Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States




Abstract
1. Introduction
1.1. An Overview of Health Care and the Role of Community-Based Pharmacists
1.2. Defining Community-Based Pharmacist Practitioners
1.3. Challenges Facing Community-Based Pharmacist Practitioners in the United States
2. Methods
3. Findings
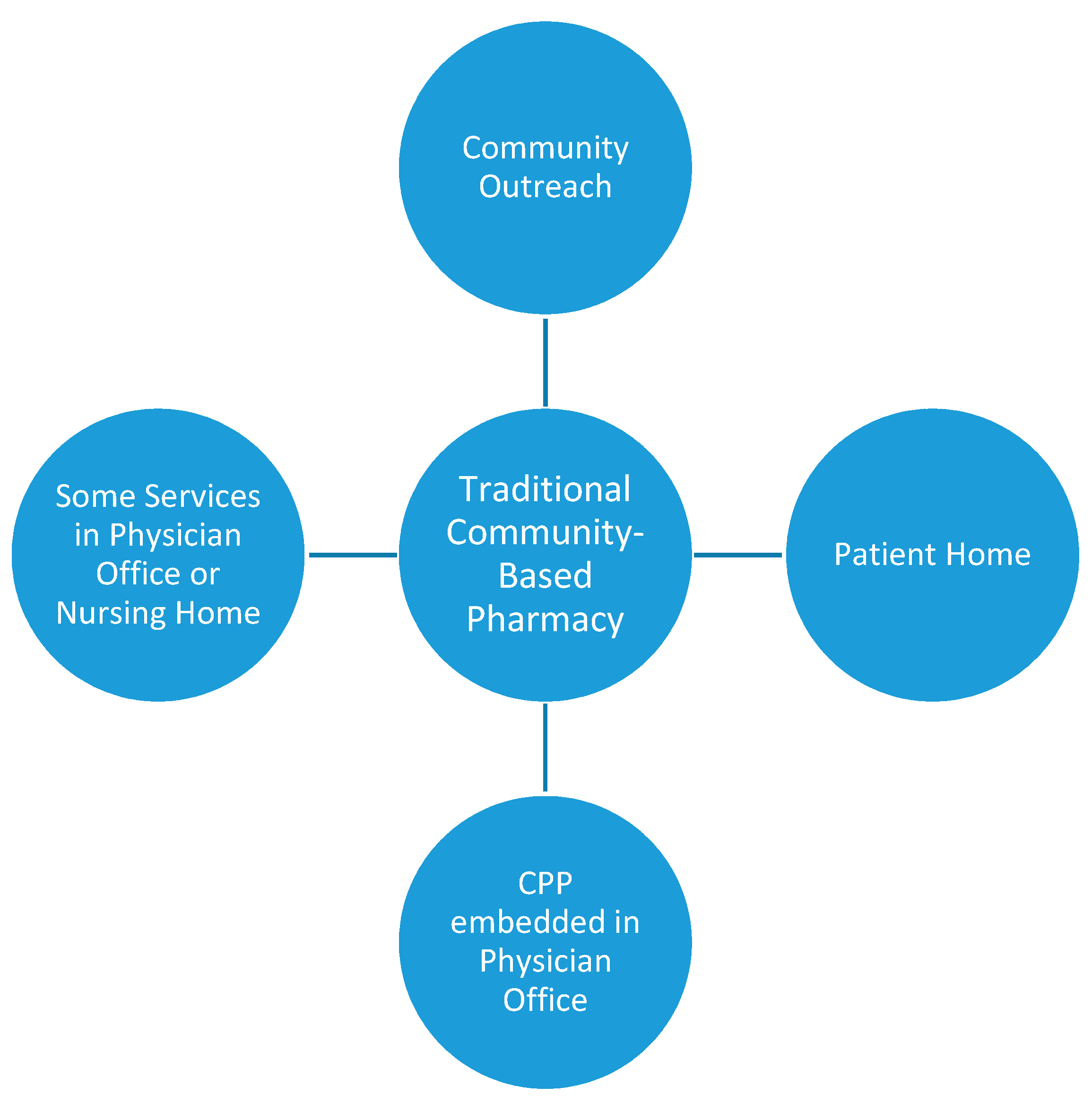
3.1. Models of Community-Based Patient Care Service Delivery
3.2. Community-Based Pharmacy Services
3.2.1. Medication Optimization
3.2.2. Wellness and Prevention
3.2.3. Chronic Care Management
3.2.4. Acute Care Management
3.2.5. Education
3.2.6. Other Services
4. Innovation in the US and Global Impact
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Policarpo, V.; Romano, S.; António, J.H.; Correia, T.S.; Costa, S. A new model for pharmacies? Insights from a quantitative study regarding the public’s perceptions. BMC Health Serv. Res. 2019, 19, 186. [Google Scholar] [CrossRef] [PubMed]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicaid and Medicare Services. National Health Expenditure Projections 2018–2027. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/ForecastSummary.pdf (accessed on 13 April 2019).
