A Consumer Health Information System to Assist Patients Select Quality Home Health Services †


Abstract
:1. Introduction
2. Materials and Methods
- ■
- Star Rating, summary of HCAHPS survey (Summary);
- ■
- Star rating, health care services quality (Quality);
- ■
- Star rating, professionalism of care from health team (Professionalism);
- ■
- Star Rating, communication of health team with patient (Communication);
- ■
- Percentage of patients who would definitely recommend the HHA to friends and family (% Recommend).
3. Results
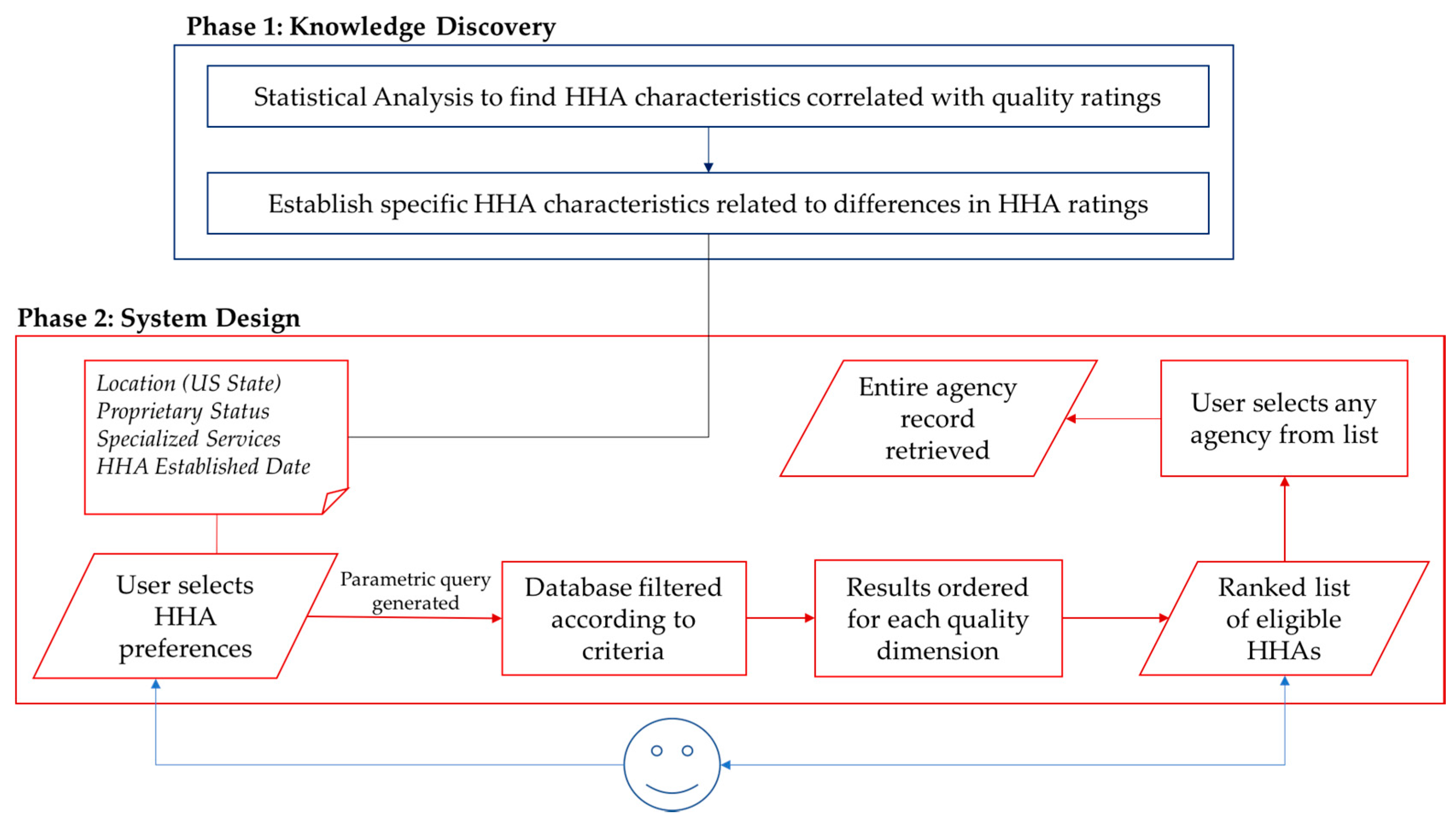
3.1. Knowledge Discovery Phase
3.1.1. Relationship between HCAHPS Ratings and HHA Age
