1. Introduction
Graduates with a pharmacy degree are employed in a variety of positions, the most important (in terms of numbers) being community, hospital and industrial pharmacy. The discussion on whether these three domains require specific skills with a specific education has long been contentious. Industrial pharmacy as a university discipline is recognized by some European pharmacy departments. The PHARMINE study (
Pharmacy Education in Europe) reported that pharmacy departments in 10/31 European countries give elective pre-graduate courses in industrial pharmacy, and 11/31 departments give post-graduate industrial pharmacy courses [
1]. Most of the graduates from such courses go on to to work in an industrial setting. The PHARMINE study reported that a substantial number (37,308) of European pharmacists (6% of the industrial workforce) work in the pharmaceutical industry [
2]; this is similar to the worldwide figure of 10% given by the International Pharmaceutical Federation [
3].
In some European countries the status of the industrial pharmacist is officially recognized. In France, the profession of “industrial pharmacist” is defined by national law and the statutes of the pharmacy professional body [
4]. On the global European level, this is not the case. In the European Union (EU), the 1985 EU directive on the profession of pharmacy [
5], and the 2013 update [
6], do not recognize any specialization in pharmacy (although these are recognized in medicine).
There is a second EU directive that is relevant in this case, however, and that is the EU directive on qualified persons working in the pharmaceutical industry [
7]. In some EU member states, such as Germany [
8], only those with a pharmacy degree meet the requirements set down in the qualified persons directive.
It appears, therefore, that the argument is equivocal for the existence of a specialized pharmacy job description of “industrial pharmacist” (i.e., a pharmacist working in industry) that is different from that of other specialties such as community pharmacy. This paper looks at one aspect of this discussion: whether industrial pharmacists rank competences for practice differently than do community pharmacists. It is possible that pharmacists working within such specialties view the pharmacy profession differently. Within this context we investigated, therefore, whether the ranking by industrial pharmacists of competences for practice is different from that of community pharmacists.
In the PHAR-QA (“
Quality Assurance in European PHARmacy Education and Training”) project [
9], we asked community and industrial pharmacists to rank competences for pharmacy practice. This paper describes the similarities and differences between the ways in which European industrial and community pharmacists respectively rank competences for pharmacy practice.
2. Experimental Section
Ranking data on competences for practice were obtained using the PHAR-QA
surveymonkey [
10] questionnaire that was available online from 14 February 2014 to 1 November 2014,
i.e., 8.5 months [
11]. Respondents came from 36/49 countries of the European Higher Education Area [
12].
The first six questions were on the profile of the respondent (duration of practice, country of residence, current occupation (industrial, community… pharmacist)). There was also a question on the job title. This allowed a subdivision of industrial pharmacists according to their experience/activity: regulatory affairs, research and development, etc. A similar subdivision of the activities of community pharmacists was not possible, as all respondents in this group were involved in some form of dispensation to patients.
Questions 7 through 19 asked about 13 clusters of 68 competences (see
Appendix A). Questions in clusters 7 to 11 were concerned with personal competences, and in clusters 12 to 19 with patient care competences.
Respondents were asked to rank the proposals for competences on a 4-point Likert scale:
- (1)
Not important = Can be ignored;
- (2)
Quite important =Valuable but not obligatory;
- (3)
Very important = Obligatory, with exceptions depending upon field of pharmacy practice;
- (4)
Essential = Obligatory.
There was also a “cannot rank” possibility as well as that of leaving the answer blank.
Results are presented in the form of “scores” calculated as follows:
Ranking score = (frequency rank 3 + frequency rank 4) as % of total frequency, which represents the percentage of respondents that considered a given competence as “obligatory”.
This calculation is based on a similar calculation made by the MEDINE consortium that studied the ranking of competences for medical practice [
13]. Such scores are used for descriptive purposes only, and no conclusions on statistical differences amongst groups are based on scores.
Leik ordinal consensus [
14] was calculated as an indication of the dispersion of the data using an Excel spreadsheet. The original Leik paper cited previously gives an explicit mathematical example of the calculation of ordinal consensus. Responses for consensus were arbitrarily classified as: < 0.2 poor, 0.21–0.4 fair, 0.41–0.6 moderate, 0.61–0.8 substantial, > 0.81 good, according to the scale used in MEDINE study.
The statistical significance of differences between rankings of competences or between rankings by different categories of respondents was tested by the chi-square test (confidence level 95%). Statistical tests were performed using GraphPad software [
15].
Results are presented at 2 levels: that of the 13 clusters and that of the 68 competences.
Respondents could also add their comments on the different clusters. An attempt was made to analyze comments using the NVivo10 program [
16] for the semi-quantitative analysis of unstructured data. It was found that the numbers involved were too small to draw significant conclusions.
3. Results and Discussion
The distribution by duration of practice of the groups is given in
Table 1.
Table 1.
Distribution of duration of practice (years) in industrial and community pharmacist responders. n: number in each category.
Table 1.
Distribution of duration of practice (years) in industrial and community pharmacist responders. n: number in each category.
| Respondents | < 5 | 6–10 | 11–20 | 21–40 | Blank | Total |
|---|
| Industrial pharmacists (n) | 26 | 31 | 28 | 23 | 27 | 135 |
| Community pharmacists (n) | 50 | 51 | 41 | 56 | 60 | 258 |
Most respondents had less than 20 years of experience, thus in both cases a relatively “young” population was involved. This may be due to the higher motivation of a younger population to reply to a questionnaire.
Respondents came from 36 European countries. Nineteen countries provided 5 or more respondents to one or both groups; they were: Belgium, Croatia, Czech Republic, Estonia, Finland, Germany, Greece, Hungary, Ireland, Italy, Macedonia, Montenegro, Norway, Romania, Slovenia, Spain, Switzerland, The Netherlands, and the United Kingdom.
The numbers of industrial pharmacy respondents arranged according to experience/activity are given in
Table 2.
Table 2.
Numbers of industrial pharmacy respondents subdivided according to experience/activity.
Table 2.
