
Effect of Peroneus Longus Muscle Release on Abductor Hallucis Muscle Activity and Medial Longitudinal Arch before Toe-Tap Exercise in Participants with Flexible Pes Planus


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.2.1. Electromyography of Abductor Hallucis and Peroneus Longus Activity
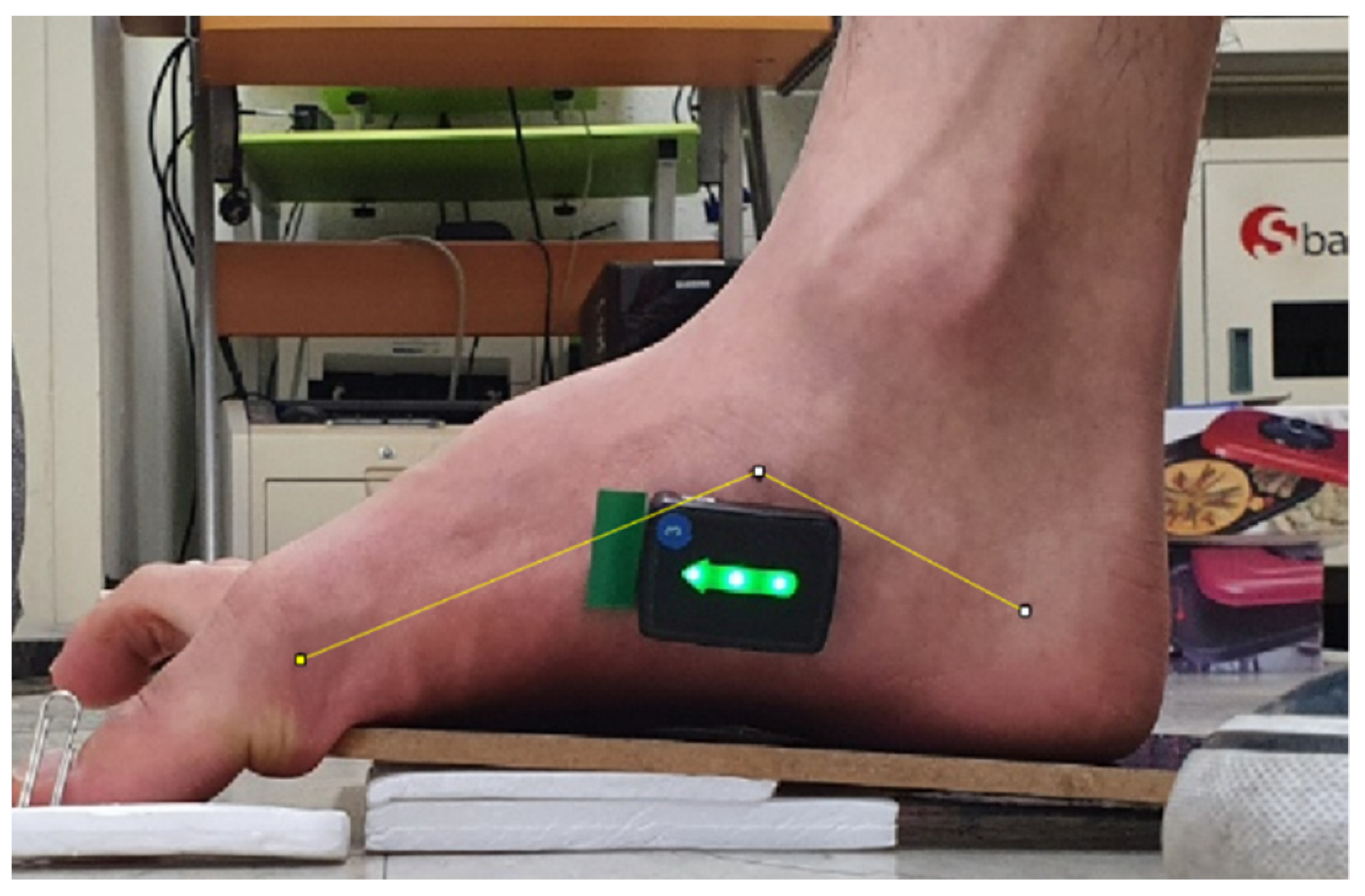
2.2.2. Measurement of the Medial Longitudinal Arch
2.3. Exercise Methods
2.3.1. Toe-Tap Exercise
2.3.2. Myofascial Release of the Peroneus Longus Muscle Using a Foam Roller
2.4. Data analysis
3. Results
3.1. The Abductor Hallucis and Peroneus Longus Activity
3.2. The Medial Longitudinal Arch Angles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, E.J.; Vanore, J.V.; Thomas, J.L.; Kravitz, S.R.; Mendelson, S.A.; Mendicino, R.W.; Silvani, S.H.; Gassen, S.C. Clinical practice guideline pediatric flatfoot panel of the American College of Foot and Ankle Surgeons. Diagnosis and Treatment of Pediatric Flatfoot. J. Foots Ankle Surg. 2004, 43, 341–373. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.E.; Link, C.L.; Felson, D.T.; Crincoli, M.G.; Keysor, J.J.; McKinlay, J.B. Prevalence of foot and ankle conditions in a multiethnic community sample of older adults. Am. J. Epidemiol. 2004, 159, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Lou, S.Z.; Huang, C.Y.; Su, F.C. Effects of foot orthoses on gait patterns of flat feet patients. Clin. Biomech. 2010, 25, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.R.; Shibley, N.J.; Austin, W.M.; Yochum, T.R. Radiographic evaluation of weight-bearing orthotics and their effect on flexible pes planus. J. Manipulative Physiol. Ther. 1999, 22, 221–226. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Musculoskeletal System-E-Book: Foundations for Rehabilitation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Barton, C.J.; Bonanno, D.; Levinger, P.; Menz, H.B. Foot and Ankle Characteristics in Patellofemoral Pain Syndrome: A Case Control and Reliability Study. J. Orthop. Sports Phys. Ther. 2010, 40, 286–296. [Google Scholar] [CrossRef]
- Coplan, J.A. Rotational motion of the knee: A comparison of normal and pronating subjects. J. Orthop. Sports Phys. Ther. 1989, 10, 366–369. [Google Scholar] [CrossRef][Green Version]
- Pinney, S.J.; Lin, S.S. Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int. 2006, 27, 66–75. [Google Scholar] [CrossRef]
- Tome, J.; Nawoczenski, D.A.; Flemister, A.; Houck, J. Comparison of foot kinematics between subjects with posterior tibialis tendon dysfunction and healthy controls. J. Orthop. Sports Phys. Ther. 2006, 36, 635–644. [Google Scholar] [CrossRef]
- Verbruggen, L.A.; Thompson, M.M.; Durall, C.J. The effectiveness of low-dye taping in reducing pain associated with plantar fasciitis. J. Sport Rehabil. 2018, 27, 94–98. [Google Scholar] [CrossRef]
- Bertani, A.; Cappello, A.; Benedetti, M.G.; Simoncini, L.; Catani, F. Flat foot functional evaluation using pattern recognition of ground reaction data. Clin. Biomech. 1999, 14, 484–493. [Google Scholar] [CrossRef]
- Rose, G. Disorder of the Foot and Ankle, Pes planus. MH Jahss; WB Saunders: Philadelphia, PA, USA, 1991. [Google Scholar]
- Van Boerum, D.H.; Sangeorzan, B.J. Biomechanics and pathophysiology of flat foot. Foot Ankle Clin. 2003, 8, 419–430. [Google Scholar] [CrossRef]
