
Post-Hypoxic Myoclonus Status following Out-of-Hospital Cardiac Arrest—Does It still Predict a Poor Outcome? A Retrospective Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. System Setting
2.2. Data Collection
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Variables
- Age;
- Sex;
- Initial cardiac rhythm;
- Time to ROSC;
- EEG obtained at the hospital;
- Any myoclonic convulsions at the ICU.
- Cerebral Performance Score.
2.6. Statistical Methods
2.7. Ethical Considerations
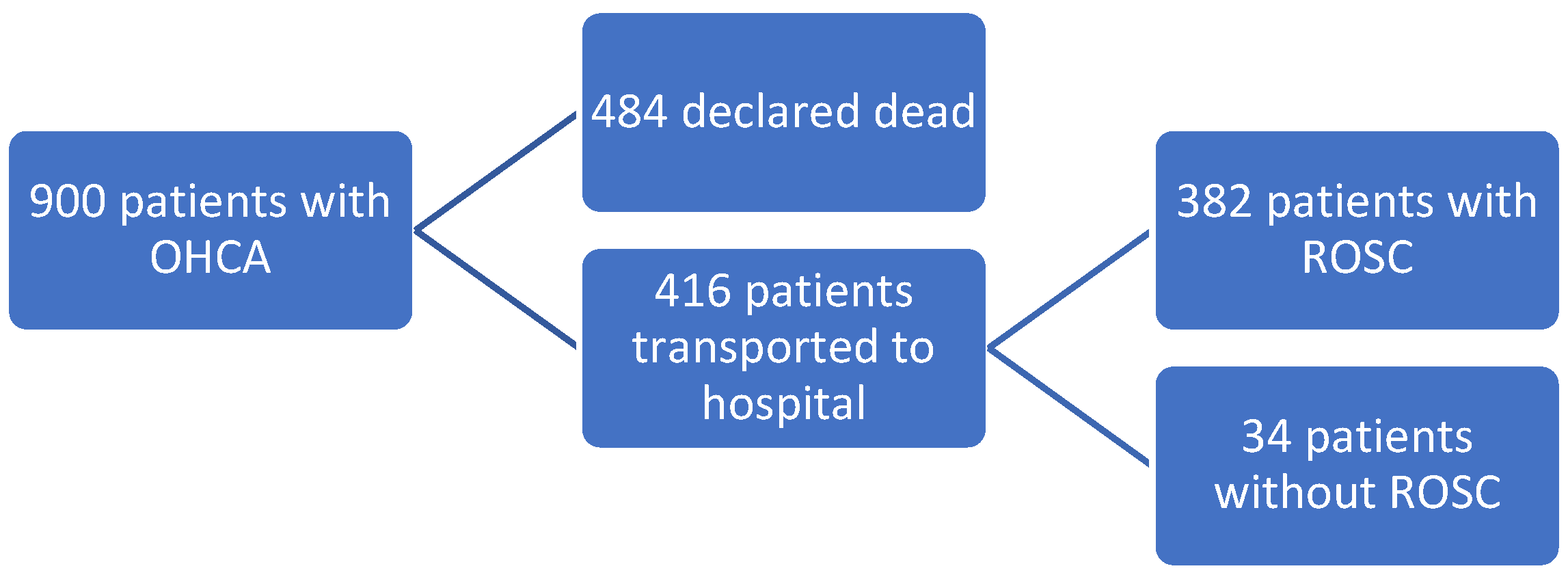
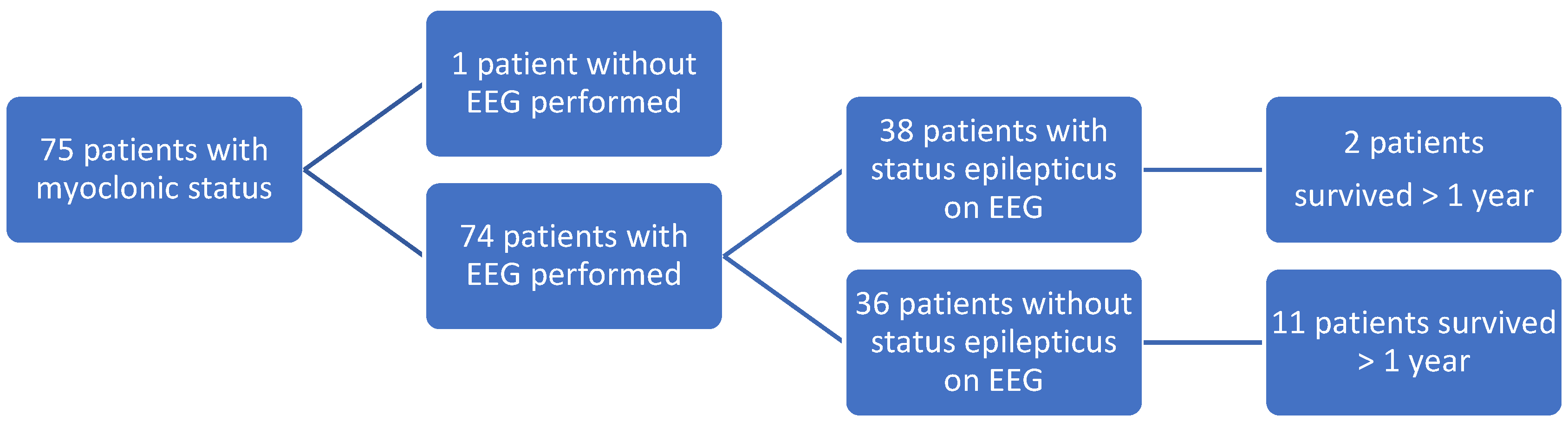
3. Results
Survival in OHCA Patients with Myoclonic Status
4. Discussion
4.1. Outcome
4.2. The Prehospital Setting
4.3. The in-Hospital Setting
4.4. OHCA, Then and Now
4.5. Limitations
4.6. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Danish Cardiac Arrest Registry. (In Danish). Available online: http://hjertestopregister.dk/wp-content/uploads/2019/11/Dansk-Hjertestopregister-2018-2.pdf (accessed on 27 October 2021).
- Rajan, S.; Folke, F.; Hansen, S.M.; Hansen, C.M.; Kragholm, K.; Gerds, T.A.; Lippert, F.; Karlsson, L.; Møller, S.; Køber, L.; et al. Resuscitation. Incidence and survival outcome according to heart rhythm during resuscitation attempt in out-of-hospital cardiac arrest patients with presumed cardiac etiology. Resuscitation 2017, 114, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Young, G.B. Myoclonus status in comatose patients after cardiac arrest. Lancet 1994, 343, 1642–1643. [Google Scholar] [CrossRef]
- Wijdicks, E.F.; Parisi, J.E.; Sharbrough, F.W. Prognostic value of myoclonus status in comatose survivors of cardiac arrest. Ann. Neurol. 1994, 35, 239–243. [Google Scholar] [CrossRef]