3.1.2. Comparison of HCAHPS Ratings According to the Services Offered
3.1.3. Comparison of HCAHPS Ratings across HHAs in Different US States
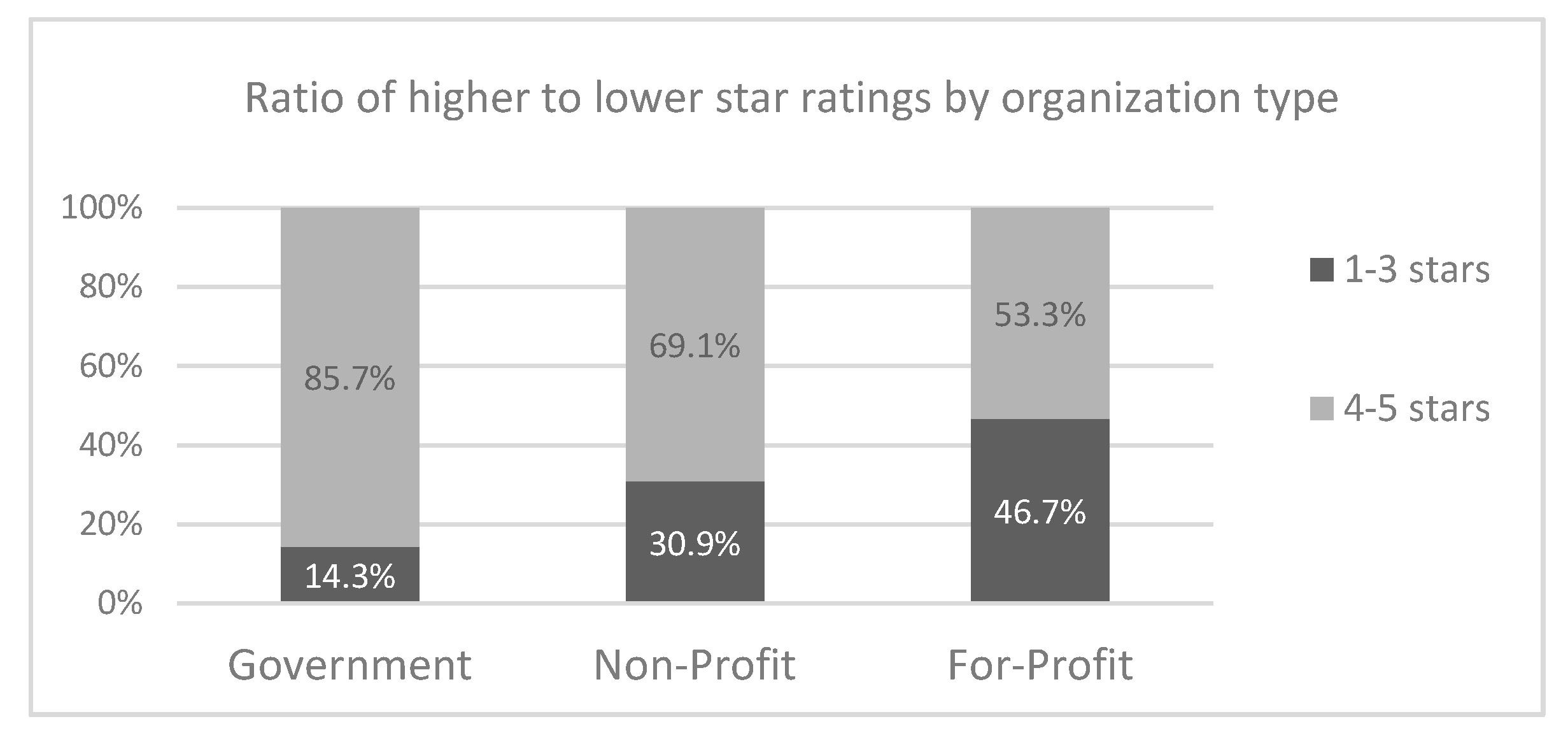
3.1.4. Comparison of HCAHPS Ratings across the Three Proprietary Status Types
3.2. System Design Phase: Prototype CHI System to Assist Patients Compare HHAs
- (i)
- Select preferred criteria to see eligible HHAs and ratings for each of these HHAs. Search results are presented to the user in a ranked order. These criteria include
- Preference for specialized service offered by the HHA;
- Patient location;
- Proprietary Status;
- HHA year of establishment.