- Avalere Health. Exploring Pharmacists’ Role in a Changing Health Care Environment. May 2014. Available online: https://avalere.com/insights/exploring-pharmacists-role-in-a-changing-healthcare-environment (accessed on 26 May 2019).
- American Association of Medical Colleges. Workforce Projections. Available online: https://www.aamc.org/newsroom/newsreleases/458074/2016_workforce_projections_04052016.html (accessed on 25 May 2019).
- United States Bureau of Labor Statistics. Available online: https://www.bls.gov/oes/current/oes291051.htm (accessed on 24 May 2019).
- US Department of Health and Human Services. Reforming America’s Healthcare System through Choice and Competition. Available online: https://www.hhs.gov/sites/default/files/Reforming-Americas-Healthcare-System-Through-Choice-and-Competition.pdf (accessed on 13 April 2019).
- Moose, J.; Branham, A. Pharmacists as Influencers of Patient Adherence. Pharmacy Times. 21 August 2014. Available online: https://www.pharmacytimes.com/publications/directions-in-pharmacy/2014/august2014/pharmacists-as-influencers-of-patient-adherence- (accessed on 13 April 2019).
- Bennett, M.; Goode, J.V. Recognition of community-based pharmacist practitioners: Essential health care providers. J. Am. Pharm. Assoc. 2016, 56, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Erickson, A. Community-Based Pharmacists Extend Care Far Beyond the Pharmacy Walls. Available online: https://www.pharmacytoday.org/article/S1042-0991(16)31227-0/fulltext (accessed on 25 May 2019).
- Beatty, S.J.; Westberg, S.M.; Sharma, A. Professional responsibilities reported by pharmacists completing residencies in community-based settings. J. Am. Pharm. Assoc. 2019, 59, 217–221.e2. [Google Scholar] [CrossRef] [PubMed]
- Andreski, M.; Myers, M.; Gainer, K.; Pudlo, A. The Iowa new practice model: Advancing technician roles to increase pharmacists’ time to provide patient care services. J. Am. Pharm. Assoc. 2018, 58, 268–274.e1. [Google Scholar] [CrossRef] [PubMed]
- Fleagle Miller, R.; Cesarz, J.; Rough, S. Evaluation of community pharmacy tech-check-tech as a strategy for practice advancement. J. Am. Pharm. Assoc. 2018, 58, 652–658. [Google Scholar] [CrossRef]
- Schommer, J.C.; Olson, A.W.; Isetts, B.J. Transforming community-based pharmacy practice through financially sustainable centers for health and personal care. J. Am. Pharm. Assoc. 2019, 59, 306–309. [Google Scholar] [CrossRef]
- McDonough, R. Embracing a New Business Model for Community-Based Pharmacy Practice. Pharmacy Today. Available online: https://www.pharmacytoday.org/article/S1042-0991(17)30604-7/fulltext (accessed on 25 May 2019).
- Hughes, C.A.; Guirguis, L.M.; Wong, T.; Ng, K.; Ing, L.; Fisher, K. Influence of pharmacy practice on community pharmacists’ integration of medication and lab value information from electronic health records. J. Am. Pharm. Assoc. 2011, 51, 591–598. [Google Scholar] [CrossRef]
- Faiella, A.; Casper, K.A.; Bible, L.; Seifert, J. Implementation and use of an electronic health record in a charitable community pharmacy. J. Am. Pharm. Assoc. 2019, 59, S110–S117. [Google Scholar] [CrossRef]
- Pharmacist ECare Plan Initiative. Available online: https://www.ecareplaninitiative.com/ (accessed on 26 May 2019).
