
Is Happiness Linked to Subjective Life Expectancy? A Study of Chilean Senior Citizens




Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Shapley–Owen–Shorrocks Decomposition
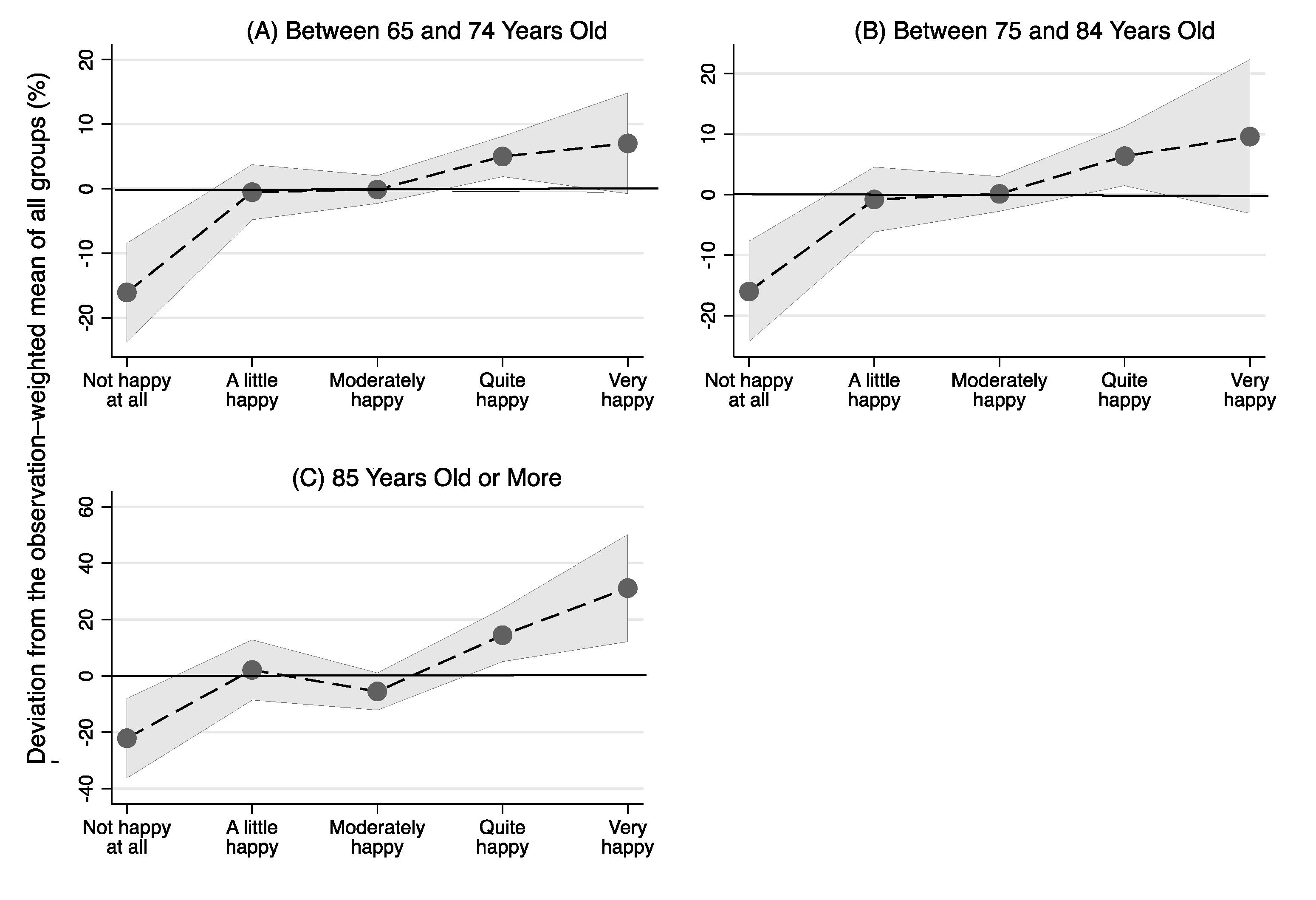
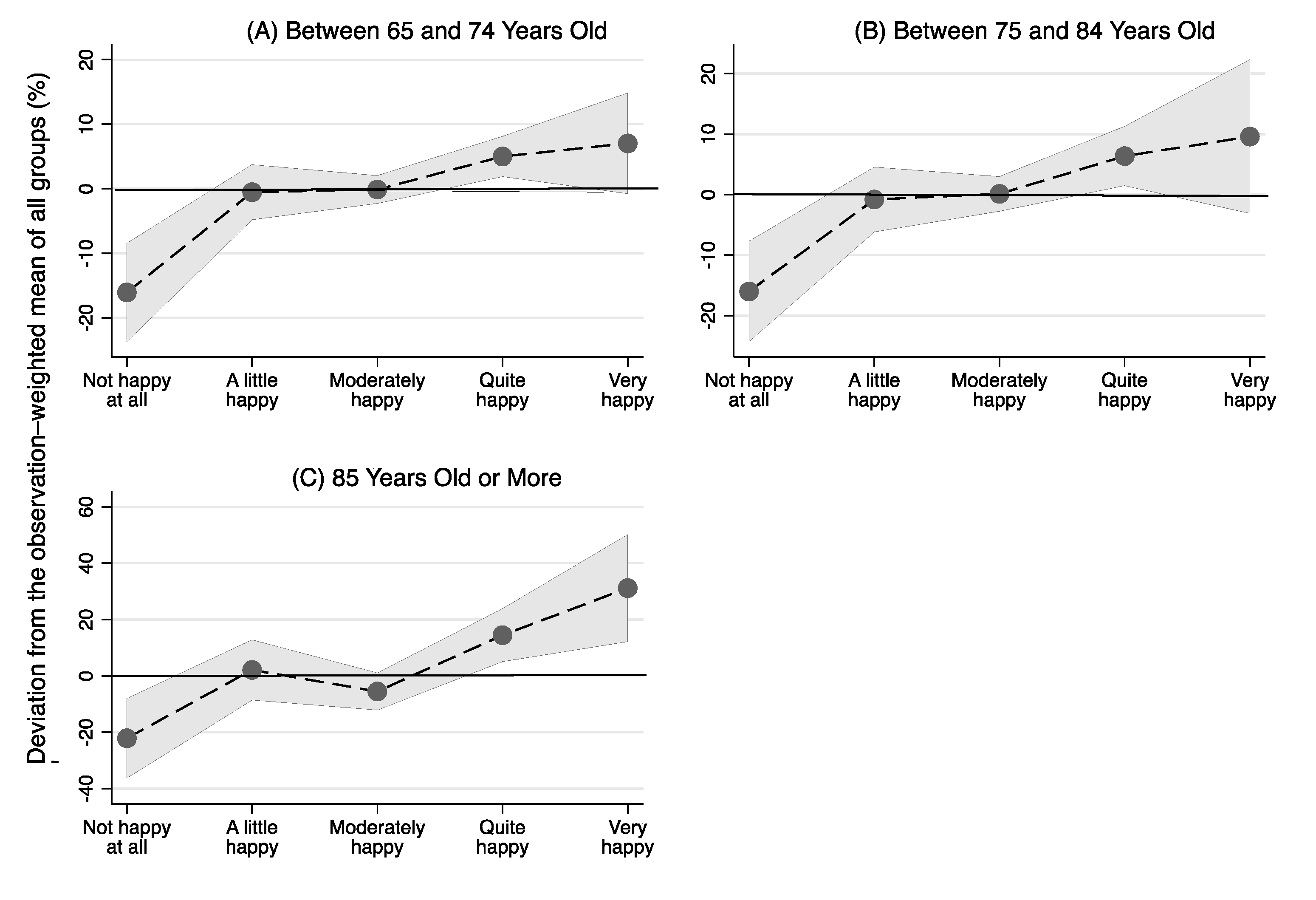
3.2. Contrasts of Marginal Linear Predictions of the Equality of the Means
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Calculating the Shapley–Owen–Shorrocks Decomposition
References
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association Between Income and Life Expectancy in the United States, 2001–2014. JAMA 2016, 315, 1750. [Google Scholar] [CrossRef] [PubMed]
- Oeppen, J. DEMOGRAPHY: Enhanced: Broken Limits to Life Expectancy. Science 2002, 296, 1029–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaupel, J.W. Biodemography of Human Ageing. Nature 2010, 464, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future Life Expectancy in 35 Industrialised Countries: Projections with a Bayesian Model Ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Word Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- John, F.; Helliwell, J.F.; Huang, H.; Wang, S.; Shiplett, H. International Migration and World Happiness. In World Happiness Report, Chapter 2; Halliwell, J., Layard, R., Sachs, J., Eds.; Sustainable Development Solutions Network: New York, NY, USA, 2018. [Google Scholar]
- Rojas, M. Latin American Happiness has Social Foundations. In World Happiness Report, Chapter 6; Halliwell, J., Layard, R., Sachs, J., Eds.; Sustainable Development Solutions Network: NewYork, NY, USA, 2018. [Google Scholar]
- O’Dea, C.; Sturrock, D. Subjective Expectations of Survival and Economic Behavior; IFS Working Papers W18/14; Institute for Fiscal Studies: London, UK, 2018. [Google Scholar] [CrossRef]
- Griffin, B.; Loh, V.; Hesketh, B. A Mental Model of Factors Associated with Subjective Life Expectancy. Soc. Sci. Med. 2013, 82, 79–86. [Google Scholar] [CrossRef]