- Hajizadeh, M.; Desmyttere, G.; Ménard, A.L.; Bleau, J.; Begon, M. Understanding the role of foot biomechanics on regional foot orthosis deformation in flatfoot individuals during walking. Gait Posture. 2022, 91, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Harradine, P.; Bevan, L. A Review of the theoretical unified approach to podiatric biomechanics in relation to foot orthoses therapy. J. Am. Podiatr. Med. Assoc. 2009, 99, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Cen, X.; Gao, L.; Yang, M.; Liang, M.; Bíró, I.; Gu, Y. Arch-support induced changes in foot-ankle coordination in young males with flatfoot during unplanned gait termination. J. Clin. Med. 2021, 10, 5539. [Google Scholar] [CrossRef]
- Gray, E.G.; Basmajian, J.V. Electromyography and cinematography of leg and foot (‘normal’ and flat) during walking. Anat. Rec. 1968, 161, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Murley, G.S.; Landorf, K.B.; Menz, H.B.; Bird, A.R. Effect of foot posture, foot orthoses and footwear on lower limb muscle activity during walking and running: A systematic review. Gait Posture. 2009, 29, 172–187. [Google Scholar] [CrossRef]
- Jung, D.Y.; Kim, M.H.; Koh, E.K.; Kwon, O.Y.; Cynn, H.S.; Lee, W.H. A comparison in the muscle activity of the abductor hallucis and the medial longitudinal arch angle during toe curl and short foot exercises. Phys. Ther. Sport. 2011, 12, 30–35. [Google Scholar] [CrossRef]
- Mann, R.; Inman, V.T. Phasic Activity of intrinsic muscles of the foot. J. Bone Joint Surg. Am. 1964, 46, 469–481. [Google Scholar] [CrossRef]
- Wong, Y.S. Influence of the abductor hallucis muscle on the medial arch of the foot: A kinematic and anatomical cadaver study. Foot Ankle Int. 2007, 28, 617–620. [Google Scholar] [CrossRef]
- Lee, J.H.; Cynn, H.S.; Yoon, T.L.; Choi, S.A.; Kang, T.W. Differences in the angle of the medial longitudinal arch and muscle activity of the abductor hallucis and tibialis anterior during sitting short-foot exercises between subjects with pes planus and subjects with neutral foot. J. Back Musculoskelet. Rehabil. 2016, 29, 809–815. [Google Scholar] [CrossRef]
- Kang, M.H.; Cha, S.M.; Oh, J.S. The effect of toe-tap exercise on abductor hallucis activity and medial longitudinal arch angle in individuals with pes planus. Isokinet. Exer. Sci. 2020, 28, 415–422. [Google Scholar] [CrossRef]
- Wiewelhove, T.; Döweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A meta-analysis of the effects of foam rolling on performance and recovery. Front. Physiol. 2019, 10, 376. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Koh, E.K.; Jung, D.Y. The effect of arch support taping on plantar pressure and navicular drop height in subjects with excessive pronated foot during 6 weeks. J. Korean Soc. Phys. Med. 2011, 6, 483–490. [Google Scholar]
- Power, V.; Clifford, A.M. The effects of rearfoot position on lower limb kinematics during bilateral squatting in asymptomatic individuals with a pronated foot type. J. Hum. Kinet. 2012, 31, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.S. Kinematic analysis of ankle stiffness in subjects with and without flat foot. Foot (Edinb) 2016, 26, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Sawilowsky, S.S. New effect size rules of thumb. J. Mod. Appl. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Lee, J.H.; Cynn, H.S.; Yoon, T.L.; Ko, C.H.; Choi, W.J.; Choi, S.A.; Choi, B.S. The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. J. Electromyogr. Kinesiol. 2015, 25, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Cynn, H.; Shin, A.; Kim, B. Combined effects of gastrocnemius stretch and tibialis anterior resistance exercise in subjects with limited ankle dorsiflexion. Phys. Ther. Rehabil. Sci. 2021, 10, 10–15. [Google Scholar] [CrossRef]