Numbers of industrial pharmacy respondents subdivided according to experience/activity.
| Experience/Activity | Number |
|---|
| Management | 24 |
| Regulatory affairs | 23 |
| Research and development | 18 |
| Quality assurance/compliance | 16 |
| Pharmaceutical technology | 10 |
| Clinical/medical affairs | 8 |
| Pharmacovigilance | 5 |
| Qualified person | 5 |
| Marketing and sales | 5 |
| Research student/Ph.D. | 1 |
| “Industrial pharmacist” or “pharmacist” | 8 |
| Blank | 12 |
Table 2 shows that, while some respondents work in a typically “pharmaceutical” environment (such as regulatory affairs and pharmaceutical technology), many others work in more “generic” environments (such as management and quality assurance). If we consider that industrial surroundings correspond to 4 groups/stages, namely (1) research and development; (2) production; (3) analyses and quality assurance; and (4) marketing and sales, it appears that not all pharmacists employed in marketing and sales feel that they are industrial pharmacists. Indeed, marketing and sales representatives of “big pharma” are sometimes very far from classical industrial surroundings, even though they are employed in industry.
Table 3 shows the overall distribution of rankings by industrial and community pharmacists.
Table 3.
Overall distribution (over 13 clusters of 68 competences) of rankings by industrial and community pharmacists.
Table 3.