- Falba, T.A.; Busch, S.H. Survival Expectations of the Obese: Is Excess Mortality Reflected in Perceptions? Obes. Res. 2005, 13, 754–761. [Google Scholar] [CrossRef] [Green Version]
- Hesketh, B.; Griffin, B.; Loh, V. A Future-Oriented Retirement Transition Adjustment Framework. J. Vocat. Behav. 2011, 79, 303–314. [Google Scholar] [CrossRef]
- Post, T.; Hanewald, K. Longevity Risk, Subjective Survival Expectations, and Individual Saving Behavior. J. Econ. Behav. Organ. 2013, 86, 200–220. [Google Scholar] [CrossRef]
- Salm, M. Subjective Mortality Expectations and Consumption and Saving Behaviours among the Elderly. Can. J. Econ. Rev. Can. D’écon. 2010, 43, 1040–1057. [Google Scholar] [CrossRef]
- Griffin, B.; Hesketh, B.; Loh, V. The Influence of Subjective Life Expectancy on Retirement Transition and Planning: A Longitudinal Study. J. Vocat. Behav. 2012, 81, 129–137. [Google Scholar] [CrossRef]
- Van Solinge, H.; Henkens, K. Living Longer, Working Longer? The Impact of Subjective Life Expectancy on Retirement Intentions and Behaviour. Eur. J. Public Health 2010, 20, 47–51. [Google Scholar] [CrossRef]
- Wright, W.F.; Bower, G.H. Mood Effects on Subjective Probability Assessment. Organ. Behav. Hum. Decis. Process. 1992, 52, 276–291. [Google Scholar] [CrossRef]
- Wu, S.; Stevens, R.; Thorp, S. Cohort and Target Age Effects on Subjective Survival Probabilities: Implications for Models of the Retirement Phase. J. Econ. Dyn. Control 2015, 55, 39–56. [Google Scholar] [CrossRef]
- Mykletun, A.; Bjerkeset, O.; Øverland, S.; Prince, M.; Dewey, M.; Stewart, R. Levels of Anxiety and Depression as Predictors of Mortality: The HUNT Study. Br. J. Psychiatry 2009, 195, 118–125. [Google Scholar] [CrossRef]
- Lima, M.G.; Belon, A.P.; Barros, M.B. Happy Life Expectancy among Older Adults: Differences by Sex and Functional Limitations. Rev. Saúde Pública 2016, 50. [Google Scholar] [CrossRef] [Green Version]
