
The Pharmacist’s Role in Managing COVID-19 in Chronic Kidney Disease Patients: A Review of Existing Strategies and Future Implications

 , , , ,
, , , ,
Abstract
:1. Introduction
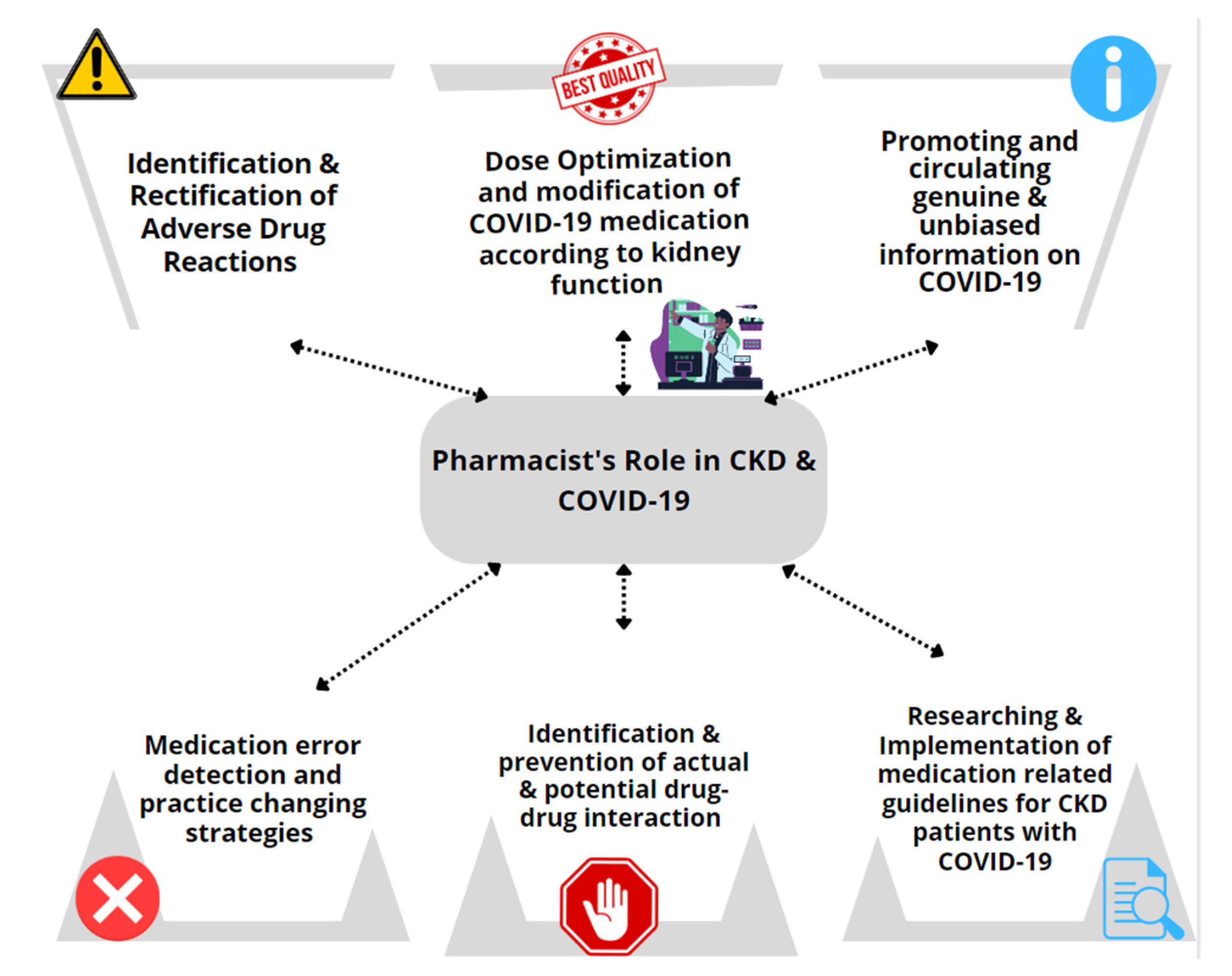
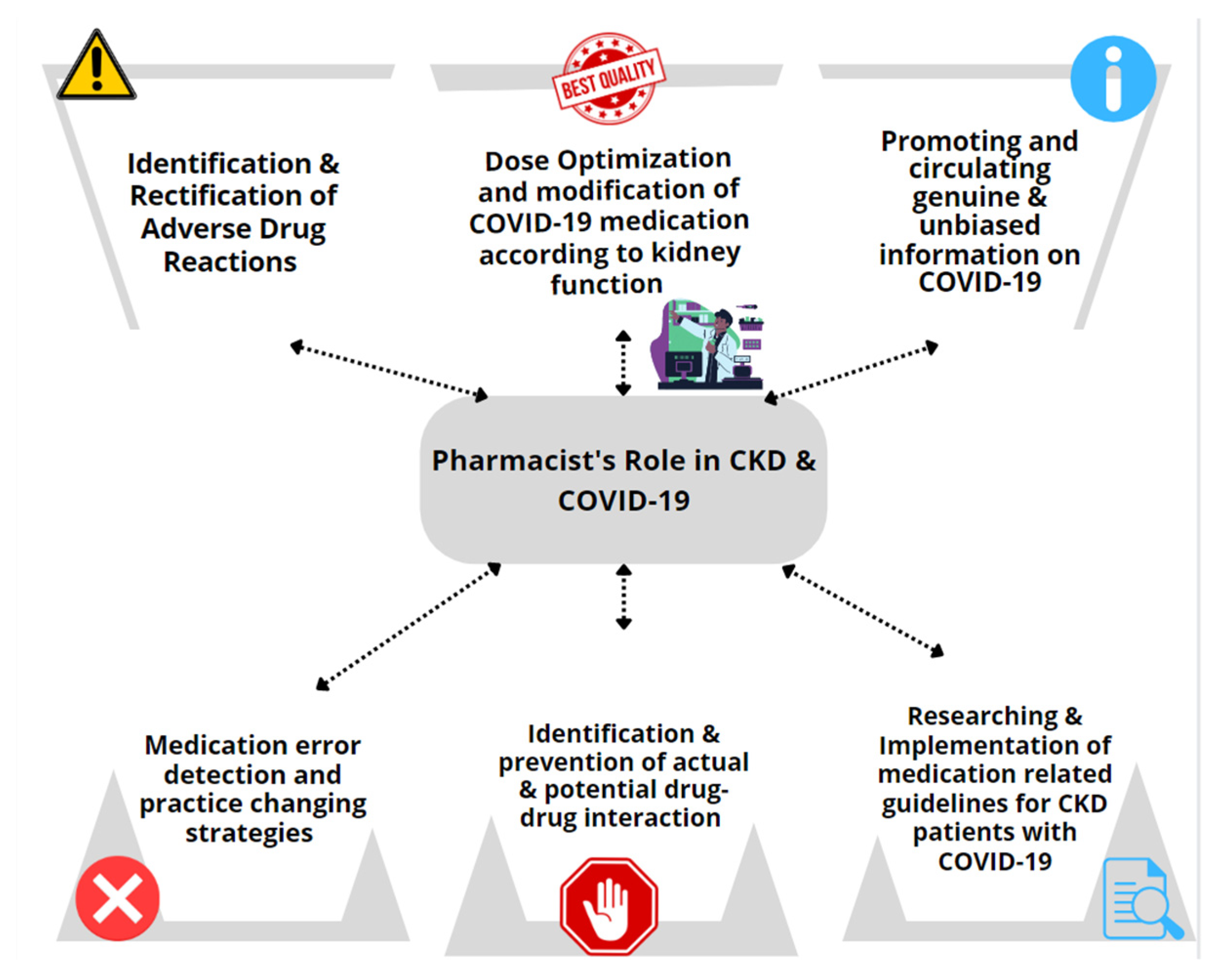
Role of Pharmacists toward CKD Patients during a Pandemic
2. Treating COVID-19 in CKD Patients: A Pharmacist’s Perspective
2.1. Identification of Adverse Drug Reactions and Drug-Related Errors
2.2. Counteracting Drug-Drug Interactions in COVID-19 Patients with CKD
2.3. Tele-Pharmacy Based Pharmaceutical Care Services for CKD Patients
2.4. Pharmacists Managed Home Delivery Service for CKD Patients
2.5. Prevention and Management Strategies for Pandemic Related Risks
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 12 July 2022).
