Aminoglycoside Allergic Reactions


Abstract
1. Introduction
2. Medicinal Chemistry
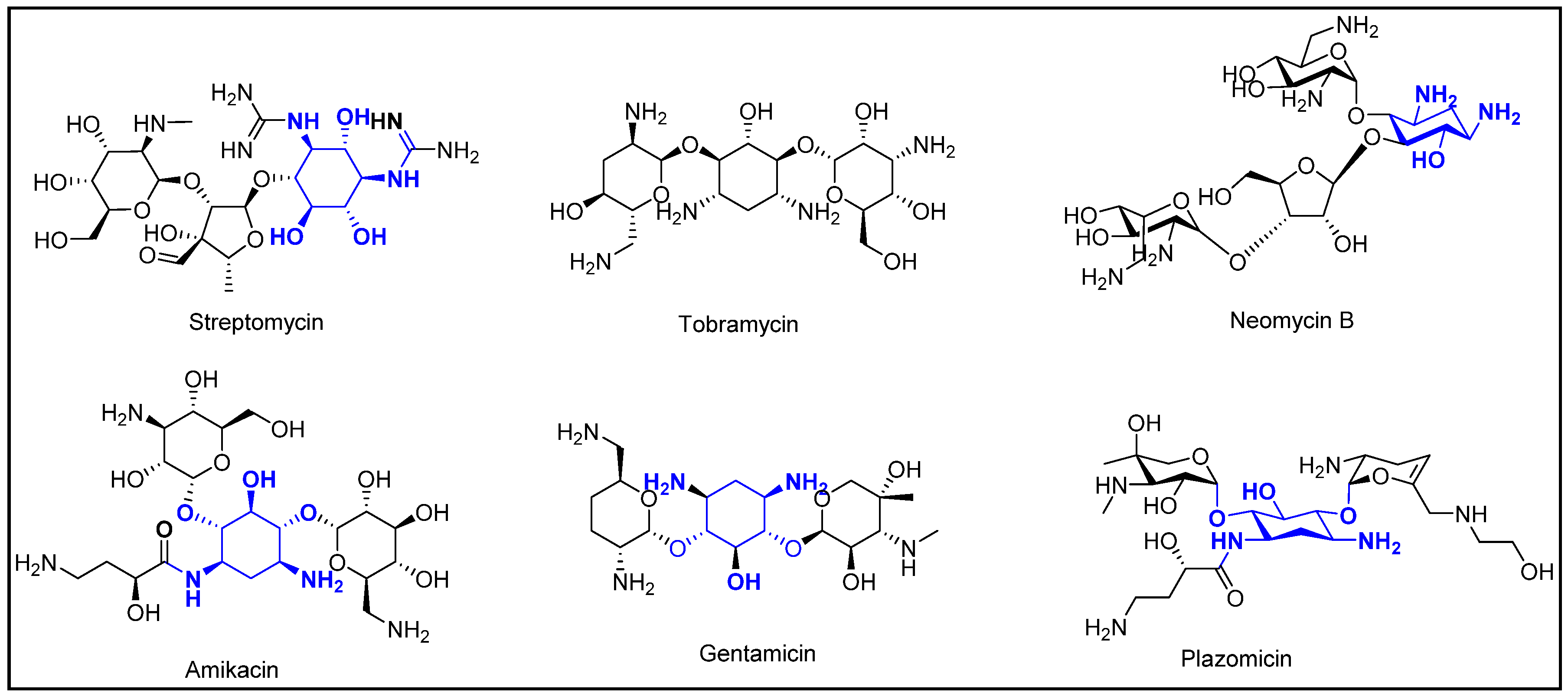
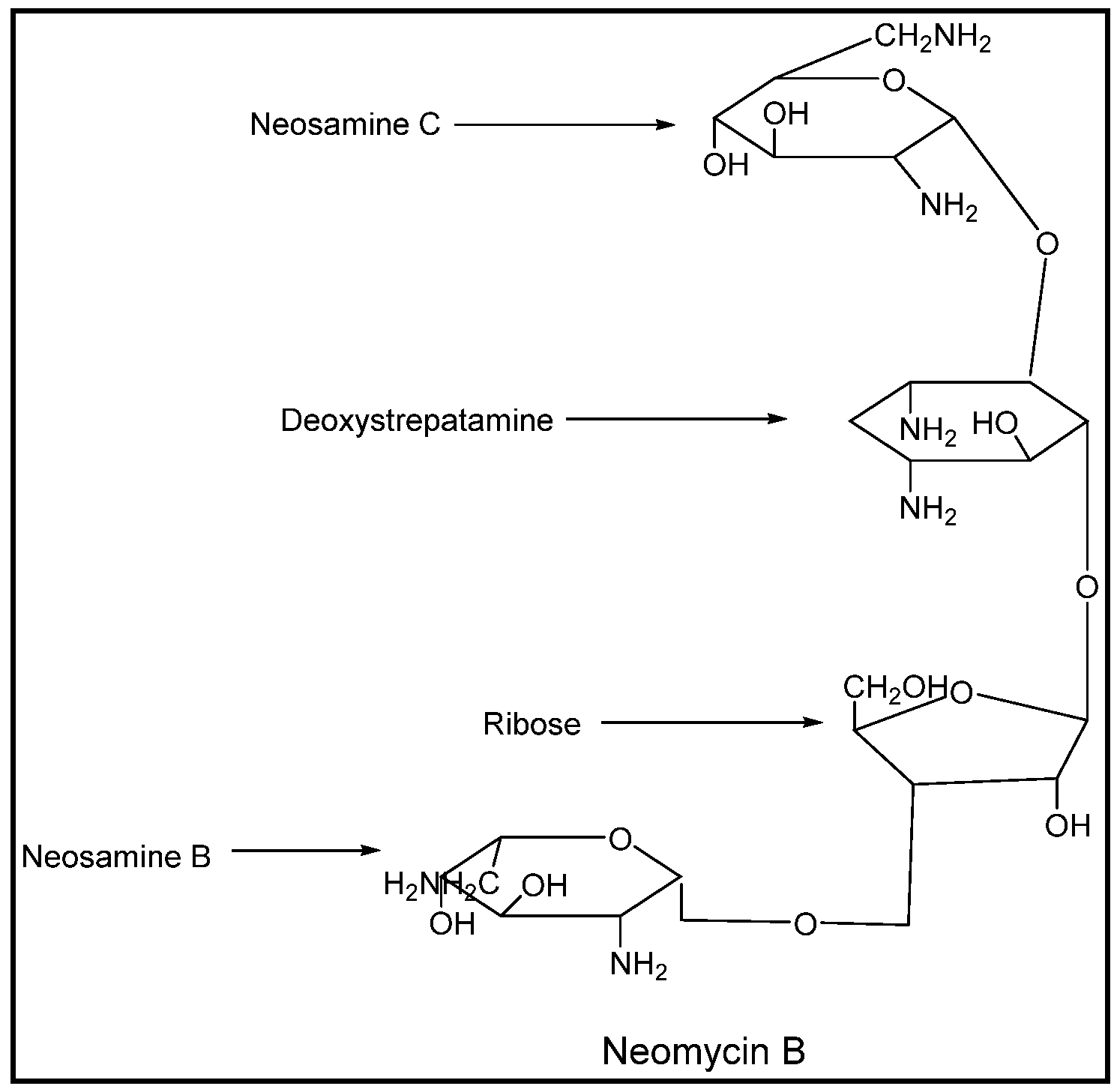
2.1. Aminoglycoside Structure
2.2. Structural Aspects behind Cross-Reactivity
3. Medical Conditions for Which Aminoglycosides Are Used
4. Documented Allergic Reactions
5. Desensitization
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Blumental, K.G.; Peter, J.G.; Trubiano, J.A.; Phillips, E.J. Antibiotic allergy. Lancet 2019, 393, 183–198. [Google Scholar] [CrossRef]
- Sanchez-Borges, M.; Thong, B.; Blanca, M.; Ensina, L.F.C.; González-Díaz, S.; Greenberger, P.A.; Jares, E.; Jee, Y.K.; Kase-Tanno, L.; Khan, D.; et al. Hypersensitivity reaction to non beta-lactam antimicrobial agents, a statement of the WAO special committee on drug allergy. World Allergy Organ. J. 2013, 31, 18. [Google Scholar] [CrossRef] [PubMed]
- dePadua, C.A.; Uter, W.; Schnuch, A. Contact allergy to topical drugs: Prevalence in a clinical setting and estimation of frequency at the population level. Pharmacoepidemiol. Drug Saf. 2007, 16, 377–384. [Google Scholar]
- Macy, E.; Romano, A.; Khan, D. Practical management of antibiotic hypersensitivity in 2017. J. Allergy Clin. Immunol. Pract. 2017, 5, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Serio, A.W.; Keepers, T.; Andrews, L.; Krause, K.M. Aminoglycoside revival: Review of a historically important class of antimicrobials undergoing rejuvenation. EcoSal Plus 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Schorr, W.F.; Ridgway, H.B. Tobramycin-neomycin cross-sensitivity. Contact Dermat. 1977, 3, 133–137. [Google Scholar] [CrossRef]
