
A Fuzzy Recommendation System for the Automatic Personalization of Physical Rehabilitation Exercises in Stroke Patients

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Related Work
- Firstly, a recommendation module which can automatically modify rehabilitation plans previously devised by physicians is proposed. Conditional knowledge is defined to select the most suitable exercise for the patients, depending on their current condition and how they progress in terms of rehabilitation;
- Secondly, the gap between the rehabilitation system in which the recommendation module is integrated and the patients/physicians is reduced, thanks to the use of fuzzy logic to both represent and infer knowledge. This approach facilitates the understanding of the artificial system, and particularly, how the recommendation module operates. We think that this contribution is especially relevant when it comes to explain how artificial systems make decisions. Furthermore, the feedback provided to the patients can be used to guide the rehabilitation process in a dynamic way;
- Thirdly, the proposal sets the foundations for providing physicians with a tool that reduces the time spent supervising stroke patients. Currently, there is a lack of specialized personnel to supervise, face-to-face and on a regular basis, patients affected by neurological diseases that require physical rehabilitation. Our work may eventually help improve the quality and effectiveness of remote rehabilitation by addressing the automatic adaptation of rehabilitation routines.
3. Material and Methods
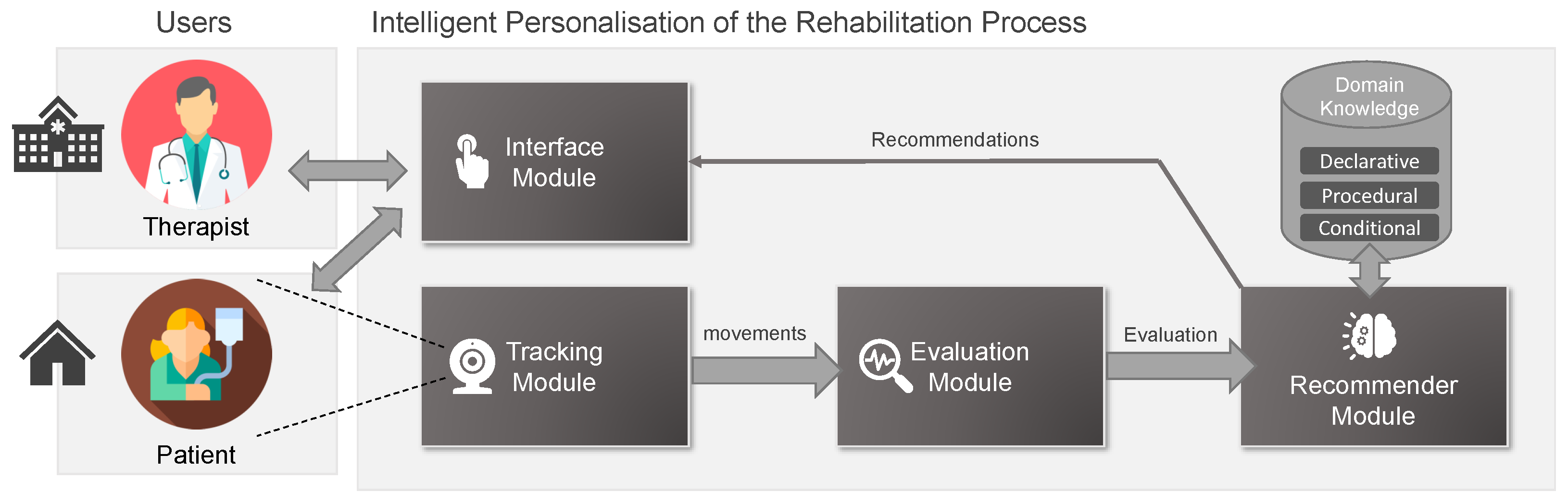
3.1. Remote Rehabilitation System Overview
- Declarative knowledge. It refers to the facts or static knowledge. In this regard, it defines the set of existent body joints that can be exercised during the rehabilitation, which will be recognized by the system (i.e., https://docs.microsoft.com/bs-latn-ba/azure/kinect-dk/body-joints, accessed on 11 June 2021), the constraints associated with them (i.e., ), the associated variables to monitor the rehabilitation exercise of patients (i.e., );
- Procedural knowledge. This knowledge defines the rehabilitation exercises and the game dynamics associated with them (i.e., . In each , the patient works out a concrete joint (i.e., ) with a different degree of complexity, trying to rehabilitate a body member with low mobility. The procedural knowledge also includes the knowledge required to check how well the patient performs an exercise and to determine how the patient is progressing in the rehabilitation process;
- Conditional knowledge. This knowledge will be used to recommend the next exercise to be performed in the patients’ rehabilitation plan (i.e., ), based on their degree of injury and their progress towards recovery. Fundamentally, it makes use of a set of fuzzy (if–then) rules (i.e., ) to achieve the aforementioned goal. This will be deepened in the following section.