- (ii)
- The system provides to the user the option to view plots comparing HHAs based on the aforementioned system output;
- (iii)
- Alternatively, the user can search directly for a specific agency name to view information about that agency (HHA characteristics and star ratings). In this case, the system auto-generates a query that filters down the database, according to the characteristics of the selected agency. The user-selected HHA is therefore ranked against the filtered results. The user is informed accordingly how their selection stacks up against similar agencies for each of the quality star ratings under study;
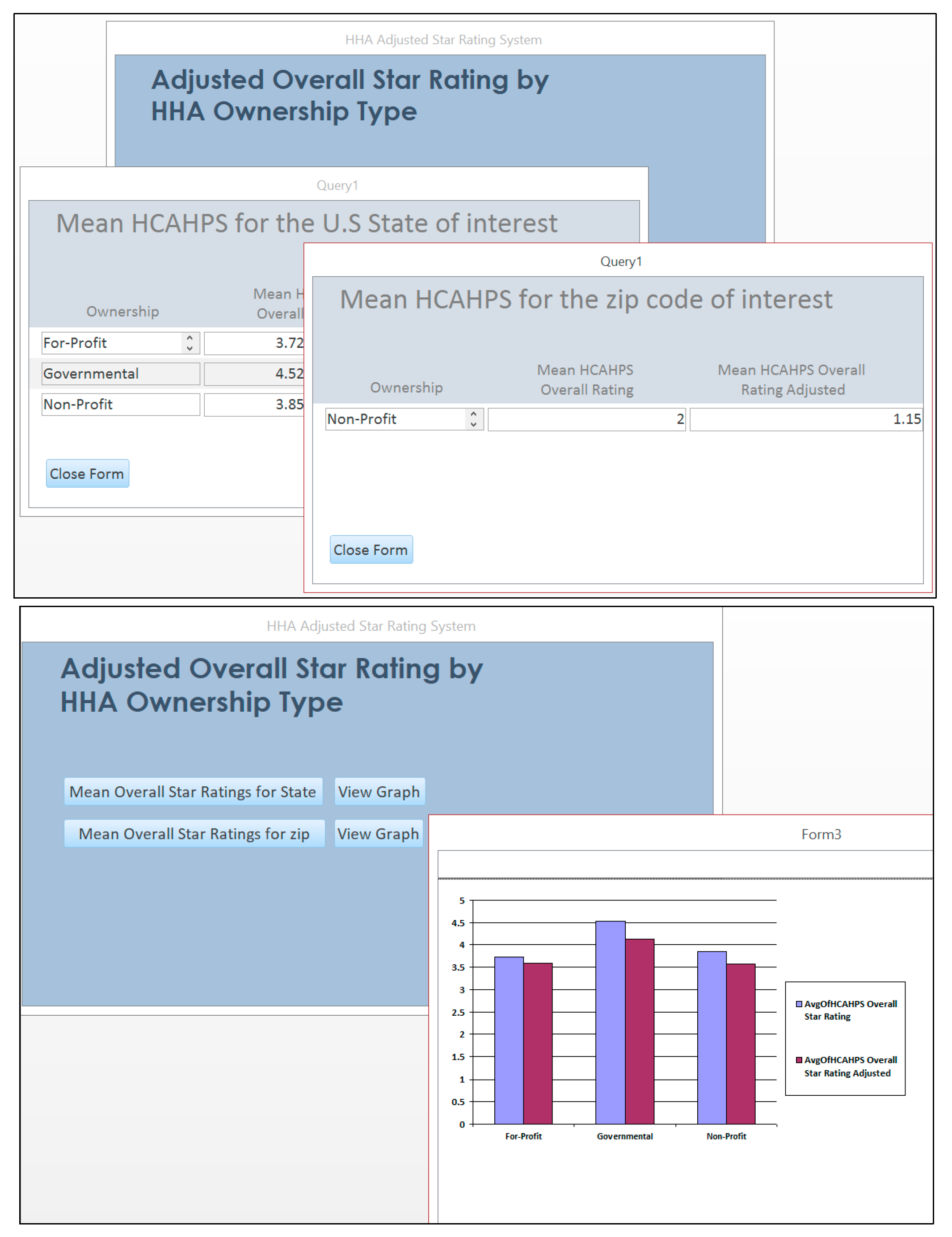
- (iv)
- The user can explore plots to compare the overall rating scores and adjusted scores of each HHA proprietary status types for the US state, zip code, or home health agency of interest.
4. Discussion
Author Contributions
Conflicts of Interest
References
- Konetzka, R.T.; Perraillon, M.C. Use of nursing home compare website appears limited by lack of awareness and initial mistrust of the data. Health Aff. 2016, 35, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.S. Market Conditions and Performance in the Nursing Home Compare Five-Star Rating. J. Health Politics Policy Law 2016, 41, 939–968. [Google Scholar] [CrossRef] [PubMed]
- Sprague, L. The Star Rating System and Medicare Advantage Plans. Issue Brief Natl. Health Policy Forum 2015, 854, 1–10. [Google Scholar]
- Werner, R.M.; Konetzka, R.T.; Polsky, D. Changes in consumer demand following public reporting of summary quality ratings: An evaluation in nursing homes. Health Serv. Res. 2016, 51, 1291–1309. