
Impact of a Digital Intervention for Literacy in Depression among Portuguese University Students: A Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context and Ethical Considerations
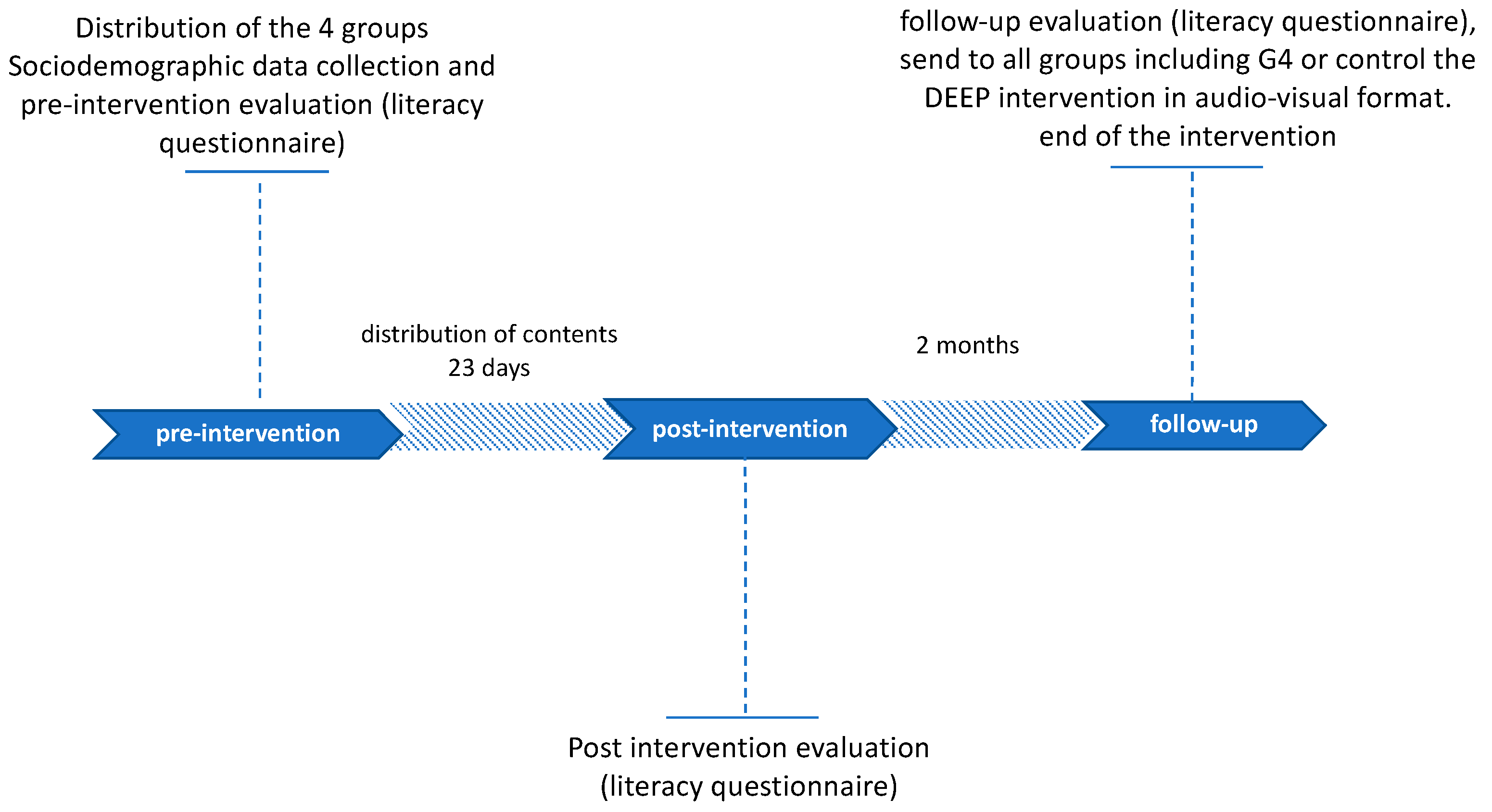
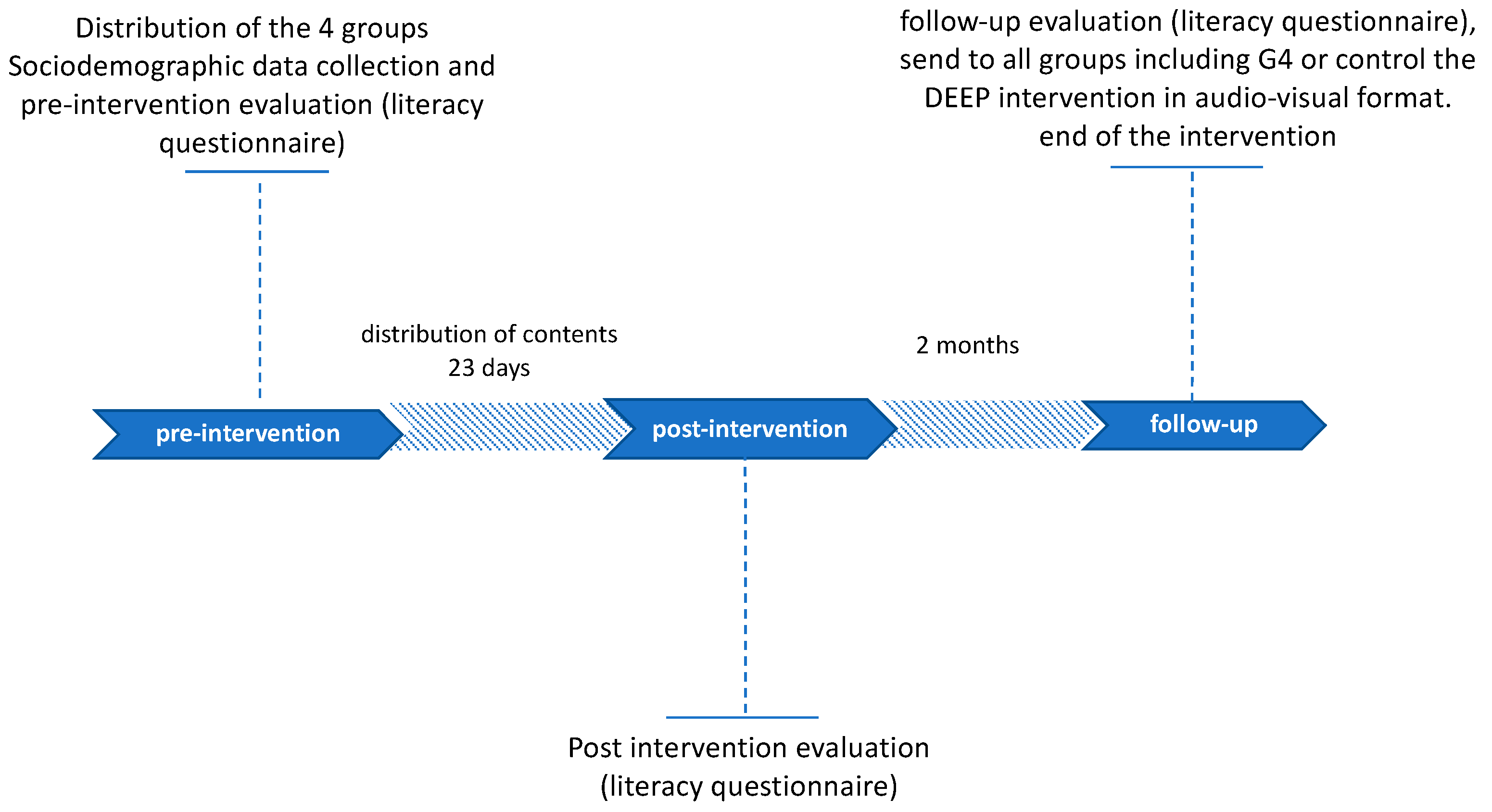
2.2. Study Design and Sample
2.3. Recruitment of Participants
2.4. Instruments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Mon | Tue | Wed | Thu | Fri |
|---|---|---|---|---|
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 |
| Day 6 | Day 7 | Day 8 | Day 9 | Day 10 |
| Day 11 | Day 12 | Day 13 | Day 14 | Day 15 |
| Day 16 | Day 17 | Day 18 | Day 19 | Day 20 |
| Day 21 | Day 22 | Day 23 | Day24 | Day 25 |
| Day 26 | Day 27 | Day 28 | Day 29 | Day 30 |
| Day 31 | Day 32 | Day 33 | Day 34 | Day 35 |
| Day 36 | Day 37 | Day 38 | Day 39 | Day 40 |
| Content Distribution Schedule | ||||
|---|---|---|---|---|
| Day | Hour | Content Group 1 | Content Group 2 | Content Group 3 |
| Day 1 | 16:00 | Teaser/PE-Video 1 | Teaser/PE-Video 1 | Article 1 |
| Day 2 | 18:00 | FS Video 1 | FS text 1 | |
| Day 5 | 19:00 | PE Video 2 | PE text 2 | |
| Day 7 | 17:00 | FS Video 2 | FS text 2 | |
| Day 9 | 16:00 | PE Video 3 | PE text 3 | |
| Day10 | 18:00 | FS Video 3 | FS text 3 | |
| Day 11 | 19:00 | PE Video 4 | PE text 4 | |
| Day 13 | 18:00 | FS Video 4 | FS text 4 | Article 2 |
| Day 14 | 19:00 | PE Video 5 | PE tex5 | |
| Day 17 | 16:00 | FS Video 5 | FS text 5 | |
| Day 20 | 19:00 | PE Video 6 | PE text 6 | |
| Day 21 | 17:00 | FS Video 6 | FS text 6 | |
| Day 23 | 16:00 | FS Video 7 | FS text 7 | |
| Day 24 | 18:00 | PE Video 7 | PE text 7 | Article 3 |
| Day 27 | 17:00 | FS Video 8 | FS text 8 | |
| Day 28 | 19:00 | PE Video 8 | PE text 8 | |
| Day 30 | 16:00 | FS Video 9 | FS text 9 | |
| Day 31 | 19:00 | PE Video 9 | PE text 9 | |
| Day 34 | 17:00 | FS Video 10 | FS text 10 | |
| Day 35 | 18:00 | FS Video 11 | FS text 11 | |
| Day 37 | 16:00 | FS Video 12 | FS text 12 | Article 4 |
| Day 38 | 19:00 | PE Video 10 | PE text 10 | |
| Day 40 | 17:00 | FS Video 13 | FS text 13 | |
References
- Carbonell, X.; Chamarro, A.; Oberst, U.; Rodrigo, B.; Prades, M. Problematic Use of the Internet and Smartphones in University Students: 2006–2017. Int. J. Environ. Res. Public Health 2018, 15, 475. [Google Scholar] [CrossRef] [Green Version]