Overall distribution (over 13 clusters of 68 competences) of rankings by industrial and community pharmacists.
| Ranking | Industrial Pharmacists | Community Pharmacists |
|---|
| Number of respondents | 138 | 258 |
| Theoretical number of replies | 9384 (= 138 × 68) | 17,544 (= 258 × 68) |
| Rank | Number | % | Number | % |
| 4 | 2510 | 26.8 | 6643 | 37.9 |
| 3 | 3502 | 37.3 | 6002 | 34.2 |
| 2 | 1876 | 20.0 | 3076 | 17.5 |
| 1 | 432 | 4.6 | 608 | 3.5 |
| Cannot rank + blanks | 1064 | 11.3 | 1215 | 6.9 |
| Score (%) | =((2510 + 3502)/8320) × 100) = 72.3 | = ((6643 + 6002)/16,329) × 100 = 77.4 |
| Leik ordinal consensus | 0.58 | 0.55 |
All but 7–11% of respondents were able to rank all competences. This suggests that the majority in both groups of respondents believed that they were sufficiently informed to reply to almost all the questions asked.
As judged from the Leik ordinal consensus values, dispersion was low. This suggests that both groups were relatively homogeneous and that subgroups with responses significantly different from the overall group do not exist. Similar values for ordinal consensus have been reported by the MEDINE consortium.
Overall ranking by industrial pharmacists was significantly lower (72%) than that by community pharmacists (77%). This raises the question of whether industrial pharmacists globally believed that the competence framework was less applicable; however, the global score was high with almost 3/4 of industrial pharmacists considering the competences “obligatory”. The global lower score of industrial pharmacists was weighted by the low scores they gave to patient care competences (see later).
