
Social Prescribing Competence among Community Pharmacists and Pharmacy Students in Norway



Abstract
1. Introduction
1.1. Social Prescribing or Community Referral
1.2. Role of Pharmacists in Social Prescribing or Community Referral
2. Methods
2.1. Study Design and Population
2.2. Construction of the Questionnaire
2.3. Pilot Testing of the Questionnaire
2.4. Ethical Assessment
2.5. Data Collection and Handling
2.6. Statistical Analysis
3. Results
3.1. Socio-Demographic Information
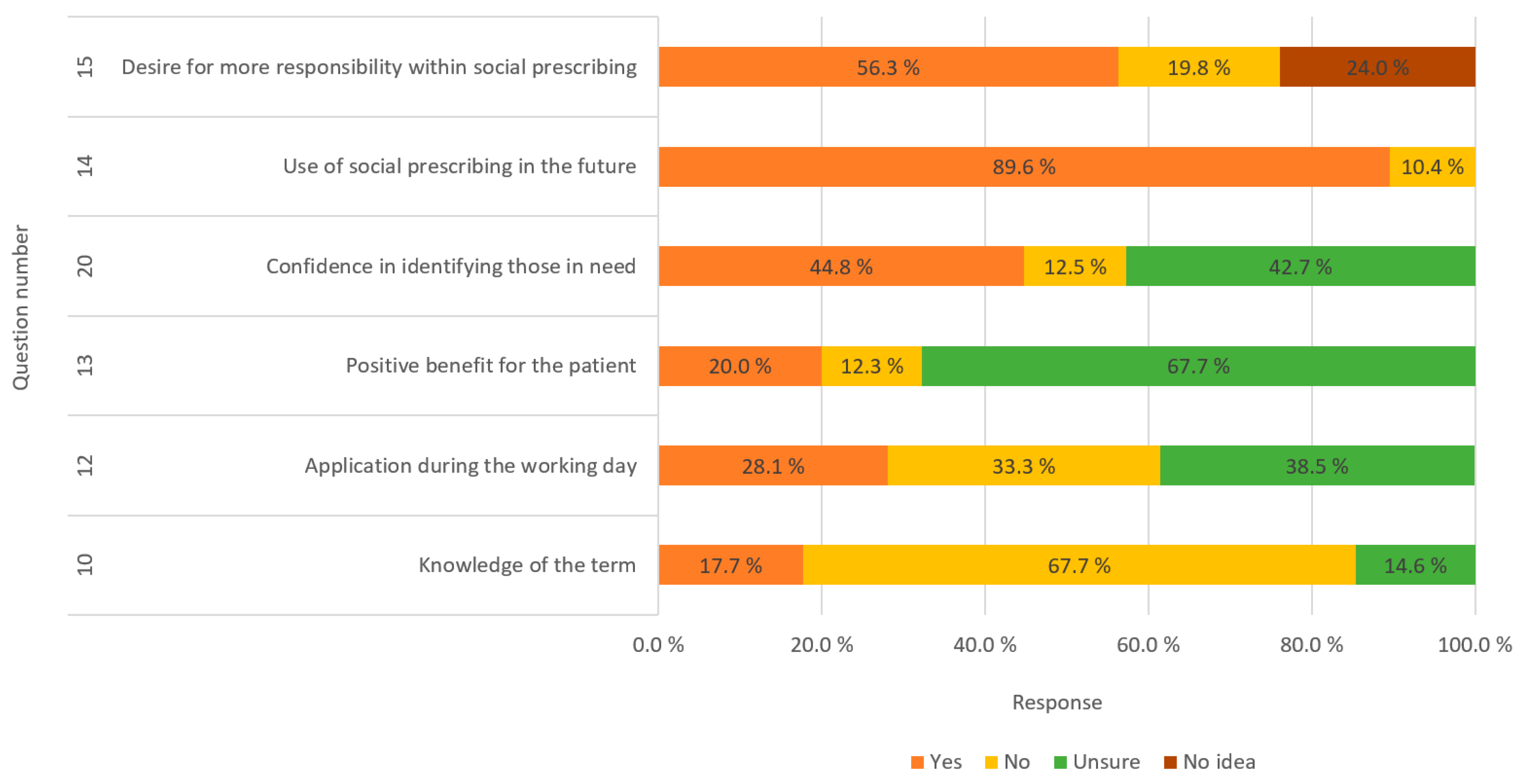
3.2. Questions with Dichotomous Answer Options
4. Discussion
4.1. Knowledge and Perceptions towards Social Prescribing among Pharmacy Students and Community Pharmacists in Norway
4.2. Competence
4.3. Study Strengths and Limitations
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hough, K.; Kotwal, A.A.; Boyd, C.; Tha, S.H.; Perissinotto, C. What Are “Social Prescriptions” and How Should They Be Integrated into Care Plans? AMA J. Ethics 2023, 25, E795–E801. [Google Scholar] [CrossRef]
- Oster, C.; Skelton, C.; Leibbrandt, R.; Hines, S.; Bonevski, B. Models of social prescribing to address non-medical needs in adults: A scoping review. BMC Health Serv. Res. 2023, 23, 642. [Google Scholar] [CrossRef]
- Husk, K.; Elston, J.; Gradinger, F.; Callaghan, L.; Asthana, S. Social prescribing: Where is the evidence? Br. J. Gen. Pract. 2019, 69, 6–7. [Google Scholar] [CrossRef]
- Hassan, S.M.; Ring, A.; Goodall, M.; Abba, K.; Gabbay, M.; van Ginneken, N. Social prescribing practices and learning across the North West Coast region: Essential elements and key challenges to implementing effective and sustainable social prescribing services. BMC Health Serv. Res. 2023, 23, 562. [Google Scholar] [CrossRef] [PubMed]
- Vidovic, D.; Reinhardt, G.Y.; Hammerton, C. Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 5276. [Google Scholar] [CrossRef] [PubMed]
- Turk, A.; Tierney, S.; Wong, G.; Todd, J.; Chatterjee, H.J.; Mahtani, K.R. Self-growth, wellbeing and volunteering—Implications for social prescribing: A qualitative study. SSM—Qual. Res. Health 2022, 2, 100061. [Google Scholar] [CrossRef]