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Rojas, M.A.; Vega-Vega, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Renal. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.-H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Jose, R.J.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Respir. Med. 2020, 8, e46–e47. [Google Scholar] [CrossRef]
- Naicker, S.; Yang, C.-W.; Hwang, S.-J.; Liu, B.-C.; Chen, J.-H.; Jha, V. The Novel Coronavirus 2019 epidemic and kidneys. Kidney Int. 2020, 97, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.M.; Friesner, D.L.; Rathke, A.M.; Doherty-Johnsen, S. Medication error reporting in rural critical access hospitals in the North Dakota Telepharmacy Project. Am. J. Health Syst. Pharm. 2014, 71, 58–67. [Google Scholar] [CrossRef]
- Okoro, R.N. COVID-19 pandemic: The role of community pharmacists in chronic kidney disease management supportive care. Res. Soc. Adm. Pharm. 2021, 17, 1925–1928. [Google Scholar] [CrossRef]
- Wang, D.; Liu, Y.; Zeng, F.; Shi, C.; Cheng, F.; Han, Y.; Zhang, Y. Evaluation of the role and usefulness of clinical pharmacists at the Fangcang Hospital during COVID-19 outbreak. Int. J. Clin. Pract. 2021, 75, e14271. [Google Scholar] [CrossRef]
- Zekan, L.; Mestrovic, A.; Perisin, A.S.; Bukic, J.; Leskur, D.; Rusic, D.; Modun, D. Improving community pharmacists’ clinical knowledge to detect and resolve drug-related problems in Croatia: A before/after survey study investigating the efficacy of an educational intervention. BMJ Open 2020, 10, e034674. [Google Scholar] [CrossRef]
- Menon, S.; Sander, J.W. Effects of the COVID-19 pandemic on medication adherence: In the case of antiseizure medications, A scoping review. Seizure 2021, 93, 81–87. [Google Scholar] [CrossRef]
- Saha, S.K.; Adhikary, A.; Jha, A. Enhancement in medication adherence amidst COVID-19 using active reminders. Eur. Phys. J. Spec. Top. 2022, 1–8. [Google Scholar] [CrossRef]
- Kretchy, I.A.; Asiedu-Danso, M.; Kretchy, J.-P. Medication management and adherence during the COVID-19 pandemic: Perspectives and experiences from low-and middle-income countries. Res. Soc. Adm. Pharm. 2021, 17, 2023–2026. [Google Scholar] [CrossRef]
- Li, H.; Radhakrishnan, J. A pharmacist-physician collaborative care model in chronic kidney disease. J. Clin. Hypertens. 2021, 23, 2026–2029. [Google Scholar] [CrossRef]
- Schütze, A.; Hohmann, C.; Haubitz, M.; Radziwill, R.; Benöhr, P. Medicines optimization for patients with chronic kidney disease in the outpatient setting: The role of the clinical pharmacist. Int. J. Pharm. Pract. 2021, 29, 587–597. [Google Scholar] [CrossRef]
- Aghili, M.; Kasturirangan, M.N. Management of Drug–Drug Interactions among Critically Ill Patients with Chronic Kidney Disease: Impact of Clinical Pharmacist’s Interventions. Indian J. Crit. Care Med. 2021, 25, 1226–1231. [Google Scholar] [CrossRef]
- Islahudin, F.; Lee, F.Y.; Kadir, T.N.I.T.A.; Abdullah, M.Z.; Makmor-Bakry, M. Continuous medication monitoring: A clinical model to predict adherence to medications among chronic kidney disease patients. Res. Soc. Adm. Pharm. 2021, 17, 1831–1840. [Google Scholar] [CrossRef]