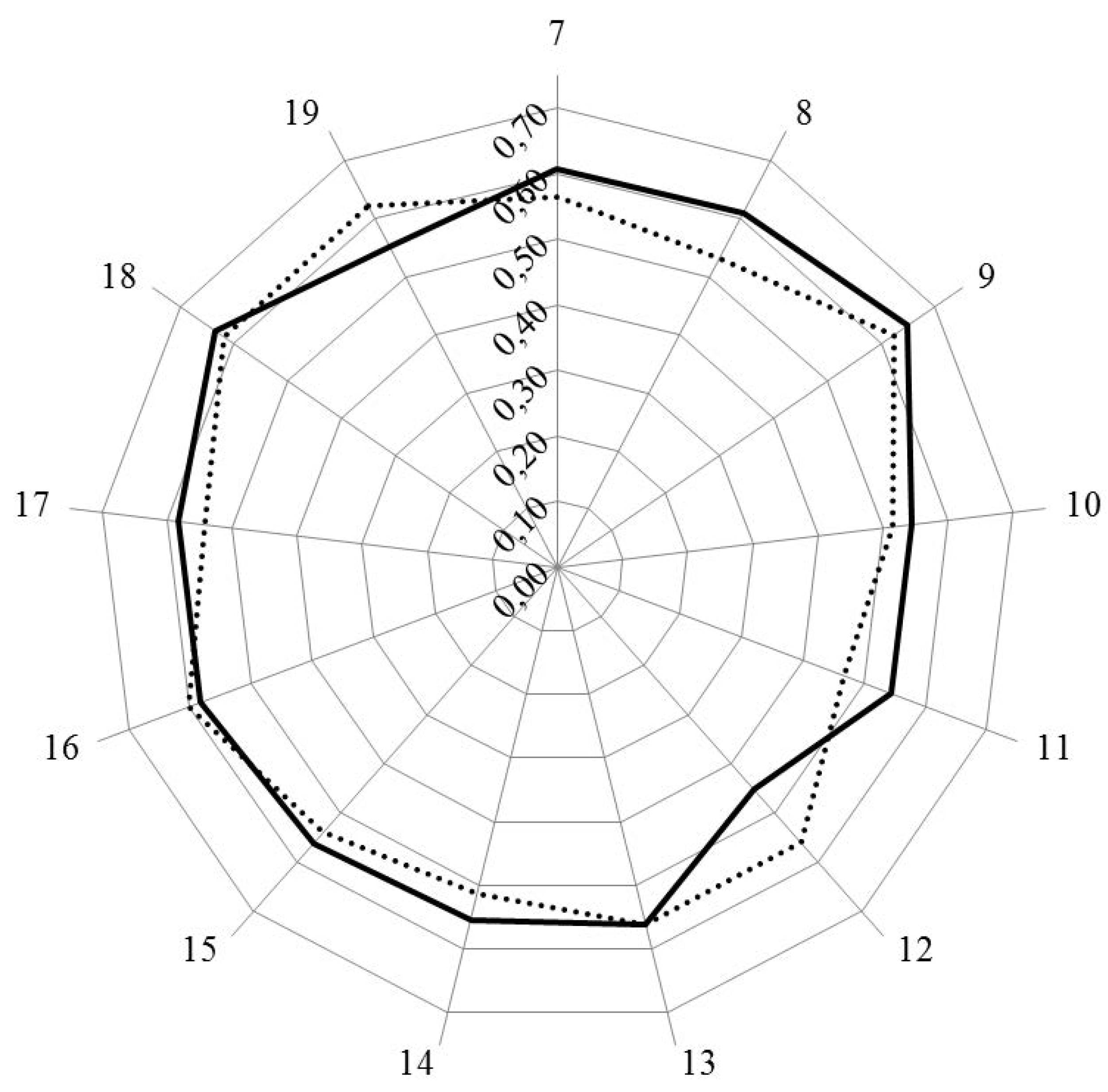
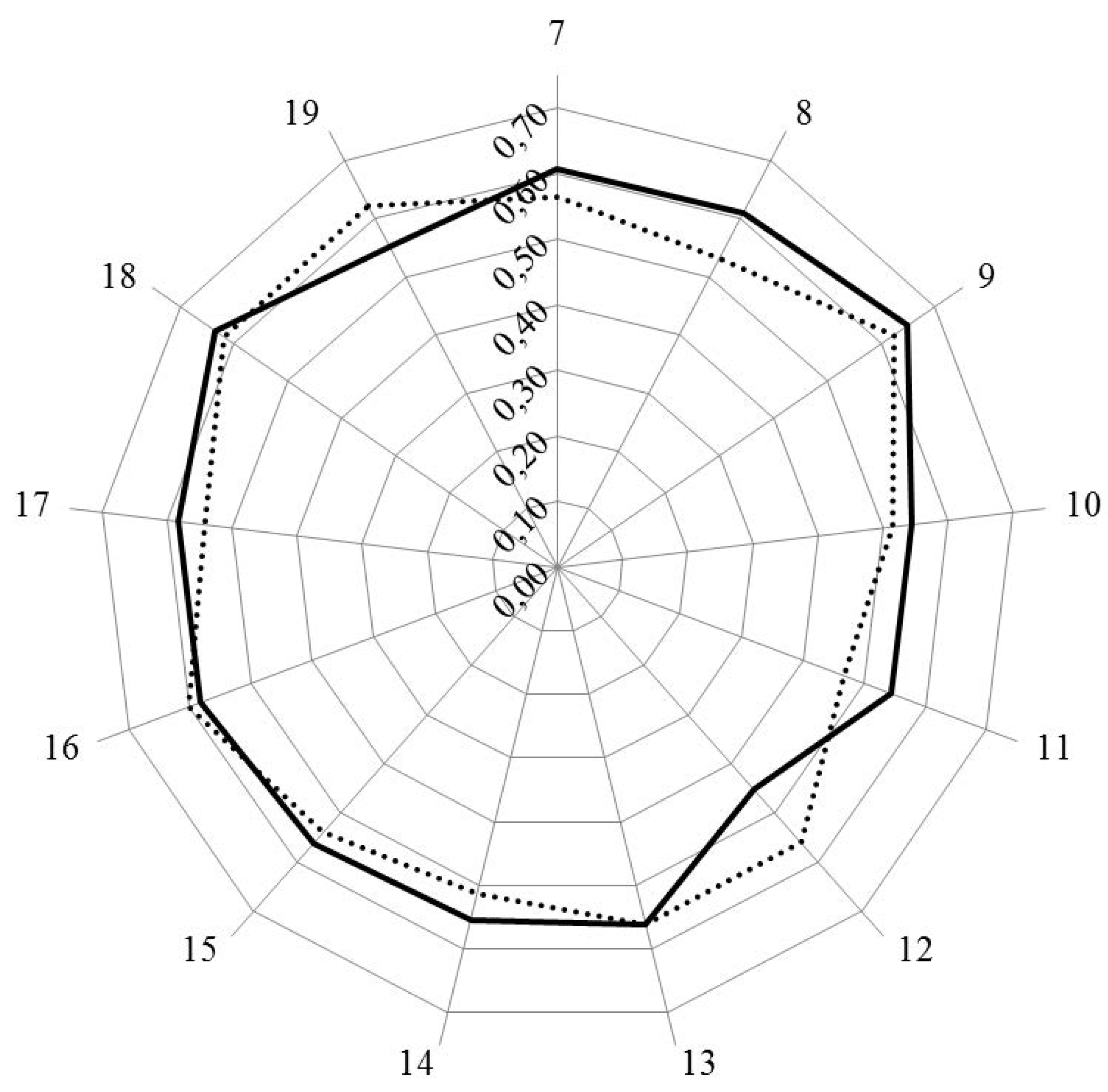
Figure 1 and
Figure 2 show the results for analysis by clusters. In
Figure 1, the values for Leik ordinal consensus are shown.
Leik ordinal consensus was higher for industrial pharmacists in 10/13 clusters including cluster 11 that dealt with competences for industrial pharmacy.
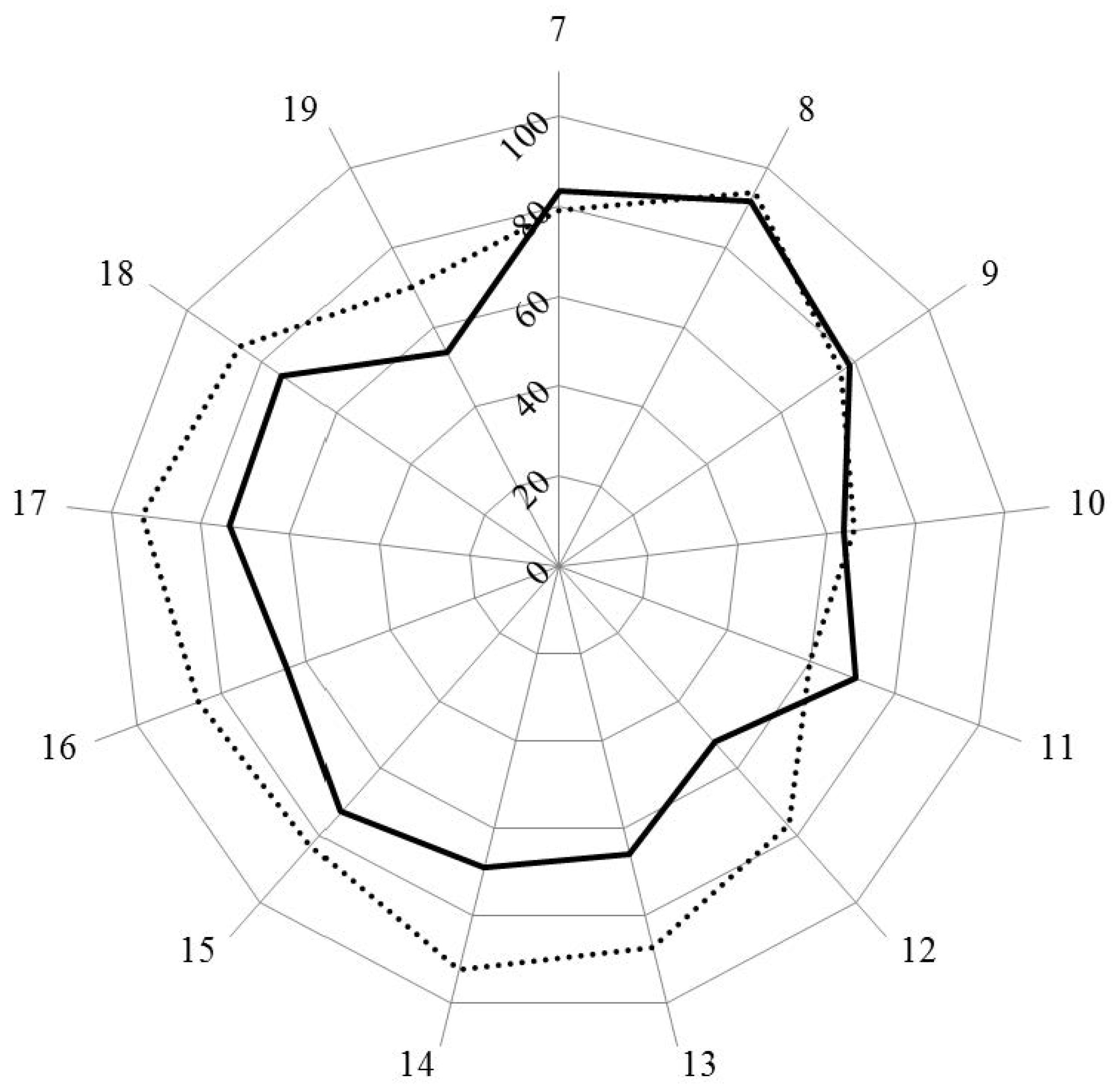
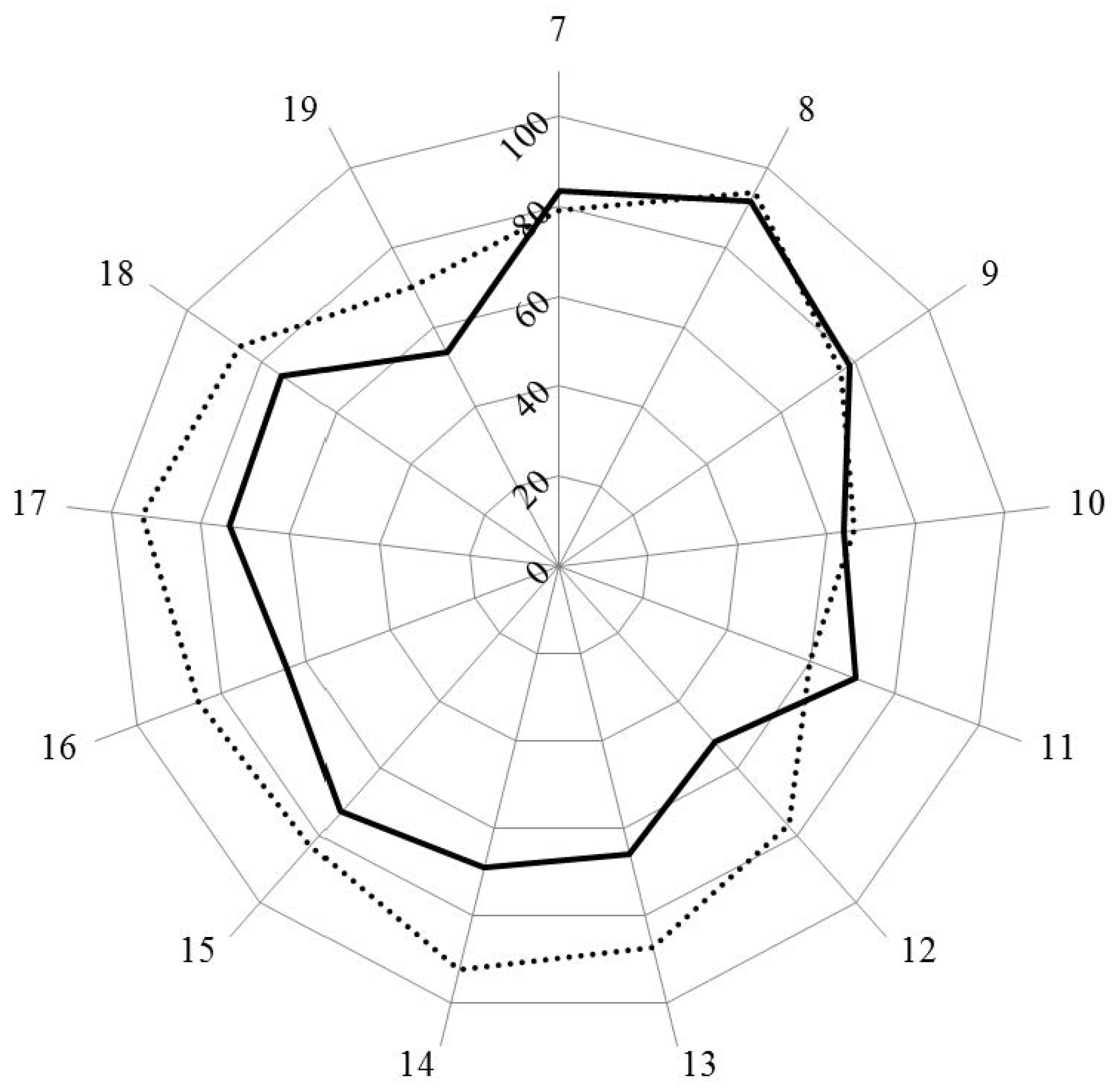
Scores for personal competences (clusters 7 to 11) were similar in industrial and community pharmacists, except for cluster 11, dealing with industrial pharmacy, for which industrial pharmacists scored higher. Scores for clusters dealing with patient care competences (clusters 12 to 19) were lower for industrial pharmacists.
Figure 1.
Leik ordinal consensus for rankings by clusters for industrial (solid line) and community (dotted line) pharmacists.
Figure 1.
Leik ordinal consensus for rankings by clusters for industrial (solid line) and community (dotted line) pharmacists.
Figure 2.
Scores (%) for rankings by clusters for industrial (solid line) and community (dotted line) pharmacists.
Figure 2.
Scores (%) for rankings by clusters for industrial (solid line) and community (dotted line) pharmacists.