- is a description of the exercise ;
- is the set associated with the joints involved in the rehabilitation exercise , i.e., ;
- is the setup of the exercise which is defined as a 4-tuple . indicates the degree of success by achieving a step in the rehabilitation exercise (); are the repetitions required to perform the exercise (); t is the time needed to finish the exercise (); and c is the degree of complexity of the exercise ();
- represents the virtual objects positioned in a playable scene in the 3D space. Examples of this objects may be rings, spheres and hoops, among others;
- refers to the trajectories associated with the movements that a patient will make when performing the exergame . is defined as a set of virtual points that establish the movements the patient must perform;
- is a set of rules that contains the game mechanics of the exercise , which are based on the interaction between and in the 3D space to achieve an objective. Formally, , where each particular rule of the game is used to define the function where:
- -
- establishes the joints that interact with the game rule;
- -
- establishes the virtual nodes that interact with the game rule;
- -
- O is a set of objectives defined to satisfy the game rules ();
- -
- is a set of game mechanics to be triggered when a joint involved interacts with a virtual node meeting a certain objective . Example of game mechanics may be visual feedback provided to the patient to correct a bad movement.
- is a set of constraints that are associated with joints that the patient should not ideally move to compensate for the lack of mobility or strength in the exercise (i.e., );
- is a set of key performance indicators that are used to monitor the patient’s evolution according to the performance of the exercise .
3.2. Proposed Recommendation Module
3.2.1. Fundamental Ideas
3.2.2. Recommender Module Definition
- difference_number_steps () is the difference between the number of steps that the patients and the therapists performed to carry out the last rehabilitation exercise (i.e., the patient fails to pass through all the virtual points that establish the exercise trajectory);
- accumulated_deviation () is the cumulative spatial deviation between the patient’s exercise and that gold standard or the therapist’s exercise (i.e., this calculation is based on the distance accumulated when traversing the trajectory associated to the last exercise );
- difference_time () is the temporal difference regarding the execution of the last exercise between the patient and the therapist.
- . It chooses an exercise from E whose lesion and joint are similar to the last exercise . This function takes into account an exercise that has not yet been performed, since the system internally stores information about the patients and the exercises they performed, i.e., their level of success regarding the exercise, their points, as well as the time spent by the patient to complete it. To do this, this function takes two parameters: (1) a label indicating the complexity of the exercise to be searched for (, more complexity; , same complexity; , less complexity) based on the (2) last performed exercise ();
- . It recommends the repetition of the last exercise performed by the patient based on modifying its configuration. This function takes as parameters (number of repetitions) and t (time needed to finish the exercise) from .
| Algorithm 1: Behavior of proposed exergame function. |
 |
| : | IF is {} |
| AND is {} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {M} |
| AND is {M} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {} |
| AND is {,H} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {M} |
| AND is {M} | |
| AND is {M} | |
| AND is {} | |
| THEN AND is {} |
3.2.3. Functions Of The Proposed Recommender System
- The next rehabilitation exercise that the patient should perform;
- How to alter the value of the patient’s progress level.