- Chung, C.W.; Carson, T.R. Cross-sensitivity of common aminoglycoside antibiotics. Arch. Dermatol. 1976, 112, 1101–1107. [Google Scholar] [CrossRef]
- Kimura, M.; Kawada, A. Contact sensitivity induced by neomycin with cross-sensitivity to other aminoglycoside antibiotics. Contact Dermat. 1998, 39, 148–150. [Google Scholar] [CrossRef]
- Romano, A.; Caubet, J.C. Antibiotic allergies in children and adults: From clinical symptoms to skin testing diagnosis. J. Allergy Clin. Immunol. Pract. 2014, 2, 3–12. [Google Scholar] [CrossRef]
- Amikacin Sulfate Injection; Package Insert; Sagent Pharmaceuticals: Schaumburg, IL, USA, 2018.
- Gentamicin Sulfate Injection; Package Insert; Fresenius Kabi: Lake Zurich, IL, USA, 2017.
- Tobramycin Injection; Package Insert; Pfizer: New York, NY, USA, 2011.
- Zemdri (Plazomicin) Injection; Package Insert; Achaogen: South San Francisco, CA, USA, 2018.
- Santos, V.M.; dos Machado, H.S. Antibiotic allergy: A clinical review. J. Allergy Ther. 2017, 8. [Google Scholar] [CrossRef]
- Nesbitt, W.J.; Aronoff, D. Amikacin. In Kucers’ the Use of Antibiotics, 7th ed.; Grayson, M., Ed.; CRC Press: Boca Raton, FL, USA, 2018; Available online: https://online.vitalsource.com (accessed on 22 May 2019).