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.A.; Hanson, K.T.; Yost, K.J.; Mathis, K.L.; Cima, R.R.; Zielinski, M.D.; Habermann, E.B. Achieving a 5-star rating: Analysis of hospital consumer assessment of healthcare providers and systems (HCAHPS) scores among patients undergoing elective colorectal operations. Surgery 2016, 160, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.C.; Morton, D.J.; Braun, B.I.; Longo, B.A.; Baker, D.W. Comparing Public Quality Ratings for Accredited and Non-Accredited Nursing Homes. J. Am. Med. Dir. Assoc. 2017, 18, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Desai, V.; Nau, D.; Conklin, M.; Heaton, P.C. Impact of Environmental Factors on Differences in Quality of Medication Use: An Insight for the Medicare Star Rating System. J. Manag. Care Spec. Pharm. 2016, 22, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Konetzka, R.T.; Grabowski, D.C.; Perraillon, M.C.; Werner, R.M. Nursing home 5-star rating system exacerbates disparities in quality, by paper source. Health Aff. 2015, 34, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.E.; Tsugawa, Y.; Figueroa, J.F.; Jha, A.K. Association between the centers for medicare and medicaid services hospital star rating and patient outcomes. JAMA Intern. Med. 2016, 176, 848–850. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.A.; Hanson, K.T.; Yost, K.J.; Zielinski, M.D.; Habermann, E.B.; Cima, R.R. Effect of Hospital Case Mix on the Hospital Consumer Assessment of Healthcare Providers and Systems Star Scores: Are All Stars the Same? Ann. Surg. 2016, 264, 666–673. [Google Scholar] [CrossRef] [PubMed]
- American Medical Informatics Association. Consumer Health Informatics. Available online: https://www.amia.org/applications-informatics/consumer-health-informatics (accessed on 23 November 2017).