- Kageyama, J. Happiness and Sex Difference in Life Expectancy. J. Happiness Stud. 2012, 13, 947–967. [Google Scholar] [CrossRef]
- Van Doorn, C. A Qualitative Approach to Studying Health Optimism, Realism, and Pessimism. Res. Aging 1999, 21, 440–457. [Google Scholar] [CrossRef]
- Bowen, C.E.; Skirbekk, V. Old Age Expectations Are Related to How Long People Want to Live. Ageing Soc. 2017, 37, 1898–1923. [Google Scholar] [CrossRef] [Green Version]
- Busseri, M.A. How Dispositional Optimists and Pessimists Evaluate Their Past, Present and Anticipated Future Life Satisfaction: A Lifespan Approach. Eur. J. Personal. 2013, 27, 185–199. [Google Scholar] [CrossRef]
- Holt-Lundstad, J.; Simth, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-Analytic Review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Evans, G.F.; Soliman, E.Z. Happier Countries, Longer Lives: An Ecological Study on the Relationship between Subjective Sense of Well-Being and Life Expectancy. Glob. Health Promot. 2019, 26, 36–40. [Google Scholar] [CrossRef]
- Sargent-Cox, K.A.; Anstey, K.J.; Luszcz, M.A. Patterns of Longitudinal Change in Older Adults’ Self-Rated Health: The Effect of the Point of Reference. Health Psychol. 2010, 29, 143–152. [Google Scholar] [CrossRef]
- Moreno, X.; Albala, C.; Lera, L.; Sánchez, H.; Fuentes-García, A.; Dangour, A.D. The Role of Gender in the Association between Self-Rated Health and Mortality among Older Adults in Santiago, Chile: A Cohort Study. PLoS ONE 2017, 12, e0181317. [Google Scholar] [CrossRef] [Green Version]
- Ross, C.E.; Mirowsky, J. Family Relationships, Social Support and Subjective Life Expectancy. J. Health Soc. Behav. 2002, 43, 469. [Google Scholar] [CrossRef] [PubMed]
- Aroca, P.; Gonzalez, P.A.; Valdebenito, R. The Heterogeneous Level of Life Quality across Chilean Regions. Habitat Int. 2017, 68, 84–98. [Google Scholar] [CrossRef]