- Andermann, A. Taking action on the social determinants of health in clinical practice: A framework for health professionals. Cmaj 2016, 188, E474–E483. [Google Scholar] [CrossRef] [PubMed]
- Islam, K.F.; Awal, A.; Mazumder, H.; Munni, U.R.; Majumder, K.; Afroz, K.; Tabassum, M.N.; Hossain, M.M. Social cognitive theory-based health promotion in primary care practice: A scoping review. Heliyon 2023, 9, e14889. [Google Scholar] [CrossRef] [PubMed]
- Bild, E.; Pachana, N.A. Social prescribing: A narrative review of how community engagement can improve wellbeing in later life. J. Community Appl. Soc. Psychol. 2022, 32, 1148–1215. [Google Scholar] [CrossRef]
- Morse, D.F.; Sandhu, S.; Mulligan, K.; Tierney, S.; Polley, M.; Chiva Giurca, B.; Slade, S.; Dias, S.; Mahtani, K.R.; Wells, L.; et al. Global developments in social prescribing. BMJ Glob. Health 2022, 7, e008524. [Google Scholar] [CrossRef]
- Chatterjee, H.J.; Camic, P.M.; Lockyer, B.; Thomson, L.J.M. Non-clinical community interventions: A systematised review of social prescribing schemes. Arts Health 2018, 10, 97–123. [Google Scholar] [CrossRef]
- Islam, M.M. Social Prescribing-An Effort to Apply a Common Knowledge: Impelling Forces and Challenges. Front. Public Health 2020, 8, 515469. [Google Scholar] [CrossRef] [PubMed]
- Kilgarriff-Foster, A.; O’Cathain, A. Exploring the components and impact of social prescribing. J. Public Ment. Health 2015, 14, 127–134. [Google Scholar] [CrossRef]
- Cooper, M.; Flynn, D.; Avery, L.; Ashley, K.; Jordan, C.; Errington, L.; Scott, J. Service user perspectives on social prescribing services for mental health in the UK: A systematic review. Perspect. Public Health 2023, 143, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Davis-Hall, M. The Bromley by Bow Centre: Harnessing the power of community. Br. J. Gen. Pract. 2018, 68, 333. [Google Scholar] [CrossRef] [PubMed]
- Leavell, M.A.; Leiferman, J.A.; Gascon, M.; Braddick, F.; Gonzalez, J.C.; Litt, J.S. Nature-Based Social Prescribing in Urban Settings to Improve Social Connectedness and Mental Well-being: A Review. Curr. Environ. Health Rep. 2019, 6, 297–308. [Google Scholar] [CrossRef]