- Horgan, Á.; Sweeney, J. Young Students’ Use of the Internet for Mental Health Information and Support. J. Psychiatr. Ment. Health Nurs. 2010, 17, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Burns, J.M.; Davenport, T.A.; Durkin, L.A.; Luscombe, G.M.; Hickie, I.B. The Internet as a Setting for Mental Health Service Utilisation by Young People. Med. J. Aust. 2010, 192 (Suppl. 11), S22–S26. [Google Scholar] [CrossRef]
- Chen, W.; Zheng, Q.; Liang, C.; Xie, Y.; Gu, D. Factors Influencing College Students’ Mental Health Promotion: The Mediating Effect of Online Mental Health Information Seeking. Int. J. Environ. Res. Public Health 2020, 17, 4783. [Google Scholar] [CrossRef]
- Christensen, H.; Griffiths, K. The Internet and Mental Health Literacy. Aust. N. Z. J. Psychiatry 2016, 34, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Mathews, S.C.; McShea, M.J.; Hanley, C.L.; Ravitz, A.; Labrique, A.B.; Cohen, A.B. Digital Health: A Path to Validation. NPJ Digit. Med. 2019, 2, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cova Solar, F.; Alvial, S.W.; Aro, D.M.; Bonifetti, D.A.; Hernández, M.M.; Rodríguez, C.C. Problemas de Salud Mental En Estudiantes de La Universidad de Concepción. Ter. Psicológica 2007, 25, 105–112. [Google Scholar] [CrossRef]
- Oliveira, C.; Varela, A.; Esteves, J.; Henriques, C.; Ribeiro, A. Programas De Prevenção Para a Ansiedade E Depressão: Avaliação Da Percepção Dos Estudantes Universitários. Programas Prevenção Para A Ansiedade E Depress 2016, 111, 96–111. [Google Scholar]
- Frazier, P.; Meredith, L.; Greer, C.; Paulsen, J.A.; Howard, K.; Dietz, L.R.; Qin, K. Randomized Controlled Trial Evaluating the Effectiveness of a Web-Based Stress Management Program among Community College Students. Anxiety Stress Coping 2014, 28, 576–586. [Google Scholar] [CrossRef]
- Hoare, E.; Collins, S.; Marx, W.; Callaly, E.; Moxham-Smith, R.; Cuijpers, P.; Holte, A.; Nierenberg, A.A.; Reavley, N.; Christensen, H.; et al. Universal Depression Prevention: An Umbrella Review of Meta-Analyses. J. Psychiatr. Res. 2021, 144, 483–493. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Oon-Arom, A.; Karawekpanyawong, N.; Lohanan, T.; Leesawat, T.; Wongpakaran, T. Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students. Healthc 2021, 9, 1399. [Google Scholar] [CrossRef] [PubMed]
- WHO. Depression. WHO, 2017. Available online: http://www.who.int/mental_health/management/depression/en/ (accessed on 16 June 2020).
