Abstract
Medical students face cognitive overload and disengagement due to the rigorous demands of their education. This study evaluates the impact of Medimon Learning Cards, a mnemonic-based trading card game, on engagement, satisfaction, and knowledge retention among students in a medical immunology course. These cards incorporate visual and linguistic mnemonics, coupled with strategic gameplay, to create an interactive learning experience. This study was conducted on 39 first-year medical students enrolled in an immunology course, divided into experimental Learning Card and control groups. The Learning Card group received the Medimon Learning Cards and participated in a structured play session, while both groups received identical in-class instruction. The results from the Situational Interest Survey for Multimedia revealed high engagement and satisfaction among the Learning Card group, with students expressing enthusiasm for expanding the scope of the cards to other topics. However, no significant differences were observed in knowledge retention or exam performance between the groups. These findings suggest that Medimon Learning Cards can serve as a valuable supplementary tool with which to enhance motivation and interest, though their impact on cognitive outcomes requires further investigation. These findings suggest that incorporating mnemonic-based card games such as Medimon Learning Cards can enhance learner motivation and interest, although their impact on cognitive outcomes warrants further study.
1. Introduction
Medical and health sciences students face significant challenges in their educational journeys, including cognitive overload, mental health issues, and burnout (Bhugra & Molodynski, 2024). These challenges are exacerbated by the demanding academic and clinical requirements inherent in medical education (Densen, 2011; Klatt & Klatt, 2011). To address these challenges, the use of innovative teaching methods is essential to enhance engagement and support knowledge retention (Ho et al., 2021). Some such innovative approaches involve the use of game-based learning (GBL) (Xu et al., 2023) and mnemonic-based tools (Mostafa & El Midany, 2017) designed to align with the principles of the Cognitive Theory of Multimedia Learning (CTML), which emphasizes the importance of the synergistic combination of words and images (Mayer, 2012).
Game-based learning has emerged as a promising approach in medical education, leveraging the principles of gamification and serious games to enhance motivation, engagement, and active learning (Abou Hashish et al., 2024; Khorammakan et al., 2023; Xu et al., 2023). Gamification refers to the use of game design elements in non-game contexts (Deterding et al., 2011) and is widely employed in medical education to increase engagement (Gentry et al., 2019; van Gaalen et al., 2021). Typical examples include awarding badges for timely module completion, unlocking bonus content, or posting student leaderboards on learning-management systems (Hamari et al., 2014). While gamification can boost motivation, some critics argue that surface-level rewards may not support deep learning unless they are closely tied to curricular objectives (Koivisto & Hamari, 2019). In response, educators are increasingly looking beyond gamification toward more immersive game-based strategies.
One such strategy is the use of serious games, which are full-fledged games designed for a primary purpose other than pure entertainment, typically being educational in nature (Abt, 1987). These include games in both digital and analog formats that are intentionally structured to reinforce specific learning outcomes. While digital games have received the bulk of research attention (Xu et al., 2023), analog games such as board and card games are gaining recognition for their educational potential, especially in resource-limited settings (Edwards et al., 2024). For example, others have shown that card-based games can improve conceptual understanding and retention in veterinary education (Ober, 2018), and similar evidence was reported for a board game for human pharmacology (Jones et al., 2015). These GML approaches are particularly well-suited for medical education, where students must master vast amounts of information while maintaining high levels of engagement and resilience (Gutierrez et al., 2016; Samarasekera et al., 2018).
Mnemonic-based education is a powerful approach to enhancing learning and retention of complex information, particularly in the context of STEM education (Lubin & Polloway, 2016). Mnemonics are memory aids that facilitate the encoding, storage, and retrieval of information by associating new material with previously learned knowledge or mental imagery (Bellezza, 1981). Visual mnemonics, in particular, leverage the brain’s exceptional capacity for processing and retaining visual information (Chang et al., 2022). One of the key advantages of visual mnemonics is the dual coding theory, which posits that information can be encoded and stored in two distinct systems: verbal and non-verbal (Clark & Paivio, 1991). This dual representation increases the chances of recalling information since it can be retrieved through either system. Empirical evidence supports the effectiveness of visual mnemonics in improving learning outcomes (Scruggs & Mastropieri, 1990). Mnemonics have long been used in medical education to simplify complex biomedical concepts (O’Hanlon & Laynor, 2019). They act as cognitive aids, enabling students to recall detailed information by linking it to memorable cues (Radović & Manzey, 2019). However, traditional mnemonic techniques often lack the interactivity and engagement required to sustain student interest over time (Putnam, 2015). To address this, we developed Medimon, a game similar to the Pokemon franchise, utilizing GBL and mnemonic-based characters representing cells, organ systems, and disease (Bland & Guo, 2024). These characters were designed by using visual mnemonics to represent and simplify complex biomedical ideas, making them more accessible and memorable for learners. Building on this concept, we applied Medimon’s principles to a prototype trading card game (TCG), incorporating mechanics that encourage active learning, strategic thinking, and social interaction. This approach is aimed at enhancing interactivity and engagement, creating an immersive learning experience while maintaining educational rigor.
Analog games, such as the Medimon Learning Cards, offer distinct advantages in our increasingly digital world. They facilitate tactile and interpersonal interaction, fostering collaboration and critical thinking in a way that digital tools sometimes cannot (Altschul & Deary, 2020; Kuo et al., 2018). Analog games can be more accessible in resource-limited environments, where digital devices or stable internet connections may not be available (Vita-Barrull et al., 2023). They encourage face-to-face social interaction, which can strengthen communication skills and teamwork among players. These qualities make analog games particularly valuable as educational tools that blend cognitive engagement with social learning, offering a counterbalance to the isolation sometimes associated with digital learning methods (von Steinkeller & Grosse, 2022).
The primary goal of this research was to evaluate the effectiveness of Medimon Learning Cards in improving student engagement, satisfaction, and knowledge retention within the context of immune system education. We hypothesized that the Medimon Learning Cards would enhance student engagement and satisfaction and improve long-term knowledge retention compared to traditional instructional methods alone.