- Callard, F.; Friedli, L. Imagine East Greenwich: Evaluating the impact of the arts on health and well-being. J. Public Ment. Health 2005, 4, 29–41. [Google Scholar] [CrossRef]
- Chen, I.; Opiyo, N.; Tavender, E.; Mortazhejri, S.; Rader, T.; Petkovic, J.; Yogasingam, S.; Taljaard, M.; Agarwal, S.; Laopaiboon, M.; et al. Non-clinical interventions for reducing unnecessary caesarean section. Cochrane Database Syst. Rev. 2018, 9, Cd005528. [Google Scholar] [CrossRef]
- Mohiuddin, A.K. The Excellence of Pharmacy Practice. Innov. Pharm. 2020, 11. [Google Scholar] [CrossRef]
- Katoue, M.G.; Schwinghammer, T.L. Competency-based education in pharmacy: A review of its development, applications, and challenges. J. Eval. Clin. Pract. 2020, 26, 1114–1123. [Google Scholar] [CrossRef]
- Allayla, T.H.; Nouri, A.I.; Hassali, M.A.A. Pharmacist Role in Global Health: A Review of Literature. Malays. J. Pharm. Sci. 2018, 16, 45–54. [Google Scholar] [CrossRef]
- Ilardo, M.L.; Speciale, A. The Community Pharmacist: Perceived Barriers and Patient-Centered Care Communication. Int. J. Environ. Res. Public Health 2020, 17, 536. [Google Scholar] [CrossRef] [PubMed]
- Piquer-Martinez, C.; Urionagüena, A.; Benrimoj, S.I.; Calvo, B.; Martinez-Martinez, F.; Fernandez-Llimos, F.; Garcia-Cardenas, V.; Gastelurrutia, M.A. Integration of community pharmacy in primary health care: The challenge. Res. Soc. Adm. Pharm. 2022, 18, 3444–3447. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.A.; Nicholls, G.M.; Taylor, A.D.J. Perceptions of Pharmacy Involvement in Social Prescribing Pathways in England, Scotland and Wales. Pharmacy 2019, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, L.; Hughes, S.; Rathbone, A. Social prescribing in community pharmacy: A systematic review and thematic synthesis. Pharm. J. 2021, 307. [Google Scholar]
- Kors, R. Røde Kors Sosial Resept. Available online: https://www.rodekors.no/lokalforeninger/hordaland/om/aktiviteter/sosial-resept/ (accessed on 14 January 2024).
