
Can Social Media Be Used as a Community-Building and Support Tool among Jewish Women Impacted by Breast and Ovarian Cancer? An Evidence-Based Observational Report

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Sampling and Constructs
2.3. Analyses
3. Results
3.1. Sample Characteristics
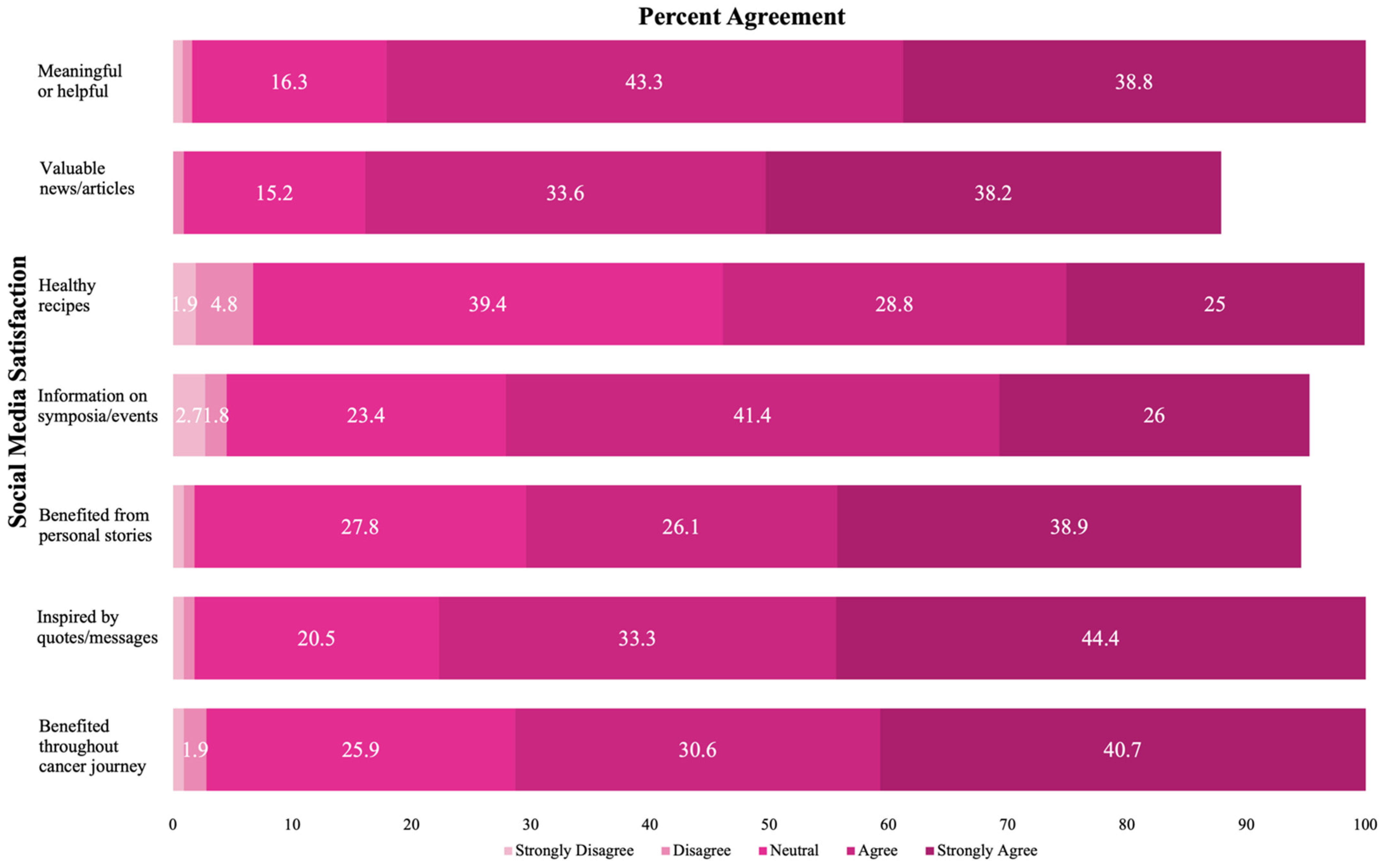
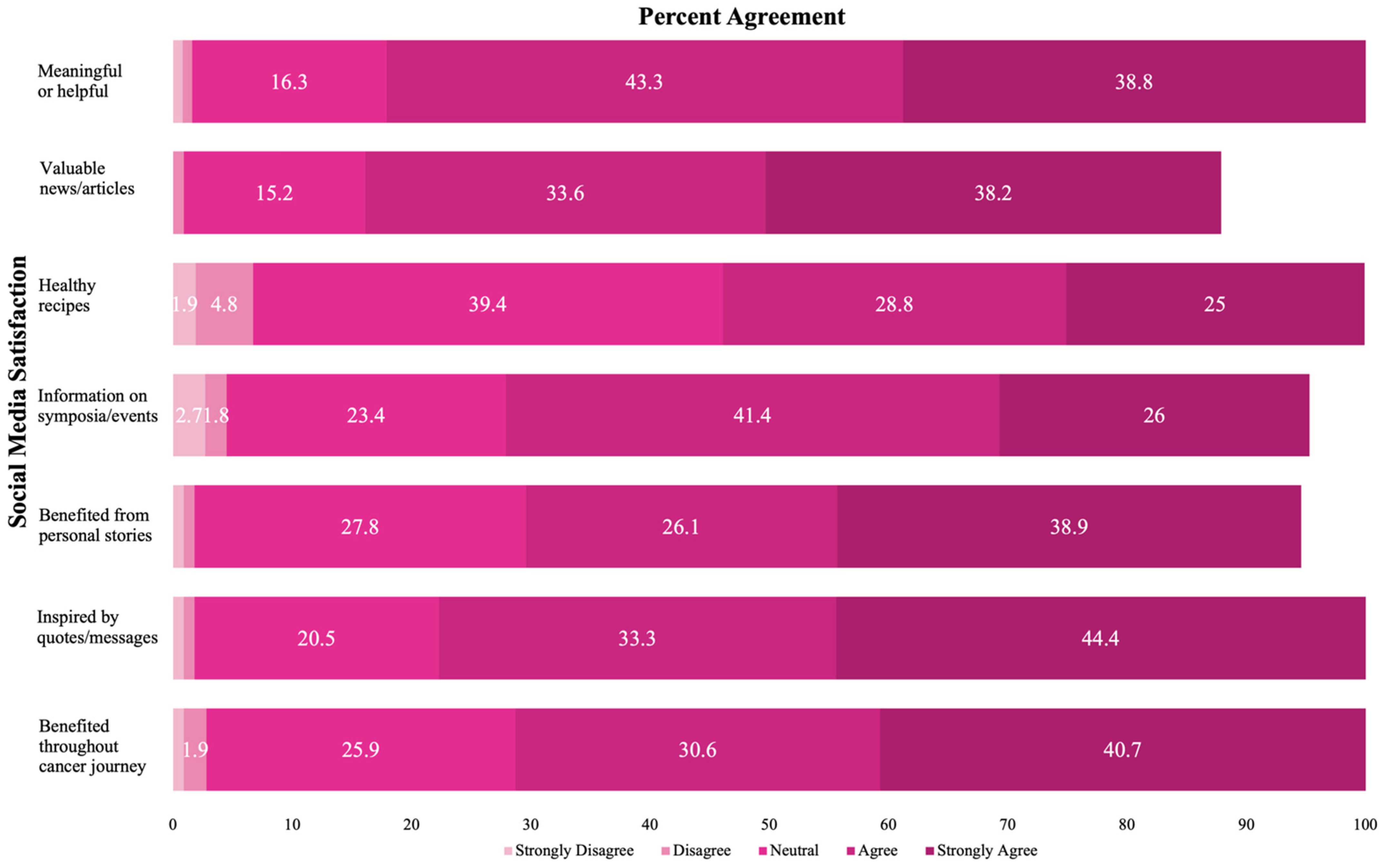
3.2. Constituents’ Social Media Engagement and Satisfaction
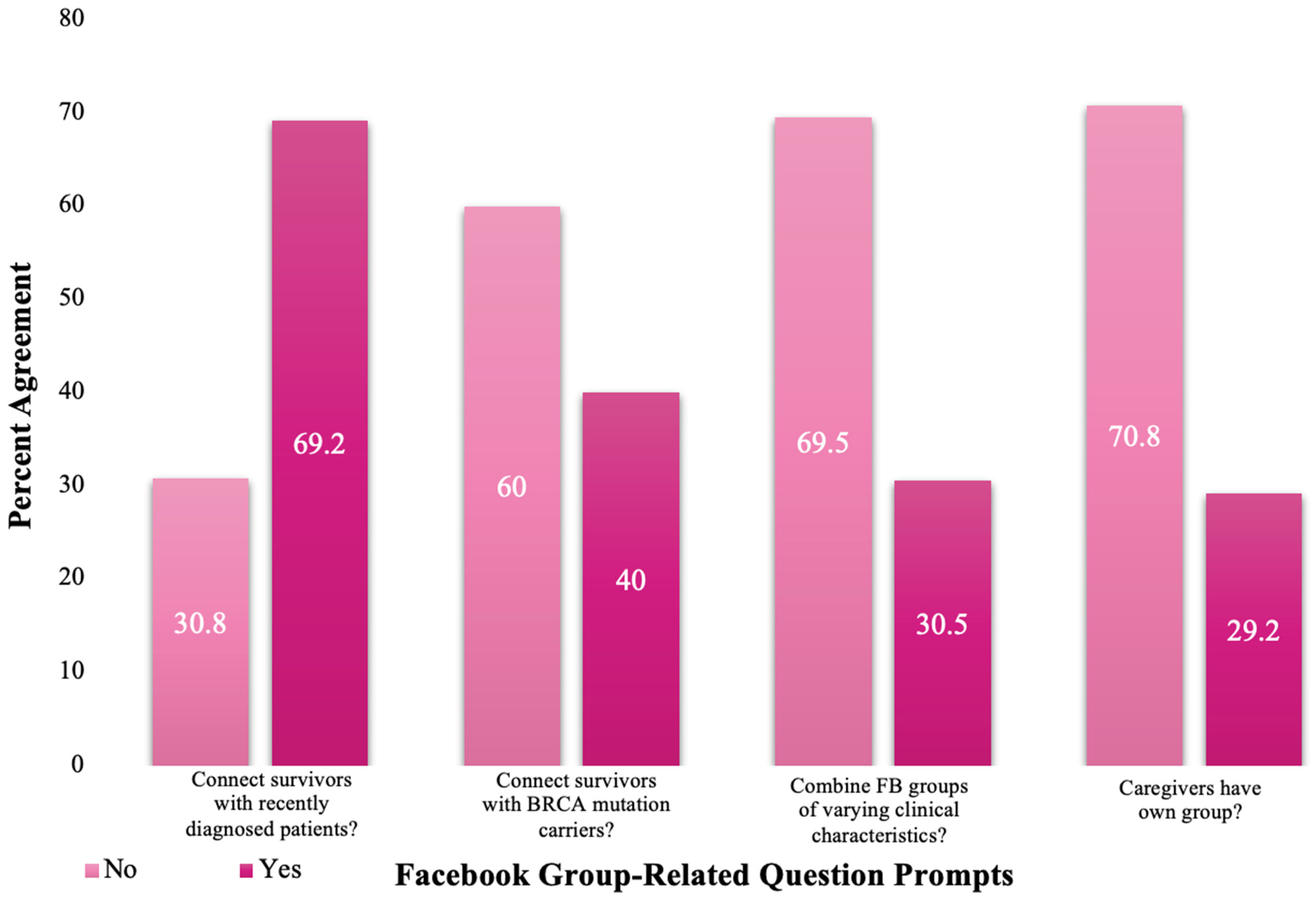
