio, H.M. In situ effect of a proanthocyanidin mouthrinse on dentin subjected to erosion. J. Appl. Oral Sci. 2020, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Boteon, A.P.; Kato, M.T.; Buzalaf, M.A.R.; Prakki, A.; Wang, L.; Rios, D.; Honório, H.M. Effect of proanthocyanidin-enriched extracts on the inhibition of wear and degradation of dentin demineralized organic matrix. Arch. Oral Biol. 2017, 84, 118–124. [Google Scholar] [CrossRef]
- Fawzy, A.S.; Priyadarshini, B.M.; Selvan, S.T.; Lu, T.B.; Neo, J. Proanthocyanidins-loaded nanoparticles enhance dentin degradation resistance. J. Dent. Res. 2017, 96, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Jawale, K.; Kamat, S.; Patil, J.; Nanjannawar, G.; Chopade, R. Grape seed extract: An innovation in remineralization. J. Conserv. Dent. 2017, 20, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Onwubu, S.C.; Mdluli, P.S.; Singh, S.; Nyembe, S.; Thakur, R. Corrigendum to “An in situ evaluation of the protective effect of nano eggshell/titanium dioxide against erosive acids”. Int J. Dent. 2019, 2019, 7209168. [Google Scholar] [CrossRef] [PubMed]
- Onwubu, S.C.; Mdluli, P.S.; Singh, S.; Tlapana, T. A novel application of nano eggshell/titanium dioxide composite on occluding dentine tubules: An in vitro study. Braz. Oral Res. 2019, 33, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Onwubu, S.C.; Mdluli, P.S.; Singh, S.; Madikizela, L.; Ngombane, Y. Characterization and in vitro evaluation of an acid resistant nanosized dental eggshell-titanium dioxide material. Adv. Powder Technol. 2019, 30, 766–773. [Google Scholar] [CrossRef]
- Passos, V.F.; Rodrigues, L.K.A.; Santiago, S.L. The effect of magnesium hydroxide-containing dentifrice using an extrinsic and intrinsic erosion cycling model. Arch. Oral Biol. 2018, 86, 46–50. [Google Scholar] [CrossRef]
- Park, K.S.; Kim, B.J.; Lih, E.; Park, W.; Lee, S.H.; Joung, Y.K.; Han, D.K. Versatile effects of magnesium hydroxide nanoparticles in PLGA scaffold–mediated chondrogenesis. Acta Biomater. 2018, 73, 204–216. [Google Scholar] [CrossRef]
- Passos, V.F.; Rodrigues Gerage, L.K. Magnesium hydroxide-based dentifrice as an anti-erosive agent in an in situ intrinsic erosion model. Am. J. Dent. 2017, 30, 137–141. [Google Scholar]
- Abdallah, M.-N.; Eimar, H.; Bassett, D.C.; Schnabel, M.; Ciobanu, O.; Nelea, V.; McKee, M.D.; Cerruti, M.; Tamimi, F. Diagenesis-inspired reaction of magnesium ions with surface enamel mineral modifies properties of human teeth. Acta Biomater. 2016, 37, 174–183. [Google Scholar] [CrossRef]
- Kato, M.T.; Leite, A.L.; Hannas, A.R.; Oliveira, R.C.; Pereira, J.C.; Tjäderhane, L.; Buzalaf, M.A.R. Effect of iron on matrix metalloproteinase inhibition and on the prevention of dentine erosion. Caries Res. 2010, 44, 309–316. [Google Scholar] [CrossRef]
- Kato, M.T.; Leite, A.L.; Hannas, A.R.; Calabria, M.P.; Magalhães, A.C.; Pereira, J.C.; Buzalaf, M.A.R. Impact of protease inhibitors on dentin matrix degradation by collagenase. J. Dent. Res. 2012, 91, 1119–1123. [Google Scholar] [CrossRef]
- Sales-Peres, S.H.C.; Pessan, J.P.; Buzalaf, M.A.R. Effect of an iron mouthrinse on enamel and dentine erosion subjected or not to abrasion: An in situ/ex vivo study. Arch. Oral Biol. 2006, 52, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.T.; Buzalaf, M.A.R. Iron supplementation reduces the erosive potential of a cola drink on enamel and dentin in situ. J. Appl. Oral Sci. 2012, 20, 318–322. [Google Scholar] [CrossRef]
- Messias, D.C.F.; Turssi, C.P.; Hara, A.T.; Serra, M.C. Sodium bicarbonate solution as an anti-erosive agent against simulated endogenous erosion. Eur. J. Oral Sci. 2010, 118, 385–388. [Google Scholar] [CrossRef]
- Messias, D.; Serra, M.C.; Turssi, C.P. Potential effect of sodium bicarbonate-containing dentifrice in controlling enamel erosion in situ. Am. J. Dent. 2008, 21, 300–302. [Google Scholar]
- Messias, D.C.F.; Martins, M.E.N.; Serra, M.C.; Turssi, C.P. Feasibility of using sodium bicarbonate solution as a damage-limiting strategy for erosion lesions. Oral Health Prev. Dent. 2008, 6, 155–158. [Google Scholar]