- Majchrowska, A.; Bogusz, R.; Nowakowska, L.; Pawlikowski, J.; Piątkowski, W.; Wiechetek, M. Public Perception of the Range of Roles Played by Professional Pharmacists. Int. J. Environ. Res. Public Health 2019, 16, 2787. [Google Scholar] [CrossRef] [PubMed]
- Shirdel, A.; Pourreza, A.; Daemi, A.; Ahmadi, B. Health-promoting services provided in pharmacies: A systematic review. J. Educ. Health Promot. 2021, 10, 234. [Google Scholar] [CrossRef]
- Nelson, N.R.; Armistead, L.T.; Blanchard, C.M.; Rhoney, D.H. The pharmacist’s professional identity: Preventing, identifying, and managing medication therapy problems as the medication specialist. JACCP J. Am. Coll. Clin. Pharm. 2021, 4, 1564–1571. [Google Scholar] [CrossRef]
- Lott, B.E.; Anderson, E.J.; Villa Zapata, L.; Cooley, J.; Forbes, S.; Taylor, A.M.; Manygoats, T.; Warholak, T. Expanding pharmacists’ roles: Pharmacists’ perspectives on barriers and facilitators to collaborative practice. J. Am. Pharm. Assoc. 2021, 61, 213–220. [Google Scholar] [CrossRef]
- Janzen, D.; Fitzpatrick, K.; Jensen, K.; Suveges, L. Women in pharmacy: A preliminary study of the attitudes and beliefs of pharmacy students. Can. Pharm. J. 2013, 146, 109–116. [Google Scholar] [CrossRef]
- Wu, M.-J.; Zhao, K.; Fils-Aime, F. Response rates of online surveys in published research: A meta-analysis. Comput. Hum. Behav. Rep. 2022, 7, 100206. [Google Scholar] [CrossRef]
- Lee, H.; Koh, S.B.; Jo, H.S.; Lee, T.H.; Nam, H.K.; Zhao, B.; Lim, S.; Lim, J.A.; Lee, H.H.; Hwang, Y.S.; et al. Global Trends in Social Prescribing: Web-Based Crawling Approach. J. Med. Internet Res. 2023, 25, e46537. [Google Scholar] [CrossRef]