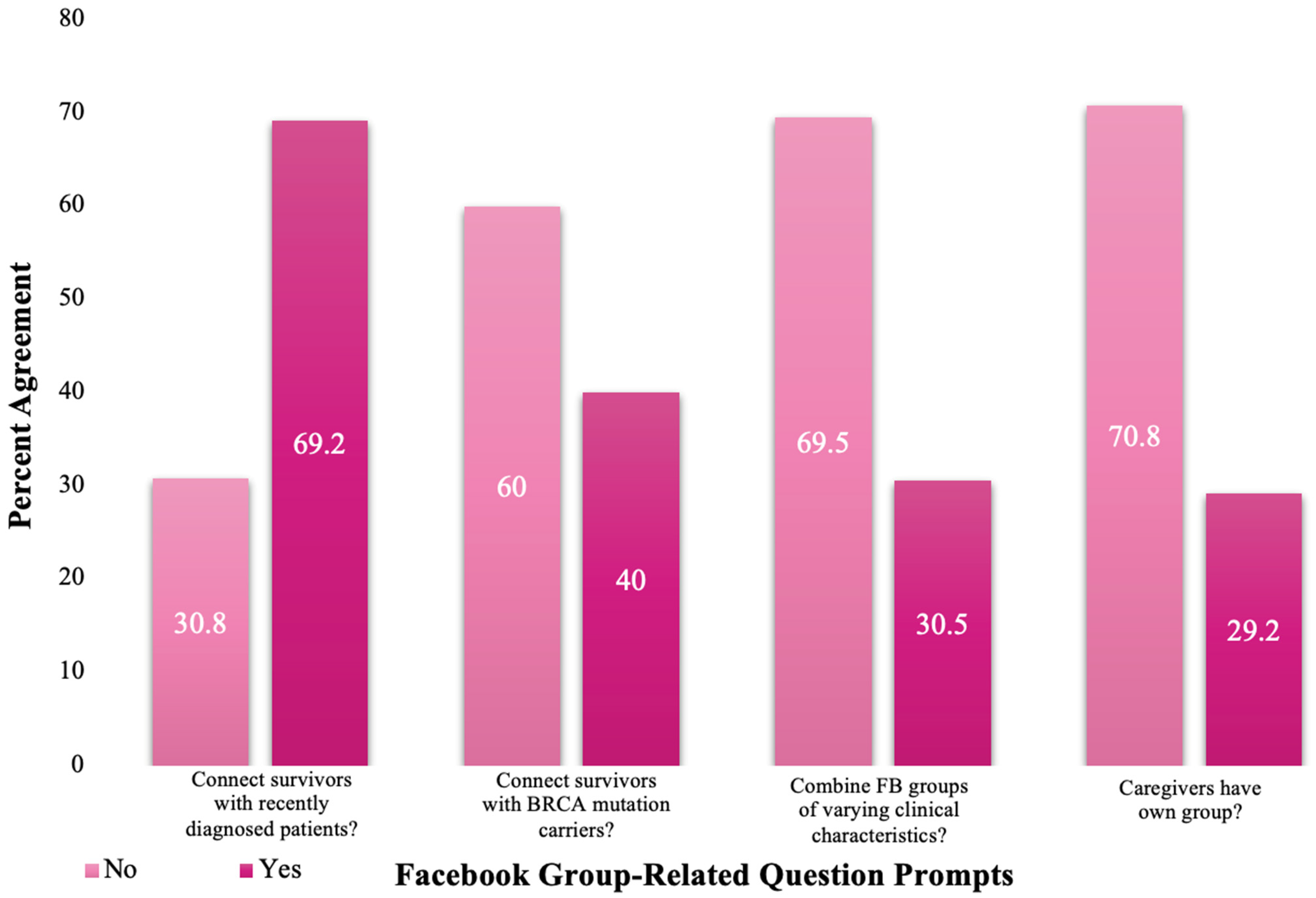
3.3. Constituents’ Facebook Group Feedback
3.4. Key Informant Interview Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- US Preventative Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; et al. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: US Preventative Services Task Force Recommendation Statement. JAMA 2019, 322, 652–665. [Google Scholar]
- Study Estimates Breast/Ovarian Cancer Risk by Age for Women with BRCA Mutations. Available online: https://www.breastcancer.org/research-news/risk-estimates-by-age-for-brca-mutations (accessed on 9 June 2021).
- How Common Is Breast Cancer? Breast Cancer Statistics. Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 9 June 2021).
- Key Statistics for Ovarian Cancer. Available online: https://www.cancer.org/cancer/ovarian-cancer/about/key-statistics.html (accessed on 9 June 2021).
- Moriarty, C. Too Young to Screen: Breast Cancer in Younger Women. Available online: https://www.yalemedicine.org/news/breast-cancer-younger-women (accessed on 10 June 2021).
- Solano, A.R.; Liria, N.C.; Jalil, F.S.; Faggionato, D.M.; Mele, P.G.; Mampel, A.; Cardoso, F.C.; Podesta, E.J. BRCA1 and BRCA2 Mutations Other Than the Founder Alleles Among Ashkenazi Jewish in the Population of Argentina. Front. Oncol. 2018, 8, 323. [Google Scholar] [CrossRef] [PubMed]
- Reducing Cancer Risk When You Are BRCA-Positive. Available online: https://www.uofmhealth.org/health-library/abo7122 (accessed on 10 June 2021).