- Zhou, L.; Parmanto, B. Development and Validation of a Comprehensive Well-Being Scale for People in the University Environment (Pitt Wellness Scale) Using a Crowdsourcing Approach: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e15075. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, C.; Chambers, D.; Coyle, D. Young People’s Online Help-Seeking and Mental Health Difficulties: Systematic Narrative Review. J. Med. Internet Res. 2019, 21, e13873. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of Web-Based Depression Literacy and Cognitive–Behavioural Therapy Interventions on Stigmatising Attitudes to Depression. Br. J. Psychiatry 2004, 185, 342–349. [Google Scholar] [CrossRef] [Green Version]
- Warchoł, T. Przegląd Badań Edukacyjnych Educational Studies Review Tomasz Warchoł A Sense of the Role and Value of Non-Formal Education in the Opinion of Students Participating in Interactive Workshops. Przegląd Badań Eduk. Educ. Stud. Rev. 2018, 2, 71–84. [Google Scholar] [CrossRef]
- Beck, A.; Rush, A.; Shaw, B.; Emery, G. Cognitive Therapy of Depression. Aust. N. Z. J. Psychiatry 1979, 36, 272–275. [Google Scholar] [CrossRef]
- Garrido, S.; Millington, C.; Cheers, D.; Boydell, K.; Schubert, E.; Meade, T.; Nguyen, Q.V. What Works and What Doesn’t Work? A Systematic Review of Digital Mental Health Interventions for Depression and Anxiety in Young People. Front. Psychiatry 2019, 10, 759. [Google Scholar] [CrossRef] [PubMed]
- Frank, E.; Pong, J.; Asher, Y.; Soares, C.N. Smart Phone Technologies and Ecological Momentary Data: Is This the Way Forward on Depression Management and Research? Curr. Opin. Psychiatry 2018, 31, 3–6. [Google Scholar] [CrossRef]
- Peng, Z.; Hu, Q.; Dang, J. Multi-Kernel SVM Based Depression Recognition Using Social Media Data. Int. J. Mach. Learn. Cybern. 2019, 10, 43–57. [Google Scholar] [CrossRef]
- Wei, Y.; McGrath, P.J.; Hayden, J.; Kutcher, S. Mental Health Literacy Measures Evaluating Knowledge, Attitudes and Help-Seeking: A Scoping Review. BMC Psychiatry 2015, 15, 291. [Google Scholar] [CrossRef] [Green Version]
- Giosan, C.; Mogoaşe, C.; Cobeanu, O.; Szentágotai Tătar, A.; Mureşan, V.; Boian, R. Using a Smartphone App to Reduce Cognitive Vulnerability and Mild Depressive Symptoms: Study Protocol of an Exploratory Randomized Controlled Trial. Trials 2016, 17, 609. [Google Scholar] [CrossRef] [Green Version]
- Mohr, D.C.; Tomasino, K.N.; Lattie, E.G.; Palac, H.L.; Kwasny, M.J.; Weingardt, K.; Karr, C.J.; Kaiser, S.M.; Rossom, R.C.; Bardsley, L.R.; et al. IntelliCare: An Eclectic, Skills-Based App Suite for the Treatment of Depression and Anxiety. J. Med. Internet Res. 2017, 19, e10. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.M.P.; Almeida, H.S.; Figueiredo-Braga, M. Mobile Solutions in Depression: Enhancing Communication with Patients Using an SMS-Based Intervention. Procedia Comput. Sci. 2018, 138, 89–96. [Google Scholar] [CrossRef]