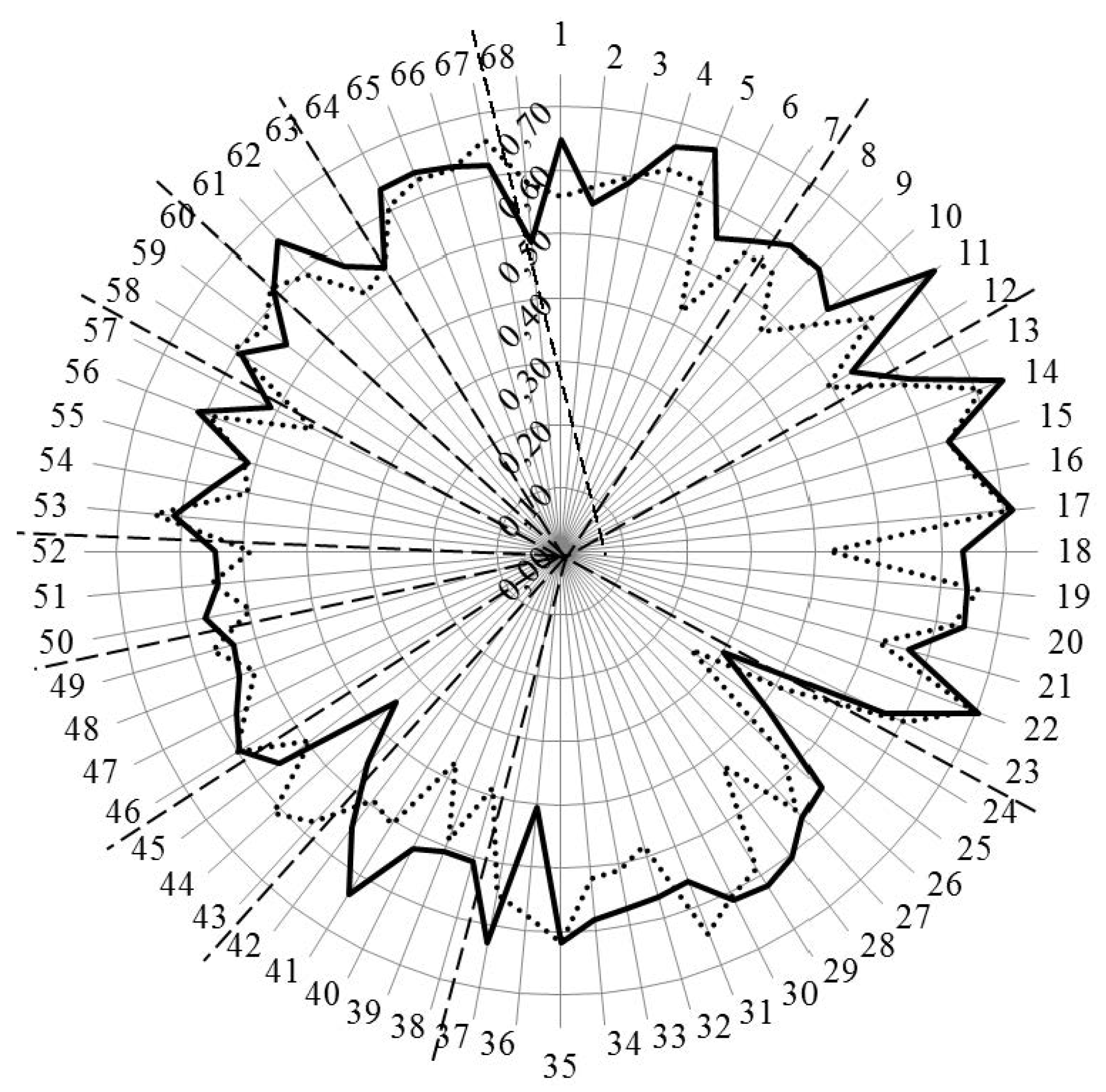
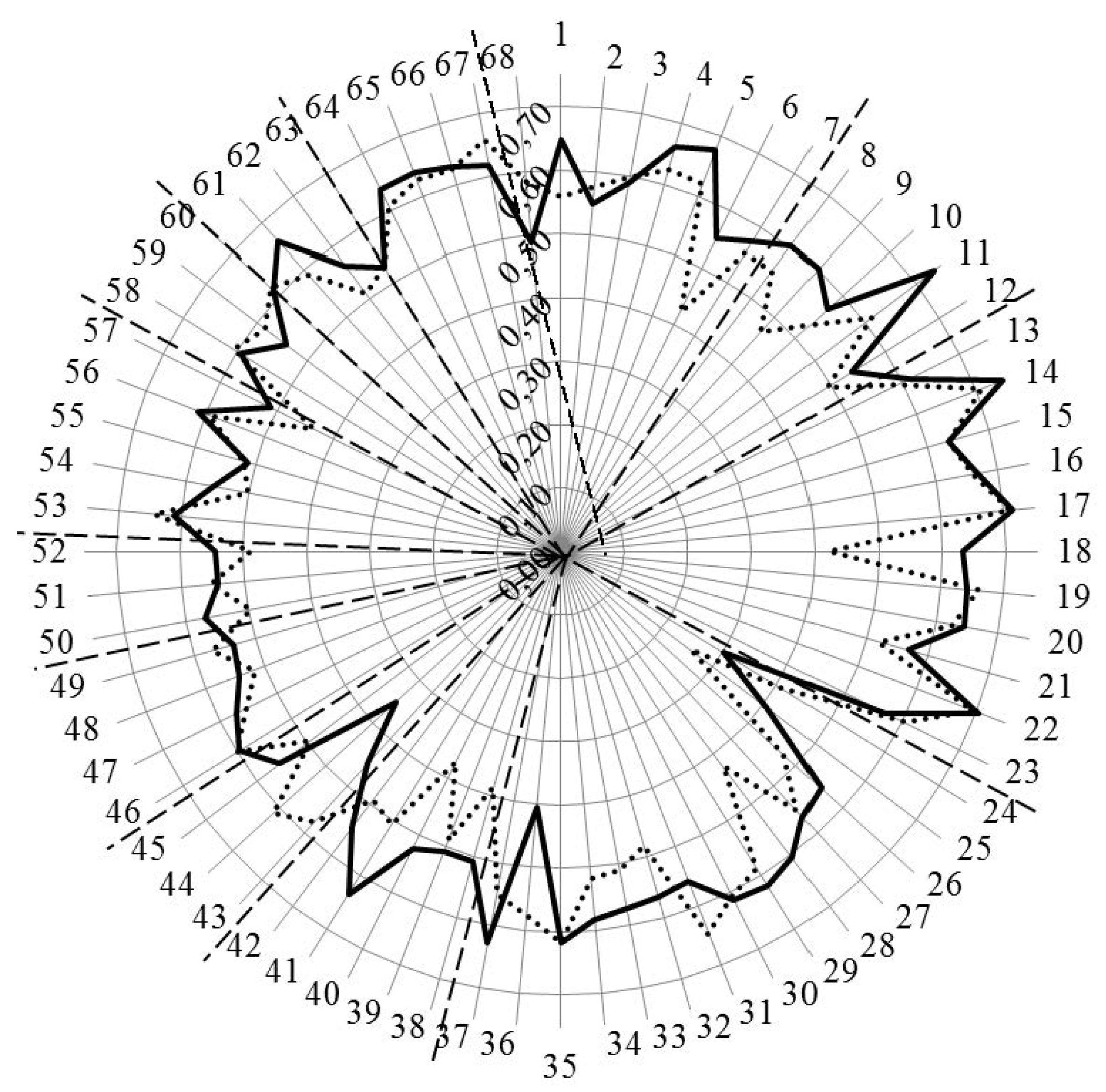
Figure 3 and
Figure 4 show the results for analysis by competences. In
Figure 3, the values for Leik ordinal consensus are shown.