- Duffull, S.B.; Wright, D.F.B.; Marra, C.A.; Anakin, M.G. A philosophical framework for pharmacy in the 21st century guided by ethical principles. Res. Soc. Adm. Pharm. 2018, 14, 309–316. [Google Scholar] [CrossRef]
- McDermott, I.; Astbury, J.; Jacobs, S.; Willis, S.; Hindi, A.; Seston, E.; Schafheutle, E. To be or not to be: The identity work of pharmacists as clinicians. Sociol. Health Illn. 2023, 45, 623–641. [Google Scholar] [CrossRef]
- Dinh, J.V.; Traylor, A.M.; Kilcullen, M.P.; Perez, J.A.; Schweissing, E.J.; Venkatesh, A.; Salas, E. Cross-Disciplinary Care: A Systematic Review on Teamwork Processes in Health Care. Small Group Res. 2019, 51, 125–166. [Google Scholar] [CrossRef]
- Daly, C.J.; Quinn, B.; Mak, A.; Jacobs, D.M. Community Pharmacists’ Perceptions of Patient Care Services within an Enhanced Service Network. Pharmacy 2020, 8, 172. [Google Scholar] [CrossRef]
- Hayhoe, B.; Cespedes, J.A.; Foley, K.; Majeed, A.; Ruzangi, J.; Greenfield, G. Impact of integrating pharmacists into primary care teams on health systems indicators: A systematic review. Br. J. Gen. Pract. 2019, 69, e665–e674. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.; Cartright, N.; Kirschner, J.; Nadarasa, A.; Rathbone, A.P.; Lindsey, L. Social prescribing in pharmacies: What is it, does it work and what does it mean for Canadian pharmacies? Can. Pharm. J. 2024, 157, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Lynch, M.; Spencer, L.H. A Systematic Review to Examine the Evidence in Developing Social Prescribing Interventions That Apply a Co-Productive, Co-Designed Approach to Improve Well-Being Outcomes in a Community Setting. Int. J. Environ. Res. Public Health 2021, 18, 3896. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Answer Alternatives | Number of Points | The Score Intervals for Competence |