- Ludwig, A.; Zimper, A. A Parsimonious Model of Subjective Life Expectancy. Theory Decis. 2013, 75, 519–541. [Google Scholar] [CrossRef] [Green Version]
- Bissonnette, L.; Hurd, M.D.; Michaud, P. Individual Survival Curves Comparing Subjective and Observed Mortality Risks. Health Econ. 2017, 26, e285–e303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y. Dynamic Implications of Subjective Expectations: Evidence from Adult Smokers. Am. Econ. J. Appl. Econ. 2014, 6, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Ross, C.E.; Mirowsky, J. Neighborhood Socioeconomic Status and Health: Context or Composition? City Community 2008, 7, 163–179. [Google Scholar] [CrossRef]
- Gonza, G.; Burger, A. Subjective Well-Being During the 2008 Economic Crisis: Identification of Mediating and Moderating Factors. J. Happiness Stud. 2017, 18, 1763–1797. [Google Scholar] [CrossRef]
- Schimmel, J. Development as Happiness: The Subjective Perception of Happiness and UNDP’s Analysis of Poverty, Wealth and Development. J. Happiness Stud. 2009, 10, 93–111. [Google Scholar] [CrossRef]
- Encuesta de Protección Social-Subsecretaría de Previsión Social. Available online: https://www.previsionsocial.gob.cl/sps/biblioteca/encuesta-de-proteccion-social/ (accessed on 31 May 2021).
- Behrman, J.R.; Mitchell, O.S.; Soo, C.K.; Bravo, D. How Financial Literacy Affects Household Wealth Accumulation. Am. Econ. Rev. 2012, 102, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Bucciol, A.; Manfrè, M.; Gimenez, G. The 2008 Chilean Pension Reform: Household Financial Decisions and Gender Differences. J. Econ. Policy Reform 2020, 1–18. [Google Scholar] [CrossRef]
- Subsecretaría de Previsión Social del Ministerio de Trabajo y Previsión Social del Gobierno de Chile and Centro de Encuestas y Estudios Longitudinales de la Pontificia Universidad Católica de Chile. In Diseño Muestral y Factores de Expansión VI Ronda EPS; Ministerio de Trabajo y Previsión Social: Santiago de Chile, Chile, 2016.
