3.2. Number of Steps
The participants took, on average, 12,034 steps per day. Total steps reported elsewhere in the international literature approximately range anywhere from 10,000 to 16,000 [
13], 10,906 to 12,259 [
15], or 9377 to 10,738 [
8]. The steps observed in this study (
Table 6) suggest that, in terms of their overall pedometer-measured PA, children in Malta are generally at par with those in other countries.
It could be argued that participants in both the treatment and control groups demonstrated the attainment of over 10,000 steps. Within the framework specified by Naseer [
17], all students participating in the study conducted in Malta could be classified as physically active. This assertion aligns with criteria established in international literature, which categorises students aged 13–16 as inactive if they achieve fewer than 10,000 daily steps and as physically active if they surpass this threshold on all days of the week. While the 10,000 steps/day was recognised as a cut-off point [
18], on the basis of the data presented in the literature, Gomersall et al. [
19] indicated that we could expect boys (typically between 6–11 years) to average 12,000 to 16,000 daily steps and girls to average 10,000 to 13,000 daily steps. There is scant evidence that maintaining total daily physical activity within the range of 10,000 to 14,000 steps is correlated with engaging in 60 to 100 min of moderate to vigorous physical activity [
20].
With an average of 5215 steps taken exclusively during school hours, the percentage of total steps taken at school was 43%. In their systematic review of 31 pedometer-based studies worldwide, out of a total of 12k to 16k steps per weekday for boys, and 10k to 14k for girls, Tudor-Locke et al. [
13] reported that 42–48% of total steps occurred at school in the case of boys and 41–47% for girls. The 4239 steps taken by those in the control group and 5836 by those in the treatment group represent 35% and 48% of total average daily steps, respectively. This suggests that, with a daily PA programme in place, Maltese state primary schools, at least in the case of Year Four classes, fall on the low side of international conventions (41 to 48%). In the context of the relevant literature, Malta’s closest neighbour, Cyprus, reported 41 to 44% among children