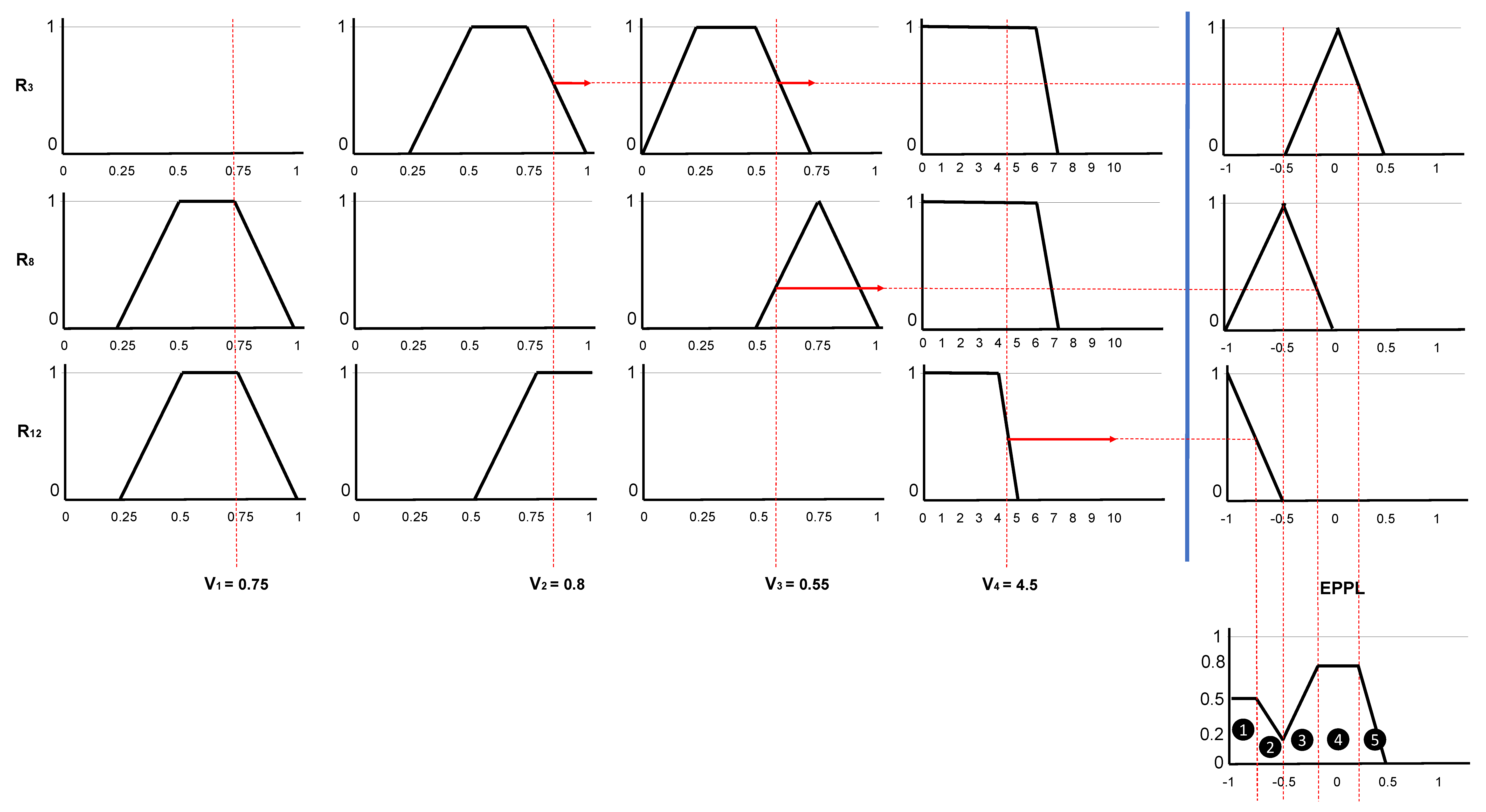
- Evaluate the antecedent for each rule to obtain a single membership value, i.e., activation degree (). We will do this as in the previous case;
- Obtain the conclusion of each rule in . To do this, we truncate the fuzzy value taken by the consequent of the rule in the variable using the minimum with the activation degree() on its membership function. The output will be a new fuzzy set defined by means of a membership function where:and it is defined aswith being the value that the variable takes in the rule ().
- Aggregate rule’s conclusions into a single fuzzy set defined by means of the function , using a fuzzy aggregation operator. The t-conorm of the maximum has been used to aggregate the truncated output functions returned by the previous step:
- Defuzzification. Since we want to obtain a crisp value that affects to the value, which we recall is confined to the range , so we need to transform the fuzzy set obtained in step 3 into a single numerical value. To do this, we used the defuzzification method of the centroid, which returns the center of the area under the fuzzy set obtained in step 3. It should be pointed out that the total area of the membership function distribution used to represent the combined control action is divided into a number of sub-areas. We denote the centroid as and it is calculated aswhere N indicates the number of sub-areas, and represent the area and the centroid of the area, respectively, of the sub-area.