- Kerst, A.; Zielasek, J.; Gaebel, W. Smartphone Applications for Depression: A Systematic Literature Review and a Survey of Health Care Professionals’ Attitudes towards Their Use in Clinical Practice. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 270, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Durán, L.; Almeida, A.M.; Figueiredo-Braga, M. Digital Audiovisual Contents for Literacy in Depression: A Pilot Study with University Students. Procedia Comput. Sci. 2021, 181, 239–246. [Google Scholar] [CrossRef]
- Sin, J.; Gillard, S.; Spain, D.; Cornelius, V.; Chen, T.; Henderson, C. Effectiveness of Psychoeducational Interventions for Family Carers of People with Psychosis: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2017, 56, 13–24. [Google Scholar] [CrossRef]
- Khan, I.; Melro, A.; Oliveira, L.; Amaro, A.C. Internet of Things Prototyping for Cultural Heritage Dissemination. J. Digit. Media Interact. 2020, 3, 20–35. [Google Scholar]
- Grigsby, T.J.; Unger, J.B.; Molina, G.B.; Baron, M. Evaluation of an Audio-Visual Novela to Improve Beliefs, Attitudes and Knowledge toward Dementia: A Mixed-Methods Approach. Clin. Gerontol. 2017, 40, 130–138. [Google Scholar] [CrossRef]
- Uddin, S.; Al Mamun, A.; Iqbal, M.A.; Nasrullah, M. Internet Addiction Disorder and Its Pathogenicity to Psychological Distress and Depression among University Students: A Cross-Sectional Pilot Study in Bangladesh. Psychology 2016, 7, 1126–1137. [Google Scholar] [CrossRef] [Green Version]
- Chu, J.T.; Wang, M.P.; Shen, C.; Viswanath, K.; Lam, T.H.; Chan, S.S.C. How, When and Why People Seek Health Information Online: Qualitative Study in Hong Kong. Interact. J. Med. Res. 2017, 6, e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, L.T.; Figueiredo, V.A. Redes Sociais: Oportunidade de Buscar Evidências Nas Informações Compartilhadas Pelos Alunos. Rev. Inf. Educ. 2020, 1, 1–8. [Google Scholar]
- Thornicroft, G.; Mehta, N.; Clement, S.; Evans-Lacko, S.; Doherty, M.; Rose, D.; Koschorke, M.; Shidhaye, R.; O’Reilly, C.; Henderson, C. Evidence for Effective Interventions to Reduce Mental-Health-Related Stigma and Discrimination. Lancet 2016, 387, 1123–1132. [Google Scholar] [CrossRef]