aged 10 to 12. Therefore, introducing a daily PA programme in schools pulls Maltese schools up to the high end of Tudor-Locke et al.’s proportion range in terms of contribution to overall daily PA. Relative to other countries, with daily PA sessions in place, Maltese schools have the potential to attain world-leading capacity in terms of PA provision.
While, as shown in
Table 7, there was a difference between girls (
M = 10,794) and boys (
M = 13,026) in absolute terms, as reported elsewhere [
8,
14,
17], the difference (−2232) was not statistically significant (
t = 47,
df = 16,
p = 0.89). It cannot be claimed with confidence, therefore, that PA differs systematically between girls and boys attending primary state schools in Malta.
3.3. Effects of School Intervention on the Step Count
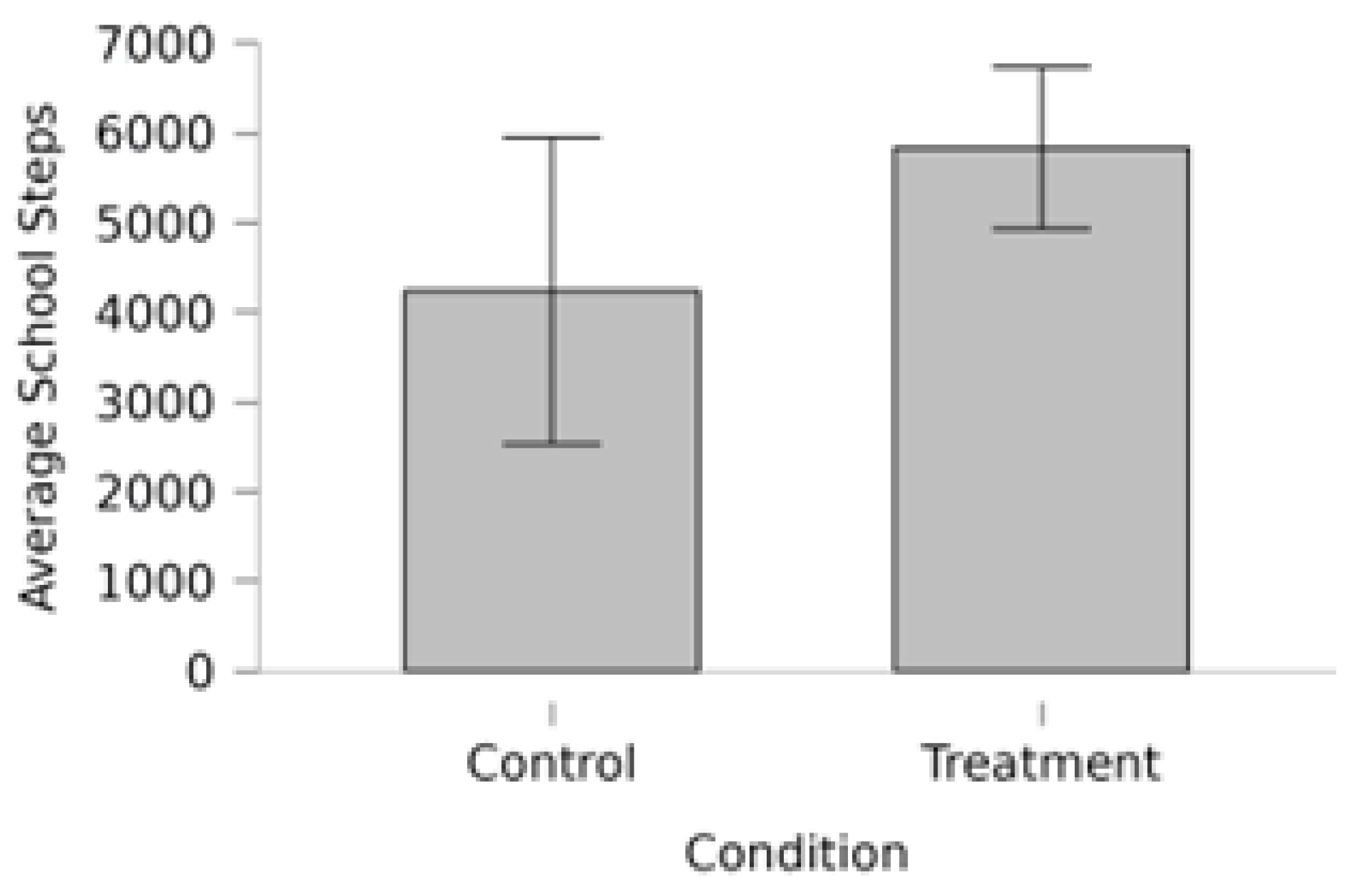
H1 posited that mean steps performed during school hours varied across the treatment and control groups. This hypothesis sought to test whether school days with or without structured daily PA sessions resulted in significant differences in overall pedometer-measured activity. There was a mean difference of 1597 steps per day between the treatment (
M = 5836) and control (
M = 4239) groups, which was statistically significant (
p = 0.03) (
Table 7).
Figure 1 provides a visual illustration of this difference.
Our findings support those of Varela Garrote et al. [
8], in that school days with structured PA sessions systematically differ from those without. However, our results differ regarding whether such a difference holds in the context of overall steps performed throughout the day.
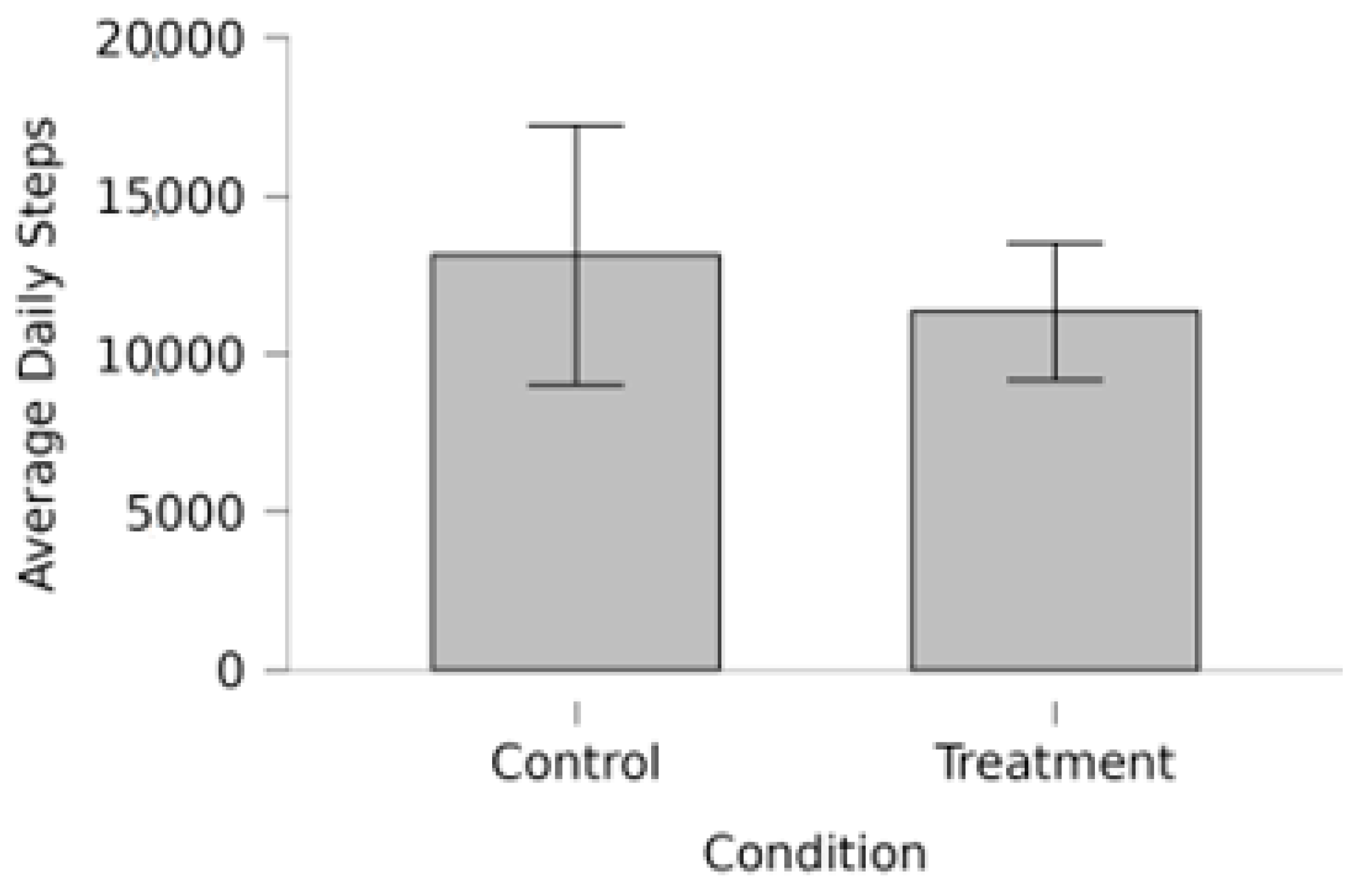
H2 posited that the mean total daily steps varied across the treatment and control groups. In order to make the evidence-based claim that a school-based PA intervention exerts a significant effect on overall PA, it would be necessary to reject the null hypothesis of no difference between the treatment and control groups in terms of overall daily steps. However, the evidence was insufficient to reject this null hypothesis (
p = 0.83) (
Table 7). Although statistically insignificant, the descriptives actually reveal more steps in the control group (
M = 13,127) than in the treatment group (
M = 11,338). Bars and confidence bands are shown in
Figure 2.
