“It Made a Difference to Me”: A Comparative Case Study of Community Pharmacists’ Care Planning Services in Primary Health Care




Abstract
1. Introduction
2. Materials and Methods
2.1. Context
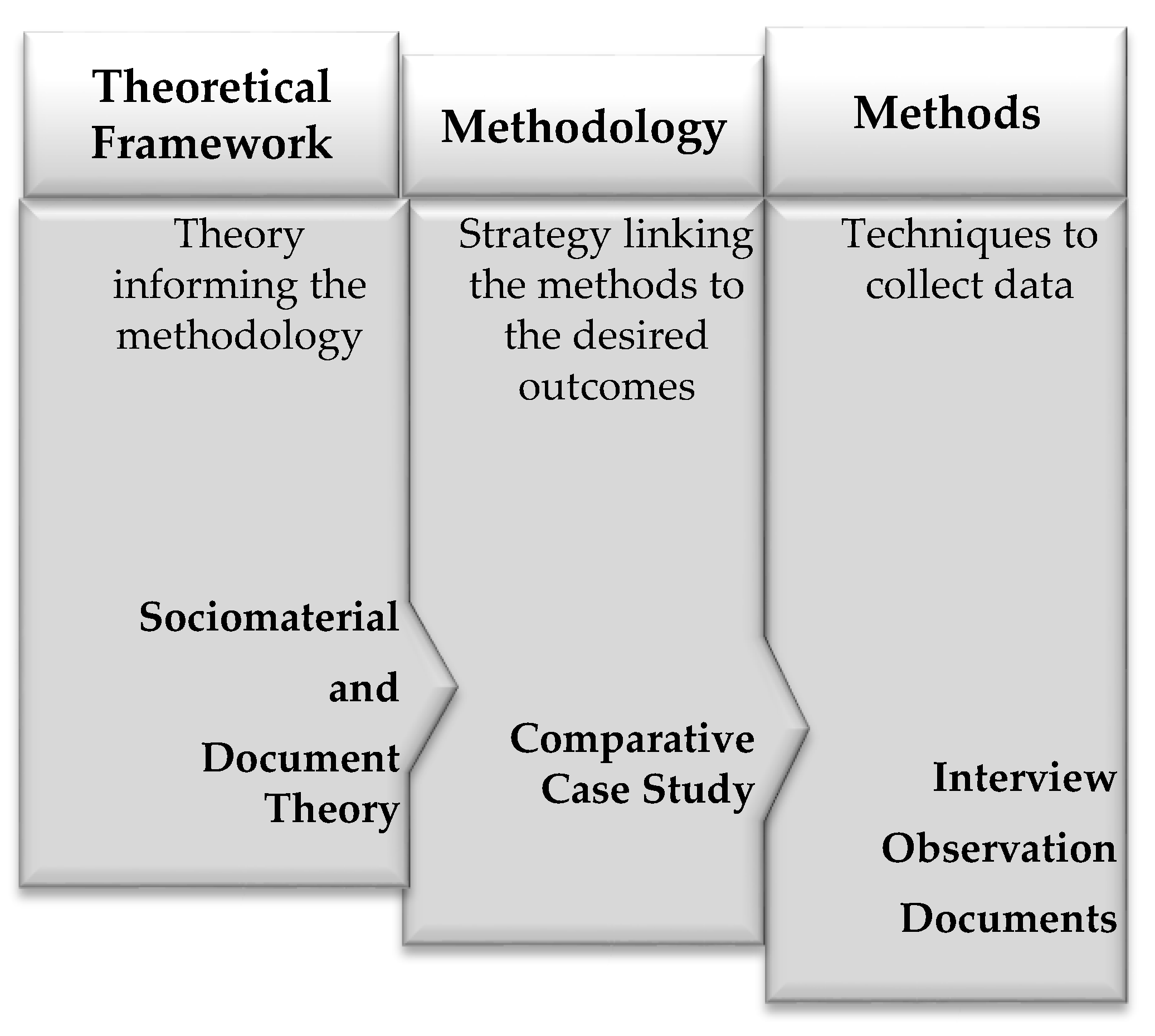
2.2. Theoretical Framework
2.3. Methodology—Comparative Case Study
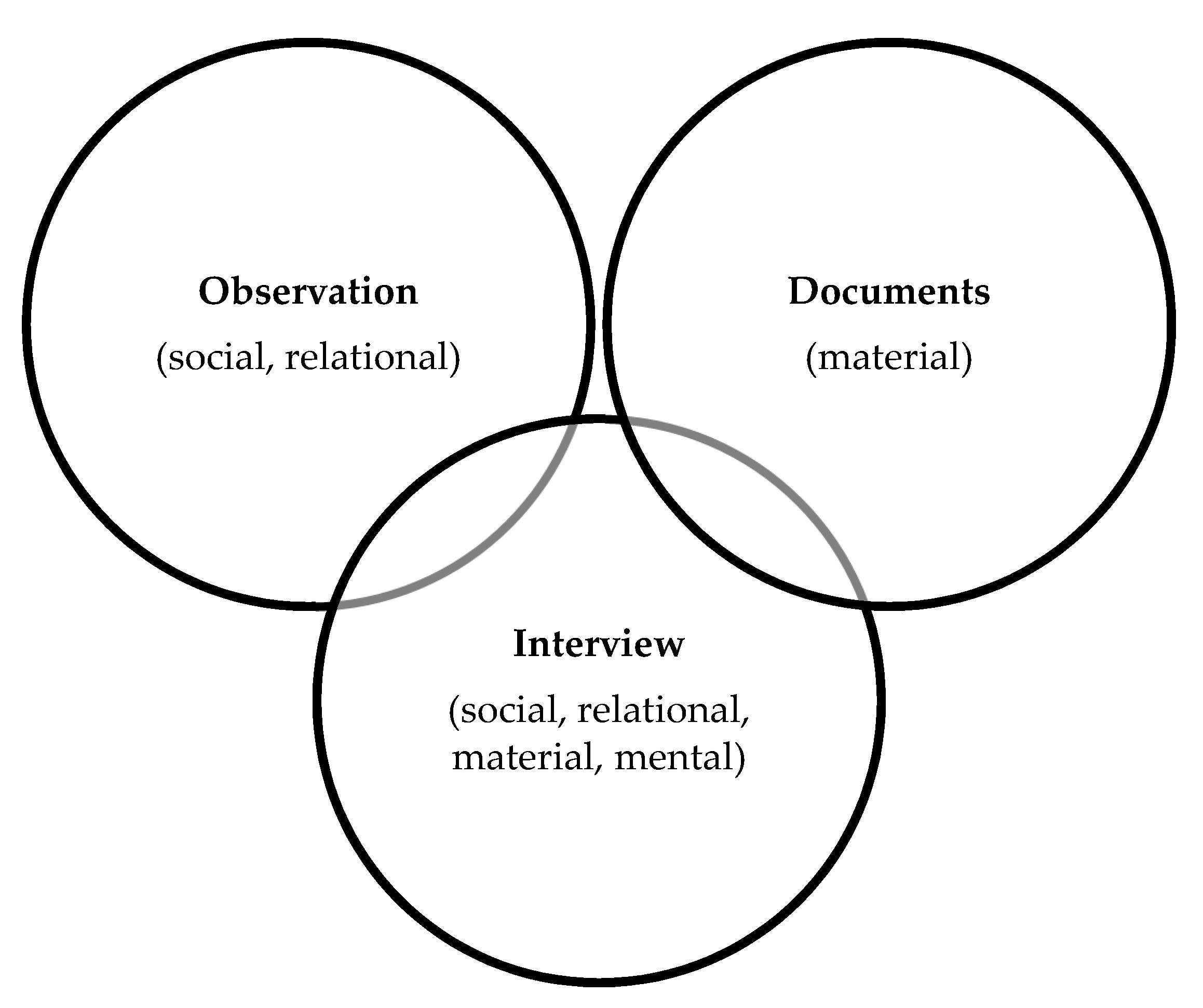
2.4. Methods
2.5. Recruitment
2.6. Data Analysis
2.7. Rigour
2.8. Reflexivity
3. Results
3.1. Sites
3.2. Data Collected
3.3. Value of Care Planning Services
3.3.1. Reinforcing Patient-Centered Care
“I like the structure and deliberateness… [it] is a remarkable way to connect with people and to help them manage their health. It’s been really good that way to make that a deliberate process”(Site 2, Pharmacy Manager)
3.3.2. Reducing Waiting Time for Care
“I waited actually over 15 months to see a specialist… The pharmacist in five minutes told me more than that specialist did, and there was no waiting period.”(Site 3, Patient 1)
3.3.3. Co-Creating Individualized Plans with Patients
“It made a difference to me. I mean, I appreciate it. I appreciate the chance to go over my meds and things that bother me at the time or what we could do about one thing or another.”(Site 1, Patient 4)
3.3.4. Collaborating with Physicians and Other Health Care Providers
”It’s a wonderful adjunct to my practice. It makes my practice better… It makes me think about things in a different way.”(Site 4, Physician 2)
3.3.5. Revealing Possibilities for Pharmacists’ Contributions to Primary Health Care
“I didn’t know that [the pharmacist] would talk to me about it. I thought I would just walk in, get my prescription and walk out, right? That’s the way I thought it was.”(Site 4, Patient 1)
3.3.6. Meaning of Pharmacists’ Roles in Primary Health Care
“I like what I do better, because it feels like I’m contributing more and I know I’m contributing more. And I appreciate being compensated for it. I’ve come to value it more appropriately as well … Now that we do have compensation for some of the clinical skills that we’re using all of the time, it makes it far more satisfying.”(Site 2, Pharmacy Manager)
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Participant | Topics |
|---|---|
| Patient | History with the pharmacy |
| Experiences with care planning (CACP) services | |
| Perceptions and explanations of the value of care planning (CACP) services | |
| Added for site visit 3: Do you talk about your care plan goals? Do you have an action plan after a care plan has been developed for you? | |
| Physician, Other Health Care Professional | History of the practice |
| Experiences with the pharmacy | |
| Experiences with care planning (CACP) services provided by pharmacists | |
| How is the CACP stored? | |
| Perceptions and explanations of the value of care planning (CACP) services | |
| Pharmacist, Pharmacy Technician, and Pharmacy Staff | History with the pharmacy |
| Description of patient care services | |
| Experiences with care planning (CACP) services | |
| Implementation of care planning services | |
| Support provided/required to provide patient care services | |
| Benefits/challenges associated with provision of patient care services | |
| Changes, if any, to the professional role or activities of the pharmacy staff since the implementation of the Compensation Plan for Pharmacy Services | |
| Learning and professional development related to provision of patient care services | |
| Perceptions and explanations of the value of care planning (CACP) services | |
| Added for site visit 3: What information sources do you use for care planning (CACP) services? Do you have access to the medical care plan? What kind of feedback have you received on your care plans? How do you know if the care plan makes a difference? What professional development was helpful? |
| Observational Data—Comprehensive Annual Care Plan (CACP) Services |