- Tercyak, K.P.; Silber, E.; Johnson, A.C.; Fleischmann, A.; Murphy, S.E.; Mays, D.; O’Neill, S.C.; Sharkey, C.M.; Shoretz, R. Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience. Healcare 2015, 3, 324–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heldman, A.B.; Schindelar, J.; Weaver, J.B. Social Media Engagement and Public Health Communication: Implications for Public Health Organizations Being Truly “Social”. Public Heal. Rev. 2013, 35, 13. [Google Scholar] [CrossRef] [Green Version]
- Allicock, M.; Haynes-Maslow, L.; Johnson, L.-S.; Carpenter, W.R.; Vines, A.I.; Belle, D.G.; Phillips, R.; Cherry, M.W. Peer Connect for African American breast cancer survivors and caregivers: A train-the-trainer approach for peer support. Transl. Behav. Med. 2017, 7, 495–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conley, C.; Otto, A.; McDonnell, G.; Tercyak, K. Multiple Approaches to Enhancing Cancer Communication in the Next Dec-ade: Translating Research into Practice and Policy. Transl. Behav. Med. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Rehberg, K.; Fleischmann, A.; Silber, E.; O’neill, S.C.; Lewis, F.M.; Tercyak, K.P. Facilitators of Peer Coaching/Support Engagement and Dissemination among Women at Risk for and Surviving with Breast Cancer. Transl. Behav. Med. 2019, 11, 153–160. [Google Scholar] [CrossRef]
- Lazard, A.J.; Collins, M.K.R.; Hedrick, A.; Varma, T.; Love, B.; Valle, C.G.; Brooks, E.; Benedict, C. Using Social Media for Peer-to-Peer Cancer Support: Interviews With Young Adults With Cancer. JMIR Cancer 2021, 7, e28234. [Google Scholar] [CrossRef]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Rev. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Moraliyage, H.; De Silva, D.; Ranasinghe, W.; Adikari, A.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Cancer in Lockdown: Impact of the COVID -19 Pandemic on Patients with Cancer. Oncologist 2020, 26, e342–e344. [Google Scholar] [CrossRef]
- Colomer-Lahiguera, S.; Ribi, K.; Dunnack, H.J.; Cooley, M.E.; Hammer, M.J.; Miaskowski, C.; Eicher, M. Experiences of People Affected by Cancer during the Outbreak of the COVID-19 Pandemic: An Exploratory Qualitative Analysis of Public Online Forums. Support. Care Cancer 2021, 29, 4979–4985. [Google Scholar] [CrossRef]
- Bender, J.L.; Jimenez-Marroquin, M.-C.; Jadad, A.R. Seeking Support on Facebook: A Content Analysis of Breast Cancer Groups. J. Med. Internet. Res. 2011, 13, e16. [Google Scholar] [CrossRef]
- Framework for Program Evaluation—CDC. Available online: https://www.cdc.gov/eval/framework/index.htm (accessed on 10 June 2021).
