
Association between Teenage Pregnancy and Family Factors: An Analysis of the Philippine National Demographic and Health Survey 2017


Abstract
1. Introduction
2. Materials and Methods
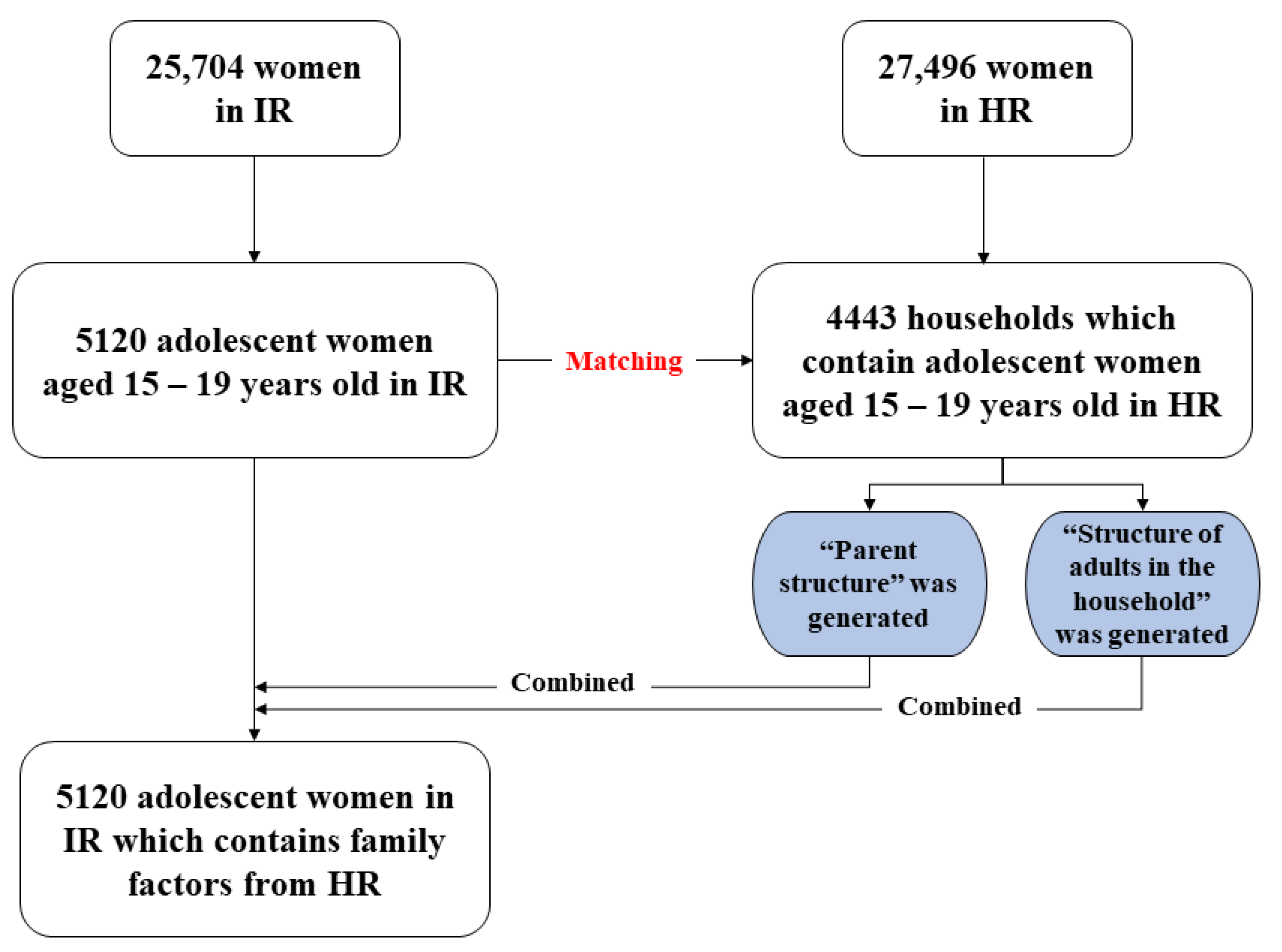
2.1. Data Preparation
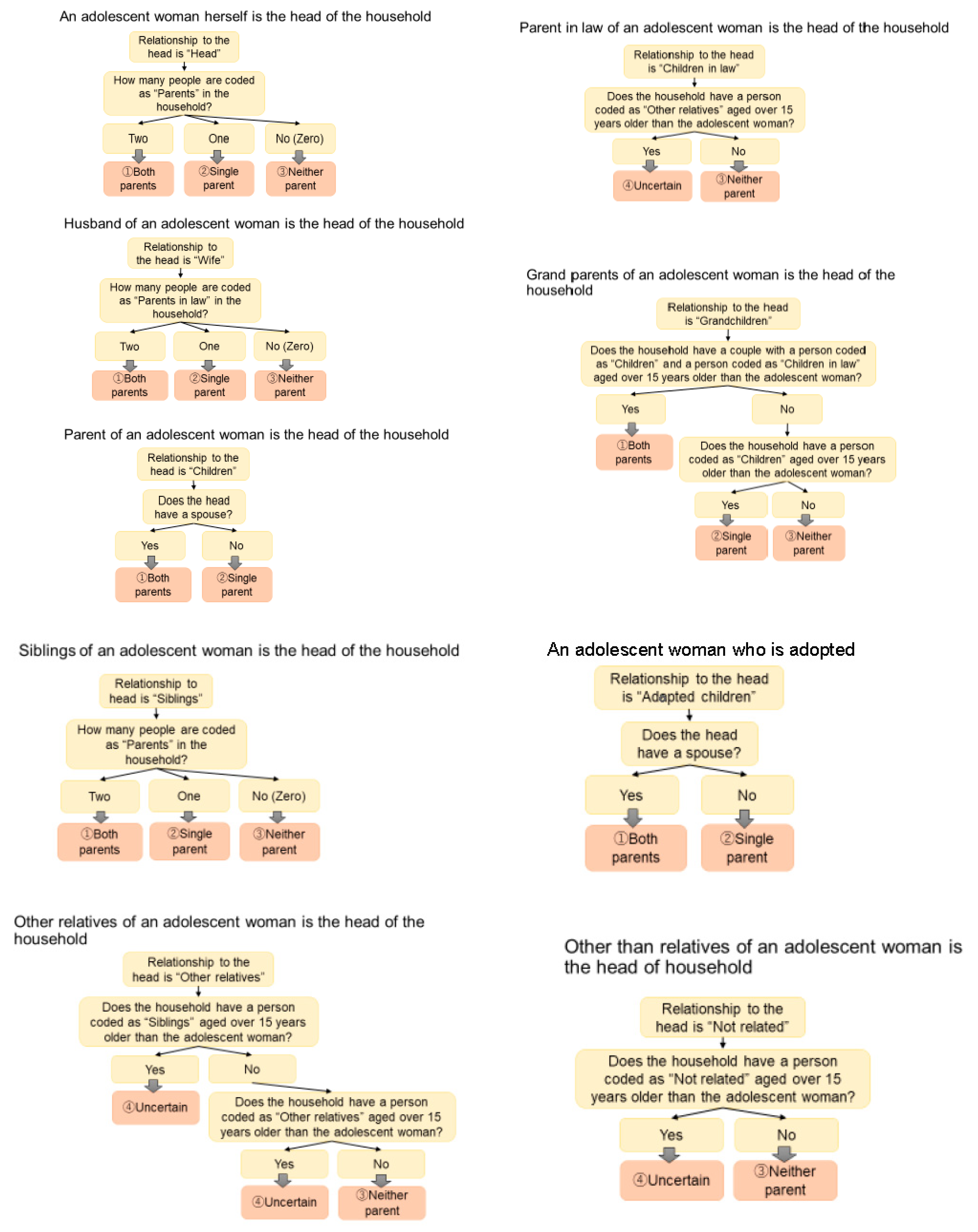
2.2. Outcome Variable
2.3. Exposure Variables
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Teenage Pregnancy
3.2. Association between Teenage Pregnancy and Factors
3.3. Results from Multivariable Logistic Regression
4. Discussion
4.1. Relation of Family Factors on Teenage Pregnancy
4.2. SES and Teenage Pregnancy
4.3. Role of Age on Teenage Pregnancy
4.4. Counterintuitive Result about Knowledge of Contraception
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNFPA; UNESCO; WHO. Sexual and Reproductive Health of Young People in Asia and Pacific: A Review of Issues, Policies and Programmes; UNFPA: Bangkok, Thailand, 2015; p. 129.