- Liu, X.-X.; Wang, H.-X.; Hu, Y.-Y.; Zhu, X.-T.; Tan, X.; Yang, Y.; Hang, Y.-F.; Zhu, J.-G. Drug-related problems identified by clinical pharmacists in nephrology department of a tertiary hospital in China—A single center study. Ann. Palliat. Med. 2021, 10, 8701–8708. [Google Scholar] [CrossRef]
- Jonny; Violetta, L.; Kartasasmita, A.S.; Roesli, R.M.A.; Rita, C. Pharmacological Treatment Options for Coronavirus Disease-19 in Renal Patients. Int. J. Nephrol. 2021, 2021, e4078713. [Google Scholar] [CrossRef]
- Marra, F.; Smolders, E.J.; El-Sherif, O.; Boyle, A.; Davidson, K.; Sommerville, A.J.; Marzolini, C.; Siccardi, M.; Burger, D.; Gibbons, S.; et al. Recommendations for Dosing of Repurposed COVID-19 Medications in Patients with Renal and Hepatic Impairment. Drugs R D 2021, 21, 9–27. [Google Scholar] [CrossRef]
- Koshi, E.; Saito, S.; Okazaki, M.; Toyama, Y.; Ishimoto, T.; Kosugi, T.; Hiraiwa, H.; Jingushi, N.; Yamamoto, T.; Ozaki, M.; et al. Efficacy of favipiravir for an end stage renal disease patient on maintenance hemodialysis infected with novel coronavirus disease 2019. CEN Case Rep. 2020, 10, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Gök, S.; Bahçecioğlu, Ö.F.; Durmuş, M.; Gün, Z.Ü.; Ersoy, Y.; Aytemur, Z.A.; Ulutaş, Ö. The safety profile of favipiravir in COVID-19 patients with severe renal impairment. Int. J. Clin. Pract. 2021, 75, e14938. [Google Scholar] [CrossRef] [PubMed]
- Thakare, S.; Gandhi, C.; Modi, T.; Bose, S.; Deb, S.; Saxena, N.; Katyal, A.; Patil, A.; Patil, S.; Pajai, A.; et al. Safety of Remdesivir in Patients With Acute Kidney Injury or CKD. Kidney Int. Rep. 2020, 6, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.-Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Lê, M.P.; Le Hingrat, Q.; Jaquet, P.; Wicky, P.-H.; Bunel, V.; Massias, L.; Visseaux, B.; Messika, J.; Descamps, D.; Mal, H.; et al. Removal of Remdesivir’s Metabolite GS-441524 by Hemodialysis in a Double Lung Transplant Recipient with COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01521-20. [Google Scholar] [CrossRef]
- Hiremath, S.; McGuinty, M.; Argyropoulos, C.; Brimble, K.S.; Brown, P.A.; Chagla, Z.; Cooper, R.; Hoar, S.; Juurlink, D.; Treleaven, D.; et al. Prescribing Nirmatrelvir/Ritonavir for COVID-19 in Advanced CKD. Clin. J. Am. Soc. Nephrol. 2022, 17, 1–4. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Ltd, B.P.G. Two New Oral Antivirals for COVID-19: ▼Molnupiravir and ▼Nirmatrelvir Plus Ritonavir. DTB 2022, 60, 73–77. [Google Scholar]
- Lopinavir and Ritonavir: Drug Information–UpToDate. Available online: https://www.uptodate.com/contents/lopinavir-and-ritonavir-drug-information (accessed on 7 June 2022).
- Information on COVID-19 Treatment, Prevention and Research. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 7 June 2022).
- Lescure, F.-X.; Honda, H.; Fowler, R.A.; Lazar, J.S.; Shi, G.; Wung, P.; Patel, N.; Hagino, O.; Bazzalo, I.J.; Casas, M.M.; et al. Sarilumab in patients admitted to hospital with severe or critical COVID-19: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 522–532. [Google Scholar] [CrossRef]
- Commissioner O of the Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal Antibody for Treatment of COVID-19. FDA 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-monoclonal-antibody-treatment-covid-19 (accessed on 7 June 2022).