- Faiola, A.; Holden, R. Consumer Health Informatics: Empowering Healthy-Living-Seekers Through mHealth. Prog. Cardiovasc. Dis. 2017, 59, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Monkman, H.; Kushniruk, A.W. The Consumer Health Information System Adoption Model. Stud Health Technol. Inform. 2015, 218, 26–31. [Google Scholar]
- LeRouge, C.; Wickramasing, N. A Review of User-Centered Design for Diabetes-Related Consumer Health Informatics Technologies. J. Diabetes Sci. Technol. 2013, 7, 1039–1056. [Google Scholar] [CrossRef] [PubMed]
- Medicare. Home Health Compare Datasets. Available online: https://data.medicare.gov/data/home-health-compare (accessed on 23 November 2017).
- O'Brien, M.; Stewart, S.J. Measuring satisfaction with social work services. Soc. Work Health Care 2009, 48, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Daigle, S.; Mojica, J.; Hurley, RW. Patient perception of pain care in hospitals in the United States. J. Pain Res. 2009, 2, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Nothelle, S.K.; Sharma, R.; Oakes, A.H.; Jackson, M.; Segal, J.B. Determinants of Potentially Inappropriate Medication Use in Long-Term and Acute Care Settings: A Systematic Review. J. Am. Med. Dir. Assoc. 2017, 18, 806.e1–806.e17. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.B.; Wilson, I.B.; Trivedi, A.N. State Variation in Quality Outcomes and Disparities in Outcomes in Community Health Centers. Med. Care 2017, 55, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma-Frankema, K.; Woolthuis, R.K. Trust under Pressure: Empirical Investigations of Trust and Trust Building in Uncertain Circumstances; Edward Elgar: Cheltenham, UK; Northampton, MA, USA, 2005. [Google Scholar]
- Hu, J.; Jordan, J.; Rubinfeld, I.; Schreiber, M.; Waterman, B.; Nerenz, D. Correlations among Hospital Quality Measures: What “Hospital Compare” Data Tell Us. Am. J. Med. Qual. 2016, 32, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Sinaiko, A.D.; Eastman, D.; Rosenthal, M.B. How report cards on physicians, physician groups, and hospitals can have greater impact on consumer choices. Health Aff. 2012, 3, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Gebele, C.; Tscheulin, D.K.; Lindenmeier, J.; Drevs, F.; Seemann, A.K. Applying the concept of consumer confusion to healthcare: Development and validation of a patient confusion model. Health Serv. Manag. Res. 2014, 27, 10–21. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Std. Dev. | Range |
|---|---|---|---|
| Home Health Agency Age (years) | 22.38 | 13.22 | 49 |
| Percent of Governmental agencies (%) | 5.32 | 22.40 | 100 |
| HHAs Offering Physical Therapy Services (%) | 100 | 4.70 | 100 |
| HHAs Offering Speech Pathology Services (%) | 94 | 24 | 100 |
| HHAs Offering Medical Social Services (%) | 89 | 31.0 | 100 |
| HHAs Offering Home Health Aide Services (%) | 97 | 15.9 | 100 |