- Hui, A.C.; Cheng, C.; Lam, A.; Mok, V.; Joynt, G.M. Prognosis following Postanoxic Myoclonus Status epilepticus. Eur. Neurol. 2005, 54, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Cariou, A.; Cavallaro, F.; Cronberg, T.; Friberg, H.; Hoedemaekers, C.; Horn, J.; Nolan, J.P.; Rossetti, A.O.; Soar, J. Prognostication in comatose survivors of cardiac arrest: An advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1816–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thömke, F.; Weilemann, S.L. Poor prognosis despite successful treatment of postanoxic generalized myoclonus. Neurology 2010, 74, 1392–1394. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 2015, 95, 202–222. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Bottiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]
- Andersen, M.S.; Johnsen, S.P.; Sorensen, J.N.; Jepsen, S.B.; Hansen, J.B.; Christensen, E.F. Implementing a nationwide criteria-based emergency medical dispatch system: A register-based follow-up study. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 53. [Google Scholar] [CrossRef] [Green Version]
- Mikkelsen, S.; Lossius, H.M.; Toft, P.; Lassen, A.T. Characteristics and prognoses of patients treated by an anaesthesiologist-manned prehospital emergency care unit. A retrospective cohort study. BMJ Open 2017, 7, e014383. [Google Scholar] [CrossRef]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. ICD-10 Classification System. Available online: https://icd.who.int/browse10/2014/en#/I30-I52 (accessed on 27 October 2021).