- Sojo-Dorado, J.; Rodríguez-Baño, J. Gentamicin. In Kucers’ the Use of Antibiotics, 7th ed.; Grayson, M., Ed.; CRC Press: Boca Raton, FL, USA, 2018; Available online: https://online.vitalsource.com (accessed on 22 May 2019).
- Gálvez-Acebal, J.; Rodríguez-Baño, J. Tobramycin. In Kucers’ the Use of Antibiotics, 7th ed.; Grayson, M., Ed.; CRC Press: Boca Raton, FL, USA, 2018; Available online: https://online.vitalsource.com (accessed on 22 May 2019).
- Vidal, L.; Gafter-Gvili, A.; Borok, S.; Fraser, A.; Leibovici, L.; Paul, M. Efficacy and safety of aminoglycoside monotherapy: Systematic review and meta-analysis of randomized controlled trials. J. Antimicrob. Chemother. 2007, 60, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.N.; Leggett, J.E. Aminoglycosides. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; El Sevier Inc.: Philadelphia, PA, USA, 2015. [Google Scholar]
- Tobramycin Inhalation Solution; Package Insert; Akorn, Inc.: Lake Forest, IL, USA, 2016.
- Tobramycin Ophthalmic Solution; Package Insert; Akorn, Inc.: Lake Forest, IL, USA, 2013.
- Tobramycin Ophthalmic Ointment; Package Insert; Alcon a Novartis Company: Puurs, Belgium, 2018.
- Shaeer, K.M.; Zmarlicka, M.T.; Chahine, E.B.; Piccicacco, N.; Cho, J.C. Plazomicin: A next-generation aminoglycoside. Pharmacotherapy 2019, 39, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Gentamicin Sulfate Opthalmic Ointment; Package Insert; Perrigo: Bronx, NY, USA, 2018.
- Gentamicin Sulfate Opthalmic Solution; Package Insert; Bausch & Lomb: Bridgewater, NJ, USA, 2016.