- Nguyen, E.; Holmes, J.T. Pharmacist-provided services: Barriers to demonstrating value. J. Am. Pharm. Assoc. 2019, 59, 117–120. [Google Scholar] [CrossRef]
- Schindel, T.J.; Yuksel, N.; Breault, R.; Daniels, J.; Varnhagen, S.; Hughes, C.A. Perceptions of pharmacists’ roles in the era of expanding scopes of practice. Res. Soc. Adm. Pharm. 2017, 13, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.J.; Weaver, K.K. The continuum of pharmacist prescriptive authority. Ann. Pharmacother. 2016, 50, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Catizone, C.; Maine, L.; Menighan, T. Charting Accreditation’s Future: Continuing our collaboration to create practice-ready, team oriented patient care pharmacists. Am. J. Pharm. Educ. 2013, 77, 43. [Google Scholar] [CrossRef] [PubMed]
- Feehan, M.; Walsh, M.; Godin, J.; Sundwall, D.; Munger, M.A. Patient preferences for healthcare delivery through community pharmacy settings in the USA: A discrete choice study. J. Clin. Pharm. Ther. 2017, 42, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Easter, J.C.; DeWalt, D.A. The medication optimization value proposition aligning teams and education to improve care. NCMJ 2017, 3, 168–172. [Google Scholar] [CrossRef]
- Nguyen, E.; Sobieraj, D. The impact of appointment based medication synchronization on medication taking behaviour and health outcomes: A systematic review. J. Clin. Pharm. Ther. 2017, 42, 404–413. [Google Scholar] [CrossRef]
- Holdford, D.A.; Inocencio, T.J. Adherence and persistence associated with an appointment-based medication synchronization program. J. Am. Pharm. Assoc. 2013, 53, 576–583. [Google Scholar] [CrossRef]
- Kadia, N.K.; Schroeder, M.N. Community pharmacy-based adherence programs and the role of the pharmacy technician: A review. J. Pharm. Technol. 2015, 31, 51–57. [Google Scholar] [CrossRef]
- Mooney, E.V.; Hamper, J.G.; Willis, R.T.; Farinha, T.L.; Ricchetti, C.A. Evaluating patient satisfaction with pharmacist-administered long-acting injectable antipsychotics in a community pharmacy. J. Am. Pharm. Assoc. 2018, 58, S24–S29.e2. [Google Scholar] [CrossRef]
- McNab, D.; Bowie, P.; Ross, A.; MacWalter, G.; Ryan, M.; Morrison, J. Systematic review and meta-analysis of the effectiveness of pharmacist-led medication reconciliation in the community after hospital discharge. BMJ Qual. Saf. 2018, 27, 308–320. [Google Scholar] [CrossRef]
- Mueller, S.; Sponsler, K.; Kripalani, S.; Schnipper, J. Hospital-based medication reconciliation practices: A systematic review. Arch. Int. Med. 2012, 172, 1057–1069. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services. Hospital Readmissions Reduction Program. Available online: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/value-based-programs/hrrp/hospital-readmission-reduction-program.html (accessed on 26 May 2019).
- Kilcup, M.; Schultz, D.; Carlson, J.; Wilson, B. Postdischarge pharmacist medication reconciliation: Impact on readmission rates and financial savings. J. Am. Pharm. Assoc. 2013, 53, 78–84. [Google Scholar] [CrossRef]
- Ravn-Nielsen, L.V.; Duckert, M.L.; Lund, M.L.; Henriksen, J.P.; Nielsen, M.L.; Eriksen, C.S.; Buck, T.C.; Pottegard, A.; Hansen, M.R.; Hallas, J. Effect of an in-hospital multifaceted clinical pharmacist intervention on the risk of readmission: A randomized clinical trial. JAMA Int. Med. 2018, 178, 375–382. [Google Scholar] [CrossRef]
- Foster, A.; Gatewood, S.; Kaefer, T.; Goode, J. Decision-maker and staff perceptions of the pharmacist’s role in transitions of care programs. J. Am. Pharm. Assoc. 2019, 59, S101–S105. [Google Scholar] [CrossRef]
- Paul, S.; DiDonato, K.L.; Liu, Y. Rural health systems’ perceptions of referral to community pharmacists during transitions of care. J. Am. Pharm. Assoc. 2016, 56, 562–567. [Google Scholar] [CrossRef]
- Joint Commission of Pharmacy Practitioners. Medication Management Services (MMS) Definition and Key Points. 14 March 2018. Available online: https://jcpp.net/wp-content/uploads/2018/05/Medication-Management- Services-Definition-and-Key-Points-Version-1.pdf (accessed on 31 May 2019).