|---|---|---|
| Very high | 5 | ≥4.5 |
| High | 4 | 3.5–4.4 |
| Average | 3 | 2.5–3.4 |
| Low | 2 | 1.5–2.4 |
| Very low | 1 | ≤1.4 |
| Hypotheses | Independent Variable | Dependent Variable | Statistical Analysis |
|---|---|---|---|
| H0: There is no significant relationship between competence in social prescribing or community referral and experience in the pharmacy profession | Experience in the pharmacy profession Type: Categorical ordinal | Competence in social referral Type: Continuous interval data | Linear regression |
| H0: There is no significant difference in social prescribing or community referral competence between pharmacists, provisional pharmacists, and pharmacy students | Education level Type: Categorical (independent groups) | Competence in social referral Type: Continuous interval data | Analysis of variance |
| H0: There is no significant difference between males and females in social prescribing or community referral competence | Gender Type: Categorical dichotomous | Competence in social referral Type: Continuous interval | Independent t-test (parametric) or Mann–Whitney U test (non-parametric) |
| Information | Answers | Number of Answers (Out of 96) | Percentage (%) |
|---|---|---|---|
| Gender | Woman | 76 | 79.2 |
| Man | 20 | 22.8 | |
| Other | 0 | 0 | |
| Do not want to answer | 0 | 0 | |
| Age | 18–24 | 22 | 22.9 |
| 25–34 | 39 | 40.6 | |
| 35–44 | 23 | 24. | |
| 45–54 | 8 | 8.3 | |
| 55 and over | 4 | 4.2 | |
| Education level | Provisional pharmacist | 38 | 39.6 |
| Prescription pharmacist | 47 | 49 | |