|---|
| Observations |
| Pre-CACP activities |
| Pharmacist–staff interactions |
| Patient–staff interactions |
| Patient–pharmacist interactions |
| Patient involvement in CACP development |
| Information seeking and use |
| Documents/forms/tools used |
| “Take away” documentation provided to the patient |
| Physician (or other) communication |
| CACP documentation sharing, storing |
| Post-patient interaction activities |
| Time spent on the activity |
| Clarifications |
| Questions to ask in interviews |
| Description of the setting |
| Location of staff in the setting, including changes over the course of the observation |
| Physical description of the setting |
| Researcher reflexivity |
| What changes to the observation process should be made for the next time? |
| How does the researcher feel about the day’s occurrences? |
| How do the observed actions compare to the findings from the document analysis? Do the key messages found there affect/influence/contradict the observations? |
| Did the researcher(s) have any apparent influence on the activities? |
| Site 1 | Site 2 | Site 3 | Site 4 |
|---|---|---|---|
| Care Plan Template (Example) | Care Plan Template | Care Plan Template | Care Plan Template |
| Initial Assessment with APA Template | Smoking Cessation Template | Smoking Assessment Template | Initial Assessment Template |
| Medication Sheet (Example) | Follow up Progress Notes (Example) | Adult Vaccination Assessment Template | Medication History Template |
| Alberta Health Services | Summary of Care Plan to a physician (Example) | Specific Disease-based Templates | Pharmacy Balance Care Plan Template |
| Care Plan Summary Template | Asthma Action Plan Template | Pharmacy Balance Patient Goal and Plan Template | |
| Continuing Care Template | Letter to a physician (Example) | ||
| Alberta College of Pharmacy Documentation Templates | Pharmacist Prescribing Adaptation (Example) |
| Value | Representative Quotes |
|---|---|
| Reinforcing patient-centered care | |
| The value of it is a connection. The start of the connection. Before, you kind of got a connection with a patient sometimes if you listened to them over the counter and they told you their story … But now it seems like a given if you get the opportunity to sit down in the room with that patient. (Site 1, Pharmacy Manager) | |
| I feel like this… allowed [pharmacists] to prioritize what was important … I feel like I’ve been supported more. (Site 3, Pharmacy Manager) | |
| I like the structure and deliberateness. … [it] is a remarkable way to connect with people and to help them manage their health. It’s been really good that way to make that a deliberate process. (Site 2, Pharmacy Manager) | |
| This whole care plan process has made our pharmacists here do more for the patients. Like, we’re doing more—I’m not saying we weren’t doing the work before, but I feel like this, the whole care plan process has [compelled] us to really make sure that we’re following up with our patients with regards to a lot of medical conditions and medications that they start, you know, whereas we didn’t necessarily do that before. (Site 3, Pharmacy Manager) | |
| We build a relationship … That’s the foundation of my process of care…. So, instead of having my fulfillment come from any sort of outcome, it’s definitely attached to the process. (Site 4, Pharmacist 2) | |
| It’s [making] you close to patients—feel you’re close and patient. They phone and ask for [us] by names … they feel more comfortable talking to me or to [other pharmacists]. And you have more relationship with the patient. (Site 3, Pharmacist 1) | |
| Reducing waiting time for care | |
| I waited actually over 15 months to see a specialist with all my diabetes. The pharmacist in five minutes told me more than that specialist did, and there was no waiting period. (Site 3, Patient 1) | |