- Santos, M.I.; Rosário, F. A score for assessing the risk of first-time adolescent pregnancy. Fam. Pract. 2011, 28, 482–488. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sawyer, S.M.; Afifi, R.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Ganchimeg, T.; Ota, E.; Morisaki, N.; Laopaiboon, M.; Lumbiganon, P.; Zhang, J.; Yamdamsuren, B.; Temmerman, M.; Say, L.; Tunçalp, Ö; et al. Pregnancy and childbirth outcomes among adolescent mothers: A World Health Organization multicountry study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 40–48. [Google Scholar] [CrossRef]
- UNICEF (Ed.) Adolescence: An Age of Opportunity; UNICEF: New York, NY, USA, 2011. [Google Scholar]
- Singh, S. Adolescent Childbearing in Developing Countries: A Global Review. Stud. Fam. Plan. 1998, 29, 117–136. [Google Scholar] [CrossRef]
- Hediger, M.L.; Scholl, T.O.; Schall, J.I.; Krueger, P.M. Young maternal age and preterm labor. Ann. Epidemiol. 1997, 7, 400–406. [Google Scholar] [CrossRef]
- World Bank. Adolescent Fertility Rate (Births per 1000 Women Ages 15–19)|Data; World Bank Open Dataadoles: Washington, DC, USA, 2018. [Google Scholar]
- World Health Organization. Risk and Protective Factors Affecting Adolescent Reproductive Health in Developing Countries: An Analysis of Adolescent Sexual and Reproductive Health Literature from around the World: Summary/[Robert Blum and Kristin Mmari]; World Health Organization: Geneva, Switzerland, 2004; p. 17.
- Mmari, K.; Sabherwal, S. A Review of Risk and Protective Factors for Adolescent Sexual and Reproductive Health in Developing Countries: An Update. J. Adolesc. Health 2013, 53, 562–572. [Google Scholar] [CrossRef]
- Maness, S.B.; Buhi, E.R.; Daley, E.M.; Baldwin, J.A.; Kromrey, J.D. Social Determinants of Health and Adolescent Pregnancy: An Analysis From the National Longitudinal Study of Adolescent to Adult Health. J. Adolesc. Health 2016, 58, 636–643. [Google Scholar] [CrossRef]
- Habitu, Y.A.; Yalew, A.; Bisetegn, T.A. Prevalence and Factors Associated with Teenage Pregnancy, Northeast Ethiopia, 2017: A Cross-Sectional Study. J. Pregnancy 2018, 2018, 1714527. [Google Scholar] [CrossRef] [PubMed]
- Mathewos, S.; Mekuria, A. Teenage Pregnancy and Its Associated Factors among School Adolescents of Arba Minch Town, Southern Ethiopia. Ethiop. J. Health Sci. 2018, 28, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Gaudie, J.; Mitrou, F.; Lawrence, D.; Stanley, F.J.; Silburn, S.R.; Zubrick, S.R. Antecedents of teenage pregnancy from a 14-year follow-up study using data linkage. BMC Public Health 2010, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, H.; Kågesten, A.; Emerson, M.; Decker, M.; Olumide, A.; Ojengbede, O.; Lou, C.; Sonenstein, F.L.; Blum, R.W.; Delany-Moretlwe, S. Prevalence and Determinants of Adolescent Pregnancy in Urban Disadvantaged Settings Across Five Cities. J. Adolesc. Health 2014, 55, S48–S57. [Google Scholar] [CrossRef]
- ICF. Demographic and Health Surveys Standard Recode Manual for DHS7; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Croft, T.N.; Aileen, M.J.M.; Courtney, K.A.; Arnold, F.; Assaf, S.; Balian, S.; Bekele, Y.; Bizimana, J.d.D.; Burgert, C.; Collison, D.; et al. Guide to DHS Statistics; USAID: Rockville, MD, USA, 2018.
- Yansaneh, I.S. Construction and Use of Sample Weights. Designing Household Survey Samples; United Nations: Geneva, Switzerland, 2008; pp. 109–127. [Google Scholar] [CrossRef]
- DHS Program. In Part III: Demonstration of How to Weight DHS Data in Stata—YouTube; USAID: Rockville, MD, USA, 2015.