| Under pharmacy education | 11 | 11 | |
| Other | 0 | 0 | |
| Educational institution | UiT | 3 | 3.1 |
| OsloMet | 13 | 13.5 | |
| NTNU | 6 | 6.3 | |
| UiB | 4 | 4.2 | |
| Nord | 3 | 3.1 | |
| UiO | 8 | 8.3 | |
| Fully qualified pharmacist | 52 | 54.2 | |
| Fully trained pharmacist from abroad | 7 | 7.3 | |
| Workplace | Pharmacy | 88 | 91.7 |
| Industry | 2 | 2.1 | |
| Organization | 0 | 0 | |
| Other | 6 | 6.3 | |
| Experience | Under 1 year | 20 | 20.8 |
| 1–3 years | 15 | 15.6 | |
| 3–6 years | 19 | 19.8 | |
| 6–9 years | 12 | 12.5 | |
| 10 years and over | 30 | 31.3 | |
| District in Norway | East | 54 | 56.3 |
| West | 17 | 17.7 | |
| North | 10 | 10.4 | |
| Trøndelag | 12 | 12.5 | |
| South | 3 | 3.1 | |
| Position | Full time | 64 | 66.7 |
| Part-time | 7 | 7.3 | |
| On-call substitute | 25 | 26 | |
| Customer relations | Very good | 47 | 49 |
| Good | 43 | 44.8 | |
| Neutral | 6 | 6.3 | |
| Weak | 0 | 0 | |
| Very weak | 0 | 0 |
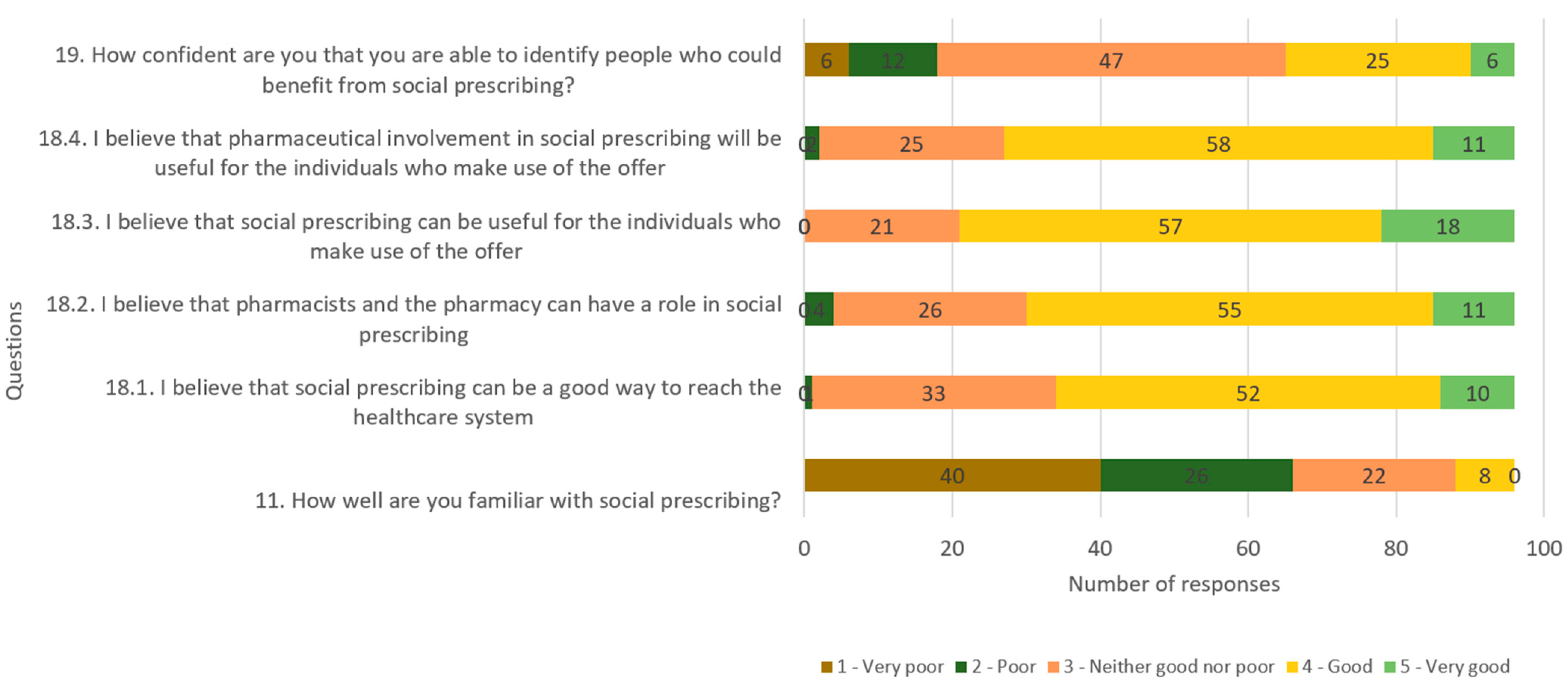
| Competence Question | Average Score (Out of 5) |
|---|---|
| How well are you familiar with social prescribing? | 1.98 |
| I believe that social prescribing can be a good way to reach the healthcare system. | 3.74 |
| I believe that pharmacists and the pharmacy can have a role in social prescribing. | 3.76 |
| I believe that social prescribing can be useful for the individuals who use the offer. | 3.97 |
| I believe that pharmaceutical involvement in social prescribing will be useful for the individuals who make use of the offer. | 3.81 |
| How confident are you that you are able to identify people who could benefit from social prescribing? | 3.14 |
| Hypothesis H0: | Statistical Analysis | Result |