- Patient-Centered Primary Collaborative. The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes. June 2012. Available online: https://www.pcpcc.org/sites/default/files/media/medmanagement.pdf (accessed on 26 May 2019).
- Viswanathan, M.; Kahwati, L.C.; Golin, C.E.; Blalock, S.; Coker-Schwimmer, E.; Posey, R.; Lohr, K.N. Medication therapy management interventions in outpatient settings. JAMA Int. Med. 2015, 175, 76–87. [Google Scholar] [CrossRef]
- Isetts, B.J.; Schondelmeyer, S.W.; Artz, M.B.; Lenarz, L.A.; Heaton, A.H.; Wadd, W.B.; Brown, L.M.; Cipolle, R.J. Clinical and economic outcomes of medication therapy management services: The Minnesota experience. J. Am. Pharm. Assoc. 2008, 48, 203–211. [Google Scholar] [CrossRef]
- Doucette, W.R.; McDonough, R.P.; Klepser, D.; McCarthy, R. Comprehensive medication therapy management: Identifying and resolving drug-related issues in a community pharmacy. Clin. Ther. 2005, 27, 1104–1111. [Google Scholar] [CrossRef]
- Kehrer, J.; James, D. The Role of Pharmacists and Pharmacy Education in Point-of-Care Testing. Am. J. Pharm. Educ. 2016, 80, 129. [Google Scholar]
- Buss, V.H.; Naunton, M. Analytical quality and effectiveness of point of care testing in community pharmacies: A systematic literature review. Res. Soc. Adm. Pharm. 2019, 15, 483–495. [Google Scholar] [CrossRef]
- Klepser, M.E.; Adams, A.J.; Srnis, P.; Mazzucco, M.; Klepser, D. U.S. community pharmacies as CLIA-waived facilities: Prevalence, dispersion, and impact on patient access to testing. Res. Soc. Adm. Pharm. 2016, 12, 614–621. [Google Scholar] [CrossRef]
- Gubbins, P.O.; Klepser, M.E.; Dering-Anderson, A.M.; Bauer, K.A.; Darin, K.M.; Klepser, S.; Matthias, K.R.; Scarsi, K. Point-of-care testing for infectious disease: Opportunities, barriers, and considerations in community pharmacy. J. Am. Pharm. Assoc. 2014, 54, 163–171. [Google Scholar] [CrossRef]
- Weidle, P.J.; Lecher, S.; Botts, L.W.; Jones, L.; Spach, D.H.; Alvarez, J.; Jones, R.; Thomas, V. HIV testing in community pharmacies and retail clinics: A model to expand access to screening for HIV infection. J. Am. Pharm. Assoc. 2014, 54, 486–492. [Google Scholar] [CrossRef]
- Haga, S.B.; Moaddeb, J.; Mills, R.; Voora, D. Assessing feasibility of delivering pharmacogenetic testing in a community pharmacy setting. Pharmacogenomics 2017, 18, 327–335. [Google Scholar] [CrossRef]
- Hogue, M.D.; Grabenstein, J.D.; Foster, S.L.; Rothholz, M.C. Pharmacist involvement with immunizations: A decade of professional advancement. J. Am. Pharm. Assoc. 2006, 46, 168–179. [Google Scholar] [CrossRef]
- Isenor, J.E.; Edwards, N.T.; Alia, T.A.; Slaytor, K.L.; MacDougall, D.M.; McNeil, S.A.; Bowles, S.K. Impact of pharmacists as immunizers on vaccination rates: A systematic review and meta-analysis. Vaccine 2016, 34, 5708–5723. [Google Scholar] [CrossRef]
- Baroy, J.; Chung, D.; Frisch, R.; Apgar, D.; Slack, M.K. The impact of pharmacist immunization programs on adult immunization rates: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 2016, 56, 418–426. [Google Scholar] [CrossRef]
- Gatewood, S.B.S.; Stanley, D.D.; Goode, J.R. Implementation of a Pre-Travel Health Clinic in a Supermarket Pharmacy. J. Am. Pharm. Assoc. 2009, 49, 110–119. [Google Scholar] [CrossRef]
- Hurley-Kim, K.; Goad, J.; Seed, S.; Hess, K.M. Pharmacy-Based Travel Health Services in the United States. Pharmacy 2018, 7, 5. [Google Scholar] [CrossRef]
- Hess, K.M.; Dai, C.W.; Garner, B.; Law, A.V. Measuring outcomes of a pharmacist-run travel health clinic located in an independent community pharmacy. J. Am. Pharm. Assoc. 2010, 50, 174–180. [Google Scholar] [CrossRef]
- Tran, D.; Gatewood, S.; Moczygemba, L.R.; Stanley, D.D.; Goode, J.V. Evaluating health outcomes following a pharmacist-provided comprehensive pretravel health clinic in a supermarket pharmacy. J. Am. Pharm. Assoc. 2015, 55, 143–152. [Google Scholar] [CrossRef]
- Patwardhan, P.D.; Chewning, B.A. Tobacco users’ perceptions of a brief tobacco cessation intervention in community pharmacies. J. Am. Pharm. Assoc. 2010, 50, 568–574. [Google Scholar] [CrossRef]
- National Alliance of State Pharmacy Associations. Pharmacists Prescribing for Tobacco Cessation Medications. Available online: https://naspa.us/resource/tobacco-cessation/ (accessed on 26 May 2019).