- Magalhães, A.C.; Wiegand, A.; Rios, D.; Hannas, A.; Attin, T.; Buzalaf, M.A.R. Chlorhexidine and green tea extract reduce dentin erosion and abrasion in situ. J. Dent. 2009, 37, 994–998. [Google Scholar] [CrossRef]
- Charone, S.; Cardoso, C.D.A.B.; Kato, M.T.; Ducati, P.; Fukushima, R.; Gennaro, G.; Magalhães, A.C.; Buzalaf, M.A.R. The effect of mouthwashes containing biguanides on the progression of erosion in dentin. BMC Oral Health 2014, 14, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Ozan, G.; Sar Sancakli, H.; Yucel, T. Effect of black tea and matrix metalloproteinase inhibitors on eroded dentin in situ. Microsc. Res. Tech. 2020, 83, 834–842. [Google Scholar] [CrossRef]
- Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Lo, E.C.-M.; Chu, C.-H. A review of the common models used in mechanistic studies on demineralization-remineralization for cariology research. Dent. J. 2017, 5, 20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Agents | Concentration of Active Ingredients | Delivery System | Example of Product Names and Companies |
|---|---|---|---|
| NaF | 1100 ppm F of NaF | Toothpaste |
|
| 1450 ppm F of NaF | Toothpaste | ||
| 5000 ppm F of NaF | Toothpaste |
| |
| AmF + SnCl2 | 800 ppm Sn SnCl2 + 500 ppmF of NaF+ AmF | Mouthrinse | |
| AmF + SnF2 | 250 ppm F of AmF + SnF2 | Mouthrinse |
|
| 1450 ppmF of AmF + SnF2 | Toothpaste |
| |
| SnF2 | 0.4–0.454% SnF2, 1100–1450 ppm F of SnF2 | Toothpaste |
|
| 1450 ppm F of NaF + SnF2 | Toothpaste | ||
| CPP-ACP | 10% CPP-ACP | Gum |
|
| 10% CPP-ACP | Cream |
| |
| 10% CPP-ACP with 900 ppm F of NaF | Cream |
| |
| 2% CPP-ACP + 22,600 ppm F of NaF | Varnish |
| |
| CSSP | CSSP with 1450 ppm F of SMFP | Toothpaste | |
| β-TCP | 5% TCP + 22,600 ppm F of NaF | Varnish |
|
| n-HAP | 2.25–20% n-HAP | Toothpaste | |
| 1% n-HAP + 1450 ppm F of NaF | Toothpaste |
| |
| Arginine | 1.5% Arginine + 1450 ppm F of SMFP | Toothpaste | ∙ Colgate® Maximum Cavity Protection, Colgate-Palmolive [115,117] |
| 8% Arginine + 1450 ppm F of SMFP | Toothpaste | ||
| Chitosan | 0.5% Chitosan + 1400 ppm F AmF/NaF + 3500 ppm Sn SnCl2 | Toothpaste |
|
| CHX | 0.2% Chlorhexidine | Mouthrinse |
| Form a Protective Layer | Modify Hydroxy-Apatite | Modify Salivary Pellicle | Neutralise Acid | Supply Mineral Ions | Inhibit MMPs | |
|---|---|---|---|---|---|---|
| Fluoride agents | ||||||
| NaF | ||||||
| AmF | ? | ? | ||||
| SnF2 | ||||||
| TiF4 | ? | ? | ||||
| SDF | ? | |||||
| Calcium phosphate-based agents | ||||||
| CPP-ACP | ||||||
| CSSP | ? | |||||
| β-TCP | ? | |||||
| n-HAP | ? | |||||
| TMP/SHP | * | |||||
| LPP | * | |||||
| Pyrophosphate | ? | |||||
| Calcium lactate | ? | |||||
| Organic compounds | ||||||
| PVM/MA | ? | |||||
| Carbopol | * | |||||
| PGA | * | |||||
| Arginine | ? | |||||
| Aspartame | ? | ? | ||||
| CaneCPI-5 | ||||||
| Casein | ||||||
| Chitosan | ||||||
| Palm oil | ? | |||||
| EGCG | ||||||
| Euclea natalensis | ||||||
| Proanthocyanidin | ? | |||||
| Other agents | ||||||
| EBTiO2 | ? | |||||
| Mg(OH)2 | ? | |||||
| FeSO4 | ? | |||||
| NaHCO3 | ? | ? | ||||
| CHX | ? | ? | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chawhuaveang, D.D.; Yu, O.Y.; Yin, I.X.; Lam, W.Y.H.; Chu, C.H. Topical Agents for Nonrestorative Management of Dental Erosion: A Narrative Review. Healthcare 2022, 10, 1413. https://doi.org/10.3390/healthcare10081413
Chawhuaveang DD, Yu OY, Yin IX, Lam WYH, Chu CH. Topical Agents for Nonrestorative Management of Dental Erosion: A Narrative Review. Healthcare. 2022; 10(8):1413. https://doi.org/10.3390/healthcare10081413
Chicago/Turabian StyleChawhuaveang, Darren Dhananthat, Ollie Yiru Yu, Iris Xiaoxue Yin, Walter Yu Hang Lam, and Chun Hung Chu. 2022. "Topical Agents for Nonrestorative Management of Dental Erosion: A Narrative Review" Healthcare 10, no. 8: 1413. https://doi.org/10.3390/healthcare10081413
APA StyleChawhuaveang, D. D., Yu, O. Y., Yin, I. X., Lam, W. Y. H., & Chu, C. H. (2022). Topical Agents for Nonrestorative Management of Dental Erosion: A Narrative Review. Healthcare, 10(8), 1413. https://doi.org/10.3390/healthcare10081413