The results suggest that, while PA sessions at school significantly increase steps taken during school hours, such an effect becomes dissipated when considering overall variations in steps that take place throughout the day. In other words, the results suggest that total variations in PA occurring naturally among children in Malta are sufficient to mask any significant, systemic effect of structured PA carried out at school. At this stage, our results diverge from Varela Garrote et al. [
8], who reported that, on weekdays, Spanish 10-year-olds took a significantly different amount of total daily steps on days with (10,738) and without (9377) PE lessons. Given the relatively low number of steps taken overall by children in the Varela Garrote et al. study, it is likely that the steps associated with a normal structured PE session at school were equivalent to a higher proportion of total steps and, therefore, a stronger effect size. In other words, the more steps children take overall, the less significant the contribution of a single PE/PA lesson at school is likely to be.
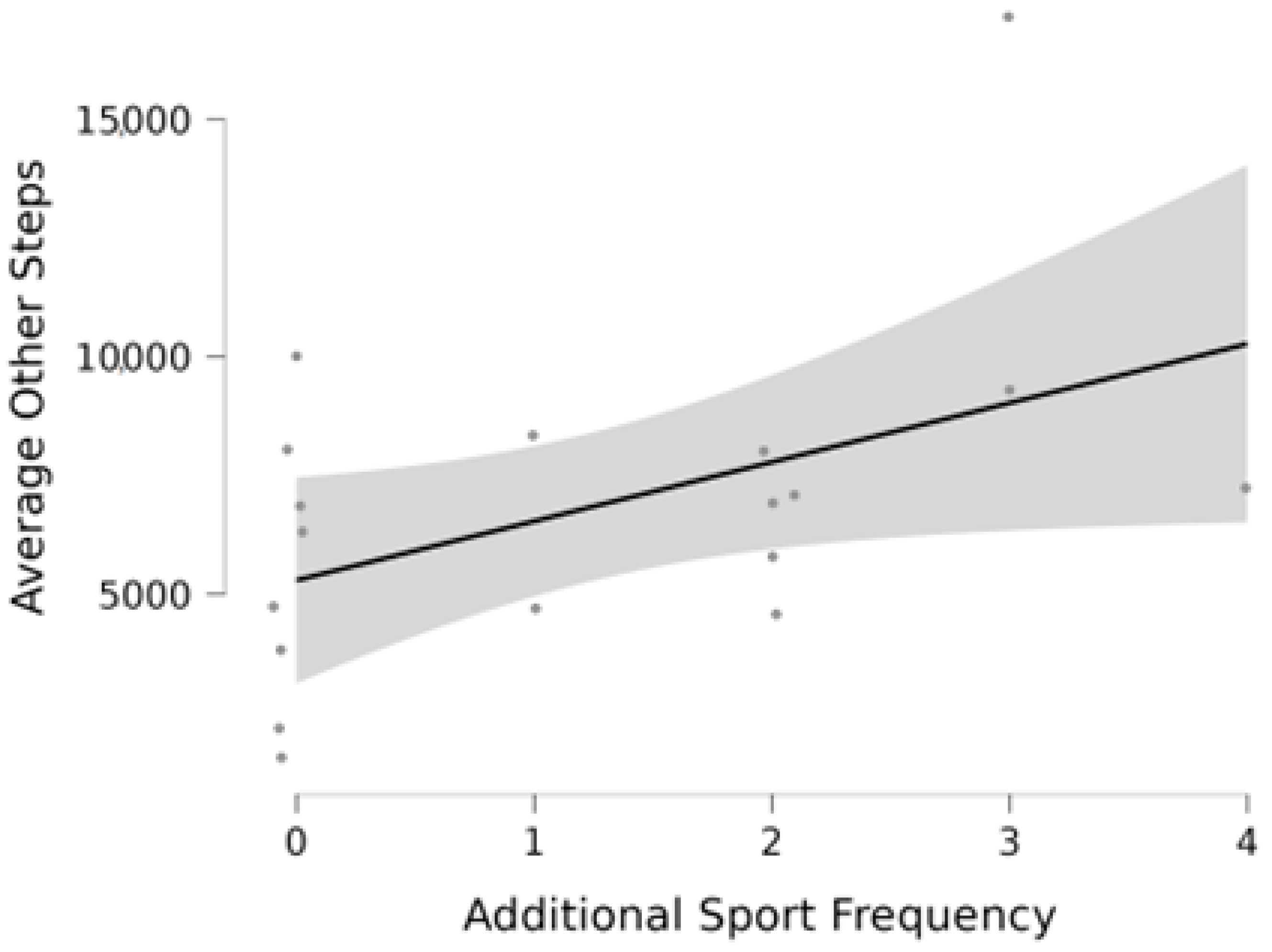
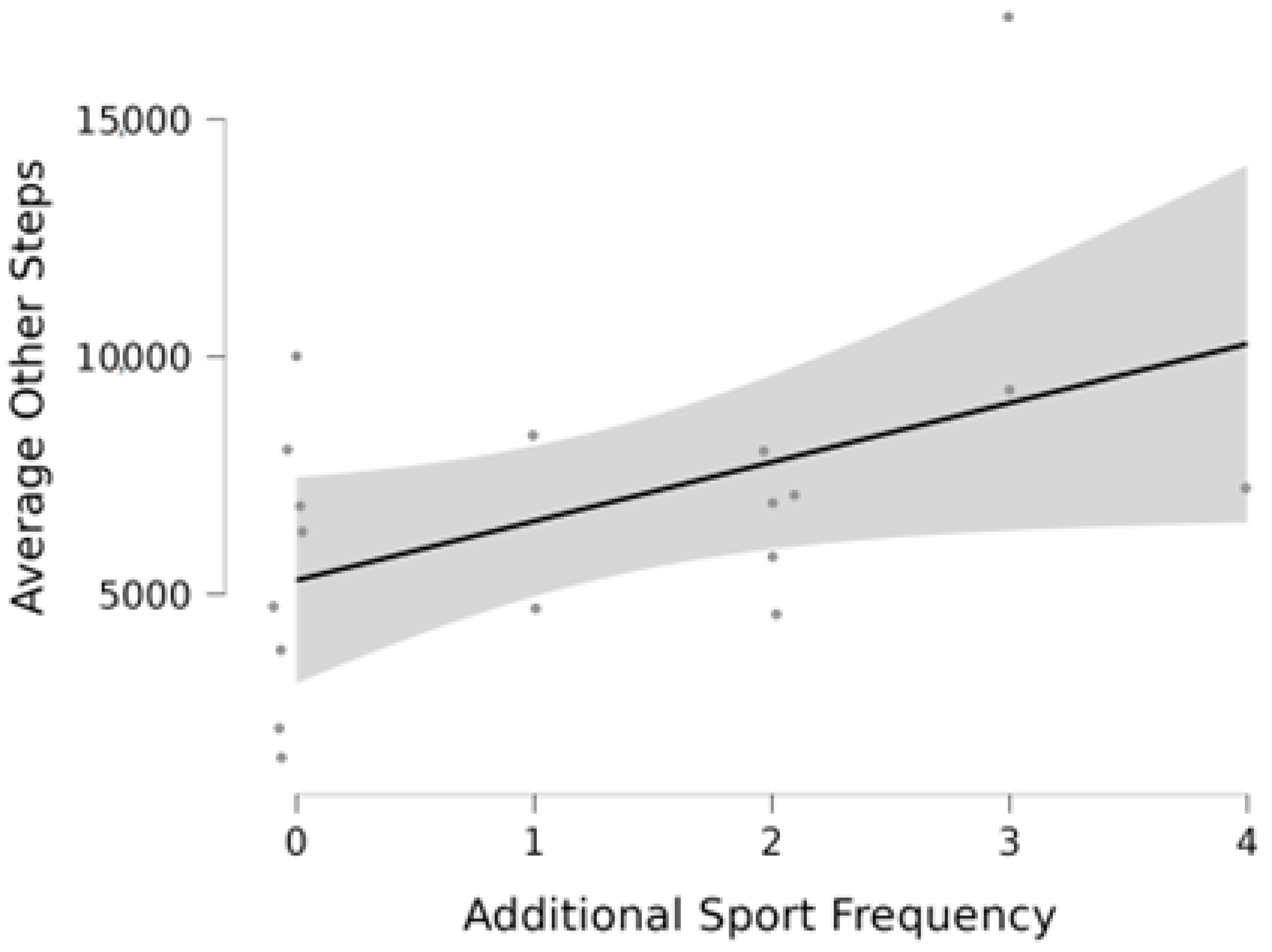
H3 posited that mean steps beyond school hours are associated with the weekly frequency of structured sports or PA sessions performed outside of school (
Figure 3). This hypothesis looked to ascertain if the number of daily steps taken, on average, corresponds to how active children are in terms of their participation in structured sports or PA outside of school. The evidence was not sufficient to reject the null hypothesis of no association (
rs = 0.43,
p = 0.07). In other words, the evidence does not support the idea that structured sports/PA among children in Malta has any significant and systemic impact on the amount of PA children engage in after school hours. Additional research has posited a link between socioeconomic status and participation in sports among children in Malta [
21]; therefore, future studies might investigate whether the effect of sports participation on PA among the entire population is confounded by restricted access to sports participation among those children raised in low socioeconomic conditions.