- National Alliance of State Pharmacy Associations. Pharmacists Authorized to Prescribe Birth Control in More States. Available online: https://naspa.us/2017/05/pharmacists-authorized-prescribe-birth-control-states/ (accessed on 26 May 2019).
- Abouk, R.; Pacula, R.L.; Powell, D. Association between state laws facilitating pharmacy distribution of naloxone and risk of fatal overdose. JAMA Int. Med. 2019, 179, 805–811. [Google Scholar] [CrossRef]
- Rosenthal, M.; Ward, L.M.; Teng, J.; Haines, S. Weight management counseling among community pharmacists: A scoping review. Int. J. Pharm. Pract. 2018, 26, 475–484. [Google Scholar] [CrossRef]
- Mott, D.A.; Martin, B.; Breslow, R.; Michaels, B.; Kirchner, J.; Mahoney, J.; Margolis, A. The Development of a Community-Based, Pharmacist-Provided Falls Prevention MTM Intervention for Older Adults: Relationship Building, Methods, and Rationale. Innov. Pharm. 2014, 5, 140. [Google Scholar] [CrossRef]
- Ferreri, S.P.; Greco, A.J.; Michaels, N.M.; O’Connor, S.K.; Chater, R.W.; Viera, A.J.; Faruki, H.; McLeod, H.L.; Roederer, M.W. Implementation of a pharmacogenomics service in a community pharmacy. J. Am. Pharm. Assoc. 2014, 54, 172–180. [Google Scholar] [CrossRef]
- Nacopoulos, A.G.; Lewtas, A.J.; Ousterhout, N.M. Syringe exchange programs: Impact on injection drug users and the role of the pharmacist from a U.S. perspective. J. Am. Pharm. Assoc. 2010, 50, 148–157. [Google Scholar] [CrossRef]
- Lystlund, S.; Stevens, E.; Planas, L.G.; Marcy, T.R. Patient participation in a clinic-based community pharmacy medication take-back program. J. Am. Pharm. Assoc. 2014, 54, 280–284. [Google Scholar] [CrossRef]
- Shepard, J.E.; Bopp, J. Pharmacy-based care for perimenopausal and postmenopausal women. J. Am. Pharm. Assoc. 2002, 42, 700–711. [Google Scholar]
- Evans, T.A.; Fable, P.H.; Ziegler, B. Community-pharmacist delivered Medicare Annual Wellness Visits within a family medicine practice. J. Am. Pharm. Assoc. 2017, 57, S247–S251. [Google Scholar] [CrossRef]
- Department of Health and Human Services. Centers for Medicare & Medicaid Services. Chronic Care Management Service. Available online: www.cms.gov/outreach-and-education/medicare-learning-networkmln/mlnproducts/downloads/chroniccaremanagement.pdf (accessed on 24 May 2019).
- American Pharmacists Association. Chronic Care Management (CCM): An Overview for Pharmacists. Available online: www.pharmacist.com/sites/default/files/CCM-An-Overview-forPharmacists-FINAL.pdf (accessed on 23 May 2019).