2. Materials and Methods
2.1. Participants
The participants included first-year medical students enrolled at the University of Idaho WWAMI Medical Education Program. All students received the same lecture content and exam questions. After a brief recruitment briefing, students assigned themselves to study arms. The first 20 volunteers who expressed interest in trying the Medimon card game were placed in the experimental Learning Card group (n = 20), whereas the remaining students—who were either uninterested or preferring usual study methods—formed the control group (n = 19). This opt-in approach was adopted because the intervention was supplemental, and high engagement was expected only from students who actively wished to use the cards. Both groups received identical in-class instruction and examinations throughout the course.
2.2. Intervention
All students were enrolled in a 6-week infections and immunology (I&I) course during which they received instruction related to immune systems, cell types, and functions. At the beginning of the course, the Learning Card group received 51 Medimon Learning Cards (Figure 1B and Figure S1). These included cards of the following Medimon characters:
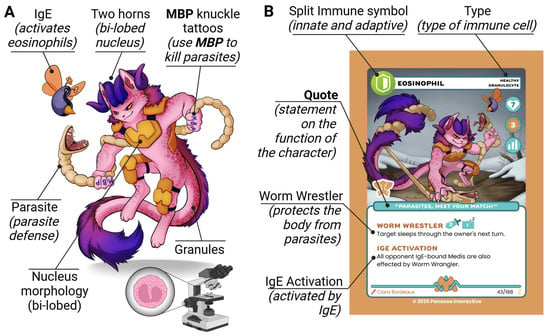
Figure 1.
Eosinophil Medimon. (A) The character design of the Eosinophil Medimon (Healthy Granulocyte family). Visual mnemonics expressing functions and characteristics of real-life eosinophils are labeled. (B) Eosinophil Medimon Learning Card. Visual and linguistic mnemonics are labeled.
- Killer Family: Natural Killer Cell, Killer T-Cell, and CAR T-Cell;
- Macrophage Family: Monocyte, Dendritic Cell, and Macrophage;
- B-Cell Family: B-Cell, Plasma Cell, and Memory B-Cell;
- Helper T Family: Helper T-Follicular, Helper T2, and Helper T1;
- Granulocyte Family: Mast Cell, Basophil, Eosinophil, and Neutrophil;
- Antibodies: IgM, IgA, IgE, and IgG.
The Learning Card group participants had three weeks to interact with the cards and were encouraged to incorporate them into their study routines. During this time, they were tasked with building their playing decks utilizing 35 of the 51 Medimon cards plus an additional 25 ATP energy cards to assemble their playing deck of 60 cards (35 character cards + 25 ATP cards). The control group did not receive the Medimon Learning Cards but had access to all other standard course materials, including the same lectures, study guides, and assessments as the Learning Card group. The Medimon and their mnemonics were presented in course lectures, which were presented to both groups, during the first three weeks of the course, and the slides were accessible to all students after the lectures (Figure 1A). This ensured that any observed differences in outcomes could be attributed to the intervention rather than discrepancies in instruction or resources.
2.3. Design
The Medimon Learning Cards were designed with elements from the original video game but featured new artwork tailored to card format. This redesign was aimed at enhancing student interest and engagement by creating visually distinct and educationally rich materials while preserving the mnemonic elements of the original game. Each card included specific features designed to align with the pedagogical objectives and the themes of the immune system. This included a cohesive visual and structural framework that integrated specific icons and linguistic mnemonics that highlight the function of the immune-related entity the Medimon represents (Figure 1).
The top of each card displayed the name of the Medimon, which corresponded to the real-world immune system component it represented. For example, the Eosinophil card featured the name prominently at the top of the card. The major type of each Medimon was indicated by a prominent immune symbol—a shield—to represent the protective nature of the immune system. This prototype focused exclusively on immune-type Medimon. Additionally, the shield featured a split design with two colors to indicate the two branches of the immune system: adaptive and innate. Each card’s minor type—whether healthy or diseased—was also identified near the top. All cards in this set represented healthy Medimon and included the following families: Granulocyte, B-cell, Killer, Helper T, and Macrophage (Figure S1).
Each Medimon card included a short, thematic quote related to its immune function. For example, the Eosinophil Medimon’s quote, “Parasites, meet your match,” reflects its role in combating parasitic infections. These quotes added a layer of personality to the cards, making the content more engaging and memorable for learners.
Each card listed one or two moves that the Medimon could perform in the game. These moves served as both gameplay mechanics and mnemonics for real-world biological functions. For example, Eosinophil’s moves included “Worm Wrestler” (representing its parasitic defense role) and “IgE Activation” (highlighting IgE’s ability to activate eosinophils).
The cards included multiple symbols to represent key gameplay mechanics. Each card featured a set of three bars indicating the stage of the Medimon: baby (one bar filled), adolescent (two bars filled), or adult (three bars filled). These stages corresponded to the developmental progression of each Medimon family. The attack strength of each move was represented by a sword icon containing a numeric value, while a pillow icon with a number indicated the number of turns the Medimon must rest before performing another move, akin to the tapping mechanism in Magic: The Gathering. Additionally, the cards displayed the artist’s name, card number, and rarity. Rarity levels were represented as H (Horses) for common, SH (Striped Horses) for uncommon, and Z (Zebras) for rare. These levels were inspired by Dr. Theodore Woodward’s adage, “When you hear hoofbeats, think horses, not zebras,” which advises clinicians to consider common conditions before rare ones. The inclusion of Striped Horses added nuance, symbolizing common diseases that present in atypical ways.
This design approach ensured that the cards were not only visually engaging but also pedagogically effective.
2.4. Game Mechanics
The mechanics of the game were inspired by the trading card game Magic: The Gathering, providing a familiar yet tailored framework for strategic play and resource management (Methods S1). The mechanics of the game were based on a structured framework to ensure clarity, balance, and replayability. Players engaged in multiplayer play, with the objective of reducing opponents’ life counts to zero, starting with a baseline of 20 life points.
Each turn consisted of three phases: the Draw Phase, Play Phase, and Attack Phase. In the Draw Phase, players drew a card from their deck and refreshed their ATP cards (energy resources) by returning them to an upright position. During the Play Phase, players could play one ATP card and as many Medimon cards as their available ATP resources allowed. The ATP costs varied by the stage of the Medimon, with Stage 1 cards requiring one ATP, Stage 2 requiring two, and Stage 3 requiring three. Medimon that had been played could not attack on the same turn unless otherwise specified.