- Baye, F.M. Growth, Redistribution and Poverty Changes in Cameroon: A Shapley Decomposition Analysis. J. Afr. Econ. 2006, 15, 543–570. [Google Scholar] [CrossRef]
- Shorrocks, A.F. Decomposition Procedures for Distributional Analysis: A Unified Framework Based on the Shapley Value. J. Econ. Inequal. 2013, 11, 99–126. [Google Scholar] [CrossRef] [Green Version]
- Gimenez, G.; Martín-Oro, Á.; Sanaú, J. The Effect of Districts’ Social Development on Student Performance. Stud. Educ. Eval. 2018, 58. [Google Scholar] [CrossRef]
- Gimenez, G.; Barrado, B.; Arias, R. El Papel Del Profesorado y El Entorno de Aprendizaje En El Rendimiento de Los Estudiantes Costarricenses: Un Análisis a Partir de PISA. Rev. Complut. de Educ. 2019, 30, 1127–1145. [Google Scholar] [CrossRef]
- Barcenilla, S.; Gimenez, G.; López-Pueyo, C. Differences in Total Factor Productivity Growth in the European Union: The Role of Human Capital by Income Level. Prague Econ. Pap. 2019, 28, 70–85. [Google Scholar] [CrossRef] [Green Version]
- Barrado, B.; Gimenez, G.; Sanaú, J. The Use of Decomposition Methods to Understand the Economic Growth Gap between Latin America and East Asia. Sustainability 2021, 13, 6674. [Google Scholar] [CrossRef]
- Israeli, O. A Shapley-Based Decomposition of the R-Square of a Linear Regression. J. Econ. Inequal. 2007, 5, 199–212. [Google Scholar] [CrossRef]
- Nathans, L.L.; Oswald, F.L.; Nimon, K. Interpreting Multiple Linear Regression: A Guidebook of Variable Importance. Pract. Assess. Res. Eval. 2012, 17, 1–19. [Google Scholar]
- Huettner, F.; Sunder, M. Rego: Stata Module for Decomposing Goodness of Fit According to Owen and Shapley Values. In United Kingdom Stata Users’ Group Meetings 2012; Stata Users Group: London, UK, 2012. [Google Scholar]
- Skaff, M.A. Sense of control and health: A dynamic duo in the aging process. In Handbook of Health Psychology and Aging; Press, T.G., Aldwin, C.M., Park, C.L., Spiro, A., Eds.; The Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Scott-Sheldon, L.A.J.; Carey, M.P.; Vanable, P.A.; Senn, T.E. Subjective Life Expectancy and Health Behaviors among STD Clinic Patients. Am. J. Health Behav. 2010, 34, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathieu, S.I. Happiness and Humor Group Promotes Life Satisfaction for Senior Center Participants. Act. Adapt. Aging 2008, 32, 134–148. [Google Scholar] [CrossRef]
- Sumngern, C.; Azeredo, Z.; Subgranon, R.; Sungvorawongphana, N.; Matos, E. Happiness among the Elderly in Communities: A Study in Senior Clubs of Chonburi Province, Thailand. Jpn. J. Nurs. Sci. 2010, 7, 47–54. [Google Scholar] [CrossRef]
- Chen, W. How Education Enhances Happiness: Comparison of Mediating Factors in Four East Asian Countries. Soc. Indic. Res. 2012, 106, 117–131. [Google Scholar] [CrossRef]
- Shapley, L. A value for n-person games. In Contributions to the Theory of Games, Volume 2; Press, P.U., Kuhn, H.W., Tucker, A.W., Eds.; Princeton University Press: Princeton, NJ, USA, 1953. [Google Scholar]
- Owen, G. Values of games with priori unions. In Essays in Mathematical Economics and Game Theory; Heim, R., Moeschlin, O., Eds.; Springer: New York, NY, USA, 1977. [Google Scholar]