- Taylor, A.M.; Bingham, J.; Schussel, K.; Axon, D.R.; Dickman, D.J.; Boesen, K.; Martin, R.; Warholak, T.L. Integrating innovative telehealth solutions into an interprofessional team-delivered chronic care management pilot program. J. Manag. Care Spec. Pharm. 2018, 24, 813–818. [Google Scholar] [CrossRef]
- Johnson, M.; Jastrzab, R.; Tate, J.; Johnson, K.; Hall-Lipsy, E.; Martin, R.; Taylor, A.M.; Warholak, T. Evaluation of an academic-community partnership to implement MTM services in rural communities to improve pharmaceutical care for patients with diabetes and/or hypertension. J. Manag. Care Spec. Pharm. 2018, 24, 132–141. [Google Scholar] [CrossRef]
- Armour, C.L.; Smith, L.; Krass, I. Community pharmacy, disease state management, and adherence to medication. Dis. Manag. Health Outcomes 2008, 16, 245–254. [Google Scholar] [CrossRef]
- Victor, R.G.; Lynch, K.; Blyler, C.; Muhammed, E.; Handler, J.; Brettler, J.; Rashid, M.; Hsu, B.; Fox-Drew, D.; Moy, N.; et al. A cluster-randomized trial of blood-pressure reduction in black barbershops. N. Engl. J. Med. 2018, 378, 1291–1301. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance Fact Sheet. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 7 May 2019).
- Essack, S.; Bell, J.; Shepard, A. Community pharmacists—leaders for antibiotic stewardship in respiratory tract infection. J. Clin. Pharm. Ther. 2018, 43, 302–307. [Google Scholar] [CrossRef]
- Gubbins, P.O.; Klepser, M.E.; Adam, A.J.; Jacobs, D.M.; Percival, K.M.; Tallman, G.B. Potential for pharmacy-public health collaborations using pharmacy-based point-of-care testing services for infectious disease. J. Public Health Manag. Pract. 2017, 23, 593–600. [Google Scholar] [CrossRef]
- Weber, N.C.; Klepser, M.E.; Akers, J.M.; Klepser, D.G.; Adams, A.J. Use of CLIA-waived point-of-care tests for infectious diseases in community pharmacies in the United States. Expert Rev. Mol. Diagn. 2016, 16, 253–264. [Google Scholar] [CrossRef]
- Klepser, D.G.; Corn, C.E.; Schmidt, M.; Dering-Anderson, A.M.; Klepser, M.E. Health care resource utilization and costs for influenza-like illness among Midwestern health plan members. J. Manag. Care Spec. Pharm. 2015, 21, 568–573. [Google Scholar] [CrossRef]
- Klepser, M.E.; Klepser, D.G.; Dering-Anderson, A.M.; Morse, J.A.; Smith, J.K.; Klepser, S.A. Effectiveness of a pharmacist-physician collaborative program to manage influenza-like illness. J. Am. Pharm. Assoc. 2016, 56, 14–21. [Google Scholar] [CrossRef]
- Klepser, M.E.; Hagerman, J.K.; Klepser, S.A.; Bergman, S.J.; Klepser, D.G. A community pharmacy-based influenza screening and management program shortens time to treatment versus pharmacy screening with referral to standard of care. Ill. Pharm. 2014, 76, 12–18. [Google Scholar]
- Klepser, D.G.; Klepser, M.E.; Dering-Anderson, A.M.; Morse, J.A.; Smith, J.K.; Klepser, S.A. Community pharmacist-physician collaborative streptococcal pharyngitis management program. J. Am. Pharm. Assoc. 2016, 56, 323–329. [Google Scholar] [CrossRef]
- Klepser, D.G.; Klepser, M.E.; Smith, J.K.; Dering-Anderson, A.M.; Nelson, M.; Pohren, L.E. Utilization of influenza and streptococcal pharyngitis point-of-care testing in the community pharmacy practice setting. Res. Soc. Adm. Pharm. 2018, 14, 356–359. [Google Scholar] [CrossRef]
- Klepser, D.G.; Bisanz, S.E.; Klepser, M.E. Cost-Effectiveness of pharmacist-provided treatment of adult pharyngitis. Am. J. Manag. Care 2012, 4, e145–e154. [Google Scholar]
- Idaho Pharmacists can Prescribe more than 20 Categories of Medications. Pharmacy Today 2018. Available online: https://www.pharmacytoday.org/article/S1042-0991(18)31417-8/pdf (accessed on 26 May 2019).