- Michie, S.; Yardley, L.; West, R.; Patrick, K.; Greaves, F. Developing and Evaluating Digital Interventions to Promote Behavior Change in Health and Health Care: Recommendations Resulting from an International Workshop. Journal of Medical Internet Research. J. Med. Internet Res. 2017, 19, e232. [Google Scholar] [CrossRef]
- Hollis, C.; Sampson, S.; Simons, L.; Davies, E.B.; Churchill, R.; Betton, V.; Butler, D.; Chapman, K.; Easton, K.; Gronlund, T.A.; et al. Identifying Research Priorities for Digital Technology in Mental Health Care: Results of the James Lind Alliance Priority Setting Partnership. Lancet Psychiatry 2018, 5, 845–854. [Google Scholar] [CrossRef]
- Alkhaldi, G.; Hamilton, F.L.; Lau, R.; Webster, R.; Michie, S.; Murray, E. The Effectiveness of Prompts to Promote Engagement with Digital Interventions: A Systematic Review. J. Med. Internet Res. 2016, 18, e6. [Google Scholar] [CrossRef] [Green Version]
- Duran, L.Q.; Almeida, A.M.P.; Figueiredo-Braga, M. Digital Audiovisual Narratives as Depression Literacy Promoters: Development of Psychoeducational Intervention DEEP. In Proceedings of the 15th Iberian Conference on Information Systems and Technologies (CISTI), Sevilla, Spain, 24–27 June 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Patel, S.; Akhtar, A.; Malins, S.; Wright, N.; Rowley, E.; Young, E.; Sampson, S.; Morriss, R. The Acceptability and Usability of Digital Health Interventions for Adults with Depression, Anxiety, and Somatoform Disorders: Qualitative Systematic Review and Meta-Synthesis. J. Med. Internet Res. 2020, 22, e16228. [Google Scholar] [CrossRef]
- Hart, S.R.; Kastelic, E.A.; Wilcox, H.C.; Beaudry, M.B.; Musci, R.J.; Heley, K.M.; Ruble, A.E.; Swartz, K.L. Achieving Depression Literacy: The Adolescent Depression Knowledge Questionnaire (ADKQ). Sch. Ment. Health 2014, 6, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiker, D.A.; Hammer, J.H. Mental Health Literacy as Theory: Current Challenges and Future Directions. J. Ment. Health 2019, 28, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Farrer, L.; Gulliver, A.; Chan, J.K.Y.; Batterham, P.J.; Reynolds, J.; Calear, A.; Tait, R.; Bennett, K.; Griffiths, K.M. Technology-Based Interventions for Mental Health in Tertiary Students: Systematic Review. J. Med. Internet Res. 2013, 15, e101. [Google Scholar] [CrossRef] [Green Version]
- Bona, R.J. Audiovisual Narratives Aimed at Children’s Audience in the Early 1990s: Transmedia Intertextuality Practices in Cartoons. Estud. em Comun. 2018, 1, 215–229. [Google Scholar] [CrossRef] [Green Version]