- Huettner, F.; Sunder, M. Axiomatic Arguments for Decomposing Goodness of Fit According to Shapley and Owen Values. Electron. J. Stat. 2012, 6, 1239–1250. [Google Scholar] [CrossRef]

{kind=link}
| Between 65 and 74 Years Old | Between 75 and 84 Years Old | 85 Years Old and Older | ||||
|---|---|---|---|---|---|---|
| Contributing Factors | Value | Percentage | Value | Percentage | Value | Percentage |
| Happiness | 0.064 | 36% | 0.071 | 30% | 0.133 | 37% |
| (0.030, 0.104) | (0.032, 0.118) | (0.064, 0.232) | ||||
| Gender and age | 0.007 | 4% | 0.008 | 3% | 0.018 | 5% |
| (0.001, 0.021) | (0.002, 0.027) | (0.003, 0.065) | ||||
| Educational level | 0.003 | 2% | 0.007 | 3% | 0.010 | 3% |
| (0.001, 0.011) | (0.001, 0.027) | (0.002, 0.039) | ||||
| Civil status | 0.007 | 4% | 0.011 | 5% | 0.038 | 11% |
| (0.002, 0.020) | (0.003, 0.029) | (0.007, 0.091) | ||||
| Body mass index | 0.003 | 2% | 0.012 | 5% | 0.034 | 9% |
| (0.001, 0.011) | (0.002, 0.034) | (0.008, 0.092) | ||||
| Diseases suffered * | 0.053 | 30% | 0.078 | 33% | 0.064 | 18% |
| (0.026, 0.087) | (0.039, 0.131) | (0.025, 0.131) | ||||
| Subjective health condition | 0.042 | 23% | 0.048 | 20% | 0.061 | 17% |
| (0.021, 0.071) | (0.023, 0.087) | (0.023, 0.118) | ||||
| Total R-Squared | 0.179 | 100% | 0.235 | 100% | 0.358 | 100% |
| Observations | 700 | 421 | 177 | |||
| Proportion of R-Squared explained by happiness (in dark grey) |  |  |  | |||
| Between 65 and 74 Years Old | Between 75 and 84 Years Old | 85 Years Old or More | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | F | P > F | Contrast | F | P > F | Contrast | F | P > F | Contrast |
| Not happy at all | 17.15 | 0.000 | −16.063 | 14.44 | 0.000 | −16.003 | 9.60 | 0.002 | −22.099 |
| (−3.879) | (4.212) | (7.132) | |||||||
| A little happy | 0.06 | 0.811 | −0.520 | 0.09 | 0.769 | −0.799 | 0.15 | 0.695 | 2.127 |
| (2.176) | (2.715) | (5.404) | |||||||
| Moderately happy | 0.01 | 0.916 | −0.115 | 0.01 | 0.932 | 0.124 | 2.74 | 0.100 | −5.501 |
| (1.089) | (1.447) | (3.321) | |||||||
| Quite happy | 9.91 | 0.002 | 5.003 | 6.53 | 0.011 | 6.372 | 9.34 | 0.003 | 14.466 |
| (1.589) | (2.494) | (4.734) | |||||||
| Very happy | 3.15 | 0.077 | 7.036 | 2.20 | 0.139 | 9.590 | 10.57 | 0.001 | 31.159 |
| (3.966) | (6.461) | (9.583) | |||||||
| Joint | 5.84 | 0.000 | 4.56 | 0.001 | 7.50 | 0.000 | |||
| Observations | 700 | 421 | 177 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gimenez, G.; Gil-Lacruz, A.I.; Gil-Lacruz, M. Is Happiness Linked to Subjective Life Expectancy? A Study of Chilean Senior Citizens. Mathematics 2021, 9, 2050. https://doi.org/10.3390/math9172050
Gimenez G, Gil-Lacruz AI, Gil-Lacruz M. Is Happiness Linked to Subjective Life Expectancy? A Study of Chilean Senior Citizens. Mathematics. 2021; 9(17):2050. https://doi.org/10.3390/math9172050
Chicago/Turabian StyleGimenez, Gregorio, Ana Isabel Gil-Lacruz, and Marta Gil-Lacruz. 2021. "Is Happiness Linked to Subjective Life Expectancy? A Study of Chilean Senior Citizens" Mathematics 9, no. 17: 2050. https://doi.org/10.3390/math9172050
APA StyleGimenez, G., Gil-Lacruz, A. I., & Gil-Lacruz, M. (2021). Is Happiness Linked to Subjective Life Expectancy? A Study of Chilean Senior Citizens. Mathematics, 9(17), 2050. https://doi.org/10.3390/math9172050