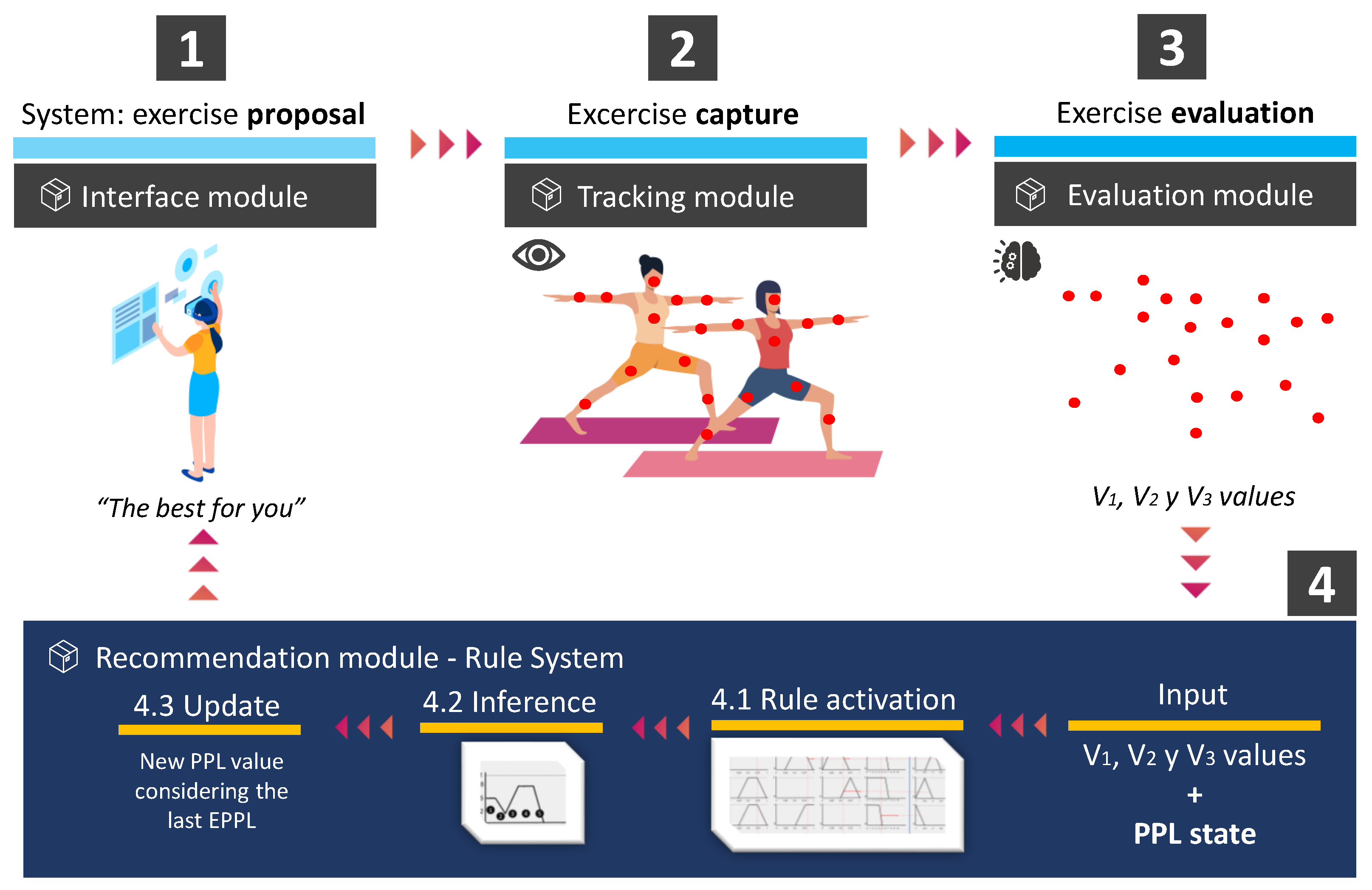
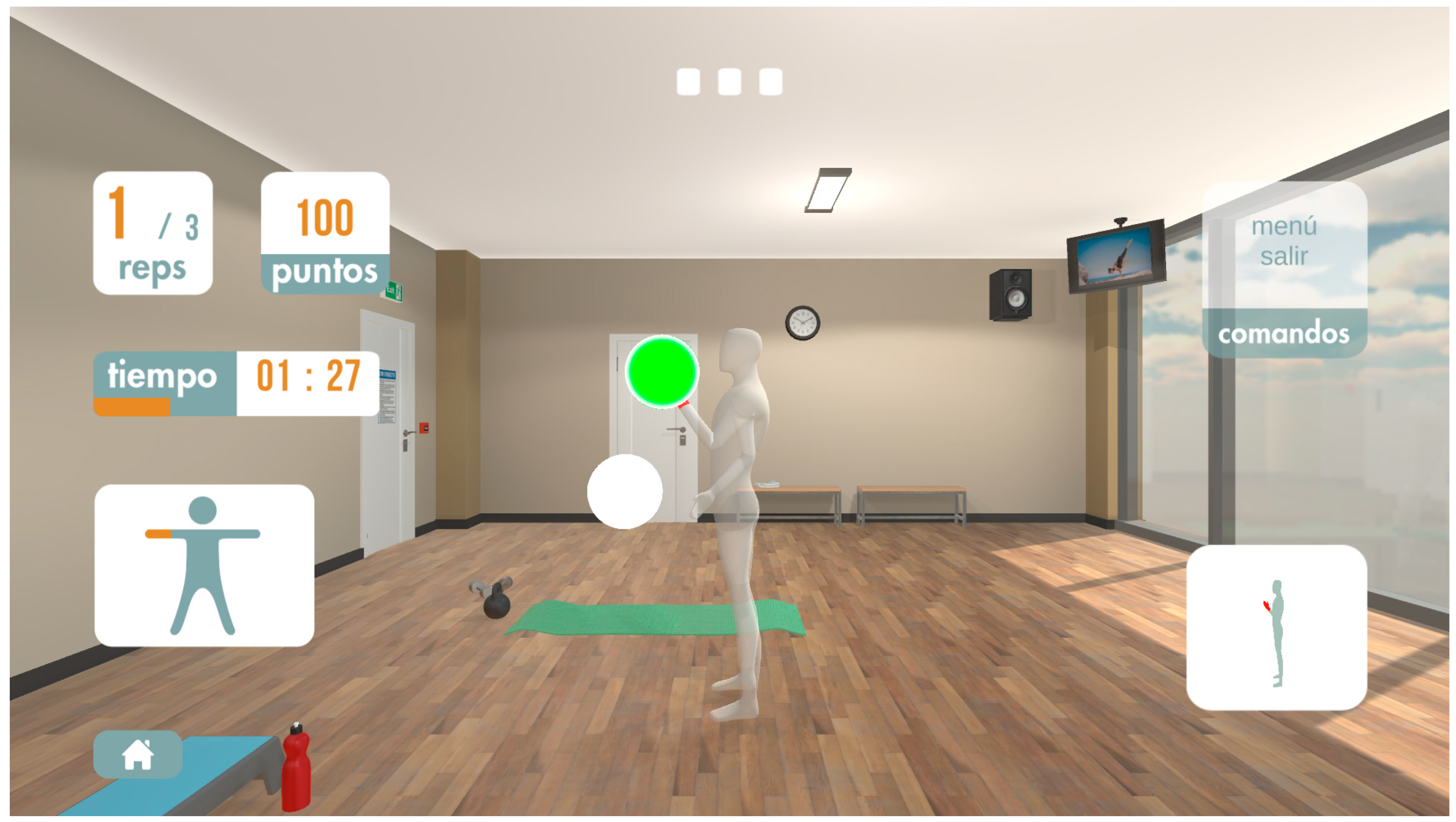
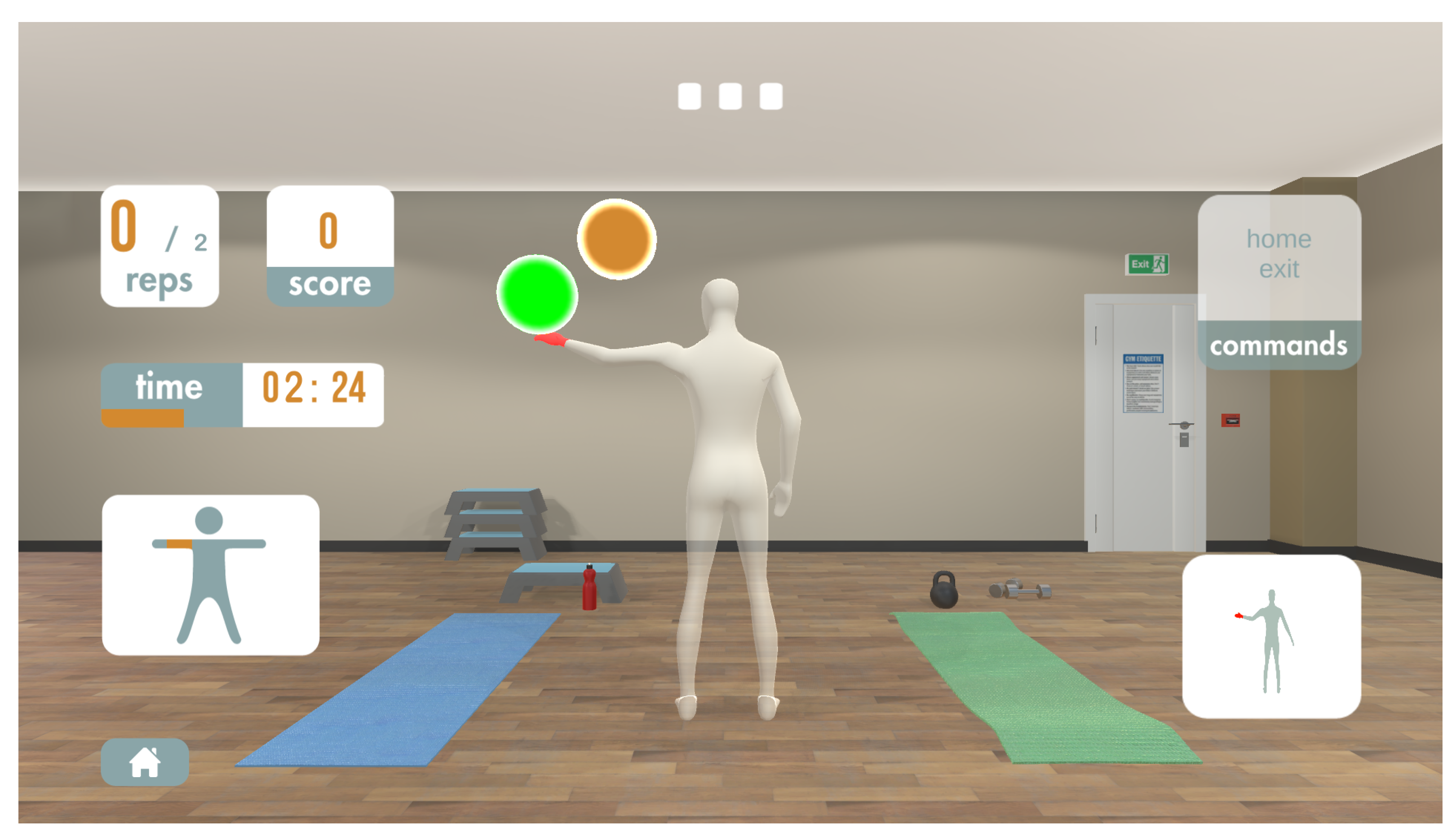
4. Proposed System In Operation
- The system proposes an exercises () to the patient through the interface module;
- The patient performs an exercise whose movements are captured by the tracking module;
- The system evaluates, through the evaluation module, the performance of the patient. Particularly, it obtains the value of the variables ();
- The system, based upon the values of the variables (, and ), triggers the rules following the next criteria:
- (a)
- It computes the activation degree of the rules belonging to the knowledge base (i.e., conditional knowledge);
- (b)
- It selects, employing the first inference system, the rule whose activation degree is greater among the set of rules. Its consequent contains the exercise to be recommended, which may be a new one or a modification of the last exercise performed;
- (c)
- It modifies, employing the second inference system, the patient’s progress level (). It should be noted that this modification takes into account the last exercise performed.