The Attack Phase allowed players to use their in-play Medimon to attack a single opponent. Players declared their attackers, announced the attacks being used, and paid the attack ATP costs for all attacks. Attacks inflicted damage on opposing Medimon or directly on the opponent if no Medimon were used for defense. Damage was tracked using counters and persisted across turns unless a given Medimon was healed. If a Medimon’s damage equaled or exceeded its health points, it was discarded.
The game incorporated elements of resource management and strategic decision-making. ATP cards, essential for performing actions, were drawn and played carefully, as only one could be placed per turn. Players could also choose to retaliate during an opponent’s attack by using defending Medimon to absorb damage and counterattack, provided they had sufficient ATP resources with which to pay for the retaliation costs. Retaliation added depth to the gameplay by introducing a risk–reward dynamic, as players balanced protecting their life points with preserving their in-play Medimon.
To maintain strategic balance, certain high-power moves triggered a brief “Sleep” cooldown—during which the affected Medimon cannot act again until the player’s next turn—thereby preventing move repetition and encouraging diverse play. This mechanism was also utilized for in-play ATP cards during use. This required players to plan their strategies around managing sleep statuses and optimizing their Medimon’s contributions to the game.
The inclusion of multiple symbols on the cards provided players with essential gameplay information at a glance. Symbols indicated attack strength, ATP costs, health points, and sleep durations, while the visual design and thematic quotes reinforced the educational objectives. These mechanics, paired with the mnemonics embedded in the Medimon Learning Cards, created a balanced blend of education and entertainment, appealing to both medical students and gaming enthusiasts.
2.5. Play Session
At the conclusion of the first three weeks of the course, the Learning Card group participated in an extracurricular, informal, one-hour play session using the Medimon Learning Cards (Figure 2). This session provided an opportunity for hands-on engagement with the material. At the beginning of the course, students received the cards and were introduced to the game’s rules and mechanics (Methods S1). Two of the authors, V.S. (a second-year medical student) and T.B., moderated this session.

Figure 2.
Play session. Learning Card group participants split into groups of 3–4 students per table and played the Medimon Learning Card game.
2.6. Achievement Measurement
To assess knowledge and retention, we conducted a series of tests (provided in Methods S2):
- Pretest: At the beginning of the course, both groups were asked to complete a multiple-choice question (MCQ) pretest to establish baseline knowledge.
- Posttest 1: After three weeks of instruction, both groups were given the same MCQ test as a posttest to measure knowledge retention.
- Posttest 2: Eight weeks after the initial posttest, the same MCQ test was administered again to measure long-term knowledge retention.
The tests were developed using a custom GPT USMLE Step 1 Question Generator and Refiner (ChatGPT—USMLE step1 question generator and refiner, n.d.) to create questions that focused on the underlying medical concepts represented by the Learning Cards and were also important topics covered in the students’ course materials (Figure 3). This custom GPT utilizes GPT 4o and was developed and refined utilizing the NBME Item Writing Guidelines (NBME item-writing guide | NBME, n.d.) along with a set of Step 1 Sample Test Questions (Step 1 sample test questions | USMLE, n.d.). These questions were then refined by a professional immunologist. Upon completion of posttest 2, participants received a USD 20 gift card as a thank you for their time and effort.
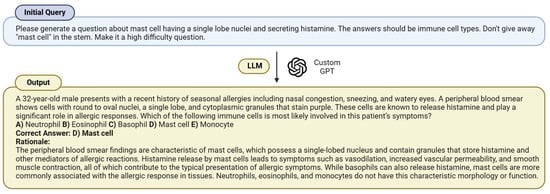
Figure 3.
Question generation. An example prompt utilized to produce the pre/posttest question that tested knowledge related to mast cells.
2.7. Data Collection
After the first three weeks of the course, on the day of completing posttest 1, students in the Learning Card group were invited to participate in a survey. All 20 students from the Learning Card group completed the Situational Interest Survey of Multimedia (SIS-M), which is designed to assess different aspects of situational interest in multimedia learning environments (Dousay, 2016; Dousay & Trujillo, 2019). This includes the measurement of triggered situational interest (initial engagement with multimedia), maintained interest, and value interest (perceived usefulness of the content). The SIS-M has recently been applied to medical education research (Bland et al., 2024), making it a suitable tool for evaluating learner engagement in this study.
The survey included questions that asked students to consent to participate and respond to the 12-item SIS-M about the Medimon Learning Cards (Table S1). The survey included items to be ranked on a Likert scale from 1 to 5 (1 = strongly disagree, 5 = strongly agree), a question asking “Would you prefer more of your medical education be supported by Medimon Learning Cards?”, and an open-ended question asking “Why do you think this is your preference.”
Student exam grades were recorded to measure baseline knowledge between the groups.
2.8. Data Analysis
We utilized Microsoft Excel, GraphPad Prism (v 9.5.1 (733)), and GPT o3 to analyze the students’ weekly course exam grades, pre/posttest scores, and SIS-M survey results. Achievement data were reported as the average scores for each group. Pre/posttest differences in achievement scores were analyzed using two-tailed Student’s t-tests and a difference-in-differences (DiD) analysis conducted utilizing a two-sample Welch t-test. A post hoc power analysis was conducted in G*Power (version 3.1.9.7). With the final sample (n = 19 vs 20) and α = 0.05 (two-tailed), this study had ≈9% power for detecting a small effect (Cohen d = 0.20) but 78% power for effects of d ≥ 0.90.
The SIS-M survey analysis considered multiple dimensions of situational interest: triggered interest (Trig), maintained interest (MT), maintained feeling (MF), and maintained value (MV). For the open-ended question in the SIS-M survey, thematic analysis was conducted using the “reasoning” LLM models ChatGPT o1 and Google Gemini 2.0 Flash Thinking Experimental (Figure 4). This involved generating initial codes and identifying themes (Alomar et al., 2025; Bland, 2025; Bland et al., 2024; Worthley et al., 2025). The prompt-engineering techniques used included Persona Prompting (J. Wang et al., 2023; White et al., 2023), Self-Criticism (Huang et al., 2022), and LLM-as-a-Judge (Gu et al., 2024). The workflow involved submitting the responses to each LLM individually. We then had both LLMs act as “judges” of each other’s outputs and asked them to output a new thematic analysis based on the original and their respective reviews of each other’s analysis. We then combined and refined these themes to address overlap and maintain relevancy. The workflow and prompts are presented in Figure 4.