- Beahm, N.P.; Smyth, D.J.; Tsuyuki, R.T. Outcomes of urinary tract infection management by pharmacists (RxOUTMAP): A study of pharmacist prescribing and care in patients with uncomplicated urinary tract infections in the community. Can. Pharm. J. 2018, 15, 305–314. [Google Scholar] [CrossRef]
- Booth, J.L.; Mullen, A.B.; Thomson, D.A.; Johnstone, C.; Galbraith, S.J.; Bryson, S.M.; McGovern, E.M. Antibiotic treatment of urinary tract infection by community pharmacists: A cross-sectional study. Br. J. Gen. Pract. 2013, 63, e244–e249. [Google Scholar] [CrossRef]
- DiDonato, K.L.; May, J.R.; Lindsey, C.C. Impact of wellness coaching and monitoring services provided in a community pharmacy. J. Am. Pharm. Assoc. 2013, 53, 14–21. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Rx for the National Diabetes Prevention Program: Action Guide for Community Pharmacists. Centers for Disease Control and Prevention, US Dept of Health and Human Services: Atlanta, GA, USA, 2018. Available online: https://www.cdc.gov/diabetes/prevention/pdf/pharmacists-guide.pdf (accessed on 14 May 2019).
- Ragucci, K.R.; Fermo, J.D.; Wessell, A.M.; Chumney, E.C. Effectiveness of pharmacist-administered diabetes mellitus education and management services. Pharmacotherapy 2005, 25, 1809–1816. [Google Scholar] [CrossRef]
- Luder, H.R.; Frede, S.M.; Kirby, J.A.; Epplen, K.; Cavanaugh, T.; Martin-Boone, J.E.; Conrad, W.F.; Kuhlmann, D.; Heaton, P.C. TransitionRx: Impact of community pharmacy postdischarge medication therapy management on hospital readmission rate. J. Am. Pharm. Assoc. 2015, 55, 246–254. [Google Scholar] [CrossRef]
- Ni, W.; Colayco, D.; Hasimoto, J.; Komoto, K.; Gowda, C.; Wearda, B.; McCombs, J. Impact of a pharmacy-based transitional care program on hospital readmissions. Am. J. Manag. Care 2017, 23, 170–176. [Google Scholar]
- Garrelts, J.C.; Gagnon, M.; Eisenberg, C.; Moerer, J.; Carrithers, J. Impact of telepharmacy in a multihospital health system. Am. J. Health Syst. Pharm. 2010, 67, 1456–1462. [Google Scholar] [CrossRef]
- Omboni, S.; Tenti, M. Telepharmacy for the management of cardiovascular patients in the community. Trends Cardiovasc. Med. 2019, 29, 109–117. [Google Scholar] [CrossRef]
- Baker, J.W.; Forkum, W.; McNeal, J. Utilizing clinical video to improve access and optimize pharmacists’ role in diabetes management. J. Am. Pharm. Assocc. 2019, 59, S63–S66. [Google Scholar] [CrossRef]
- Pincock, L.L.; Montello, M.J.; Tarosky, M.J.; Pierce, W.F.; Edwards, C.W. Pharmacist readiness roles for emergency preparedness. Am. J. Health Syst. Pharm. 2011, 68, 620–623. [Google Scholar] [CrossRef]
- Crane, J.S.; McCluskey, J.D.; Johnson, G.T.; Harbison, R.D. Assessment of community healthcare providers ability and willingness to respond to emergencies resulting from bioterrorist attacks. J. Emerg. Trauma Shock 2010, 3, 13–20. [Google Scholar] [CrossRef]
- Hecox, N. Tuberculin skin testing by pharmacists in a grocery store setting. J. Am. Pharm. Assoc. 2008, 48, 86–91. [Google Scholar] [CrossRef]
- Jakeman, B.; Gross, B.; Fortune, D.; Babb, S.; Tinker, D.; Bachyrycz, A. Evaluation of a pharmacist-performed tuberculosis testing initiative in New Mexico. J. Am. Pham. Assoc. 2015, 55, 307–312. [Google Scholar] [CrossRef]
- International Pharmaceutical Federation (FIP). An overview of Current Pharmacy Impact on Immunization: A Global Report 2016. International Pharmaceutical Federation: The Hague, The Netherlands, 2016. Available online: https://www.fip.org/files/fip/publications/FIP_report_on_Immunisation.pdf (accessed on 29 July 2019).