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Saeed, B. Impact of COVID-19 Pandemic on Management of Pediatric Kidney Transplant Recipients. Exp. Clin. Transplant. 2021, 19, 894–898. [Google Scholar] [CrossRef]
- Shafiee, M.A.; Hosseini, S.F.; Mortazavi, M.; Emami, A.; Zadeh, M.M.; Moradi, S.; Shaker, P. Anticoagulation therapy in COVID-19 patients with chronic kidney disease. J. Res. Med Sci. 2021, 26, 63. [Google Scholar] [CrossRef]
- Moores, L.K.; Tritschler, T.; Brosnahan, S.; Carrier, M.; Collen, J.F.; Doerschug, K.; Holley, A.B.; Jimenez, D.; Le Gal, G.; Rali, P.; et al. Prevention, Diagnosis, and Treatment of VTE in Patients With Coronavirus Disease 2019: CHEST Guideline and Expert Panel Report. Chest 2020, 158, 1143–1163. [Google Scholar] [CrossRef]
- Pawar, A.; Gagne, J.J.; Gopalakrishnan, C.; Iyer, G.; Tesfaye, H.; Brill, G.; Chin, K.; Bykov, K. Association of Type of Oral Anticoagulant Dispensed With Adverse Clinical Outcomes in Patients Extending Anticoagulation Therapy Beyond 90 Days After Hospitalization for Venous Thromboembolism. JAMA 2022, 327, 1051–1060. [Google Scholar] [CrossRef]
- Li, J.; Li, S.-X.; Zhao, L.-F.; Kong, D.-L.; Guo, Z.-Y. Management recommendations for patients with chronic kidney disease during the novel coronavirus disease 2019 (COVID-19) epidemic. Chronic Dis. Transl. Med. 2020, 6, 119–123. [Google Scholar] [CrossRef]
- Lee, J.Y.; Ang, A.S.Y.; Ali, N.M.; Ang, L.M.; Omar, A. Incidence of adverse reaction of drugs used in COVID-19 management: A retrospective, observational study. J. Pharm. Policy Pract. 2021, 14, 84. [Google Scholar] [CrossRef]
- Melo, J.R.R.; Duarte, E.C.; de Moraes, M.V.; Fleck, K.; Silva, A.S.D.N.E.; Arrais, P.S.D. Adverse drug reactions in patients with COVID-19 in Brazil: Analysis of spontaneous notifications of the Brazilian pharmacovigilance system. Cad. Saude Publica 2021, 37, e00245820. [Google Scholar] [CrossRef]
- Marquito, A.B.; Fernandes, N.M.; Colugnati, F.A.; Paula, R.B. Identifying potential drug interactions in chronic kidney disease patients. Brazilian J. Nephrol. 2014, 36, 26–34. [Google Scholar] [CrossRef]
- Teoli, D.; Thompson, V.; Wright, J.; Ho, I.; Vlaminck, B.; Miller, G.; Feely, M. Acute Pain Crisis Caused by Tramadol Remdesivir Drug–Drug Interaction. J. Palliat. Med. 2021, 24, 1582–1584. [Google Scholar] [CrossRef]
- Johnstone, L. Telepharmacy and chronic kidney disease—A Making Tracks investment strategy. In Proceedings of the 14th National Rural Health Conference, Canberra, Australia, 26–29 March 2017; pp. 26–29. [Google Scholar]
- Divyaveer, S.; Jha, V. COVID-19 and care for patients with chronic kidney disease: Challenges and lessons. FASEB BioAdv. 2021, 3, 569–576. [Google Scholar] [CrossRef]
- Kilova, K.; Mihaylova, A.; Peikova, L. Opportunities of information communication technologies for providing pharmaceutical care in the COVID-19 pandemic. Pharmacia 2021, 68, 9–14. [Google Scholar] [CrossRef]
- Omboni, S.; Tenti, M. Telepharmacy for the management of cardiovascular patients in the community. Trends Cardiovasc. Med. 2019, 29, 109–117. [Google Scholar] [CrossRef]
- Margolis, K.L.; Asche, S.E.; Bergdall, A.R.; Dehmer, S.P.; Groen, S.E.; Kadrmas, H.M.; Kerby, T.J.; Klotzle, K.J.; Maciosek, M.; Michels, R.D.; et al. Effect of Home Blood Pressure Telemonitoring and Pharmacist Management on Blood Pressure Control: A cluster randomized clinical trial. JAMA 2013, 310, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Amkreutz, J.; Lenssen, R.; Marx, G.; Deisz, R.; Eisert, A. Medication safety in a German telemedicine centre: Implementation of a telepharmaceutical expert consultation in addition to existing tele-intensive care unit services. J. Telemed. Telecare 2020, 26, 105–112. [Google Scholar] [CrossRef]