Figure 4.
Thematic analysis. A workflow depicting the performance of the thematic analysis on the open-ended survey responses.
2.9. Ethical Considerations
This educational research was determined exempt by the institutional review board of the University of Idaho (24-151). To ensure the confidentiality of participants, the SIS-M survey was conducted anonymously. No identifying information was collected, allowing students to provide candid feedback without concerns about personal attribution. This approach ensured the integrity of the data while protecting the privacy of all participants. Students whose faces are visible in Figure 2 gave consent to use their photos in this study.
3. Results
3.1. Achievement
Baseline knowledge was assessed by measuring the average weekly course exam scores throughout the entire course, and the results indicated no statistically significant differences between the Learning Card group and the control group (Figure 5A). This finding confirmed that both groups had similar baseline knowledge levels regarding immunology and infections throughout the study. To evaluate the impact of the Medimon Learning Cards, knowledge retention was analyzed through a series of tests (Figure 5B,C). A pretest measured baseline knowledge of the study-specific material, revealing no statistical differences between the Learning Card and control groups (Control: 38.6 ± 17.4%; Learning Card: 43.8 ± 17.9%, p = 0.368). After three weeks, posttest 1 was conducted, with the results showing a statistically significant increase in scores in both groups (Control: +50.8%, p < 0.001; Learning Cards: +48.8%, p < 0.001) but with no significant difference between the two groups (Control: 89.5 ± 11.4%; Learning Card: 92.5 ± 8.5%, p = 0.352). A difference-in-differences (DiD) analysis further indicated that there were no significant differences in scores between the two groups (Table 1). Six weeks later, the same test was administered as posttest 2, and the results indicated no statistical differences within groups (Control: −0.5%, p = 0.848; Learning Cards: −6.0%, p = 0.078) or between group (Control: 88.9 ± 14.0%; Learning Card: 87.0 ± 10.4%, p = 0.567), a result that was also supported by a DiD analysis (Table 2). Collectively, these results suggest that the addition of Medimon Learning Cards did not lead to measurable learning gains compared to traditional study methods alone.
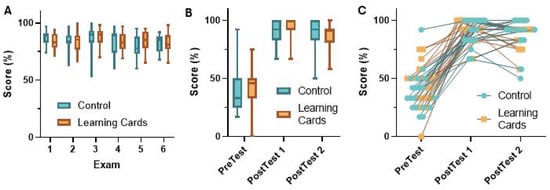
Figure 5.
Achievement analysis. (A) The average exam scores for all the exams in the course separated by group. (B,C) Average (B) and individual (C) scores on the pre/posttests separated by group. All data in (A,B) are represented as the means, with error bars representing the min/max.

Table 1.
Pre/Posttest 1 changes in score and DiD analysis.
Table 2.
Posttest 1/Posttest 2 changes in score and DiD analysis. One student in the control group and two students in the Learning Card group did not complete posttest 2, so their data was omitted from this analysis.
3.2. Engagement
The Situational Interest Survey for Multimedia (SIS-M) was used to evaluate student engagement and satisfaction with the Medimon Learning Cards among participants in the Learning Card group (n = 20). The survey assessed four key metrics: triggered situational interest, maintained situational interest, maintained situational feeling, and maintained situational value. Each metric was rated on a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating greater levels of engagement or satisfaction.
The results of the SIS-M survey demonstrated high levels of engagement across all the metrics measured (Figure 6A). The average score for triggered situational interest was 4.41 ± 0.69, suggesting that the Medimon Learning Cards effectively captured the students’ initial interest. Maintained situational interest, which evaluates sustained engagement over time, scored an average of 4.28 ± 0.82. Similarly, maintained situational feeling, reflecting emotional connection to the content, yielded an average score of 4.23 ± 0.73. Finally, maintained situational value, which assessed the perceived usefulness and relevance of the Medimon Learning Cards, yielded a mean score of 4.34 ± 0.90. These results indicate that the Medimon Learning Cards were well-received by the students, fostering both initial and sustained engagement while being perceived as valuable and emotionally resonant educational tools.
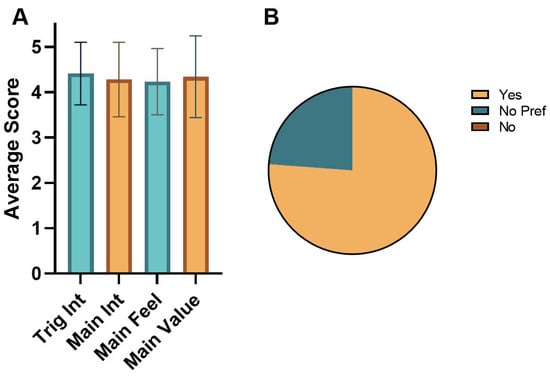
Figure 6.
SIS-M results. (A) Average score on the Likert scale (1 = strongly disagree, 5 = strongly agree) for the different types of engagement. Data is represented as the average ± standard deviation. (B) Responses to the question “Would you prefer more of your medical education be supported by Medimon Learning Cards?” Trig: Triggered, Main: Maintained, Feel: Feeling, Int: Interest.
The majority of the students in the Learning Card group expressed a strong preference for the Medimon Learning Cards and expressed enthusiasm for their expansion into other areas of the curriculum. Specifically, 75% (15/20) of the students reported that they would like to see the cards applied to additional topics, 25% (5/20) indicated they had no preference, and no students expressed opposition to expanding the use of the cards (Figure 6B).
The open-ended responses reflect a range of opinions on how the Medimon Learning Cards influenced the students’ learning experiences, retention, and overall engagement. The following themes showing both the benefits and limitations of incorporating the Medimon Learning Cards into students’ study practices emerged.
- Enhanced Memory Retention and Recall: The students found the cards helped improve their long-term memory by associating complex immunological concepts with memorable visuals and mnemonics. This visual approach aided them in both encoding and retrieving information.