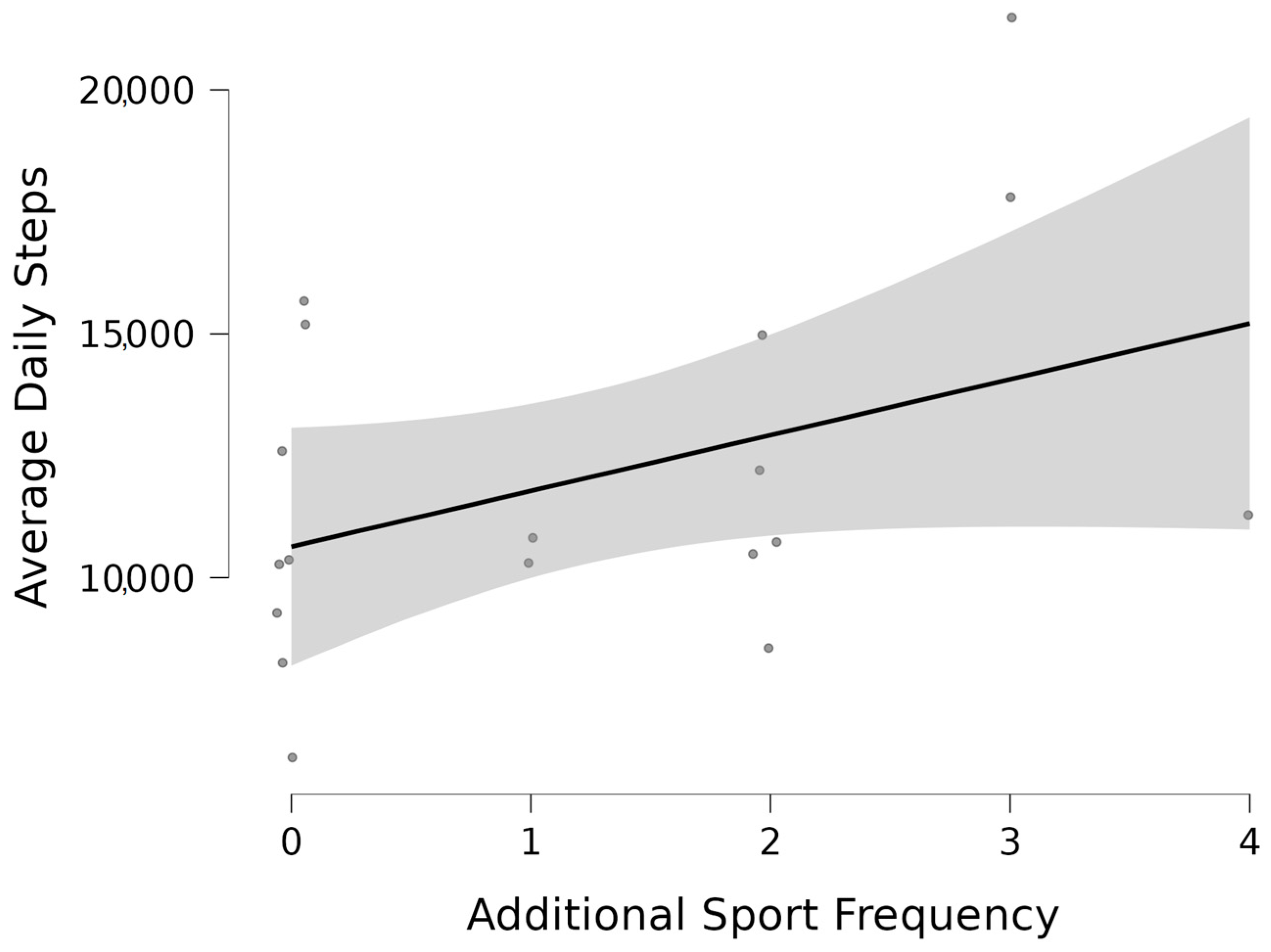
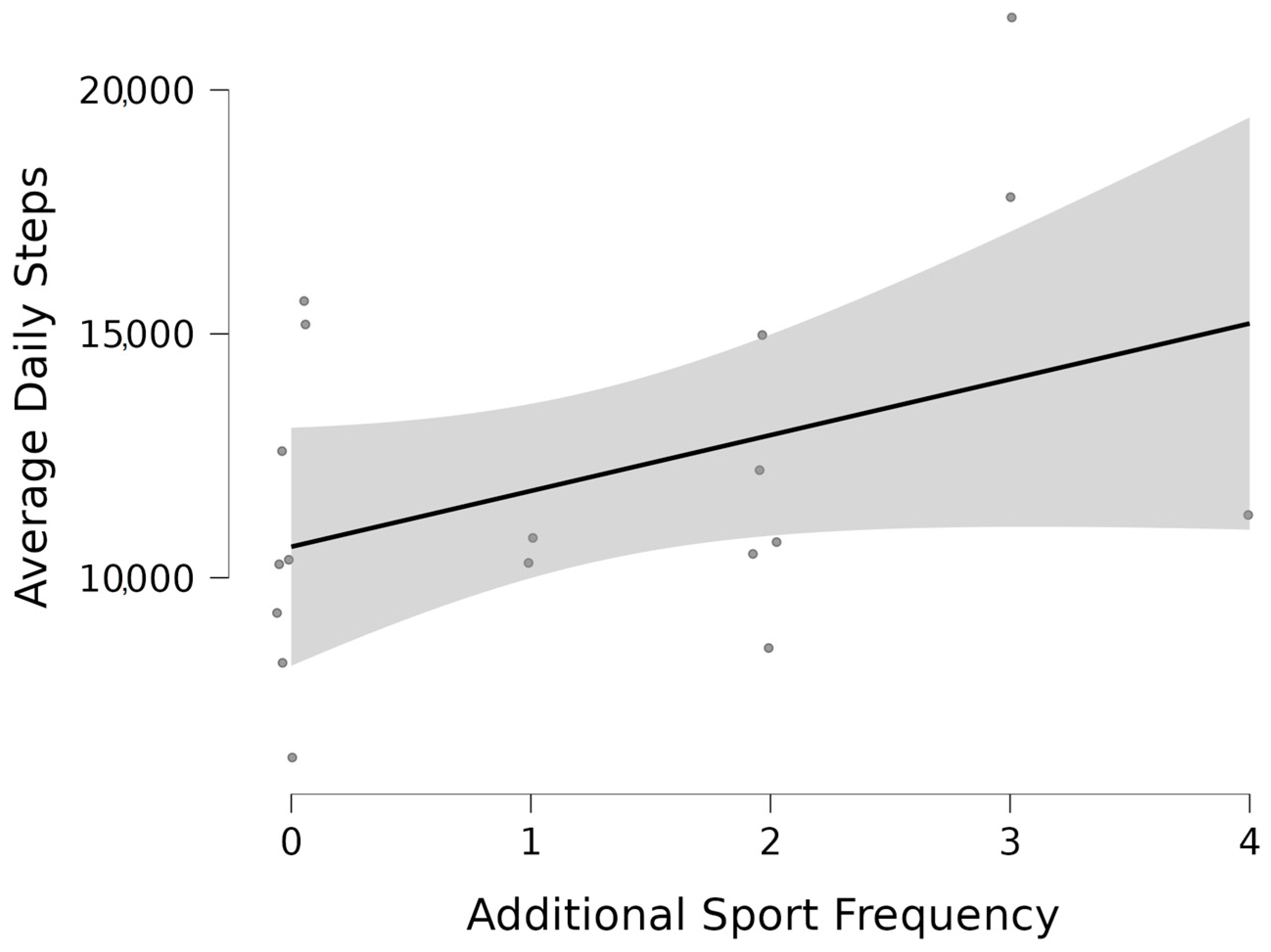
H4 further posited that mean total steps are associated with the weekly frequency of extra sport sessions (
Figure 4). Given that the frequency of structured sport/PA participation outside of school was not sufficient to predict overall activity outside of school hours, it was not surprising that no significant effect was observed on overall daily steps (
rs = 0.40,
p = 0.10). As was the case for school-based PA, the effects of participation in structured sports/PA outside of school tended to become washed out by the natural variations in overall step counts in the broader sense.