- Gentisone (Gentamicin and Hydrocortisone Acetate) Otic Drops; Package Insert; Advanz Pharma: London, UK, 2017.
- Wininger, D.A.; Fass, R.J. Antibiotic-impregnated cement and beads for orthopedic infections. Antimicrob. Agents Chemother. 1996, 40, 2675–2679. [Google Scholar] [CrossRef] [PubMed]
- Arikayce (Amikacin Liposome Inhalation Suspension); Package Insert; Insmed: Bridgewater, NJ, USA, 2018.
- Micromedex; IBM Watson Health: Greenwood Village, CO, USA, 2019; Available online: https://micromedexsolutions.com (accessed on 25 May 2019).
- Ghadially, R.; Ramsay, C.A. Gentamicin: Systemic exposure to a contact allergen. J. Am. Acad. Dermatol. 1988, 19, 428–430. [Google Scholar] [CrossRef]
- Haeberle, M.; Wittner, B. Is gentamicin-loaded bone cement a risk for developing systemic allergic dermatitis? Contact Dermat. 2009, 60, 176–177. [Google Scholar] [CrossRef] [PubMed]
- Paniagua, M.J.; Garcia-Ortega, P.; Tella, R.; Gaig, P.; Richart, C. Systemic contact dermatitis to gentamicin. Allergy 2002, 57, 1086–1087. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Perez, J.; Lopez, M.P.; De Vega Haro, J.M.; García-Díez, A. Allergic contact dermatitis from gentamicin eye drops, with cross-reactivity to kanamycin, but not neomycin. Contact Dermat. 2001, 44, 54. [Google Scholar] [CrossRef]
- Wittmann, D.; Summer, B.; Thomas, B.; Halder, A.; Thomas, P. Gentamicin allergy as an unexpected ‘hidden’ cause of complications in knee arthroplasty. Contact Dermat. 2018, 78, 293–294. [Google Scholar] [CrossRef]
- Merlob, P.; Metzker, A. Neonatal orbital irritant contact dermatitis caused by gentamicin ointment. Cutis 1996, 57, 429–430. [Google Scholar]
- Muñoz Bellido, F.J.; Moyano, J.C.; Alvarez, M.; Juan, J.L.; Bellido, J. Contact sensitivity to gentamicin with tolerance of systemic exposure. Allergy 1996, 51, 758–759. [Google Scholar] [CrossRef]
- Guin, J.D.; Phillips, D. Erythodema from systemic contact dermatitis: A complication of systemic gentamicin in a patient with contact allergy to neomycin. Cutis 1989, 43, 564–567. [Google Scholar] [PubMed]
- Spigarelli, M.G.; Hurwitz, M.E.; Nasr, S.Z. Hypersensitivity to inhaled Tobi following reaction to gentamicin. Pediatr. Pulmonol. 2002, 33, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Binenbaum, G.; Bruno, C.J.; Forbes, B.J.; Snyder, M.; Mollen, T.J.; Schmidt, B.; Peterside, I. Periocular ulcerative dermatitis associated with gentamicin ointment prophylaxis in newborns. J. Pediatr. 2010, 156, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Earl, H.S.; Sullivan, T.J. Acute desensitization of a patient with cystic fibrosis allergic to both beta-lactam and aminoglycoside antibiotics. J. Allergy Clin. Immunol. 1987, 79, 477–483. [Google Scholar] [CrossRef]
- Ramos, F.M.; Martín, R.L.; Olivo, C.Z.; Dorado Bris, J.M.; Merino Luque, M.V. Allergic contact dermatitis from tobramycin. Contact Dermat. 1990, 22, 305–306. [Google Scholar] [CrossRef]
- Gonzalez-Mendiola, M.R.; Balda, A.G.; Delgado, M.C.; Prieto, P.M.; De Olano, D.G.; Sánchez-Cano, M. Contact allergy from tobramycin eyedrops. Allergy 2005, 60, 527–528. [Google Scholar] [CrossRef] [PubMed]
- Caraffini, S.; Assalve, D.; Stingeni, L.; Lisi, P. Allergic contact conjunctivitis and blepharitis from tobramycin. Contact Dermat. 1995, 32, 186–187. [Google Scholar] [CrossRef]