- Enders, C.K. Using the Expectation Maximization Algorithm to Estimate Coefficient Alpha for Scales with Item-Level Missing Data. Psychol. Methods 2003, 8, 322–337. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Kassa, G.M.; Arowojolu, A.O.; Odukogbe, A.A.; Yalew, A.W. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and Meta-analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef]
- Yakubu, I.; Salisu, W.J. Determinants of adolescent pregnancy in sub-Saharan Africa: A systematic review. Reprod. Health 2018, 15, 15. [Google Scholar] [CrossRef] [PubMed]
- Demographic Research and Development Foundation (DRDF). 2013 YAFS4 Key Findings; University of the Philippines Population Institute (UPPI): Queson, Philippines, 2014. [Google Scholar]
- De Irala, J.; Osorio, A.; Del Burgo, C.L.; Belen, V.; De Guzman, F.; Calatrava, M.D.C.; Torralba, A.N. Relationships, love and sexuality: What the Filipino teens think and feel. BMC Public Health 2009, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Skosana, M.T.; Peu, M.D.; Mogale, R.S. Disconnections and exclusions of parents in the prevention of teenage pregnancy: A phenomenological approach. Int. J. Afr. Nurs. Sci. 2020, 13, 100251. [Google Scholar] [CrossRef]
- Jelili, M.O.; Akindele, O.A.; Ojo, A. Teenage Pregnancy and Home Environment Factors in Ogbomoso, Nigeria. Res. Humanit. Soc. Sci. 2013, 3, 69–77. [Google Scholar]
- Anifah, F.; Dasuki, D.; Triratnawati, A. Role of family structure and parenting style in adolescent pregnancy in Surabaya, Indonesia. Maj. Obstet. Ginekol. 2018, 26, 91–97. [Google Scholar] [CrossRef]
- Uwizeye, D.; Muhayiteto, R.; Kantarama, E.; Wiehler, S.; Murangwa, Y. Prevalence of teenage pregnancy and the associated contextual correlates in Rwanda. Heliyon 2020, 6, e05037. [Google Scholar] [CrossRef]
- Kunnuji, M.O.N.; Eshiet, I.; Nnorom, C.C.P. A survival analysis of the timing of onset of childbearing among young females in Nigeria: Are predictors the same across regions? Reprod. Health 2018, 15, 173. [Google Scholar] [CrossRef]
- Poudel, S.; Upadhaya, N.; Khatri, R.B.; Ghimire, P.R. Trends and factors associated with pregnancies among adolescent women in Nepal: Pooled analysis of Nepal Demographic and Health Surveys (2006, 2011 and 2016). PLoS ONE 2018, 13, e0202107. [Google Scholar] [CrossRef]
- Mohr, R.; Carbajal, J.; Sharma, B.B. The Influence of Educational Attainment on Teenage Pregnancy in Low-Income Countries: A Systematic Literature Review. J. Soc. Work. Glob. Community 2019, 4, 2. [Google Scholar] [CrossRef]
- Ahinkorah, B.O.; Hagan, J.E.J.; Seidu, A.-A.; Budu, E.; Hormenu, T.; Mintah, J.K.; Sambah, F.; Schack, T. Access to Adolescent Pregnancy Prevention Information and Services in Ghana: A Community-Based Case-Control Study. Front. Public Health 2019, 7, 382. [Google Scholar] [CrossRef] [PubMed]
- Wado, Y.D.; Sully, E.A.; Mumah, J.N. Pregnancy and early motherhood among adolescents in five East African countries: A multi-level analysis of risk and protective factors. BMC Pregnancy Childbirth 2019, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Ayele, B.G.; Gebregzabher, T.G.; Hailu, T.T.; Assefa, B.A. Determinants of teenage pregnancy in Degua Tembien District, Tigray, Northern Ethiopia: A community-based case-control study. PLoS ONE 2018, 13, e0200898. [Google Scholar] [CrossRef]