- Enjoyment, Engagement, and Fun Factor: The students frequently described the cards as enjoyable, entertaining, or “fun,” aspects they felt increased their motivation and engagement with the learning material.
- Visualization and Conceptual Clarity: The visual aspects of the cards were praised for aiding in the clarification of complex immune pathways, cascades, and interactions. The students found abstract concepts easier to understand when presented visually.
- Social and Collaborative Learning: The group “battle” format of the card game facilitated social interaction and peer learning, allowing the students to review material collaboratively in an engaging way.
- Mismatch with Exam Complexity: Some students felt that the level of detail and complexity of the cards did not fully align with the demands of exam material.
- Insufficient Instruction and Guidance: A need for a clearer explanation of how to effectively use the cards, as well as guidance in this regard, was expressed.
- Potential Time Constraints/Study Habits: Some students felt that the cards, while enjoyable, might not be the most efficient use of their study time or did not align with their preferred study methods.
Overall, the majority of the participants who expressed a preference endorsed further integration of Medimon Learning Cards in their medical education. The central positives include improved retention, visual clarity, increased engagement, and social learning advantages. However, some participants remained neutral due to exam complexity mismatches, a lack of structured guidance on using the cards effectively, or personal study preferences.
4. Discussion
This study aimed to evaluate the impact of mnemonic-based Medimon Learning Cards on student engagement, satisfaction, and knowledge retention within a first-year medical immunology course. The findings provide important insights into the roles of such tools in medical education. The high levels of engagement and satisfaction observed among the students in the Learning Card group underscore the potential of Medimon Learning Cards to enhance the learning experience. This aligns with prior research showing that interactive and visually engaging tools such as serious games can significantly improve motivation and interest in educational contexts (Graafland et al., 2012; R. Wang et al., 2016). Additionally, many students expressed interest in expanding the Medimon Learning Cards to other topics, indicating their perceived value as a supplementary educational resource.
However, this study found no significant differences in knowledge retention or exam performance between the Learning Card and control groups. This suggests that while Medimon Learning Cards may excel in fostering engagement, they may not directly enhance cognitive outcomes within the constraints of this study’s design. This aligns with previous studies suggesting that engagement alone may not always translate to measurable improvements in knowledge retention (Mayer, 2005). One factor that may explain the lack of measurable cognitive differences between the groups is that the baseline curriculum may have been sufficiently effective on its own, reducing the potential added value of the Medimon Learning Cards. While this does not negate the Medimon Learning Cards’ value as a supplemental resource, it would suggest that they cannot be used to replace traditional curriculum or classroom learning.
The Medimon Learning Cards also have the potential to reach younger audiences, particularly adolescents, by leveraging the cards’ resemblance to popular trading card games such as Pokémon (Vasquez, 2003). This format could serve as a gateway to not only instilling foundational medical knowledge in younger individuals but also inspiring them to pursue careers in health sciences, as increased familiarity and understanding of STEM topics has been shown to significantly enhance students’ interest in and likelihood of entering related career fields (Blotnicky et al., 2018). By engaging adolescents with visually appealing and interactive educational tools, the Medimon Learning Cards may help foster early interest in complex scientific topics, making them more accessible and less intimidating. Such early exposure could play a pivotal role in shaping future generations of healthcare professionals (Berk et al., 2014). Beyond immunology, the card-based format could be adapted to other areas, such as pharmacology, anatomy, or pathology, creating a comprehensive suite of educational tools that appeal to both young learners and medical students.
The discussion of analog versus digital games further broadens the potential application of these tools. Analog games, such as the Medimon Learning Cards, provide tactile and interpersonal interaction, which can foster collaboration and critical thinking in group settings (Noda et al., 2019; von Steinkeller & Grosse, 2022). The thematic analysis of our results supports this notion, as the students commended the cards’ social and collaborative learning aspects, which are sometimes missing in digital games. Conversely, digital game platforms offer dynamic and immersive experiences that can incorporate adaptive learning technologies, real-time feedback, and multimedia elements (Khan et al., 2017), allowing them to provide additional detail, which was a downside of our analog game, as some students commented on the mismatch in detail between the Learning Cards and the material required of them in their courses and exams. By combining the strengths of both analog and digital formats, hybrid models could maximize the educational impact of Medimon-inspired tools. For instance, a digital platform could supplement the Medimon Learning Cards by providing additional content, interactive quizzes, or virtual gameplay, bridging the gap between analog and digital educational strategies.
As outlined in the Introduction, analog serious games like Medimon are aimed at pairing the motivational pull of gameplay with mnemonic imagery to mitigate cognitive load (Sweller, 1994). Our data confirm strong student engagement but show that this design alone is not sufficient for translating motivation into significant learning gains, underscoring the need for tighter alignment between game mechanics and assessed outcomes. In addition, the profile of the target players—first-year medical students, some of whom had prior experience with collectible trading-card games—likely influenced how the students engaged with the intervention. Likewise, the design of Medimon was shaped by the educational goals and personal interests of the instructor–designer, who is a medical school professor with experience in game-based learning. Prior research has emphasized that both player characteristics and designer intent significantly shape the effectiveness of educational games (Bartle, 2004; Vergara et al., 2023; Williams et al., 2008). Understanding this interplay may help optimize game design for diverse learner populations and instructional settings.
4.1. Limitations
This study provides valuable insights into the application of the mnemonic-based Medimon Learning Cards in medical education, but several limitations must be acknowledged. The small sample size of 39 students at a single WWAMI site limits the statistical power and generalizability of the findings, so this study is underpowered with respect to detecting small differences between groups; null findings should therefore be interpreted as ruling out only medium-to-large effects, not subtle ones.
Additionally, the three-week intervention may have been too brief to capture the full cognitive benefits of the Medimon Learning Cards, and the achievement tests may not have been sufficiently challenging or comprehensive to reflect potential differences in knowledge retention. The focus on a single topic, immune system content, restricts the evaluation of the cards’ versatility across other areas of medical education, such as pharmacology or anatomy. While the results of this study highlight strong engagement and satisfaction metrics, deeper cognitive outcomes, such as critical thinking or problem-solving skills, were not directly assessed. Additionally, some students in the Learning Card group only engaged with the Medimon Learning Cards shortly before the play session rather than using them consistently for study throughout the intervention period. This sporadic use may have limited the potential benefits of the cards, as their effectiveness likely depends on sustained interaction and integration into regular study routines.