- Taylor, J.G.; Joubert, R. Pharmacist-led minor ailment programs: A Canadian perspective. Int. J. Gen. Med. 2016, 9, 291–302. [Google Scholar] [CrossRef]
- Paudyal, V.; Watson, M.C.; Sach, T.; Porteous, T.; Bond, C.M.; Wright, D.J.; Cleland, J.; Barton, G.; Holland, R. Are pharmacy-based minor ailment schemes a substitute for other service providers? A systematic review. Br. J. Gen. Pract. 2013, 63, e472–e481. [Google Scholar] [CrossRef]
- Smith, A.J.; Scahill, S.L.; Harrison, J.; Carroll, T.; Medlicott, N.J. Service provision in the wake of a new funding model for community pharmacy. BMC Health Serv. Res. 2018, 18, 307. [Google Scholar] [CrossRef]
- Malangu, N. The future of community pharmacy practice in South Africa in the light of the proposed new qualification for pharmacists: Implications and challenges. Glob. J. Health Sci. 2014, 6, 226–233. [Google Scholar] [CrossRef]
- Sadek, M.M.; Elnour, A.A.; Al Kabini, N.M.; Bhagavathula, A.S.; Baraka, M.A.; Aziz, A.M.; Shehab, A. Community pharmacy and the extended community pharmacist practice roles: The UAE experiences. Saudi Pharm. J. 2016, 24, 563–570. [Google Scholar] [CrossRef]
- Lee, S.; Bell, J.S. Pharmaceutical Care in Asia. In The Pharmacist Guide to Implementing Pharmaceutical Care; Da Costa, F.A., van Mil, J.W.F., Alvarez-Risco, A., Eds.; Springer International: Cham, Switzerland, 2019. [Google Scholar]
- Pharmaceutical Group of the European Union (PGEU). Pharmacy 2030: A Vision for Community Pharmacy in Europe. Belgium. Available online: https://www.pgeu.eu/wp-content/uploads/2019/03/Pharmacy-2030_-A-Vision-for-Community-Pharmacy-in-Europe.pdf (accessed on 29 July 2019).


{kind=link}
| Medication Optimization | Wellness and Prevention | Chronic Care Management | Acute Care Management | Patient Education | Other Patient Care Services |
|---|---|---|---|---|---|
| Medication Packing Home Delivery Medication Reconciliation Appointment-Based Medication Synchronization Medication Adherence Programs Comprehensive Medication Management Services Targeted Medication Review Medication Administration Deprescribing | Screenings | Diabetes HTN Cholesterol Asthma Anticoagulation Heart failure Hepatitis C Menopause Monitoring through laboratory testing
| Test and treat (rapid diagnostics)
Triage and referral | Store
Group Exercise classes Diabetes prevention program Diabetes education program | Tuberculosis testing Telehealth Durable medical equipment Care transitions Population health Emergency preparedness |
| Blood pressure Diabetes Cholesterol Osteoporosis Body Fat HIV Hepatitis C Allergy Lead poisoning | |||||
| Risk Assessment | |||||
| Falls Depression Asthma Cardiovascular risk | |||||
| Weight management Tobacco cessation Contraception Bioidentical hormone replacement Fluoride treatments Naloxone Needle exchange Drug take back Nutraceuticals Annual wellness
Sleep assessment Falls prevention Immunizations Pre-travel health services |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goode, J.-V.; Owen, J.; Page, A.; Gatewood, S. Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States. Pharmacy 2019, 7, 106. https://doi.org/10.3390/pharmacy7030106
Goode J-V, Owen J, Page A, Gatewood S. Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States. Pharmacy. 2019; 7(3):106. https://doi.org/10.3390/pharmacy7030106
Chicago/Turabian StyleGoode, Jean-Venable, James Owen, Alexis Page, and Sharon Gatewood. 2019. "Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States" Pharmacy 7, no. 3: 106. https://doi.org/10.3390/pharmacy7030106
APA StyleGoode, J.-V., Owen, J., Page, A., & Gatewood, S. (2019). Community-Based Pharmacy Practice Innovation and the Role of the Community-Based Pharmacist Practitioner in the United States. Pharmacy, 7(3), 106. https://doi.org/10.3390/pharmacy7030106