- Dowling, D.O.; Miller, K.J. Immersive Audio Storytelling: Podcasting and Serial Documentary in the Digital Publishing Industry. J. Radio Audio Media 2019, 26, 167–184. [Google Scholar] [CrossRef]
- Naslund, J.A.; Bondre, A.; Torous, J.; Aschbrenner, K.A. Social Media and Mental Health: Benefits, Risks, and Opportunities for Research and Practice. J. Technol. Behav. Sci. 2020, 5, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Glick, G.; Druss, B.; Pina, J.; Lally, C.; Conde, M. Use of Mobile Technology in a Community Mental Health Setting. J. Telemed. Telecare 2015, 22, 430–435. [Google Scholar] [CrossRef]
- Kutcher, S.; Bagnell, A.; Wei, Y. Mental Health Literacy in Secondary Schools: A Canadian Approach. Child Adolesc. Psychiatr. Clin. 2015, 24, 233–244. [Google Scholar] [CrossRef]
- Ito-Jaeger, S.; Vallejos, E.P.; Curran, T.; Spors, V.; Long, Y.; Liguori, A.; Warwick, M.; Wilson, M.; Crawford, P. Digital Video Interventions and Mental Health Literacy among Young People: A Scoping Review. J. Ment. Health 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hickie AM, I.B.; Davenport, T.A.; Luscombe, G.M.; Rong, Y.; Hickie, M.L.; Bell, M.I. The Assessment of Depression Awareness and Help-Seeking Behaviour: Experiences with the International Depression Literacy Survey. BMC Psychiatry 2007, 7, 48. [Google Scholar] [CrossRef] [Green Version]
- Janoušková, M.; Tušková, E.; Weissová, A.; Trančík, P.; Pasz, J.; Evans-Lacko, S.; Winkler, P. Can Video Interventions Be Used to Effectively Destigmatize Mental Illness among Young People? A Systematic Review. Eur. Psychiatry 2017, 41, 1–9. [Google Scholar] [CrossRef]
- Seedaket, S.; Turnbull, N.; Phajan, T.; Wanchai, A. Improving Mental Health Literacy in Adolescents: Systematic Review of Supporting Intervention Studies. Trop. Med. Int. Health 2020, 25, 1055–1064. [Google Scholar] [CrossRef]
| n = 71 | Gender | Marital Status | Place of Residence during the Period of University Classes | ||||
|---|---|---|---|---|---|---|---|
| Age Range | Male | Female | Single | Married | Partnership | Student Residence | At Home with Their Family |
| 20 and 38 years old | 24 | 47 | 60 | 9 | 2 | 51 | 20 |
| Study Group | Pre-Intervention (n = 71) | Post-Intervention (n = 56) | Follow-Up (n = 36) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Section 1 | Section 2 | Section 1 | Section 2 | Section 1 | Section 2 | |||||||
| Mean | p Value | Mean | p Value | Mean | p Value | Mean | p Value | Mean | p Value | Mean | p Value | |