Figure 3.
Leik ordinal consensus for rankings by competences for industrial (solid line) and community (dotted line) pharmacists. Dashed lines separate the different clusters of competences.
Figure 3.
Leik ordinal consensus for rankings by competences for industrial (solid line) and community (dotted line) pharmacists. Dashed lines separate the different clusters of competences.
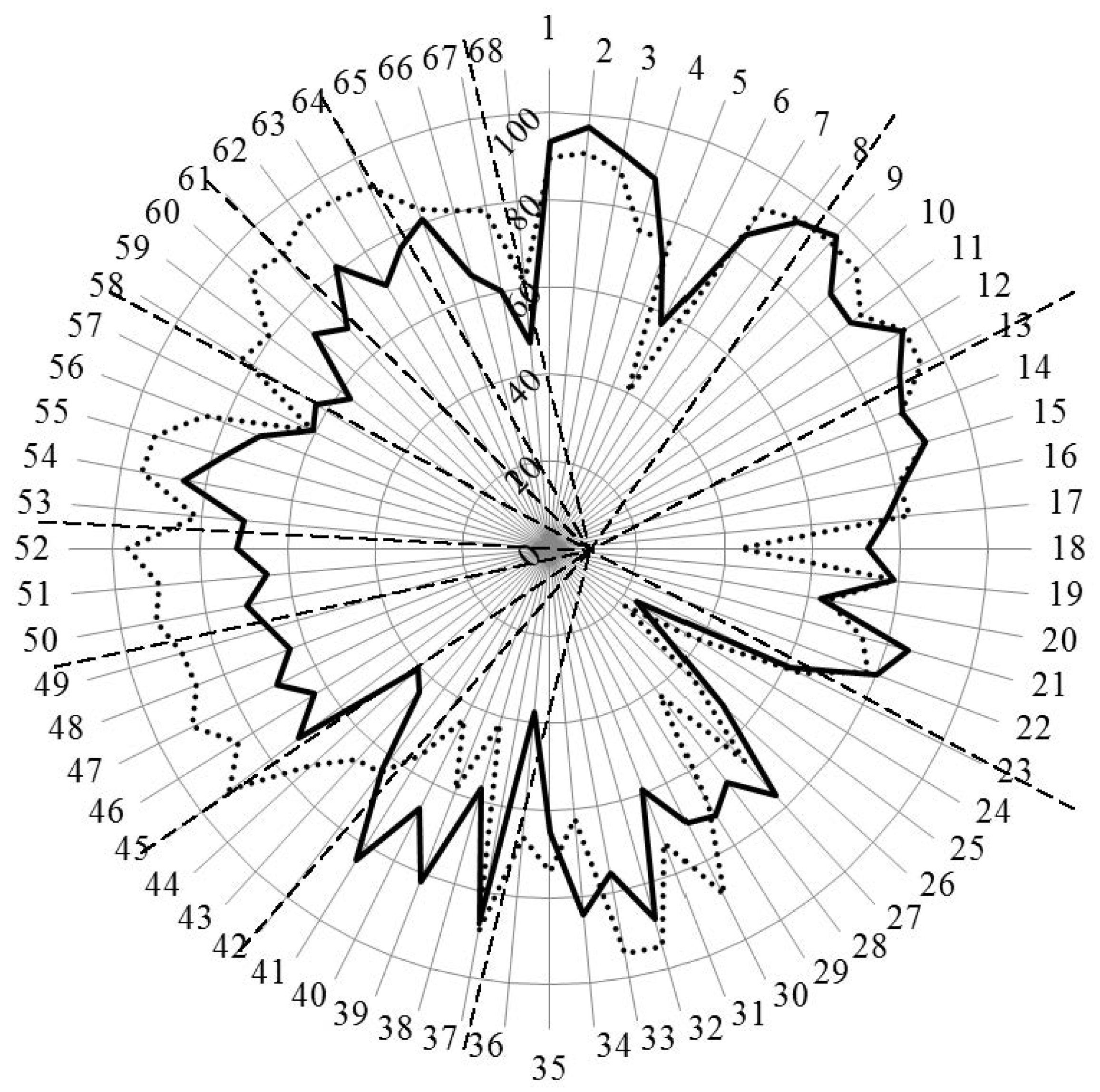
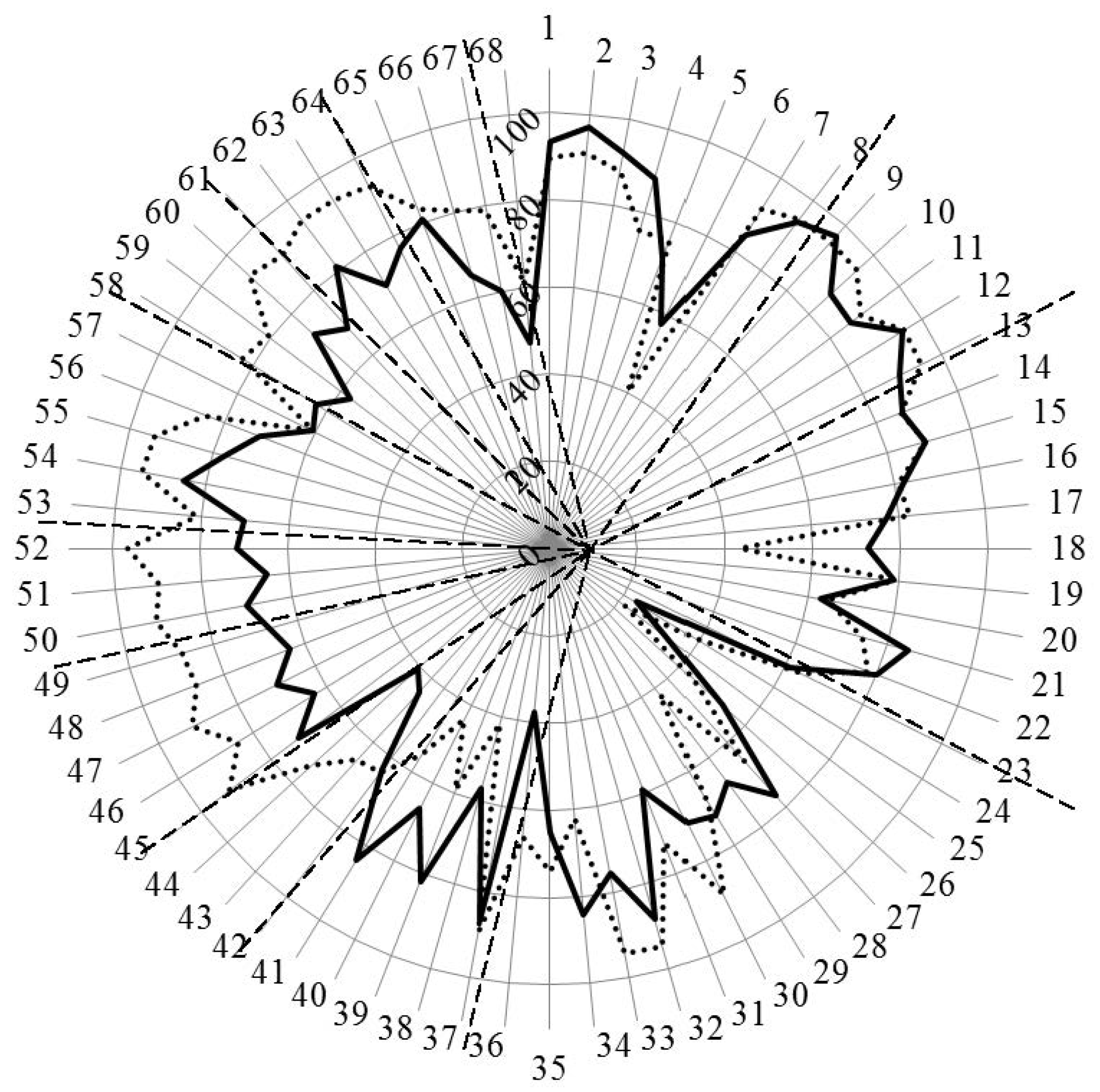
Figure 4.
Scores (%) for rankings by competences for industrial (solid line) and community (dotted line) pharmacists. Dashed lines separate the different clusters of competences.
Figure 4.
Scores (%) for rankings by competences for industrial (solid line) and community (dotted line) pharmacists. Dashed lines separate the different clusters of competences.
Overall, the ordinal consensus values were higher for industrial than for community pharmacists. This was especially true for competences 6 (research), 18 (development, production of medicines), 28 (analytical chemistry), 38 (design, synthesis,
etc. of active substances), 40 (EU directive on qualified persons), and 41 (drug registration, licensing and marketing). For all these competences, the consensus for industrial pharmacists was higher than community pharmacists (
Figure 4 and
Appendix A). For competences 31 (microbiology) and 44 (diagnostic tests) the ordinal consensus for community pharmacists was higher than that for industrial pharmacists, as were the scores (
Figure 4 and
Appendix A).
This graph shows that competences on the right-hand side concerned with personal values, subject matters and industrial pharmacy were often ranked higher by industrial pharmacists. Competences on the left-hand side concerned with patient care were often ranked higher by community pharmacists. A proviso must be added here; through a comparison between
Figure 4 with
Figure 3, it is obvious that, for competences scoring low (e.g., 24 and 25), consensus was low. Thus, the low ranking was far from unanimous.
Going into more detail,
Table 4 shows the competences for which industrial pharmacist ranked higher (upper) and for which community pharmacists ranked higher (lower).
Table 4.
Competences ranked higher by industrial pharmacist (upper) and by community pharmacists (lower). (a) Industrial > community; (b) Community > industrial.