| You just felt more comfortable. With the doctor it’s more professional or, like I said, these [pharmacists] feel like family, you know. They’re easier to talk to. (Site 1, Patient 5) | |
| Sometimes you don’t have to go to the doctor’s appointment, you think, because [the pharmacist] helped you figure it out without doing that (Site 1, Patient 1) | |
| The doctor at the pain clinic was very busy all the time and you can’t get in to see him. You have to make an appointment a month or two ahead. And so it was easier for me to come and talk to the pharmacist who was talking back and forth with me at that time. [There was time] for him to sit down and tell me what exactly the situation [was]. (Site 4, Patient 1) | |
| There has been times when I have reacted to a medication, usually an antibiotic, on a weekend where I … was too sick to get to a doctor. And [the pharmacist] would advise me on what to do to get to the point where I could go to a doctor. (Site 2, Patient 5) | |
| [The pharmacist] takes the time to explain stuff to you. So I really appreciate that, because there’s not much of that anymore. (Site 4, Patient 5) | |
| Co-creating individualized plans with patients | |
| It made a difference to me. I mean, I appreciate it. I appreciate the chance, to go over my meds and things that bother me at the time or what we could do about one thing or another. (Site 1, Patient 4) | |
| When I call her regarding something, it’s very important. She always takes some time to listen. (Site 2, Patient 5) | |
| They listen to my concerns. Like, if I have any concerns about my medication somebody always takes the time to answer my questions. (Site 3, Patient 7) | |
| They’re not just your pharmacist, you know. They’re concerned about you too, you know. So that’s a good thing. … rather than just giving you pills like they used to. (Site 1, Patient 5) | |
| Well, my goals are to get my blood sugar down to an acceptable level because I’m Type 2 diabetes, and my blood sugar was way up in the 26 range. And with the help of [named pharmacist] and my family doctor, it is now down roughly about 6. (Site 3, Patient 7) | |
| Before, I abused myself. I didn’t care, right? And now, you know, this [success] is a result of just trying a few healthy things that [the pharmacist] has expressed interest that maybe I should think about doing. [It] has changed my life. Really. (Site 2, Patient 4) | |
| Collaborating with physicians and other health care providers | |
| Before, you had your doctor. Then this. Now it seems like they’re, you know, all connected. So it’s more interaction. Everybody isn’t out in the dark, you know. It seems like it’s better that way now. [Better] than it was before. (Site 1, Patient 5) | |
| It’s a wonderful adjunct to my practice. It makes my practice better… It makes me think about things in a different way. (Site 4, Physician 2) | |
| I know that with both [pharmacist and physician] they have my best interests at heart. They are working together to do the things that I need to have done. In fact, my doctor was saying the other day that the relationship I have with her, and she has with [the pharmacist], allows her to do and follow up on things that she normally wouldn’t have the chance to do. (Site 2, Patient 5) | |
| I talked to my doctor about my pharmacist and they said, “that’s good, we’ll talk back and forth”. It started out with the pharmacist talking with my doctor… back and forth, about my care. (Site 4, Patient 1) | |
| The value of someone’s follow-ups is unbelievable when you have different pharmacists rotating … I’ll even look back and it will be an interaction [with] the other pharmacist had in May … I’m dealing with the problem in September. I’ll understand how that went. (Site 1, Pharmacy Manager) | |