- Castellazzi, M.L.; Esposito, S.; Claut, L.E.; Daccò, V.; Colombo, C. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome in two young children: The importance of an early diagnosis. Ital. J. Pediatr. 2018, 44, 93. [Google Scholar] [CrossRef]
- Karp, S.; Bakris, G.; Cooney, A.; Rubenstein, D.; Hou, S.H. Exfoliative dermatitis secondary to tobramycin sulfate. Cutis 1991, 47, 331–332. [Google Scholar]
- García-Rubio, I.; Martínez-Cócera, C.; Echarren, T.R.; Cortés, S.V. Fixed exanthema from systemic tobramycin. J. Investig. Allergol. Clin. Immunol. 2006, 16, 264–265. [Google Scholar]
- Whitaker, P.; Shaw, N.; Gooi, J.; Etherington, C.; Conway, S.; Peckham, D. Rapid desensitization for non-immediate reactions in patients with cystic fibrosis. J. Cyst. Fibros. 2011, 10, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, F.; Chapdelaine, H.; Lavoie, A.; Berthiaume, Y.; Sabbah, L.; Bernstein, S.C.; Silviet-Carricart, M. Toxic epidermal necrosis in a patient with cystic fibrosis. J. Allergy Clin. Immunol. Pract. 2016, 4, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Bensaid, B.; Rozières, A.; Nosbaum, A.; Nicolas, J.-F.; Bérard, F. Amikacin-induced drug reactions with eosinophilia and systemic symptoms syndrome: Delayed skin test and ELISPOT assay results allow the identification of the culprit drug. J. Allergy Clin. Immunol. 2012, 130, 1413–1414. [Google Scholar] [CrossRef] [PubMed]
- Hall, F.J. Anaphylaxis after gentamycin. Lancet 1977, 2, 455. [Google Scholar] [CrossRef]
- Schulze, S.; Wollina, U. Gentamicin-induced anaphylaxis. Allergy 2003, 58, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Connolly, M.; McAdoo, J.; Bourke, J.F. Gentamicin-induced anaphylaxis. Ir. J. Med. Sci. 2007, 176, 317–318. [Google Scholar] [CrossRef] [PubMed]
- Henao, C.M.G.; Morales, C.I.H.; Villa, R.C.; Henao, A.M.C. Gentamicin induced anaphylaxis, a case report. World Allergy Organ. J. 2015, 8, A269. [Google Scholar] [CrossRef]
- Christiansen, I.S.; Pedersen, P.; Krøigaard, M.; Mosbech, H.; Garvey, L.H. Anaphylaxis to intravenous gentamicin with suspected sensitization through gentamicin-loaded bone cement. J. Allergy Clin. Immunol. Pract. 2016, 4, 1258–1259. [Google Scholar] [CrossRef]
- Kendigelen, P.; Baktir, M.; Sucu, A.; Kaya, G. Anaphylaxis after administration of amikacin containing sodium metabisulfite in a premature newborn. Arch. Argent. Pediatr. 2016, 114, e195–e198. [Google Scholar]
- Chao, Y.K.; Shyur, S.D.; Wu, C.Y.; Wang, C.Y. Childhood serum sickness: A case report. J. Microbiol. Immunol. Infect. 2001, 34, 220–223. [Google Scholar]
- Ting, J.Y. Ocular tobramycin-induced bronchospasm in an adult without asthma or atopy. Can. J. Ophthalmol. 2007, 42, 883–884. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.P.; Awa, E.; Anbar, R.D. Inhaled tobramycin solution-associated recurrent eosinophilia and severe persistent bronchospasm in a patient with cystic fibrosis: A case report. BMC Pediatr. 2007, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Schretlen-Doherty, J.S.; Troutman, W.G. Tobramycin-induced hypersensitivity reaction. Ann. Pharmacother. 1995, 29, 704–706. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Uses | Aminoglycosides Indicated | Comments |
|---|---|---|
| FDA Approved Uses | ||
| Bacterial meningitis and CNS [10,11,12,29] | AMK, GEN, TOB | |
| Bacterial sepsis [10,11,12,29] | AMK, GEN, TOB | |
| Bone and joint [10,11,12,29] | AMK, GEN, TOB | |
| Burn [11,29] | AMK | |
| Cystic fibrosis-associated respiratory tract infection [10,12,20,29] | AMK, TOB | |