| : | IF is {} |
| AND is {} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {} |
| AND is {H} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {} |
| AND is {} | |
| AND is {} | |
| THEN AND is {} |
| : | IF is {L} |
| AND is {L} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {} |
| AND is {} | |
| AND is {} | |
| THEN AND is {} | |
| : | IF is {L} |
| AND is {M} | |
| AND is {} | |
| THEN AND is {} |
5. Discussion
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S. Stroke: A global response is needed. Bull. World Health Organ. 2016, 94, 634–644. [Google Scholar] [CrossRef]
- Semrau, M.; Evans-Lacko, S.; Alem, A.; Ayuso-Mateos, J.L.; Chisholm, D.; Gureje, O.; Hanlon, C.; Jordans, M.; Kigozi, F.; Lempp, H.; et al. Strengthening mental health systems in low-and middle-income countries: The Emerald programme. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mensah, G.A.; Norrving, B.; Feigin, V.L. The global burden of stroke. Neuroepidemiology 2015, 45, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-rehabilitation after stroke: An updated systematic review of the literature. J. Stroke Cerebrovasc. Dis. 2018, 27, 2306–2318. [Google Scholar] [CrossRef] [PubMed]
- Moral-Munoz, J.A.; Zhang, W.; Cobo, M.J.; Herrera-Viedma, E.; Kaber, D.B. Smartphone-based systems for physical rehabilitation applications: A systematic review. Assist. Technol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Webster, D.; Celik, O. Systematic review of Kinect applications in elderly care and stroke rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Pua, Y.; Fortin, K.; Ritchie, C.; Webster, K.E.; Denehy, L.; Bryant, A.L. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef]
- Mobini, A.; Behzadipour, S.; Saadat, F.M. Accuracy of Kinect’s skeleton tracking for upper body rehabilitation applications. Disabil. Rehabil. Assist. Technol. 2014, 9, 344–352. [Google Scholar] [CrossRef]
- Sardi, L.; Idri, A.; Fernández-Alemán, J.L. A systematic review of gamification in e-Health. J. Biomed. Inform. 2017, 71, 31–48. [Google Scholar] [CrossRef]
- Schez-Sobrino, S.; Vallejo, D.; Monekosso, D.N.; Glez-Morcillo, C.; Remagnino, P. A distributed gamified system based on automatic assessment of physical exercises to promote remote physical rehabilitation. IEEE Access 2020, 8, 91424–91434. [Google Scholar] [CrossRef]
- Vallejo, D.; Gmez-Portes, C.; Albusac, J.; Glez-Morcillo, C.; Castro-Schez, J.J. Personalized Exergames Language: A Novel Approach to the Automatic Generation of Personalized Exergames for Stroke Patients. Appl. Sci. 2020, 10, 7378. [Google Scholar] [CrossRef]
- Bhaskaran, S.; Marappan, R.; Santhi, B. Design and Analysis of a Cluster-Based Intelligent Hybrid Recommendation System for E-Learning Applications. Mathematics 2021, 9, 197. [Google Scholar] [CrossRef]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning-I. Inf. Control 1975, 8, 199–249. [Google Scholar] [CrossRef]
- González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; Torres-Carrion, P.V. Serious games for rehabilitation: Gestural interaction in personalized gamified exercises through a recommender system. J. Biomed. Inform. 2019, 97, 103266–103285. [Google Scholar] [CrossRef] [PubMed]
- Esfahlani, S.S.; Cirstea, S.; Sanaei, A.; Wilson, G. An adaptive self-organizing fuzzy logic controller in a serious game for motor impairment rehabilitation. In Proceedings of the 2017 IEEE 26th International Symposium on Industrial Electronics (ISIE), Edinburgh, UK, 19–21 June 2017; pp. 1311–1318. [Google Scholar]
- Fernandez-Cervantes, V.; Stroulia, E.; Oliva, L.E.; Gonzalez, F.; Castillo, C. Serious games: Rehabilitation fuzzy grammar for exercise and therapy compliance. In Proceedings of the 2015 IEEE Games Entertainment Media Conference (IEEE), Toronto, ON, Canada, 14–16 October 2015; pp. 1–8. [Google Scholar]