| The piece about talking to people and gathering information from them … to document that properly, really follow that up properly, and share the information properly so that other professionals I work with can be in on the story as well and can be part of that follow-up. (Site 2, Pharmacy Manager) | |
| The physician will outline a care plan for this patient… specific goals for therapy which I can then pull in to my care plans. I’m fortunate to be able to have access to those charts. (Site 4, Pharmacist 5) | |
| [The care plans] gets scanned into our EMR [electronic medical record] so that I can refer back to it at any point and also because we all share the same patients. Information is really important. (Site 1, Physician 2) | |
| We’re starting to get more of their care plans faxed to us. And because they’re doing [care plans, we are] getting more patients coming back to us with questions. And some of that’s very good because it seems we hadn’t realized he’d fallen by the way. And sometimes it’s a little bit of a nuisance because there’s a good reason why this patient isn’t on a statin and now we have to have this conversation all over again. (Site 2, Physician 1) | |
| Revealing possibilities for pharmacists’ contributions to primary health care | |
| I didn’t know that [the pharmacist] would talk to me about it. I thought I would just walk in, get my prescription and walk out, right? That’s the way I thought it was. (Site 4, Patient 1) | |
| Well, it was interesting. I’ve never done that [care plan] before, you know. The ones that give you the prescriptions are the doctors, and it seems like the pharmacy doesn’t know anything about it. But I found that I could get more information from [the pharmacist] than I could from a doctor. (Site 2, Patient 2) | |
| I don’t know if you are aware of this [pharmacist] but he’s a kind of a diabetes specialist … he gets my blood reports… he’s monitoring them …You’ve heard of a secret Santa? He’s kind of a secret doctor, you know. (Site 3, Patient 1) | |
| I think pharmacies are changing… I didn’t know that that [care planning] service was available, to tell you the truth. I always thought that, you know, pharmacists were just there to fill out the prescription, right? I didn’t think they really knew that much about what was going on. (Site 2, Patient 4) | |
| I have more respect for pharmacists now. Let’s be honest about it. I always thought they were just dispensing meds and whatever. (Site 4, Physician 2) | |
| I find that they are, have just become, an extension of my health care colleagues. (Site 4, Nurse Practitioner) | |
| This [care planning service] is a resource in limited situations like [this town]. It’s nice. We know we’re never going to have enough physicians to look after everybody properly like we should. So, it’s nice that the pharmacist can take some of that load. (Site 1, Physician 1) | |
| Meaning of pharmacists’ roles in primary care | |
| I like what I do better, because it feels like I’m contributing more and I know I’m contributing more. And I appreciate being compensated for it. I’ve come to value it more appropriately as well. … Now that we do have compensation for some of the clinical skills that we’re using all of the time, it makes it far more satisfying. (Site 2, Pharmacy Manager) | |
| I feel like even compared to a few years ago … I’ve noticed people depend on [me]—they come in more. They call you for more clinical questions. (Site 1, Pharmacist 2) | |
| It’s just like little light bulbs going off all throughout the day, it’s like I feel so good. I helped that person. I can’t believe what I just did. (Site 1, Pharmacy Manager) | |
| I’m more responsible. I feel more responsible for things than I ever did before. (Site 2, Pharmacy Manager) | |
| Being able to do at least a little bit of tracking [follow-up] to make me feel like I made a difference. (Site 4, Pharmacist 5) | |