| HCAHPS Survey Summary Star Rating (5 pt. scale) | 3.64 | 0.92 | 4 |
| HCAHPS Star Rating: Quality of Patient Care Star Rating (5 pt. scale) | 3.36 | 0.80 | 4 |
| HCAHPS Star Rating: Health Team Gave Care in a Professional Way (5 pt. scale) | 3.88 | 1.01 | 4 |
| HCAHPS Star Rating: Health Team Communicated Well With Them (5 pt. scale) | 3.92 | 0.99 | 4 |
| Patients Would Definitely Recommend HHA to Friends & Family (%) | 79.22 | 8.37 | 73 |
| HCAHPS Summary | Quality of Patient Care | Professional Care | Communication with Patient | % Recommend HHA | ||
|---|---|---|---|---|---|---|
| Year ESTD | Pearson | −0.209 | −0.051 | −0.201 | −0.247 | −0.230 |
| Sig (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Service | Offered | N | Mean | St. Dev | T | Sig. |
|---|---|---|---|---|---|---|
| Speech Pathology | No | 361 | 3.83 | 1.005 | 4.055 | 0.000 |
| Yes | 5429 | 3.62 | 0.918 | |||
| Physical Therapy | No | 13 | 3.54 | 1.050 | −0.386 | 0.700 |
| Yes | 5777 | 3.64 | 9.25 | |||
| Medical Social | No | 624 | 3.93 | 0.954 | 8.308 | 0.000 |
| Yes | 5166 | 3.60 | 0.916 | |||
| Home Health Aide | No | 151 | 3.79 | 0.928 | 2.030 | 0.042 |
| Yes | 5639 | 3.63 | 0.925 |
| Top Five States with the Highest Star Ratings | |||||
| State | HCAHPS Summary | Professional Care | Communication with Patient | % Recommend HHA | Quality of Care |
| MS | 4.47 | 4.56 | 4.56 | 85.42 | 3.605 |
| AL | 4.35 | 4.56 | 4.53 | 84.53 | 3.771 |
| LA | 4.34 | 4.55 | 4.47 | 84.26 | 3.31 |
| KY | 4.24 | 4.58 | 4.49 | 84.93 | 3.5 |
| WV | 4.22 | 4.51 | 4.57 | 84.84 | 3.725 |
| Bottom Five States with the Lowest Star Ratings | |||||
| State | HCAHPS Summary | Professional Care | Communication with Patient | % Recommend HHA | Quality of Care |
| AZ | 3.14 | 3.41 | 3.45 | 74.98 | 3.477 |
| CA | 3.11 | 3.24 | 3.34 | 74.21 | 3.57 |
| PR | 3.08 | 3.8 | 3.16 | 78.16 | 3.48 |
| NY | 3.04 | 3.17 | 3.41 | 74.09 | 3.276 |
| NV | 2.98 | 3.25 | 3.02 | 76.38 | 3.328 |
| Proprietary Status | ||||
|---|---|---|---|---|
| Stars | Governmental | Non-Profit | For-Profit | Total |
| 1 | 2 (0.65%) | 9 (0.64%) | 68 (1.67%) | 79 |
| 2 | 1 (0.32%) | 59 (4.21%) | 505 (12.38%) | 565 |
| 3 | 41 (13.31%) | 366 (26.09%) | 1333 (32.68%) | 1740 |
| 4 | 141 (45.78%) | 700 (49.89%) | 1558 (38.2%) | 2399 |
| 5 | 123 (39.94%) | 269 (19.17%) | 615 (15.08%) | 1007 |
| Total | 308 | 1403 | 4079 | 5790 |
| Descriptive Statistics | ||||
| Governm. | Non-Profit | For Profit | ||
| Summary | Mean | 4.24 | 3.83 | 3.53 |
| Std. Dev. | 0.740 | 0.806 | 0.948 | |
| Quality | Mean | 3.15 | 3.38 | 3.36 |
| Std. Dev. | 0.697 | 0.690 | 0.851 | |
| Professionalism | Mean | 4.48 | 4.09 | 3.77 |
| Std. Dev. | 0.719 | 0.856 | 1.059 | |
| Communication | Mean | 4.48 | 4.18 | 3.79 |
| Std. Dev. | 0.746 | 0.835 | 1.029 | |
| % Recommend | Mean | 84.67 | 81.17 | 78.13 |
| Std. Dev. | 6.122 | 6.835 | 8.714 | |
| One Way ANOVA Comparisons | ||||
| Df | F | Sig. | ||