Another limitation is that both groups were exposed to the core Medimon character mnemonics during in-class instruction. While the Learning Cards offered additional visual and textual reinforcements, it is possible that the primary learning benefit came from the character-based mnemonics themselves. If so, this shared exposure may have minimized measurable differences in achievement between groups.
Although SIS-M responses were gathered anonymously and no identifying data were recorded, self-report instruments are still susceptible to response distortions such as positive skew, acquiescence, and social-desirability effects. Because the research team administered the survey shortly after the intervention, the participants may have perceived an implicit expectation to provide favorable ratings. This residual bias could inflate engagement scores and should be considered when interpreting the findings. Future studies could reduce this risk by using a neutral third-party survey administrator.
The analog format of the Medimon Learning Cards, while fostering interpersonal interaction and accessibility, lacks the adaptive feedback and multimedia capabilities of digital platforms. Student enthusiasm for the novelty of the cards may have influenced engagement scores, and the uniform in-class instruction provided to both groups may have minimized potential additive effects.
4.2. Future Directions
Future research will explore longer-duration interventions and examine how Medimon Learning Cards can be integrated with other active learning strategies—such as digital versions of the game—to determine whether one format is more effective or whether combined approaches produce synergistic benefits. By extending the scope of these tools and examining their impact across diverse medical topics and student populations, we can better understand their full potential. Additionally, multi-site studies with larger cohorts would provide more robust data and enhance the generalizability of findings.
5. Conclusions
This study demonstrates that Medimon Learning Cards significantly enhance student engagement and satisfaction, though their impact on knowledge retention requires further investigation. The findings highlight the cards’ ability to significantly enhance student engagement and satisfaction, with many students expressing enthusiasm for expanding the scope of the cards to other topics. However, the lack of measurable differences in knowledge retention or exam performance suggests that the primary value of the Medimon Learning Cards lies in their ability to complement existing educational practices rather than replace them.
The results underscore the importance of designing interventions that balance engagement with cognitive outcomes. The integration of mnemonic-based tools, like Medimon Learning Cards, with traditional and active learning strategies holds promise for creating a holistic approach to medical education. Additionally, the adaptability of the cards to other medical topics and their potential appeal to younger audiences emphasize their versatility as a learning resource.
Future research should address the limitations of this study, including the short intervention duration and small sample size, to better reveal the full impact of such tools. Studies that incorporate longer-term interventions, diverse content areas, and multi-site participation can provide deeper insights into the efficacy and scalability of the Medimon Learning Cards.
While Medimon Learning Cards did not directly enhance cognitive outcomes in this study, their ability to engage and inspire learners highlights their potential as a supplementary educational resource. By leveraging innovative tools like these, educators can foster a more interactive and enjoyable learning environment, ultimately contributing to the development of future healthcare professionals.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/educsci15060768/s1. Figure S1: Learning cards used in the intervention. Methods S1: Rule book. Methods S2: Pre/posttest.
Author Contributions
Conceptualization, V.S. and T.B.; Methodology, V.S. and T.B.; Formal analysis, T.B.; Investigation, V.S. and T.B.; Data curation, T.B.; Writing—original draft, V.S. and T.B.; Writing—review & editing, T.B.; Visualization, C.B., E.F. and T.B.; Funding acquisition, T.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Idaho WWAMI Medical Education Program and the Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under Grant #P20GM103408.
Institutional Review Board Statement
This study was approved exempt by the institutional review board of the University of Idaho (24-151), 1 May 2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets presented in this article are not readily available because of the sensitive nature of students’ grades. Requests to access the datasets should be directed to Tyler Bland (tbland@uidaho.edu).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| GBL | Game-Based Learning |
| STEM | Science, Technology, Engineering, and Math |
| TCG | Trading-Card Game |
| SIS-M | Situational Interest Survey of Multimedia |
| genAI | Generative Artificial Intelligence |
| Trig | Triggered Interest |
| MT | Maintained Interest |
| MF | Maintained Feeling |
| MV | Maintained Value |
| LLM | Large Language Model |
| MCQ | Multiple-Choice Question |
| LLM | Large Language Model |
References
- Abou Hashish, E. A., Al Najjar, H., Alharbi, M., Alotaibi, M., & Alqahtany, M. M. (2024). Faculty and students perspectives towards game-based learning in health sciences higher education. Heliyon, 10(12), e32898. [Google Scholar] [CrossRef] [PubMed]
- Abt, C. C. (1987). Serious games. Available online: http://books.google.com/books?id=axUs9HA-hF8C (accessed on 20 January 2025).