| I honestly feel like the system [framework] that’s in place has allowed me to continue to stay more and more current because, you’re just looking at all the clinical stuff on a daily basis instead of just dispensing the medication… I think it definitely increased my knowledge and allowed me to stay a little bit more on top of the changes that occur. (Site 3, Pharmacy Manager) | |
| I have a responsibility to be good and to give [patients] quality and to continue to give good service. So, that kind of holds on you. It’s kind of heavy. (Site 4, Pharmacist 2) |
References
- World Health Organization. Primary Health Care. Available online: https://apps.who.int/iris/bitstream/handle/10665/39228/9241800011.pdf?sequence=1&isAllowed=y (accessed on 21 May 2019).
- Alberta Health. Alberta’s Primary Health Care Strategy. Available online: https://open.alberta.ca/dataset/1cac62b5-a383-4959-8187-1b2a6798d0ac/resource/2ff5246a-bdd9-428a-ab04-62e5475c90ed/download/6849603-2014-albertas-primary-health-care-strategy-2014-01.pdf (accessed on 10 May 2019).
- Haggerty, J.; Burge, F.; Lévesque, J.; Gass, D.; Pineault, R.; Beaulieu, M.; Santor, D. Operational definitions of attributes of primary health care: Consensus among Canadian experts. Ann. Fam. Med. 2007, 5, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Manolakis, P.; Skelton, J. Pharmacists’ contributions to primary care in the United States collaborating to address unmet patient care needs: The emerging role for pharmacists to address the shortage of primary care providers. Am. J. Pharm. Educ. 2010, 74. [Google Scholar] [CrossRef] [PubMed]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Feehan, M.; Walsh, M.; Godin, J.; Sundwall, D.; Munger, M.A. Patient preferences for healthcare delivery through community pharmacy settings in the USA: A discrete choice study. J. Clin. Pharm Ther. 2017, 42, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Policarpo, V.; Romano, S.; António, J.H.C.; Correia, T.S.; Costa, S. A new model for pharmacies? Insights from a quantitative study regarding the public’s perceptions. BMC Health Serv. Res. 2019, 19, 186. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, R.T. The primary care pharmacist. Can. Pharm. J. 2016, 149, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Munger, M.A. Primary care pharmacists: Provision of clinical-decision services in healthcare. Am. J. Pharm. Educ. 2014, 78. [Google Scholar] [CrossRef] [PubMed]
- Romanow, R.L. Building on Values: The Future of Health Care in CANADA. November 2002. Available online: http://publications.gc.ca/collections/Collection/CP32-85-2002E.pdf (accessed on 26 June 2019).
- Grindrod, K.A.; Marra, C.A.; Colley, L.; Tsuyuki, R.T.; Lynd, L.D. Pharmacists’ preferences for providing patient-centered services: A discrete choice experiment to guide health policy. Ann. Pharmacother. 2010, 44, 1554–1564. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.; Bond, C.; Inch, J.; Grant, A. Preferences of community pharmacists for extended roles in primary care: A survey and discrete choice experiment. Pharmacoeconomics 2007, 25, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Fay, A.E.; Ferreri, S.P.; Shepherd, G.; Lundeen, K.; Tong, G.L.; Pfeiffenberger, T. Care team perspectives on community pharmacy enhanced services. J. Am. Pharm. Assoc. 2018, 58, S83–S88. [Google Scholar] [CrossRef] [PubMed]
- Joint Commission of Pharmacy Practitioners. Pharmacists’ Patient Care Process. 29 May 2014. Available online: https://jcpp.net/wp-content/uploads/2016/03/PatientCareProcess-with-supporting-organizations.pdf (accessed on 26 June 2019).
- National Association of Pharmacy Regulatory Authorities. Professional Competencies for Canadian Pharmacists at Entry to Practice. 2014. Available online: https://napra.ca/pharmacists/professional-competencies-canadian-pharmacists-entry-practice-2014 (accessed on 29 June 2019).