| Summary | Between Groups | 2 | 129.89 | 0.000 |
| Within Groups | 5787 | |||
| Quality | Between Groups | 2 | 10.38 | 0.000 |
| Within Groups | 5744 | |||
| Professionalism | Between Groups | 2 | 113.74 | 0.000 |
| Within Groups | 5787 | |||
| Communication | Between Groups | 2 | 142.69 | 0.000 |
| Within Groups | 5787 | |||
| % Recommend | Between Groups | 2 | 144.69 | 0.000 |
| Within Groups | 5787 | |||
| Variable | (I) | (J) | Mean Diff. (I-J) | Std. Err. | Sig. | 95% C. I | |
|---|---|---|---|---|---|---|---|
| Low Bound | Upper Bound | ||||||
| Summary | 1 | 2 3 | 0.41 0.71 | 0.057 0.053 | 0.000 0.000 | 0.28 0.59 | 0.55 0.84 |
| 2 | 1 3 | −0.41 0.30 | 0.057 0.028 | 0.000 0.000 | −0.55 0.24 | −0.28 0.37 | |
| 3 | 1 2 | 0.41 0.71 | 0.053 0.028 | 0.000 0.000 | −0.84 −0.37 | −0.59 −0.24 | |
| Quality | 1 | 2 3 | −0.22 −0.20 | 0.051 0.048 | 0.000 0.000 | −0.34 −0.32 | −0.10 −0.09 |
| 2 | 1 3 | 0.22 0.021 | 0.051 0.025 | 0.000 0.677 | −0.10 −0.03 | 0.34 0.08 | |
| 3 | 1 2 | 0.20 0.02 | 0.048 0.025 | 0.000 0.677 | 0.09 0.08 | 0.32 0.03 | |
| Professionalism | 1 | 2 3 | 0.38 0.71 | 0.063 0.059 | 0.000 0.000 | 0.24 0.57 | 0.53 0.85 |
| 2 | 1 3 | −0.38 0.32 | 0.063 0.031 | 0.000 0.000 | −0.53 0.25 | −0.24 0.40 | |
| 3 | 1 2 | −0.71 −0.32 | 0.059 0.031 | 0.000 0.000 | −0.85 −0.40 | −0.57 −0.25 | |
| Communication | 1 | 2 3 | 0.30 0.69 | 0.061 0.057 | 0.000 0.000 | 0.16 0.56 | 0.44 0.83 |
| 2 | 1 3 | −0.30 0.39 | 0.061 0.030 | 0.000 0.000 | −0.44 0.33 | −0.16 0.47 | |
| 3 | 1 2 | −0.69 −0.39 | 0.057 0.030 | 0.000 0.000 | −0.83 −0.47 | −0.56 −0.33 | |
| % Recommend | 1 | 2 3 | 3.49 6.53 | 0.514 0.483 | 0.000 0.000 | 2.29 5.40 | 4.70 7.67 |
| 2 | 1 3 | −3.49 3.04 | 0.514 0.253 | 0.000 0.000 | −4.70 2.45 | −2.29 3.64 | |
| 3 | 1 2 | −6.53 −3.04 | 0.483 0.253 | 0.000 0.000 | −7.67 −3.64 | −5.40 −2.45 | |
| Original Star Rating | Adjusted Star Rating | ||
|---|---|---|---|
| Governmental | Non-Profit | For-Profit | |
| 1 | 1 | 1 | 1 |
| 2 | 1 | 1.15 | 1.66 |
| 3 | 1.33 | 2.56 | 2.77 |
| 4 | 3.17 | 3.72 | 3.91 |
| 5 | 5 | 5 | 5 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zikos, D.; DeLellis, N. A Consumer Health Information System to Assist Patients Select Quality Home Health Services. Technologies 2017, 5, 76. https://doi.org/10.3390/technologies5040076
Zikos D, DeLellis N. A Consumer Health Information System to Assist Patients Select Quality Home Health Services. Technologies. 2017; 5(4):76. https://doi.org/10.3390/technologies5040076
Chicago/Turabian StyleZikos, Dimitrios, and Nailya DeLellis. 2017. "A Consumer Health Information System to Assist Patients Select Quality Home Health Services" Technologies 5, no. 4: 76. https://doi.org/10.3390/technologies5040076
APA StyleZikos, D., & DeLellis, N. (2017). A Consumer Health Information System to Assist Patients Select Quality Home Health Services. Technologies, 5(4), 76. https://doi.org/10.3390/technologies5040076