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Møller, S.G.; Wissenberg, M.; Møller-Hansen, S.; Folke, F.; Malta Hansen, C.; Kragholm, K.; Bundgaard Ringgren, K.; Karlsson, L.; Lohse, N.; Lippert, F.; et al. Regional variation in out-of-hospital cardiac arrest: Incidence and survival—A nationwide study of regions in Denmark. Resuscitation 2020, 148, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Heinz, U.E.; Rollnik, J.D. Outcome and prognosis of hypoxic brain damage patients undergoing neurological early rehabilitation. BMC Res. Notes 2015, 8, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braksick, S.A.; Rabinstein, A.A.; Wijdicks, E.F.; Fugate, J.E.; Hocker, S. Post-ischemic Myoclonic Status Following Cardiac Arrest in Young Drug Users. Neurocrit. Care 2017, 26, 280–283. [Google Scholar] [CrossRef]
- Schneiderman, L.J. Defining Medical Futility and Improving Medical Care. J. Bioeth. Inq. 2011, 8, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Kragholm, K.; Wissenberg, M.; Mortensen, R.N.; Hansen, S.M.; Hansen, C.M.; Thorsteinsson, K.; Rajan, S.; Lippert, F.; Folke, F.; Gislason, G.; et al. Bystander Efforts and 1-Year Outcomes in Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2017, 376, 1737–1747. [Google Scholar] [CrossRef]
- Karlsson, L.; Hansen, C.M.; Wissenberg, M.; Møller, S.M.; Lippert, F.; Rajan, S.; Kragholm, K.; Møller, S.G.; Søndergaard, K.B.; Gislason, G.; et al. Automated external defibrillator accessibility is crucial for bystander defibrillation and survival: A registry-based study. Resuscitation 2019, 136, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Sylvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef]
- Thrane, P.G.; Kristensen, S.D.; Olesen, K.K.W.; Mortensen, L.S.; Bøtker, H.E.; Thuesen, L.; Hansen, H.S.; Abildgaard, U.; Engstrøm, T.; Andersen, H.R.; et al. 16-year follow-up of the Danish Acute Myocardial Infarction 2 (DANAMI-2) trial: Primary percutaneous coronary intervention vs. fibrinolysis in ST-segment elevation myocardial infarction. Eur. Heart J. 2020, 41, 847–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, G.B. Ultra-early application of prognostic tests for outcome after resuscitation from cardiac arrest. Resuscitation 2019, 143, 228–229. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Patients w/ Myoclonic Status and Status Epilepticus | Patients w/ Myoclonic Status | All Patients Admitted to Hospital with ROSC |
|---|---|---|---|
| Shockable Rhythm | 14 (36.8%) | 25 (33.3%) | 205 (49.3%) |
| Asystole | 19 (50%) | 37 (49.3%) | 127 (30.5%) |
| PEA | 3 (7.9%) | 10 (13.3%) | 74 (17.8%) |
| Rhythm Missing | 2 (5.3%) | 3 (4%) | 10 (2.4%) |
| Male/Female | 25/13 (65.8%/34.2%) | 53/22 (71.0%/29.0%) | 256/126 (67%/33%) |
| Age (years) (Median (Range)) | 72 (21–84) | 67 (13–91) | 66 (1–99) |
| Time to ROSC or ECMO (min) (Median (Range)) | 20 (3–35) | 18 (3–86) | 18 (2–86) |
| Coronary angiography | 18 (47.4%) | 39 (52.0%) | 85.6% * |
| Revascularisation | 7 (18.4%) | 16 (21.3%) | 54.8 % * |
| CPC Score | CPC 1 | CPC 2 | CPC 3 | CPC 4 | CPC 5 |
|---|---|---|---|---|---|
| Survivors Discharged | 7 | 1 | 2 | 1 | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brøchner, A.C.; Lindholm, P.; Jensen, M.J.; Toft, P.; Henriksen, F.L.; Lassen, J.F.; Mikkelsen, S. Post-Hypoxic Myoclonus Status following Out-of-Hospital Cardiac Arrest—Does It still Predict a Poor Outcome? A Retrospective Study. Healthcare 2022, 10, 41. https://doi.org/10.3390/healthcare10010041
Brøchner AC, Lindholm P, Jensen MJ, Toft P, Henriksen FL, Lassen JF, Mikkelsen S. Post-Hypoxic Myoclonus Status following Out-of-Hospital Cardiac Arrest—Does It still Predict a Poor Outcome? A Retrospective Study. Healthcare. 2022; 10(1):41. https://doi.org/10.3390/healthcare10010041
Chicago/Turabian StyleBrøchner, Anne C., Peter Lindholm, Margrethe J. Jensen, Palle Toft, Finn L. Henriksen, Jens F. Lassen, and Søren Mikkelsen. 2022. "Post-Hypoxic Myoclonus Status following Out-of-Hospital Cardiac Arrest—Does It still Predict a Poor Outcome? A Retrospective Study" Healthcare 10, no. 1: 41. https://doi.org/10.3390/healthcare10010041
APA StyleBrøchner, A. C., Lindholm, P., Jensen, M. J., Toft, P., Henriksen, F. L., Lassen, J. F., & Mikkelsen, S. (2022). Post-Hypoxic Myoclonus Status following Out-of-Hospital Cardiac Arrest—Does It still Predict a Poor Outcome? A Retrospective Study. Healthcare, 10(1), 41. https://doi.org/10.3390/healthcare10010041