- Alomar, Z., Guo, M., & Bland, T. (2025). AI-generated mnemonic images improve long-term retention of coronary artery occlusions in STEMI: A comparative study. Technologies, 13(6), 217. [Google Scholar] [CrossRef]
- Altschul, D. M., & Deary, I. J. (2020). Playing analog games is associated with reduced declines in cognitive function: A 68-year longitudinal cohort study. The Journals of Gerontology: Series B, 75(3), 474–482. [Google Scholar] [CrossRef] [PubMed]
- Bartle, R. A. (2004). Designing virtual worlds. New Riders. [Google Scholar]
- Bellezza, F. S. (1981). Mnemonic devices: Classification, characteristics, and criteria. Review of Educational Research, 51(2), 247–275. [Google Scholar] [CrossRef]
- Berk, L. J., Muret-Wagstaff, S. L., Goyal, R., Joyal, J. A., Gordon, J. A., Faux, R., & Oriol, N. E. (2014). Inspiring careers in STEM and healthcare fields through medical simulation embedded in high school science education. Advances in Physiology Education, 38(3), 210. [Google Scholar] [CrossRef]
- Bhugra, D., & Molodynski, A. (2024). Well-being and burnout in medical students: Challenges and solutions. Irish Journal of Psychological Medicine, 41(2), 175–178. [Google Scholar] [CrossRef]
- Bland, T. (2025). Enhancing medical student engagement through cinematic clinical narratives: Multimodal generative AI-based mixed methods study. JMIR Medical Education, 11(1), e63865. [Google Scholar] [CrossRef]
- Bland, T., & Guo, M. (2024). Visual mnemonics and gamification: A new approach to teaching muscle physiology. Journal of Technology-Integrated Lessons and Teaching, 3(1), 73–82. [Google Scholar] [CrossRef]
- Bland, T., Guo, M., & Dousay, T. A. (2024). Multimedia design for learner interest and achievement: A visual guide to pharmacology. BMC Medical Education, 24(1), 113. [Google Scholar] [CrossRef]
- Blotnicky, K. A., Franz-Odendaal, T., French, F., & Joy, P. (2018). A study of the correlation between STEM career knowledge, mathematics self-efficacy, career interests, and career activities on the likelihood of pursuing a STEM career among middle school students. International Journal of STEM Education, 5(1), 22. [Google Scholar] [CrossRef]
- Chang, L. Y., Tang, Y. Y., Lee, C. Y., & Chen, H. C. (2022). The effect of visual mnemonics and the presentation of character pairs on learning visually similar characters for chinese-as-second-language learners. Frontiers in Psychology, 13, 2031. [Google Scholar] [CrossRef] [PubMed]
- ChatGPT—USMLE step1 question generator and refiner. (n.d.). Available online: https://chatgpt.com/g/g-7kZBti7XN-usmle-step1-question-generator-and-refiner (accessed on 10 August 2024).
- Clark, J. M., & Paivio, A. (1991). Dual coding theory and education. Educational Psychology Review, 3(3), 149–210. [Google Scholar] [CrossRef]
- Densen, P. (2011). Challenges and opportunities facing medical education. Transactions of the American Clinical and Climatological Association, 122, 48. [Google Scholar]
- Deterding, S., Dixon, D., Khaled, R., & Nacke, L. (2011, September 29–30). From game design elements to gamefulness: Defining “gamification”. Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, MindTrek 2011 (pp. 9–15), Tampere, Finland. [Google Scholar] [CrossRef]
- Dousay, T. A. (2016). Effects of redundancy and modality on the situational interest of adult learners in multimedia learning. Educational Technology Research and Development, 64(6), 1251–1271. [Google Scholar] [CrossRef]
- Dousay, T. A., & Trujillo, N. P. (2019). An examination of gender and situational interest in multimedia learning environments. British Journal of Educational Technology, 50(2), 876–887. [Google Scholar] [CrossRef]
- Edwards, S. L., Zarandi, A., Cosimini, M., Chan, T. M., Abudukebier, M., & Stiver, M. L. (2024). Analog serious games for medical education: A scoping review. Academic Medicine, 100(3), 375–387. [Google Scholar] [CrossRef]
- Gentry, S. V., Gauthier, A., Ehrstrom, B. L. E., Wortley, D., Lilienthal, A., Car, L. T., Dauwels-Okutsu, S., Nikolaou, C. K., Zary, N., Campbell, J., & Car, J. (2019). Serious gaming and gamification education in health professions: Systematic review. Journal of Medical Internet Research, 21(3), e12994. [Google Scholar] [CrossRef]
- Graafland, M., Schraagen, J. M., & Schijven, M. P. (2012). Systematic review of serious games for medical education and surgical skills training. British Journal of Surgery, 99(10), 1322–1330. [Google Scholar] [CrossRef]
- Gu, J., Jiang, X., Shi, Z., Tan, H., Zhai, X., Xu, C., Li, W., Shen, Y., Ma, S., Liu, H., Wang, Y., & Guo, J. (2024). A survey on LLM-as-a-judge. Available online: https://arxiv.org/abs/2411.15594v3 (accessed on 20 January 2025).
- Gutierrez, C., Cox, S., & Dalrymple, J. (2016). The revolution in medical education. Texas Medicine, 112(2), 58–61. [Google Scholar] [PubMed]
- Hamari, J., Koivisto, J., & Sarsa, H. (2014, January 6–9). Does gamification work?—A literature review of empirical studies on gamification. Annual Hawaii International Conference on System Sciences (pp. 3025–3034), Waikoloa, HI, USA. [Google Scholar] [CrossRef]
- Ho, P. A., Girgis, C., Rustad, J., Noordsy, D., & Stern, T. (2021). Advancing medical education through innovations in teaching during the COVID-19 pandemic. The Primary Care Companion for CNS Disorders, 23(1), 25972. [Google Scholar] [CrossRef]
- Huang, J., Gu, S. S., Hou, L., Wu, Y., Wang, X., Yu, H., & Han, J. (2022, December 6–10). Large language models can self-improve. EMNLP 2023—2023 Conference on Empirical Methods in Natural Language Processing (pp. 1051–1068), Singapore. [Google Scholar] [CrossRef]
- Jones, J. S., Tincher, L., Odeng-Otu, E., & Herdman, M. (2015). An educational board game to assist PharmD students in learning autonomic nervous system pharmacology. American Journal of Pharmaceutical Education, 79(8), 114. [Google Scholar] [CrossRef] [PubMed]
- Khan, A., Ahmad, F. H., & Malik, M. M. (2017). Use of digital game based learning and gamification in secondary school science: The effect on student engagement, learning and gender difference. Education and Information Technologies, 22(6), 2767–2804. [Google Scholar] [CrossRef]
- Khorammakan, R., Omid, A., Mirmohammadsadeghi, M., & Ghadami, A. (2023). Puzzle game-based learning: A new approach to promote learning of principles of coronary artery bypass graft surgery. BMC Medical Education, 23(1), 241. [Google Scholar] [CrossRef]
- Klatt, E. C., & Klatt, C. A. (2011). How much is too much reading for medical students? Assigned reading and reading rates at one medical school. Academic Medicine, 86(9), 1079–1083. [Google Scholar] [CrossRef]
- Koivisto, J., & Hamari, J. (2019). The rise of motivational information systems: A review of gamification research. International Journal of Information Management, 45, 191–210. [Google Scholar] [CrossRef]
- Kuo, C. Y., Huang, Y. M., & Yeh, Y. Y. (2018). Let’s play cards: Multi-component cognitive training with social engagement enhances executive control in older adults. Frontiers in Psychology, 9, 2482. [Google Scholar] [CrossRef]
- Lubin, J., & Polloway, E. A. (2016). Mnemonic instruction in science and social studies for students with learning problems: A review. Learning Disabilities: A Contemporary Journal, 14(2), 207–224. [Google Scholar]
- Mayer, R. E. (2005). Introduction to multimedia learning. In The Cambridge handbook of multimedia learning (pp. 1–16). Cambridge University Press. [Google Scholar] [CrossRef]
- Mayer, R. E. (2012). Cognitive theory of multimedia learning. In The Cambridge handbook of multimedia learning (pp. 31–48). Cambridge University Press. [Google Scholar] [CrossRef]
- Mostafa, E. A., & El Midany, A. A. H. (2017). Review of mnemonic devices and their applications in cardiothoracic surgery. Journal of the Egyptian Society of Cardio-Thoracic Surgery, 25(1), 79–90. [Google Scholar] [CrossRef]
- NBME item-writing guide | NBME. (n.d.). Available online: https://www.nbme.org/educators/item-writing-guide (accessed on 24 July 2024).