- Waldrop, D.P.; O’Connor, T.L.; Trabold, N. “Waiting for the other shoe to drop”: Distress and coping during and after treatment for breast cancer. J. Psychosoc. Oncol. 2011, 29, 450–473. [Google Scholar] [PubMed]
- Mikal, J.P.; Beckstrand, M.J.; Grande, S.W.; Parks, E.; Oyenuga, M.; Odebunmi, T.; Okedele, O.; Uchino, B.; Horvath, K. Online Support Seeking and Breast Cancer Patients: Changes in Support Seeking Behavior following Diagnosis and Transition off Cancer Therapy. Heal. Commun. 2021, 36, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.; Hamilton, R.; Tercyak, K.; Peshkin, B.; Rabemananjara, K.; Isaacs, C.; O’Neill, S. Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support. Healthcare 2016, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Lazard, A.J.; Collins, M.K.R.; Hedrick, A.; Horrell, L.N.; Varma, T.; Love, B.; Valle, C.G.; Benedict, C. Initiation and Changes in Use of Social Media for Peer Support among Young Adult Cancer Patients and Survivors. Psycho-Oncology 2021, 30, 1859–1865. [Google Scholar] [CrossRef]
- Winzelberg, A.J.; Classen, C.; Alpers, G.W.; Roberts, H.; Koopman, C.; Adams, R.E.; Ernst, H.; Dev, P.; Taylor, C.B. Evaluation of an internet support group for women with primary breast cancer. Cancer 2003, 97, 1164–1173. [Google Scholar] [CrossRef] [PubMed]
- Falisi, A.L.; Wiseman, K.P.; Gaysynsky, A.; Scheideler, J.K.; Ramin, D.A.; Chou, W.-Y.S. Social media for breast cancer survivors: A literature review. J. Cancer Surviv. 2017, 11, 808–821. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Mean | SD | n | % | |
|---|---|---|---|---|
| Demographics | ||||
| Age (n = 128) | 51.8 | 11.9 | - | - |
| Marital Status (n = 131) | - | - | ||
| Married/Partnered | - | - | 90 | 68.7 |
| Separated/Divorced/Widowed/Single/Never Married | - | - | 41 | 31.3 |
| Religious Affiliation (n = 131) | - | - | - | - |
| Jewish Descent | - | - | 86 | 65.6 |
| Ashkenazi | - | - | 79 | 60.3 |
| Clinical Characteristics | ||||
| Among Survivors, Age at Cancer Diagnosis (n = 109) | 54.0 | 51.8 | - | - |
| Cancer Survivor (n = 131) | - | - | - | - |
| Yes | - | - | 110 | 0.84 |
| No | - | - | 21 | 0.16 |
| Cancer Status (n = 166) | - | - | - | - |
| At high risk for HBOC, BRCA1/2 carrier | - | - | 31 | 23.7 |
| Recently diagnosed with breast cancer | - | - | 16 | 12.2 |
| Living with breast cancer | - | - | 33 | 25.2 |
| A breast cancer survivor | - | - | 55 | 42.0 |
| Recently diagnosed with ovarian cancer | - | - | 0 | 0 |
| Living with ovarian cancer | - | - | 9 | 6.9 |
| An ovarian cancer survivor | - | - | 10 | 7.6 |
| Other | - | - | 12 | 9.2 |
| Family Composition | ||||
| Respondents with Children (n = 130) | - | - | - | - |
| Yes | - | - | 94 | 72.3 |
| No | - | - | 36 | 27.7 |
| Number of Children (n = 130) | - | - | - | - |
| 0 | - | - | 36 | 27.7 |
| 1–2 | - | - | 61 | 46.9 |
| 3 or more | - | - | 33 | 25.4 |
| Age(s) of Child(ren), in years (n = 129) | - | - | - | - |
| 0–9 | - | - | 22 | 16.8 |
| 10–17 | - | - | 42 | 32.1 |
| 18+ | - | - | 65 | 49.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dunn, C.; Campbell, S.; Marku, N.; Fleischmann, A.; Silber, E.; Rosen, M.; Tercyak, K.P. Can Social Media Be Used as a Community-Building and Support Tool among Jewish Women Impacted by Breast and Ovarian Cancer? An Evidence-Based Observational Report. Healthcare 2022, 10, 51. https://doi.org/10.3390/healthcare10010051
Dunn C, Campbell S, Marku N, Fleischmann A, Silber E, Rosen M, Tercyak KP. Can Social Media Be Used as a Community-Building and Support Tool among Jewish Women Impacted by Breast and Ovarian Cancer? An Evidence-Based Observational Report. Healthcare. 2022; 10(1):51. https://doi.org/10.3390/healthcare10010051
Chicago/Turabian StyleDunn, Catherine, Sydney Campbell, Nikoleta Marku, Adina Fleischmann, Elana Silber, Melissa Rosen, and Kenneth P. Tercyak. 2022. "Can Social Media Be Used as a Community-Building and Support Tool among Jewish Women Impacted by Breast and Ovarian Cancer? An Evidence-Based Observational Report" Healthcare 10, no. 1: 51. https://doi.org/10.3390/healthcare10010051
APA StyleDunn, C., Campbell, S., Marku, N., Fleischmann, A., Silber, E., Rosen, M., & Tercyak, K. P. (2022). Can Social Media Be Used as a Community-Building and Support Tool among Jewish Women Impacted by Breast and Ovarian Cancer? An Evidence-Based Observational Report. Healthcare, 10(1), 51. https://doi.org/10.3390/healthcare10010051