|---|---|---|
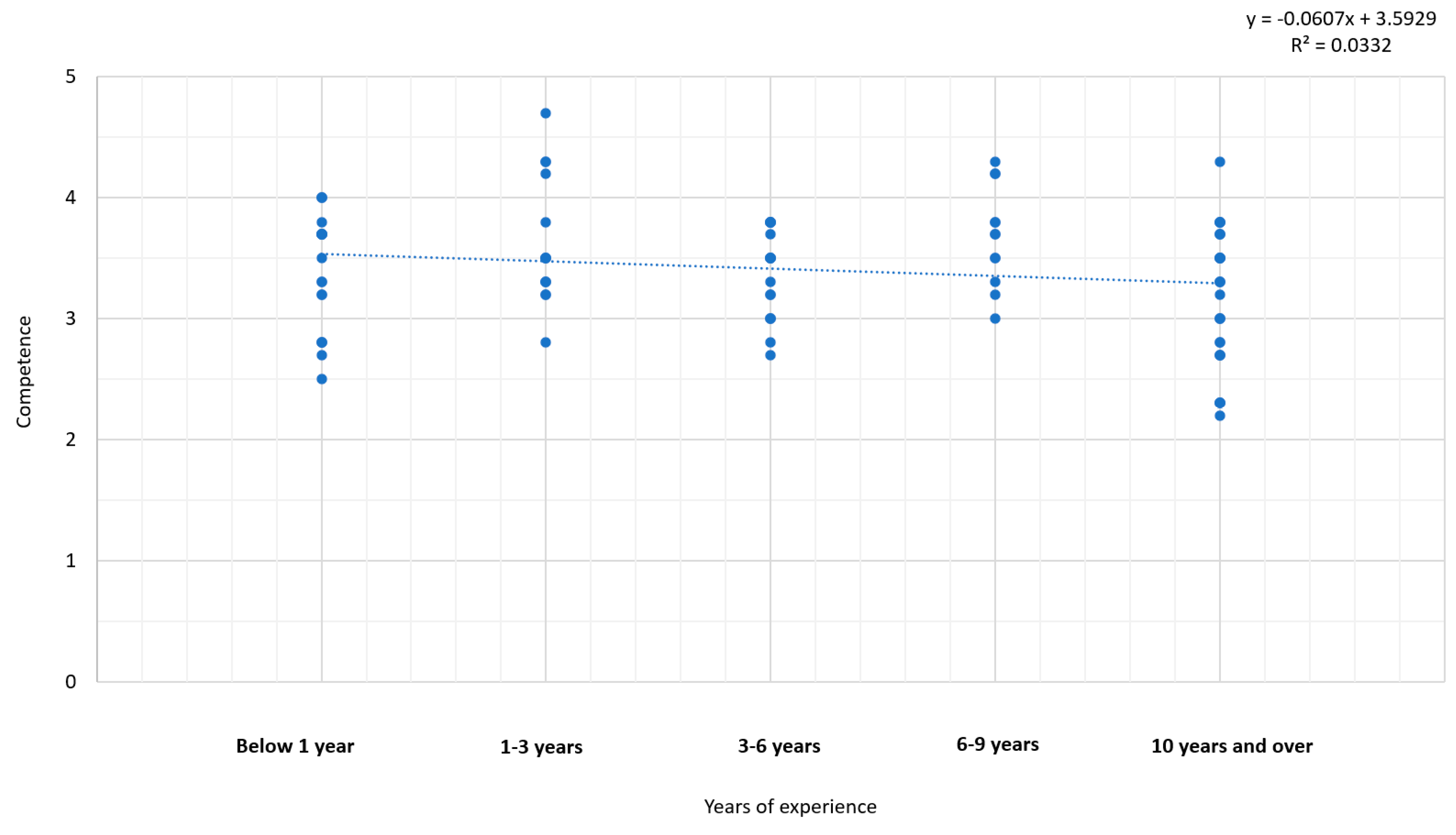
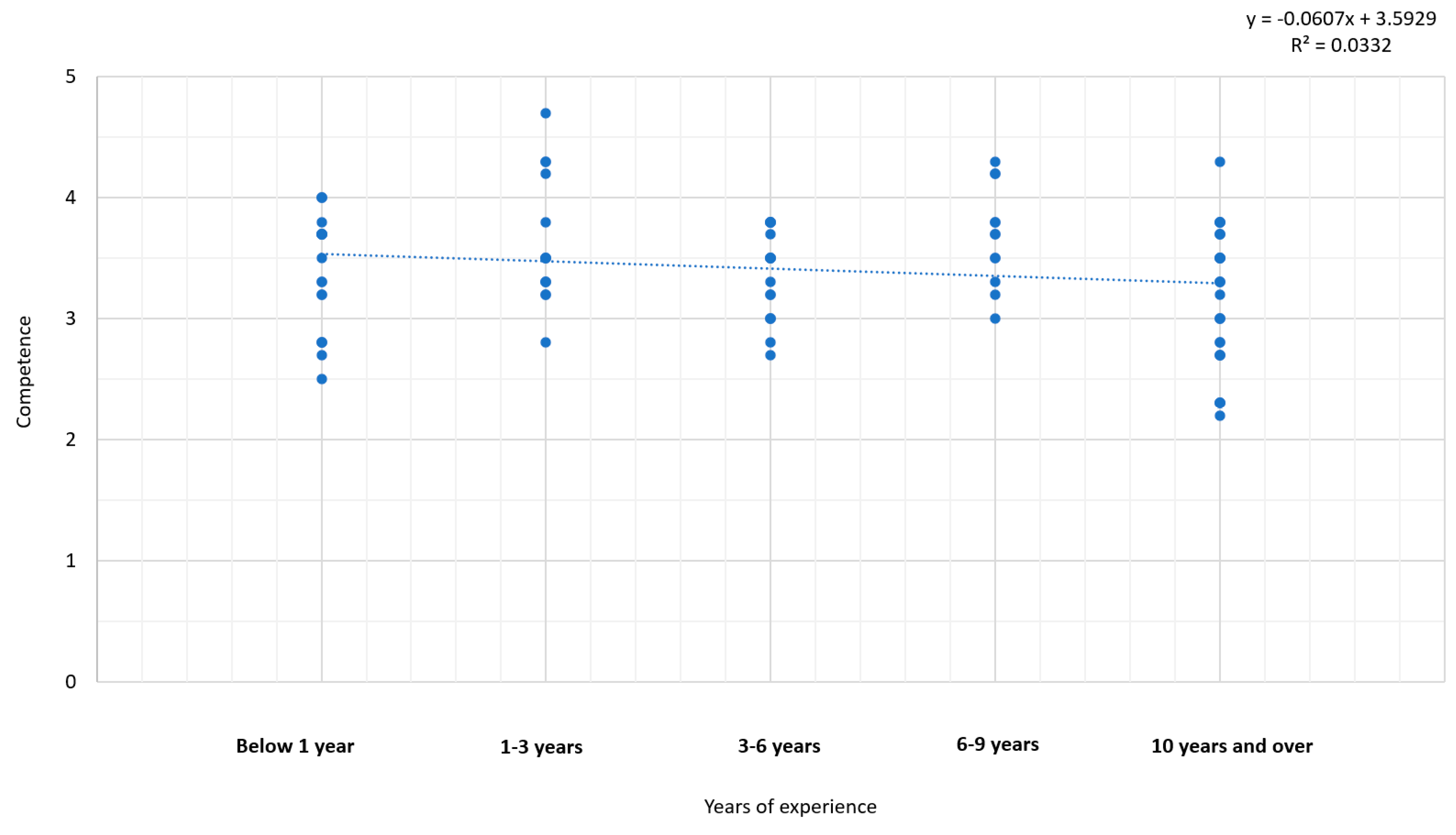
| H0 = There is no significant relationship between competence in social prescribing or community referral and experience in the pharmacy profession | Linear regression | No apparent association |
| H0 = There is no significant difference in competence about social prescribing or community referral between pharmacists, prescription pharmacists and students | Analysis of variance | No significant difference |
| H0 = There is no significant difference between competence within social prescribing or community referral and gender | Independent t-test | No significant difference |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabeyre, R.M.; Hussein, M.; Salih, S.; Amir, S.; Gazerani, P. Social Prescribing Competence among Community Pharmacists and Pharmacy Students in Norway. Pharmacy 2024, 12, 43. https://doi.org/10.3390/pharmacy12020043
Gabeyre RM, Hussein M, Salih S, Amir S, Gazerani P. Social Prescribing Competence among Community Pharmacists and Pharmacy Students in Norway. Pharmacy. 2024; 12(2):43. https://doi.org/10.3390/pharmacy12020043
Chicago/Turabian StyleGabeyre, Riyaan Mahamud, Misbah Hussein, Siedra Salih, Salia Amir, and Parisa Gazerani. 2024. "Social Prescribing Competence among Community Pharmacists and Pharmacy Students in Norway" Pharmacy 12, no. 2: 43. https://doi.org/10.3390/pharmacy12020043
APA StyleGabeyre, R. M., Hussein, M., Salih, S., Amir, S., & Gazerani, P. (2024). Social Prescribing Competence among Community Pharmacists and Pharmacy Students in Norway. Pharmacy, 12(2), 43. https://doi.org/10.3390/pharmacy12020043