- Lim, J.H.; Park, C.B.; Kim, B.G. The effects of vibration foam roller applied to hamstring on the quadriceps electromyography activity and hamstring flexibility. J. Exer. Rehabil. 2019, 15, 560–565. [Google Scholar] [CrossRef]
- Yamauchi, J.; Koyama, K. Relation between the ankle joint angle and the maximum isometric force of the toe flexor muscles. J. Biomech. 2019, 85, 1–5. [Google Scholar] [CrossRef]
- Ridge, S.T.; Myrer, J.W.; Olsen, M.T.; Jurgensmeier, K.; Johnson, A.W. Reliability of doming and toe flexion testing to quantify foot muscle strength. J. Foot Ankle Res. 2017, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.G.; Travell, J.; Simons, L. Myofascial Pain and Dysfunction: The Trigger Point Manual; Upper half of body; Williams & Wilkins: London, UK, 1999; Volume 1, pp. 21–22. [Google Scholar]
- Lee, C.; Lee, S. A literature review of the effects of self-myofascial release with a foam roller on human fascial system and cardiovascular function. Exerc. Sci. 2020, 29, 329–338. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean | ± | SD a |
|---|---|---|---|
| Age (yrs) | 23.18 | ± | 2.07 |
| Height (cm) | 170.18 | ± | 9.20 |
| Weight (kg) | 67.06 | ± | 20.32 |
| Navicular drop test (cm) | 1.20 | ± | 0.28 |
| Gender | 10 males | 6 females |
| Variables | Toe-Tap Exercise Only a | Myofascial Release of the Peroneus Longus before Toe-Tap Exercise a | Differences a | Effect Size | p |
|---|---|---|---|---|---|
| Abductor hallucis (%MVIC) | 50.75 ± 21.42 | 64.74 ± 25.95 | 13.98 ± 10.77 | 0.65 | <0.001 * |
| Peroneus longus (%MVIC) | 19.27 ± 10.76 | 12.77 ± 9.24 | 6.5 ± 5.35 | 0.60 | <0.001 * |
| Medial longitudinal arch (°) | 133.30 ± 5.56 | 130.25 ± 6.02 | 3.04 ± 2.03 | 0.55 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Lee, J. Effect of Peroneus Longus Muscle Release on Abductor Hallucis Muscle Activity and Medial Longitudinal Arch before Toe-Tap Exercise in Participants with Flexible Pes Planus. Healthcare 2022, 10, 44. https://doi.org/10.3390/healthcare10010044
Choi Y, Lee J. Effect of Peroneus Longus Muscle Release on Abductor Hallucis Muscle Activity and Medial Longitudinal Arch before Toe-Tap Exercise in Participants with Flexible Pes Planus. Healthcare. 2022; 10(1):44. https://doi.org/10.3390/healthcare10010044
Chicago/Turabian StyleChoi, Youngkyu, and Jihyun Lee. 2022. "Effect of Peroneus Longus Muscle Release on Abductor Hallucis Muscle Activity and Medial Longitudinal Arch before Toe-Tap Exercise in Participants with Flexible Pes Planus" Healthcare 10, no. 1: 44. https://doi.org/10.3390/healthcare10010044
APA StyleChoi, Y., & Lee, J. (2022). Effect of Peroneus Longus Muscle Release on Abductor Hallucis Muscle Activity and Medial Longitudinal Arch before Toe-Tap Exercise in Participants with Flexible Pes Planus. Healthcare, 10(1), 44. https://doi.org/10.3390/healthcare10010044