- Pirovano, M.; Mainetti, R.; Baud-Bovy, G.; Lanzi, P.L.; Borghese, N.A. Self-adaptive games for rehabilitation at home. In Proceedings of the 2012 IEEE Conference on Computational Intelligence and Games (IEEE), Granada, Spain, 11–14 September 2012; pp. 179–186. [Google Scholar]
- Pirovano, M.; Surer, E.; Mainetti, R.; Lanzi, P.L.; Borghese, N.A. Exergaming and rehabilitation: A methodology for the design of effective and safe therapeutic exergames. Entertain. Comput. 2016, 14, 55–65. [Google Scholar] [CrossRef]
- Anton, D.; Berges, I.; Bermúdez, J.; Goñi, A.; Illarramendi, A. A telerehabilitation system for the selection, evaluation and remote management of therapies. Sensors 2018, 18, 1459. [Google Scholar] [CrossRef]
- Karime, A.; Mohamad, E.; Alja’Am, J.M.; El Saddik, A.; Gueaieb, W. A fuzzy-based adaptive rehabilitation framework for home-based wrist training. IEEE Trans. Instrum. Meas. 2013, 63, 135–144. [Google Scholar] [CrossRef]
- Han, J.; Yang, S.; Xia, L.; Chen, Y. Deterministic adaptive robust control with a novel optimal gain design approach for a fuzzy 2DOF lower limb exoskeleton robot system. IEEE Trans. Fuzzy Syst. 2021. [Google Scholar] [CrossRef]
- Castro-Schez, J.J.; Castro, J.L.; Zurita, J. M Fuzzy Repertory Table: A Method for Acquiring Knowledge About Input Variables to Machine Learning Algorithm. IEEE Trans. Fuzzy Syst. 2004, 12, 123–139. [Google Scholar] [CrossRef]
- Klement, E.P.; Mesiar, R.; Pap, E. Fuzzy set theory, Cap. In Triangular Norms; Springer: Berlin/Heidelberg, Germany, 2000; pp. 249–264. [Google Scholar]
- Mandami, E.H.; Assilian, S. An experiment in linguistic synthesis with a fuzzy logic controller. Int. J. Man Mach. Stud. 1975, 7. [Google Scholar] [CrossRef]
- Gupta, M.M.; Qi, J. Theory of T-norms and fuzzy inference methods. Fuzzy Sets Syst. 1991, 40, 431–450. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sub-Area Number | Area () | Centroid of Area ( | Area * |
|---|---|---|---|
| 1 | 0.375 | −0.625 | −0.234375 |
| 2 | 0.0875 | −0.7084 | −0.061985 |
| 3 | 0.2 | −0.534 | −0.1068 |
| 4 | 0.16 | 0 | 0 |
| 5 | 0.16 | 0.234 | 0.03744 |
| ∑ Area = 0.9825 | ∑ Area * = −0.36572 |
| Sub-Area Number | Area () | Centroid of Area ( | Area * |
|---|---|---|---|
| 1 | 0.09 | −0.3 | −0.234375 |
| 2 | 0.24 | 0 | 0 |
| 3 | 0.0275 | 0.2167 | 0.005995925 |
| 4 | 0.0975 | 0.35 | 0.034125 |
| 5 | 0.16 | 0.5 | 0.08 |
| 6 | 0.16 | 0.74 | 0.1184 |
| ∑ Area = 0.775 | ∑ Area * = 0.21148425 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gmez-Portes, C.; Castro-Schez, J.J.; Albusac, J.; Monekosso, D.N.; Vallejo, D. A Fuzzy Recommendation System for the Automatic Personalization of Physical Rehabilitation Exercises in Stroke Patients. Mathematics 2021, 9, 1427. https://doi.org/10.3390/math9121427
Gmez-Portes C, Castro-Schez JJ, Albusac J, Monekosso DN, Vallejo D. A Fuzzy Recommendation System for the Automatic Personalization of Physical Rehabilitation Exercises in Stroke Patients. Mathematics. 2021; 9(12):1427. https://doi.org/10.3390/math9121427
Chicago/Turabian StyleGmez-Portes, Cristian, José Jesús Castro-Schez, Javier Albusac, Dorothy N. Monekosso, and David Vallejo. 2021. "A Fuzzy Recommendation System for the Automatic Personalization of Physical Rehabilitation Exercises in Stroke Patients" Mathematics 9, no. 12: 1427. https://doi.org/10.3390/math9121427
APA StyleGmez-Portes, C., Castro-Schez, J. J., Albusac, J., Monekosso, D. N., & Vallejo, D. (2021). A Fuzzy Recommendation System for the Automatic Personalization of Physical Rehabilitation Exercises in Stroke Patients. Mathematics, 9(12), 1427. https://doi.org/10.3390/math9121427