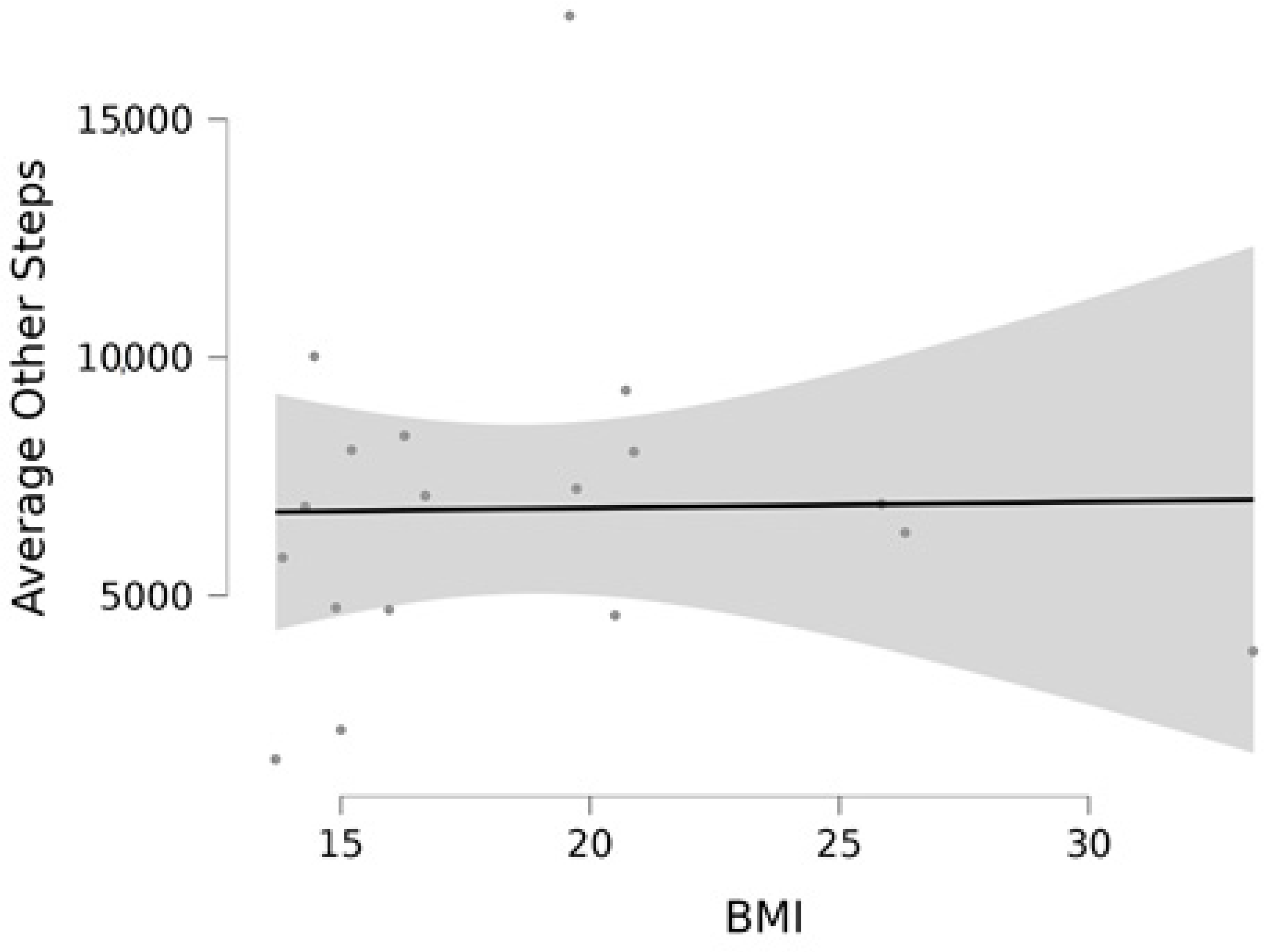
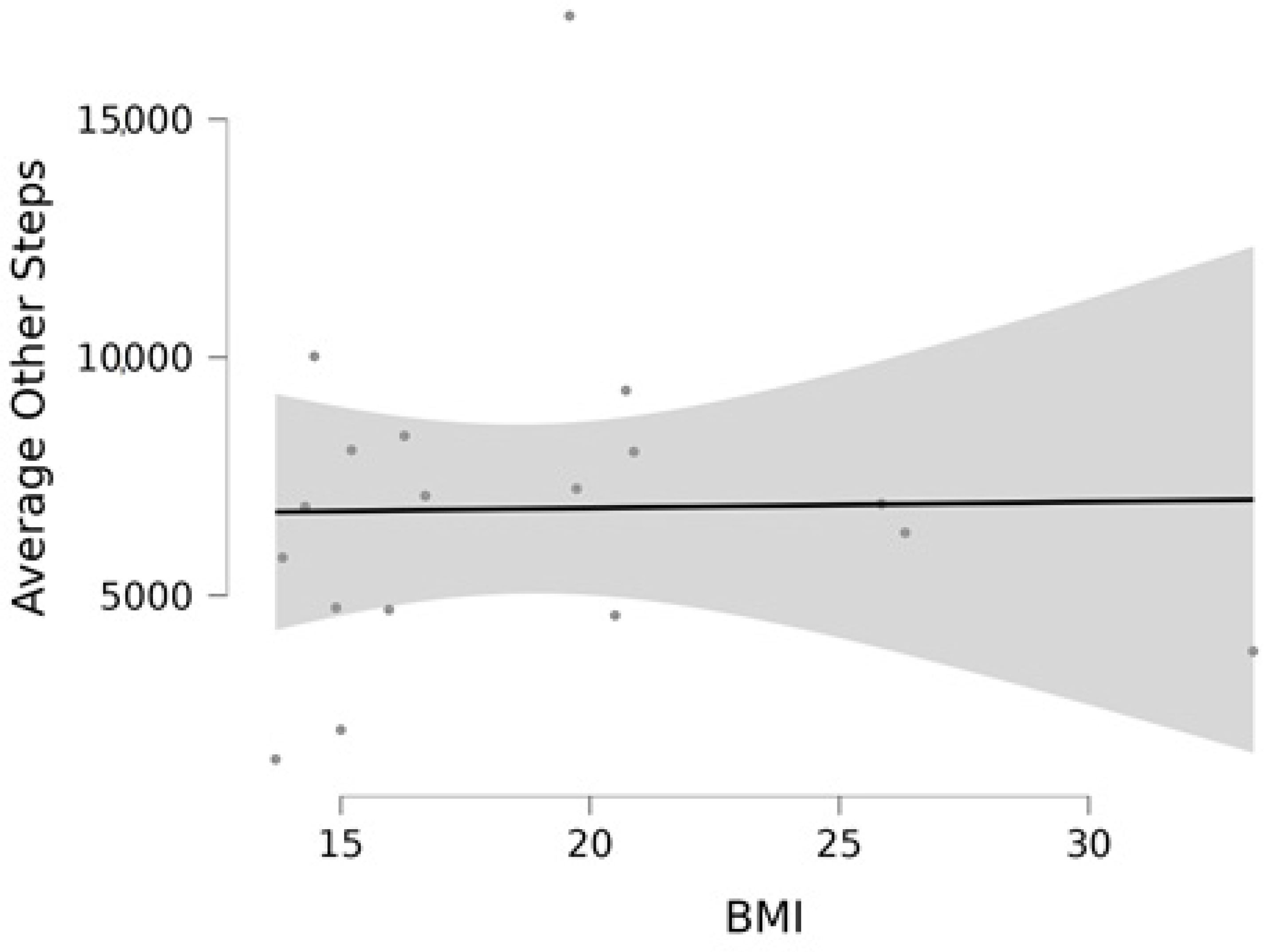
Finally,
H5 posited that mean steps beyond school hours are associated with BMI. The aim here was to ascertain if activity levels beyond the structured routine of the school environment are related to body composition. More specifically, rejection of the null hypothesis of no association would suggest that body weight influences how much activity children perform in the home environment, in which parents and children likely have a stronger influence on behaviour than school administrators. The evidence, however, was insufficient to reject the null hypothesis (
rs = 0.15,
p = 0.55), suggesting that body mass is unrelated to optional, structured sports and PA participation outside of school (
Figure 5). In other words, it is unlikely that a high BMI is a result of home-based inactivity or vice versa (a high BMI does not likely influence home-based inactivity). Similarly, one can argue that a low BMI does not predispose a child to participate in more sports or PA outside school, and sports participation outside school likewise does not cause low BMI.