- Strand, L.M.; Cipolle, R.J.; Morley, P.C. Documenting the clinical pharmacist’s activities: Back to basics. Drug Intell. Clin. Pharm. 1988, 22, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Drummond, C.; Simpson, A. ‘Who’s actually gonna read this?’ An evaluation of staff experiences of the value of information contained in written care plans in supporting care in three different dementia care settings. J. Psychiatr. Ment. Health Nurs. 2017, 24, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Lawn, S.; Delany, T.; Sweet, L.; Battersby, M.; Skinner, T. Barriers and enablers to good communication and information-sharing practices in care planning for chronic condition management. Aust. J. Prim. Health 2015, 21, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Hindi, A.M.K.; Schafheutle, E.I.; Jacobs, S. Community pharmacy integration within the primary care pathway for people with long-term conditions: A focus group study of patients’, pharmacists’ and GPs’ experiences and expectations. BMC Fam. Pract. 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The Triple Aim: Care, Health and Cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E. What is value in health care? N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef] [PubMed]
- Rollow, W.; Cucchiara, P. Achieving value in primary care: The primary care value model. Ann. Fam. Med. 2016, 14, 159–165. [Google Scholar] [CrossRef][Green Version]
- Nordgren, L. Value creation in health care services—Developing service productivity: Experiences from Sweden. Int. J. Public Sect. Manag. 2009, 22, 114–127. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Sikka, R.; Morath, J.M.; Leape, L. The quadruple aim: Care, health, cost and meaning in work. BMJ Qual. Saf. 2015, 24, 608–610. [Google Scholar] [CrossRef]
- Twigg, M.J.; Wright, D.; Barton, G.; Kirkdale, C.L.; Thornley, T. The pharmacy care plan service: Evaluation and estimate of cost-effectiveness. Res. Soc. Adm. Pharm. 2019, 15, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, E.; Holmes, J.T. Pharmacist-provided services: Barriers to demonstrating value. J. Am. Pharm. Assoc. 2019, 59, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.A.; Guirguis, L.M.; Wong, T.; Ng, K.; Ing, L.; Fisher, K. Influence of pharmacy practice on community pharmacists’ integration of medication and lab value information from electronic health records. J. Am. Pharm. Assoc. 2011, 51, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, N.; Eberhart, G.; Bungard, T.J. Prescribing by pharmacists in Alberta. Am. J. Health-Syst. Pharm. 2008, 65, 2126–2132. [Google Scholar] [CrossRef] [PubMed]
- Charrois, T.; Rosenthal, M.; Tsuyuki, R.T. Stories from the trenches: Experiences of Alberta pharmacists in obtaining additional prescribing authority. Can. Pharm. J. 2012, 145, 30–34. [Google Scholar] [CrossRef]
- Alberta College of Pharmacy. Appendix A: Patient Record Requirements. 2011. Standards of Practice for Pharmacists and Pharmacy Technicians. Available online: https://abpharmacy.ca/sites/default/files/StandardsOfPractice_May2014_v2.pdf (accessed on 29 June 2019).
- Statistics Canada. Population by Year, by Province and Territory. Available online: http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/demo02a-eng.htm (accessed on 21 May 2019).
- Alberta College of Pharmacy. Ripples of Change in the Care of ALBERTANS. 2016-107 Annual Report. Available online: https://abpharmacy.ca/sites/default/files/ACP_AR2016_FinalWeb_0.pdf (accessed on 10 May 2019).
- Guirguis, L.M.; Hughes, C.A.; Makowsky, M.J.; Sadowski, C.A.; Schindel, T.J.; Yuksel, N. Survey of pharmacist prescribing practices in Alberta. Am. J. Health-Syst. Pharm. 2017, 74, 62–69. [Google Scholar] [CrossRef]
- Schindel, T.J.; Yuksel, N.; Breault, R.; Daniels, J.; Varnhagen, S.; Hughes, C.A. Perceptions of pharmacists’ roles in the era of expanding scopes of practice. Res. Soc. Adm. Pharm. 2017, 13, 148–161. [Google Scholar] [CrossRef]
- Breault, R.; Whissell, J.; Hughes, C.A.; Schindel, T.J. Development and implementation of the compensation plan for pharmacy services in Alberta, Canada. J. Am. Pharm. Assoc. 2017, 57, 532–541. [Google Scholar] [CrossRef]
- Breault, R.; Schindel, T.J.; Whissell, J.; Hughes, C.A. Updates to the compensation plan for pharmacy services in Alberta, Canada. J. Am. Pharm. Assoc. 2018, 58, 597–598. [Google Scholar] [CrossRef]
- Gruber, J. Medication therapy management: A challenge for pharmacists. Consult. Pharm. 2012, 11, 782–796. [Google Scholar] [CrossRef]
- Government of Alberta. Compensation Plan for Pharmacy Services. Ministerial Order 614/2018. 2018. Available online: https://open.alberta.ca/dataset/0e5f556a-2ac0-40a6-8fbc-d46fb92b0ee1/resource/a6c00fcd-58db-4b45-b368-df9992111739/download/mo-614-2018-pharmacycompensation.pdf (accessed on 29 June 2019).