(a)
| n | Competence |
|---|
| 4 | Capacity to evaluate scientific data in line with current scientific and technological knowledge |
| 6 | Ability to design and conduct research using appropriate methodology |
| 18 | Ability to design and manage the development processes in the production of medicines |
| 25 | Physics |
| 28 | Analytical chemistry |
| 34 | Pharmaceutical technology including analyses of medicinal products |
| 38 | Current knowledge of design, synthesis, isolation, characterization and biological evaluation of active substances |
| 39 | Current knowledge of good manufacturing practice (GMP) and of good laboratory practice (GLP) |
| 40 | Current knowledge of European directives on qualified persons (QPs) |
| 41 | Current knowledge of drug registration, licensing and marketing |
(b)
| n | Competence |
|---|
| 24 | Plant and animal biology |
| 30 | Anatomy and physiology; medical terminology |
| 33 | Pharmacotherapy and pharmaco-epidemiology |
| 36 | Pharmacognosy |
| 43 | Ability to perform and interpret medical laboratory tests |
| 44 | Ability to perform appropriate diagnostic or physiological tests to inform clinical decision making (e.g., measurement of blood pressure) |
| 45 | Ability to recognise when referral to another member of the healthcare team is needed because a potential clinical problem is identified (pharmaceutical, medical, psychological or social) |
| 46 | Retrieval and interpretation of relevant information on the patient’s clinical background |
| 47 | Retrieval and interpretation of an accurate and comprehensive drug history if and when required |
| 48 | Identification of non-adherence and implementation of appropriate patient intervention |
| 49 | Ability to advise to physicians and, in some cases, prescribe medication |
| 50 | Identification, understanding and prioritization of drug-drug interactions at a molecular level (e.g., use of codeine with paracetamol) |
| 51 | Identification, understanding, and prioritization of drug-patient interactions, including those that preclude or require the use of a specific drug (e.g., trastuzumab for treatment of breast cancer in women with HER2 overexpression) |
| 52 | Identification, understanding, and prioritization of drug-disease interactions (e.g., NSAIDs in heart failure) |
| 55 | Critical evaluation of the prescription to ensure that it is clinically appropriate and legal |
| 56 | Familiarity with the supply chain of medicines and the ability to ensure timely flow of drug products to the patient |
| 58 | Promotion of public health in collaboration with other actors in the healthcare system |
| 59 | Provision of appropriate lifestyle advice on smoking, obesity, etc. |
| 60 | Provision of appropriate advice on resistance to antibiotics and similar public health issues |
| 61 | Ability to use effective consultations to identify the patient’s need for information |
| 62 | Provision of accurate and appropriate information on prescription medicines |
| 63 | Provision of informed support for patients in selection and use of non-prescription medicines for minor ailments (e.g., cough remedies) |
| 64 | Identification and prioritization of problems in the management of medicines in a timely manner and with sufficient efficacy to ensure patient safety |
| 66 | Undertaking of a critical evaluation of prescribed medicines to confirm that current clinical guidelines are appropriately applied |
| 67 | Assessment of outcomes on the monitoring of patient care and follow-up interventions |
| 68 | Evaluation of cost effectiveness of treatment |
The competences ranked higher by industrial pharmacists fall into three groups with, firstly, competences 4, 6 and 18 on evaluation of scientific data, research, and production of medicines. Scores for community pharmacists on 2 of these competences (6, 18) were less than 50%. The second group was concerned with the subject matters physics (25) 33%, analytical chemistry (28) 67%, and pharmaceutical technology (34) 84%. Subject matters were included because they figure in the EU directive on the sectoral profession of pharmacy. The authors recognize that they are not competences but part of the foundation of competences. Having said that, it should be noted that community pharmacists ranked these elements very low, with a score of 22% for physics and 42% for analytical chemistry. Thus, the general message that all the subject matters cited in the EU directive are essential for science-based pharmacy practice is not understood, as concerns subjects such as physics.
In the lower part of
Table 4, the competences that are ranked higher by community pharmacists are shown. Four of these concern subject areas (24, 30, 33, and 36), but the majority concern patient care competences. For the latter community pharmacists scored significantly higher than industrial pharmacists for all but five competences. This is not to say that industrial pharmacists scored low for patient care competences, as almost all of their scores were between 60% and 80%. Thus, they do recognize the need for information relating to the pharmacist as a medicine specialist (see also comments below).
Overall, the observations in the previous paragraphs suggest that the two groups are often ranking in the context of their own specific activity and, following on from this, that certain competences are needed for certain specializations. Continuing this argument further, certain competences could thus be part of an “industrial pharmacy-oriented” degree course, and others part of a “community pharmacy-oriented” degree course (taking for example, those in
Table 4). An alternative argument is that this is in favor of “amplifying” different clusters in different specializations within a single curriculum, rather than “separating” competences into different curricula for the two activities.
Comments were made by 15/138 (11%) of industrial pharmacist and 23/258 (9%) of community pharmacist respondents. Our initial objective was to evaluate whether comments were in line with scoring, but the low numbers of comments received did not permit a satisfactory analysis using semi-quantitative analysis of unstructured data (results not shown). Comments are reported here, therefore, in a “raw data” form.
Comments are grouped into areas in
Table 5.
There were several comments on the English phraseology and the construction of the questions, and these have been taken into consideration in the production of the revised version of the questionnaire. Others pointed to the esoteric nature of certain competences and the recognition of specialization, be it industrial or community. Of interest also is the fact that industrial pharmacists recognized the necessity of all competences, including patient care competences, and the nature of the pharmacist as a “medicines specialist”.
Table 5.
Comments by industrial and community pharmacists.
Table 5.
Comments by industrial and community pharmacists.
| Area | Typical Examples of Comments Made. |
|---|
| Industrial Pharmacist. | Community Pharmacist. |
|---|
| Understanding of the question | - -
I do not understand the question. - -
I have not spoken English for a long time. - -
One point only to each question. - -
Important to interpret but not necessarily done.
| - -
The question is very convoluted. - -
The question is rather unclear.
|
| Production of medicines. | | We buy rather than produce them. |
| Information sources. | | - -
I get all my information (on drugs) from reliable sources. - -
Pre-selection of new scientific information by official institutes.
|
| Framework for community pharmacy practice. | - -
Being a pharmacist, you need basic information in all areas. - -
Although I work in industry, all these competences are needed. - -
The pharmacist is a medicines specialist. - -
Response depends on the area you are working in.
| - -
All answers refer to daily work in a community pharmacy. - -
Answers relate to my working environment. - -
Pharmaceutical care is essential. - -
Some competences are for specialists. - -
Some competences are for hospital pharmacists.
|
| Economics/business administration. | Cost effectiveness assessment is a specialist role. | - -
It is vital to have economics and business administration. - -
“Business environment,” yes, but keep your eye on the health aspect. - -
Pharmacists follow recommendations of NICE not cost effectiveness.
|
| No prescription. | | - -
Pharmacists are not allowed to prescribe in my country. - -
Pharmacists are not physicians.
|
| Healthcare team. | | Pharmacists are responsible for their part of the job. |
| Subject areas. | - -
You need basic knowledge of all areas. - -
Pharmacognosy is no longer a required subject. - -
Radio-pharmacy would be useful.
| We do not need analytical chemistry as we are not analyzing any more. |
| Industrial pharmacy/research. | - -
These apply to industrial pharmacists. - -
These competences are esoteric. - -
Preclinical issues are not part of my work experience.
| - -
I have never worked in industry. - -
These competences are for industry and research.
|
| Consultation/diagnosis. | | - -
A pharmacist is not a doctor. - -
It is not uncommon that the pharmacist is the first person to whom the patient explains his symptoms. - -
We are not appropriately trained for this. - -
Commercial interests are involved.
|
Globally, the comments leave a subjective impression of backing up the scores, but, as explained in
Section 2, no solid conclusions can be drawn.



 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}