| Intra-abdominal including peritonitis [10,11,12,20,29] | AMK, GEN, TOB | In combination with agent with Gram-positive and anaerobic activity |
| Ocular [21,22,24,25,29] | GEN, TOB | |
| Otic (external) [26] | GEN | |
| Refractory MAC lung disease [28] | ALIS | In combination antibacterial drug regimen with limited or no alternative treatment options |
| Lower respiratory tract (severe) [10,11,12,29] | AMK, GEN, TOB | In combination with beta-lactam, beta-lactam/beta-lactamase inhibitor, or 3rd or 4th generation cephalosporin |
| Skin and soft tissue [10,11,12,29] | AMK, GEN, | |
| Urinary tract (severe, complicated) [10,11,12,13,29] | AMK, GEN, TOB, PLZ | |
| Post-operative [10] | AMK | |
| FDA Unapproved Indications | ||
| Actinomycosis [15] | AMK | |
| Bacterial endocarditis [29] | AMK, GEN | In combination with beta-lactam or vancomycin |
| Brucellosis [16] | GEN | |
| Decontamination of GIT [16] | GEN | |
| Febrile neutropenia (adjunct) [29] | AMK, GEN, TOB | In combination therapy |
| Female genital infection [29] | GEN | |
| Impregnated cement and beads [27] | GEN, TOB | |
| Mycobacteriosis [29] | AMK | In combination therapy |
| Ménière’s disease [16,29] | GEN | |
| Necrotizing enterocolitis in fetus or newborn [29] | GEN | |
| Nocardiosis [29] | AMK | |
| Pelvic inflammatory disease (severe) [29] | GEN | In combination with clindamycin |
| Plague [16,29] | GEN | |
| Surgical prophylaxis [16,29] | GEN, TOB | |
| Tularemia [16,29] | GEN | |
| Uterus (peripartum, postnatal) [29] | GEN | |
| Aminoglycoside Implicated | Reaction | Patient Demographics | Dosage Form | Concomitant Drugs | Patch Test or Rechallenge Confirm Aminoglycoside Allergy? | Sensitization to Previous Dosage Form of Aminoglycoside? |
|---|---|---|---|---|---|---|
| Gentamicin | Allergic Dermatitis [30] | 84-year-old female | Intravenous | None | Yes | Yes, topical |
| Allergic Dermatitis [31] | 74-year-old female | Bone cement | None | Yes | Yes, ongoing bone cement | |
| Allergic Dermatitis [32] | 30-year-old female | Intravenous | Ampicillin, bupivacaine, lidocaine, ketorolac, pethidine, metamizole magnesium | Yes | Yes, topical | |
| Allergic Dermatitis [33] | 55-year-old female | Ophthalmic solution | None | Yes | Yes, ophthalmic | |
| Allergic Dermatitis [34] | 79-year-old | Intra-articular | None | Yes | Yes, ophthalmic | |
| Contact Dermatitis [35] | 5 newborns | Ophthalmic ointment | Unknown | Unknown | Unknown | |
| Contact Sensitivity [36] | 50-year-old male | Ophthalmic solution | None | Yes | Yes, ophthalmic | |
| Exfoliative Erythroderma [37] | 66-year-old male | Intravenous | Ceftozoxime | Yes | Yes, otic | |
| Rash [38] | 9-year-old male | Intravenous | Piperacillin/tazobactam | Unknown | Unknown | |
| Ulcerative Dermatitis [39] | 26 newborns | Ophthalmic ointment | Unknown | Unknown | Unknown | |
| Gentamicin and Tobramycin, different episodes | Urticaria [40] | 15-year-old female | Intravenous | None | Yes | Unknown |
| Tobramycin | Allergic Contact Dermatitis [41] | 32-year-old female | Otic drops | Betamethasone, sulfamethazine | Yes | Unknown |
| Conjunctivitis [42] | 59-year-old female | Ophthalmic suspension | Dexamethasone, atropine, timolol, brominidine, lanatoprost, brinzolamide | Yes | Unknown | |
| Conjunctivitis [43] | 70-year-old female | Ophthalmic ointment | Loxacin, homatropine hydrobromide, tropicamide, phenylephrine, diclofenac | Yes | Unknown | |
| Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) [44] | 4-year-old female | Intravenous | Piperacillin/tazobactam | Unknown | Unknown | |
| Erythroderma, Exfoliative dermatitis [45] | 55-year-old woman | Intravenous, Intraperitoneal | Vancomcyin, clindamycin | Yes | Unknown | |
| Fixed exanthema [46] | 69-year-old female | Intramuscular | None | No | Yes, ophthalmic | |
| Rash [38] | 9-year-old male | Inhaled | Pancre-lipase, ADEK vitamins, rh DNAse, albuterol | Yes | Yes, Intravenous | |
| Rash [47] | 3 patients | Unknown | Unknown | Unknown | Unknown | |
| Toxic epidermal necrosis [48] | 42-year-old male | Intravenous | Meropenem, vancomycin, oseltamivir, ciprofloxacin | Unknown | Unknown | |
| Urticaria [47] | 3 patients | Unknown | Unknown | Unknown | Unknown | |
| Amikacin | DRESS [49] | 42-year-old male | Intravenous | Clindamycin, vancomycin | Yes | Unknown |
| Aminoglycoside Implicated | Reaction | Patient Demographics | Dosage Form | Concomitant Drugs | Patch Test or Rechallenge Confirm Aminoglycoside Allergy? | Sensitization to Previous Dosage Form of Aminoglycoside? |
|---|---|---|---|---|---|---|
| Gentamicin | Anaphylaxis [50] | 66-year-old female | Intravenous | None | Unknown | Unknown |
| Anaphylaxis [51] | 70-year-old female | Intravenous | Cefotiam | Yes | Yes, topical | |
| Anaphylaxis, Urticaria [52] | 69-year-old male | Intravenous | Midazolam | Yes | Unknown | |
| Anaphylaxis [53] | 53-year-old female | Intramuscular | None | Yes | Unknown | |
| Anaphylaxis [54] | 66-year-old female | Intravenous | Chlorhexidine, bupivacaine, dexamethasone, remifentanil, cisatracurium, suxamethonium, propofol | Yes | Yes, bone cement | |
| Amikacin | Anaphylaxis [55] | Newborn male | Intravenous | None | Unknown | Unknown |
| Aminoglycoside Implicated | Reaction | Patient Demographics | Dosage Form | Concomitant Drugs | Patch Test or Rechallenge Confirm Aminoglycoside Allergy? | Sensitization to Previous Dosage Form of Aminoglycoside? |
|---|---|---|---|---|---|---|
| Gentamicin | Serum Sickness [56] | 3-year-old male | Intravenous | Penicillin G, aspirin | Unknown | Unknown |
| Tobramycin | Arthralgia [47] | 1 patient | Unknown | Unknown | Unknown | Unknown |
| Bronchospasm [57] | 79-year-old female | Ophthalmic ointment | Phenylephrine, prednisolone | Unknown | Unknown | |
| Bronchospasm, eosinophilia [58] | 6-year-old male | Inhaled, Intravenous | Unknown | Unknown | Yes, Inhaled | |
| Bronchospasm, urticaria, pruritus [59] | 18-year-old male | Intravenous | Albuterol, cromolyn, DNAase, pancreatic enzymes, phytonadione, multivitamins, ceftazidime | Unknown | Yes, Intravenous | |
| Fever [47] | 1 patient | Unknown | Unknown | Unknown | Unknown |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Childs-Kean, L.M.; Shaeer, K.M.; Varghese Gupta, S.; Cho, J.C. Aminoglycoside Allergic Reactions. Pharmacy 2019, 7, 124. https://doi.org/10.3390/pharmacy7030124
Childs-Kean LM, Shaeer KM, Varghese Gupta S, Cho JC. Aminoglycoside Allergic Reactions. Pharmacy. 2019; 7(3):124. https://doi.org/10.3390/pharmacy7030124
Chicago/Turabian StyleChilds-Kean, Lindsey M., Kristy M. Shaeer, Sheeba Varghese Gupta, and Jonathan C. Cho. 2019. "Aminoglycoside Allergic Reactions" Pharmacy 7, no. 3: 124. https://doi.org/10.3390/pharmacy7030124
APA StyleChilds-Kean, L. M., Shaeer, K. M., Varghese Gupta, S., & Cho, J. C. (2019). Aminoglycoside Allergic Reactions. Pharmacy, 7(3), 124. https://doi.org/10.3390/pharmacy7030124