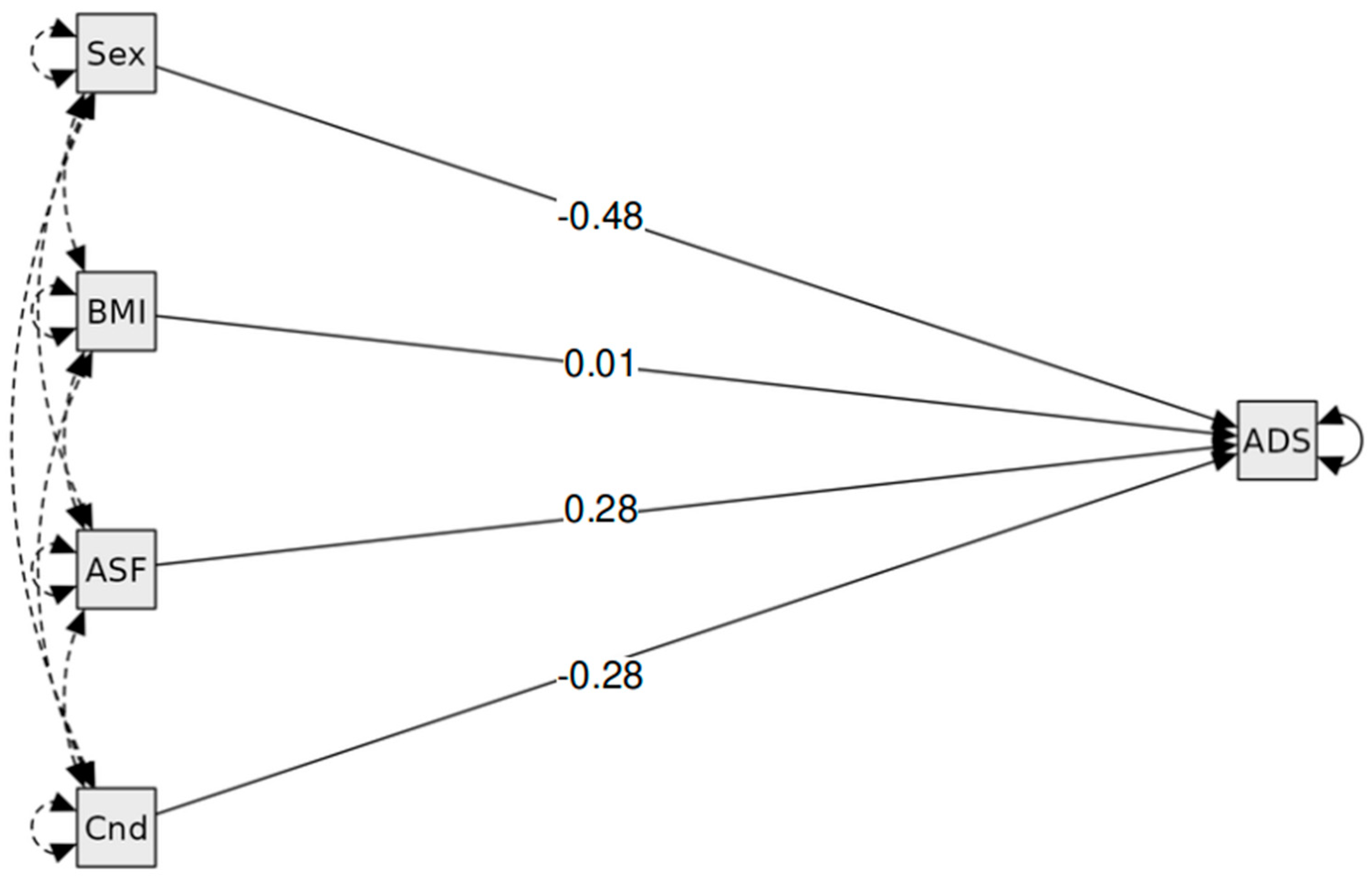
Table 8 summarises the results of the hypotheses tests performed. Finally, a model is presented (numerically in
Table 9 and visually in
Figure 6 below), explaining average daily steps as a function of treatment (participating in a daily school-based PA intervention), extra sport after school, and BMI. Standardised regression coefficient estimates and associated
p values showed no significant effects of the relevant factors on the outcome of average steps overall.
The model accounted for only a quarter of the variation in mean daily steps (R2 = 0.26), with none of the factors included representing significant predictors. In other words, the treatment did not have an effect on total average daily steps, controlling for BMI regardless of additional sports participation. The model also shows that, when controlling for additional sports participation and doing daily PA in school, BMI is not associated with total steps performed daily, on average.



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}