- Pradhan, R.; Wynter, K.; Fisher, J. Factors Associated with Pregnancy among Married Adolescents in Nepal: Secondary Analysis of the National Demographic and Health Surveys from 2001 to 2011. Int. J. Environ. Res. Public Health 2018, 15, 229. [Google Scholar] [CrossRef]
- Birhanu, B.E.; Kebede, D.L.; Kahsay, A.B.; Belachew, A.B. Predictors of teenage pregnancy in Ethiopia: A multilevel analysis. BMC Public Health 2019, 19, 601. [Google Scholar] [CrossRef] [PubMed]
- Ochen, A.M.; Chi, P.C.; Lawoko, S. Predictors of teenage pregnancy among girls aged 13–19 years in Uganda: A community based case-control study. BMC Pregnancy Childbirth 2019, 19, 211. [Google Scholar] [CrossRef]
- Kaphagawani, N.C.; Kalipeni, E. Sociocultural factors contributing to teenage pregnancy in Zomba district, Malawi. Glob. Public Health 2017, 12, 694–710. [Google Scholar] [CrossRef] [PubMed]
- Giedd, J.N.; Blumenthal, J.; Jeffries, N.O.; Castellanos, F.; Liu, H.; Zijdenbos, A.; Paus, T.; Evans, A.C.; Rapoport, J.L. Brain development during childhood and adolescence: A longitudinal MRI study. Nat. Neurosci. 1999, 2, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.; Getz, S.; Galvan, A. The adolescent brain. Dev. Rev. 2008, 28, 62–77. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Main Variable | Parent Structure |
|---|---|
| Family variable | |
| Relationship to head Sex of household head Age of household head Number of household members Structure of adults in the household | |
| Individual variable | |
| Sociodemographic variable | Age Residence Religion Ethnicity Educational attainment Wealth quintiles Marital status Current working status Occupation |
| Personal behavior factor | Media exposure Substance use |
| Family planning factors | Knowledge of contraception Knowledge of condom Current use of contraception Type of contraception currently using Contraception ever used Preferable contraception method Future intention to use contraception Perception to parental consent for obtaining contraception Access to contraception information |
| Sexual activities | Age of the first sexual intercourse Age of first birth Age of menarche onset Number of ideal children in the future |
| Variable | N | (%) | Teenage Pregnancy | Crude OR (CI) | p-Value | |
|---|---|---|---|---|---|---|
| N | (%) | |||||
| Parent structure | ||||||
| Both parents | 3364 | 66.09 | 138 | 31.87 | Reference | |
| Single parent | 772 | 15.17 | 48 | 11.09 | 1.55 (1.10, 2.16) | 0.0111 * |
| Neither parent | 954 | 18.74 | 247 | 57.04 | 8.17 (6.54, 10.23) | <0.001 *** |
| NA | 30 | 0.59 | 0 | 0 | - | - |
| Age | 2.22 (2.02, 2.44) | 0.001 *** | ||||
| Residence | ||||||
| Urban | 1702 | 33.24 | 123 | 28.41 | Reference | 0 |
| Rural | 3418 | 66.76 | 310 | 71.59 | 1.28 (1.03, 1.60) | 0.0259 * |
| Educational attainment (continuous) | 0.85 (0.81, 0.88) | <0.001 *** | ||||
| Educational attainment (categorical) | ||||||
| No education | 16 | 0.31 | 3 | 0.69 | Reference | |
| Incomplete primary | 180 | 3.52 | 55 | 12.7 | 1.91 (0.59, 8.56) | 0.3286 |
| Complete primary | 186 | 3.63 | 51 | 11.78 | 1.64 (0.50, 7.35) | 0.456 |
| Incomplete secondary | 3660 | 71.48 | 183 | 42.26 | 0.23 (0.07, 1.00) | 0.0219 * |
| Complete secondary | 292 | 5.7 | 97 | 22.4 | 2.16 (0.68, 9.56) | 0.2391 |
| Higher education | 786 | 15.35 | 44 | 10.16 | 0.26 (0.08, 1.15) | 0.0392 * |
| Wealth quintiles | ||||||
| Poorest | 1210 | 23.63 | 167 | 38.57 | 1.77 (1.34, 2.34) | <0.001 *** |
| Poorer | 1213 | 23.69 | 112 | 25.87 | 1.12 (0.84, 1.51) | 0.4482 |
| Middle | 1010 | 19.73 | 84 | 19.4 | Reference | |