| G1 | 20.85 | 0.056 | 7.55 | 0.35 | 22.19 | 0.019 * | 8.88 | 0.015 * | 20.53 | 0.095 | 8.90 | 0.092 |
| G2 | 20.82 | 0.107 | 6.71 | 0.451 | 21.36 | 0.175 | 7.14 | 0.118 | 20.11 | 0.264 | 7.00 | 0.242 |
| G3 | 21.81 | 0.054 | 7.41 | 0.262 | 19.33 | 0.045 | 7.33 | 0.092 | 18.40 | 0.043 | 5.50 | 0.468 |
| G4 | 20.41 | 0.118 | 7.71 | 0.094 | 20.42 | 0.091 | 7.50 | 0.059 | 20.80 | 0.191 | 7.60 | 0.445 |
| Teste | G1 | |
|---|---|---|
| Section 1 | Section 2 | |
| Kruskal–Wallis H | 12.367 | 7.126 |
| p value | 0.028 * | 0.02 * |
| Group G1 | Group G1 | Sheffeé Test | LSD test | ||||
|---|---|---|---|---|---|---|---|
| Section 1 | Section 2 | ||||||
| Phase (I) | Phase (J) | Mean Difference (I–J) | Std. Error | Sig. | Mean Difference (I–J) | Std. Error | Sig. |
| Pre-intervention | Post-intervention | −9.506250 | 3.872342 | 0.060 | −10.275000 * | 4.140478 | 0.017 |
| Follow-up | −17.450000 | 4.471395 | 0.001 | −10.700000 * | 4.781013 | 0.030 | |
| Post-intervention | Pre-intervention | 9.506250 | 3.872342 | 0.060 | 10.275000 * | 4.140478 | 0.017 |
| Follow-up | −7.943750 | 4.653976 | 0.244 | −0.425000 | 4.976236 | 0.932 | |
| Follow-up | Pre-intervention | 17.450000 * | 4.471395 | 0.001 | 10.700000 * | 4.781013 | 0.030 |
| Post-intervention | 7.943750 | 4.653976 | 0.244 | 0.425000 | 4.976236 | 0.932 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durán, L.D.; Almeida, A.M.; Lopes, A.C.; Figueiredo-Braga, M. Impact of a Digital Intervention for Literacy in Depression among Portuguese University Students: A Randomized Controlled Trial. Healthcare 2022, 10, 165. https://doi.org/10.3390/healthcare10010165
Durán LD, Almeida AM, Lopes AC, Figueiredo-Braga M. Impact of a Digital Intervention for Literacy in Depression among Portuguese University Students: A Randomized Controlled Trial. Healthcare. 2022; 10(1):165. https://doi.org/10.3390/healthcare10010165
Chicago/Turabian StyleDurán, Lersi D., Ana Margarida Almeida, Ana Cristina Lopes, and Margarida Figueiredo-Braga. 2022. "Impact of a Digital Intervention for Literacy in Depression among Portuguese University Students: A Randomized Controlled Trial" Healthcare 10, no. 1: 165. https://doi.org/10.3390/healthcare10010165
APA StyleDurán, L. D., Almeida, A. M., Lopes, A. C., & Figueiredo-Braga, M. (2022). Impact of a Digital Intervention for Literacy in Depression among Portuguese University Students: A Randomized Controlled Trial. Healthcare, 10(1), 165. https://doi.org/10.3390/healthcare10010165