- Noda, S., Shirotsuki, K., & Nakao, M. (2019). The effectiveness of intervention with board games: A systematic review. BioPsychoSocial Medicine, 13(1), 22. [Google Scholar] [CrossRef]
- Ober, C. (2018). Comparison of a novel card game and conventional case-based studying for learning urologic differential diagnoses in veterinary radiology. Education in the Health Professions, 1(2), 44. [Google Scholar] [CrossRef]
- O’Hanlon, R., & Laynor, G. (2019). Responding to a new generation of proprietary study resources in medical education. Journal of the Medical Library Association: JMLA, 107(2), 251. [Google Scholar] [CrossRef] [PubMed]
- Putnam, A. L. (2015). Mnemonics in education: Current research and applications. Translational Issues in Psychological Science, 1(2), 130–139. [Google Scholar] [CrossRef]
- Radović, T., & Manzey, D. (2019). The impact of a mnemonic acronym on learning and performing a procedural task and its resilience toward interruptions. Frontiers in Psychology, 10, 493110. [Google Scholar] [CrossRef]
- Samarasekera, D. D., Goh, P. S., Lee, S. S., & Gwee, M. C. (2018). The clarion call for a third wave in medical education to optimise healthcare in the twenty-first century. Medical Teacher, 40(10), 982–985. [Google Scholar] [CrossRef] [PubMed]
- Scruggs, T. E., & Mastropieri, M. A. (1990). Mnemonic instruction for students with learning disabilities: What it is and what it does. Learning Disability Quarterly, 13(4), 271–280. [Google Scholar] [CrossRef]
- Step 1 sample test questions | USMLE. (n.d.). Available online: https://www.usmle.org/exam-resources/step-1-materials/step-1-sample-test-questions (accessed on 24 July 2024).
- Sweller, J. (1994). Cognitive load theory, learning difficulty, and instructional design. Learning and Instruction, 4(4), 295–312. [Google Scholar] [CrossRef]
- van Gaalen, A. E. J., Brouwer, J., Schönrock-Adema, J., Bouwkamp-Timmer, T., Jaarsma, A. D. C., & Georgiadis, J. R. (2021). Gamification of health professions education: A systematic review. Advances in Health Sciences Education, 26(2), 683. [Google Scholar] [CrossRef]
- Vasquez, V. (2003). What pokemon can teach us about learning and literacy. Language Arts, 81(2), 118–125. [Google Scholar] [CrossRef]
- Vergara, D., Gómez-Vallecillo, A. I., Fernández-Arias, P., & Antón-Sancho, Á. (2023). Gamification and player profiles in higher education professors. International Journal of Game-Based Learning (IJGBL), 13(1). [Google Scholar] [CrossRef]
- Vita-Barrull, N., Estrada-Plana, V., March-Llanes, J., Guzmán, N., Fernández-Muñoz, C., Ayesa, R., & Moya-Higueras, J. (2023). Board game-based intervention to improve executive functions and academic skills in rural schools: A randomized controlled trial. Trends in Neuroscience and Education, 33, 100216. [Google Scholar] [CrossRef]
- von Steinkeller, A., & Grosse, G. (2022). Children are more social when playing analog games together than digital games. Computers in Human Behavior Reports, 6, 100195. [Google Scholar] [CrossRef]
- Wang, J., Liu, Z., Zhao, L., Wu, Z., Ma, C., Yu, S., Dai, H., Yang, Q., Liu, Y., Zhang, S., Shi, E., Pan, Y., Zhang, T., Zhu, D., Li, X., Jiang, X., Ge, B., Yuan, Y., Shen, D., … Zhang, S. (2023). Review of large vision models and visual prompt engineering. Meta-Radiology, 1(3), 100047. [Google Scholar] [CrossRef]
- Wang, R., DeMaria, S., Goldberg, A., & Katz, D. (2016). A systematic review of serious games in training: Health care professionals. Simulation in Healthcare, 11(1), 41–51. [Google Scholar] [CrossRef] [PubMed]
- White, J., Fu, Q., Hays, S., Sandborn, M., Olea, C., Gilbert, H., Elnashar, A., Spencer-Smith, J., & Schmidt, D. C. (2023). A prompt pattern catalog to enhance prompt engineering with ChatGPT. Available online: https://arxiv.org/abs/2302.11382v1 (accessed on 18 June 2024).
- Williams, D., Yee, N., & Caplan, S. E. (2008). Who plays, how much, and why? Debunking the stereotypical gamer profile. Journal of Computer-Mediated Communication, 13(4), 993–1018. [Google Scholar] [CrossRef]
- Worthley, B., Guo, M., Sheneman, L., & Bland, T. (2025). Antiparasitic pharmacology goes to the movies: Leveraging generative AI to create educational short films. AI, 6(3), 60. [Google Scholar] [CrossRef]
- Xu, M., Luo, Y., Zhang, Y., Xia, R., Qian, H., & Zou, X. (2023). Game-based learning in medical education. Frontiers in Public Health, 11, 1113682. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).