| Richer | 894 | 17.46 | 44 | 10.16 | 0.57 (0.39, 0.83) | <0.0035 ** |
| Richest | 793 | 15.49 | 26 | 6 | 0.37 (0.23, 0.58) | <0.001 *** |
| Working status | ||||||
| No | 4187 | 81.78 | 327 | 75.52 | Reference | |
| In the past year | 343 | 6.7 | 51 | 11.78 | 2.06 (1.49, 2.81) | <0.001 *** |
| Currently working | 571 | 11.15 | 52 | 12.01 | 1.18 (0.86, 1.59) | 0.283 |
| Working, but on leave last 7 days | 19 | 0.37 | 3 | 0.69 | 2.21 (0.51, 6.69) | 0.209 |
| Smoking tobacco | ||||||
| FALSE | 5001 | 97.68 | 408 | 94.23 | Reference | |
| TRUE | 119 | 2.32 | 25 | 5.77 | 2.99 (1.87, 4.63) | <0.001 *** |
| Internet use | ||||||
| Never | 834 | 16.29 | 124 | 28.64 | Reference | |
| Yes, last 12 month | 4200 | 82.03 | 293 | 67.67 | 0.43 (0.34, 0.54) | <0.0001 *** |
| Yes, before last 12 months | 86 | 1.68 | 16 | 3.7 | 1.31 (0.71, 2.27) | 0.36 |
| Age of menarche onset | 1.11 (1.03, 1.19) | 0.009 ** | ||||
| Knowledge of contraception | 1.17 (1.14, 1.20) | <0.001 *** | ||||
| Number of household members | 1.04 (1.00 1, 1.08) | 0.0322 * | ||||
| Age of household head | 0.96 (0.96, 0.97) | <0.001 *** | ||||
| Variable | Adjusted OR | (95% CI) |
|---|---|---|
| Parent structure | ||
| Both parents | Reference | |
| Single parent | 1.49 | (0.67, 3.31) |
| Neither parent | 4.57 | (2.56, 8.15) |
| Age | 2.17 | (1.91, 2.46) |
| Educational attainment (categorical) | ||
| No education | Reference | |
| Incomplete primary | 2.22 | (0.38, 12.96) |
| Complete primary | 1.88 | (0.32, 10.96) |
| Incomplete secondary | 0.31 | (0.06, 1.74) |
| Complete secondary | 0.81 | (0.14, 4.62) |
| Higher education | 0.08 | (0.01, 0.49) |
| Wealth quintiles | ||
| Poorest | 0.93 | (0.55, 1.58) |
| Poorer | 0.89 | (0.52, 1.51) |
| Middle | Reference | |
| Richer | 0.71 | (0.38, 1.32) |
| Richest | 0.4 | (0.18, 0.92) |
| Knowledge of contraception | 1.27 | (1.22, 1.32) |
| Number of household members | 1.14 | (1.09, 1.20) |
| Interaction of wealth quintiles | ||
| Single parent * poorest | 0.85 | (0.26, 2.74) |
| Neither parent * poorest | 3.55 | (1.67, 7.55) |
| Single parent * poorer | 1.01 | (0.34. 3.04) |
| Neither parent * poorer | 1.74 | (0.80, 3.78) |
| Single parent * richer | 2.63 | (0.82, 8.39) |
| Neither parent * richer | 0.59 | (0.23, 1.55) |
| Single parent * richest | 3 | (0.73, 12.24) |
| Neither parent * richest | 0.37 | (0.12, 1.16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabei, K.; Cuisia-Cruz, E.S.S.; Smith, C.; Seposo, X. Association between Teenage Pregnancy and Family Factors: An Analysis of the Philippine National Demographic and Health Survey 2017. Healthcare 2021, 9, 1720. https://doi.org/10.3390/healthcare9121720
Tabei K, Cuisia-Cruz ESS, Smith C, Seposo X. Association between Teenage Pregnancy and Family Factors: An Analysis of the Philippine National Demographic and Health Survey 2017. Healthcare. 2021; 9(12):1720. https://doi.org/10.3390/healthcare9121720
Chicago/Turabian StyleTabei, Kozue, Erlinda Susana S. Cuisia-Cruz, Chris Smith, and Xerxes Seposo. 2021. "Association between Teenage Pregnancy and Family Factors: An Analysis of the Philippine National Demographic and Health Survey 2017" Healthcare 9, no. 12: 1720. https://doi.org/10.3390/healthcare9121720
APA StyleTabei, K., Cuisia-Cruz, E. S. S., Smith, C., & Seposo, X. (2021). Association between Teenage Pregnancy and Family Factors: An Analysis of the Philippine National Demographic and Health Survey 2017. Healthcare, 9(12), 1720. https://doi.org/10.3390/healthcare9121720