- Fenwick, T. Sociomateriality in medical practice and learning: Attuning to what matters. Med. Educ. 2014, 48, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lund, N.W.; Skare, R. Document theory. In Encyclopedia of Library and Information Sciences, 3rd ed.; Bates, M.J., Maack, M.N., Eds.; CRC Press: Boca Raton, FL, USA, 2010; pp. 1632–1639. [Google Scholar]
- Fenwick, T.; Nerland, M.; Jensen, K. Sociomaterial approaches to conceptualising professional learning and practice. J. Educ. Work 2012, 25, 1–13. [Google Scholar] [CrossRef]
- Merriam, S.B. Qualitative case study research. In Qualitative Research: A Guide to Design and Implementation, 3rd ed.; Merriam, S.B., Ed.; Jossey-Bass: Hoboken, NJ, USA, 2014; pp. 39–54. [Google Scholar]
- Yin, R.K. Applications of Case Study Research; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Merriam, S.B. Case Study Research in Education: A Qualitative Approach; Jossey-Bass: San Francisco, CA, USA, 1988. [Google Scholar]
- Hultin, L. On becoming a sociomaterial researcher: Exploring epistemological practices grounded in a relational, performative ontology. Inf. Organ. 2019, 29, 91–104. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; Sage: London, UK, 2006. [Google Scholar]
- Statistics Canada. Population Centre and Rural Area Classification. Available online: https://www.statcan.gc.ca/eng/subjects/standard/pcrac/2016/introduction (accessed on 21 May 2019).
- Kaae, S.; Søndergaard, B.; Haugbølle, L.S.; Traulsen, J.M. Development of a qualitative exploratory case study research method to explore sustained delivery of cognitive services. Pharm. World Sci. 2010, 32, 36. [Google Scholar] [CrossRef] [PubMed]
- Denzin, N.K.; Lincoln, Y.S. Introduction: The discipline and practice of qualitative research. In The Sage Handbook of Qualitative Research, 4th ed.; Denzin, N.K., Lincoln, Y.S., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2011; pp. 1–19. [Google Scholar]
- Given, L.M.; Saumure, K. Trustworthiness. In The SAGE Encyclopedia of Qualitative Research Methods; Given, L.M., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2008; pp. 895–896. [Google Scholar]
- Hughes, C.A.; Breault, R.R.; Hicks, D.; Schindel, T.J. Positioning pharmacists’ roles in primary health care: A discourse analysis of the compensation plan in Alberta, Canada. BMC Health Serv. Res. 2017, 17, 770. [Google Scholar] [CrossRef]
- Perepelkin, J.; Dobson, R.T. Influence of ownership type on role orientation, role affinity, and role conflict among community pharmacy managers and owners in Canada. Res. Soc. Adm. Pharm. 2010, 6, 280–292. [Google Scholar] [CrossRef]
- Brown, S.; Lhussier, M.; Dalkin, S.M.; Eaton, S. Care planning: What works, for whom, and in what circumstances? A rapid realist review. Qual. Health Res. 2018, 28, 2250–2266. [Google Scholar] [CrossRef]
- Council, L.; Geffken, D.; Valeras, A.; Orzano, A.; Rechisky, A.; Anderson, S. A medical home: Changing the way patients and teams relate through patient-centered care plans. Fam. Syst. Health 2012, 30, 90–98. [Google Scholar] [CrossRef]
- Van Dongen, J.J.J.; Van Bokhoven, M.A.; Daniëls, R.; Van Der Weijden, T.; Emonts, W.W.G.P.; Beurskens, A. Developing interprofessional care plans in chronic care: A scoping review. BMC Fam. Pract. 2016, 17. [Google Scholar] [CrossRef]
- Talja, S. Information Sharing in Academic Communities: Types and Levels of Collaboration in Information Seeking and Use. New Rev. Inf. Behav. Res. 2002, 3, 143–160. Available online: https://www.researchgate.net/publication/228999169_Information_sharing_in_academic_communities_Types_and_levels_of_collaboration_in_information_seeking_and_use (accessed on 21 May 2019).
- Latif, A.; Waring, J.; Watmough, D.; Boyd, M.J.; Elliott, R.A. ‘I expected just to walk in, get my tablets and then walk out’: On framing new community pharmacy services in the English healthcare system. Sociol. Health Illn. 2018, 40, 1019–1036. [Google Scholar] [CrossRef] [PubMed]
- Dolovich, L.; Austin, Z.; Waite, N.; Chang, F.; Farrell, B.; Grindrod, K.; Houle, S.; McCarthy, L.; MacCallum, L.; Sproule, B. Pharmacy in the 21st century: Enhancing the impact of the profession of pharmacy on people’s lives in the context of health care trends, evidence and policies. Can. Pharm. J. 2019, 152, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Newbould, J.; Burt, J.; Bower, P.; Blakeman, T.; Kennedy, A.; Rogers, A.; Roland, M. Experiences of care planning in England: Interviews with patients with long term conditions. BMC Fam. Pract. 2012, 13. [Google Scholar] [CrossRef] [PubMed]
- Twigg, M.J.; Wright, D.; Kirkdale, C.L.; Desborough, J.A.; Thornley, T. The UK pharmacy care plan service: Description, recruitment and initial views on a new community pharmacy intervention. PLoS ONE 2017, 12, e0174500. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.S.; Benrimoj, S.I.; Chen, T.F.; Williams, K.A.; Aslani, P. Practice change in community pharmacy: Quantification of facilitators. Ann. Pharmacother. 2008, 42, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hong, S.H.; Meng, S.; Brown, L.M. Pharmacists’ acceptable levels of compensation for MTM services: A conjoint analysis. Res. Soc. Adm. Pharm. 2011, 7, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C.; Cottrell, W.N.; Kyle, G.; Williams, I.; Nissen, L. Integrating a pharmacist into the general practice environment: Opinions of pharmacists, general practitioners, health care consumers, and practice managers. BMC Health Serv. Res. 2012, 12. [Google Scholar] [CrossRef]
- McMillan, S.S.; Wheeler, A.J.; Sav, A.; King, M.A.; Whitty, J.A.; Kendall, E.; Kelly, F. Community pharmacy in Australia: A health hub destination of the future. Res. Soc. Adm. Pharm. 2013, 9, 863–875. [Google Scholar] [CrossRef]
- Tsuyuki, R.T.; Schindel, T.J. Changing pharmacy practice: The leadership challenge. Can. Pharm. J. 2008, 141, 174–180. [Google Scholar] [CrossRef]


| CACP 1 | CACP Follow-up | |
|---|---|---|
| Patient eligibility criteria | Two or more of the following chronic conditions: Hypertension Diabetes Chronic obstructive pulmonary disorder Asthma Heart failure Angina pectoris Ischemic heart disease Mental health disorder OR One of the above conditions plus 1 risk factor: Tobacco Obesity Addiction | CACP must have been completed. CACP Follow-up may be provided if a referral from a physician or hospital admission/discharge within 14 days of the CACP service OR A pharmacist determines that follow-up is needed. |
| Information gathered and recorded | Demographics Allergies and intolerances Health conditions Symptoms or signs to be treated Pregnancy or lactation status Medication use history/review (Best Possible Medication History—BPMH) Other health care products or devices Lifestyle factors—weight, tobacco use, illicit drug use, alcohol use, exercise Laboratory values Care plan—agreed goals of medication therapy, drug therapy problems, identification of possible interventions, plans for monitoring, and follow-up assessment | |
| Fees 2 | $100 3 | $20 4 |
| Description | Site 1 | Site 2 | Site 3 | Site 4 |
|---|---|---|---|---|
| Pharmacy type [53] | Independent | Franchise | Corporate | Independent |
| Population center [48] | Small 1 | Large 2 | Medium 3 | Large 2 |
| Pharmacists (with APA 4, injections authorization) | 3 (3,3) | 3 (1,3) | 3 (1,3) | 5 (4,5) |
| Registered technicians | 1 | - | 1 | 2 |
| Assistants | 3 | 3 | 2 | 6 |
| Pharmacy students | - | Periodically | Regularly | - |
| CACPs 5 completed per month | <20 | <20 | <20 | >100 |
| Data | Site 1 | Site 2 | Site 3 | Site 4 | Total |
|---|---|---|---|---|---|
| Total number of interviews | 27 | 15 | 16 | 19 | 77 |
| Patient | 11 | 5 | 8 | 5 | 29 |
| Physician | 2 | 2 | - | 2 | 6 |
| Nurse | 2 | - | - | 3 | 5 |
| Pharmacy staff | 4 | 4 | 2 | 3 | 13 |
| Pharmacy student | - | - | 2 | - | 2 |
| Pharmacist 1 | 8 | 4 | 4 | 6 | 22 |
| Hours of observation | 24 | 28.5 | 26 | 15.5 2 | 94 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schindel, T.J.; Breault, R.R.; Hughes, C.A. “It Made a Difference to Me”: A Comparative Case Study of Community Pharmacists’ Care Planning Services in Primary Health Care. Pharmacy 2019, 7, 90. https://doi.org/10.3390/pharmacy7030090
Schindel TJ, Breault RR, Hughes CA. “It Made a Difference to Me”: A Comparative Case Study of Community Pharmacists’ Care Planning Services in Primary Health Care. Pharmacy. 2019; 7(3):90. https://doi.org/10.3390/pharmacy7030090
Chicago/Turabian StyleSchindel, Theresa J., Rene R. Breault, and Christine A. Hughes. 2019. "“It Made a Difference to Me”: A Comparative Case Study of Community Pharmacists’ Care Planning Services in Primary Health Care" Pharmacy 7, no. 3: 90. https://doi.org/10.3390/pharmacy7030090
APA StyleSchindel, T. J., Breault, R. R., & Hughes, C. A. (2019). “It Made a Difference to Me”: A Comparative Case Study of Community Pharmacists’ Care Planning Services in Primary Health Care. Pharmacy, 7(3), 90. https://doi.org/10.3390/pharmacy7030090