- Bejarano, A.P.; Santos, P.V.; Robustillo-Cortés, M.D.L.A.; Gómez, E.S.; Rubio, M.D.S. Implementation of a novel home delivery service during pandemic. Eur. J. Hosp. Pharm. 2021, 28, e120–e123. [Google Scholar] [CrossRef]
- Surapat, B.; Sungkanuparph, S.; Kirdlarp, S.; Lekpittaya, N.; Chunnguleum, K. Role of clinical pharmacists in telemonitoring for patients with Coronavirus Disease 2019 (COVID-19). J. Clin. Pharm. Ther. 2021, 46, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Chaomuang, N.; Dede, A.J.O.; Saokaew, S.; Umnuaypornlert, A. Effects of home drug delivery on drug-related problems: Preliminary evidence for improved patient outcomes during the COVID-19 pandemic in Thailand. J. Am. Pharm. Assoc. 2022, 62, 1206–1213.e3. [Google Scholar] [CrossRef] [PubMed]
- Mash, R.J.; Schouw, D.; Daviaud, E.; Besada, D.; Roman, D. Evaluating the implementation of home delivery of medication by community health workers during the COVID-19 pandemic in Cape Town, South Africa: A convergent mixed methods study. BMC Health Serv. Res. 2022, 22, 98. [Google Scholar] [CrossRef] [PubMed]
- AlAbbasi, H.K.; Thorakkattil, S.A.; Mohiuddin, S.I.; Nemr, H.S.; Jabbour, R.; Al-Ghamdi, F. Implementation and effectiveness of drive-through medication pick-up and home delivery services. A patient safety initiative during COVID-19 pandemic. J. Patient Saf. Risk Manag. 2021, 26, 179–186. [Google Scholar] [CrossRef]
- Chang, C.-H.; Fan, P.-C.; Kuo, G.; Lin, Y.-S.; Tsai, T.-Y.; Chang, S.-W.; Tian, Y.-C.; Lee, C.-C. Infection in Advanced Chronic Kidney Disease and Subsequent Adverse Outcomes after Dialysis Initiation: A Nationwide Cohort Study. Sci. Rep. 2020, 10, 2938. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Sl No. | Medication | Usual Adult Dose | Renal Dose Modification |
|---|---|---|---|
| 1 | Favipiravir | 1.6 g, twice daily, on day 1, followed by 600 mg, twice daily, orally, for 7 to 14 days | Mild to moderate impairment: No dose adjustment required eGFR < 30 mL/min: avoid Dialysis: blood concentration of favipiravir in patients on hemodialysis similar to those with normal kidney function, suggesting it’s use in CKD. |
| 2 | Remdesivir | For hospitalized patients: 200 mg on day 1 and 100 mg daily for 5 days or until discharge. For non-hospitalized patients: 200 mg on day 1 and 100 mg on days 2 and 3 | CrCl ≥ 30 mL/min: No dose adjustment required CrCl < 30 mL/min: Manufactures do not recommend remdesivir. Significant toxicity unlikely with short term treatment (5 to 10 days) Dialysis: remdesivir at recommended doses do not normally increase serum creatinine including in patients on dialysis |
| 3 | Molnupiravir | 800 mg every 12 h for 5 days | No dose adjustment recommended |
| 4 | Nirmatrelvir and Ritonavir | CrCl ≥ 60 mL/min: Nirmatrelvir 300 mg and ritonavir 100 mg every 12 h for 5 days | CrCl 30 to <60 mL/min: nirmatrelvir 150 mg & ritonavir 100 mg, every 12 h for 5 days CrCl is <30 mL/min: Not recommended Dialysis: Not recommended Some guidelines propose nirmatrelvir 300 mg and ritonavir 100 mg on day 1, then nirmatrelvir 150 mg and ritonavir 100 mg, once daily, for 4 more days when CrCl < 30 mL/min and dialysis (dose after dialysis) |
| 5 | Sotrovimab | 500 mg IV as a single dose | No dose adjustment recommended |
| 6 | Casirivimab and Imdevimab | IV, subcutaneous: casirivimab 600 mg and imdevimab 600 mg as a single dose | No dose adjustment recommended |
| 7 | Tocilizumab | IV: 8 mg/kg once, second dose may be considered ≥ 8 h if no clinical improvement | Mild to moderate impairment: No dose adjustment recommended Severe impairment: No dose adjustment noted in the manufacturer’s label (no data), including in patients on dialysis. But significant renal elimination unlikely because of its molecular weight |
| 8 | Sarilumab | 400 mg IV once | No dose adjustment recommended |
| 9 | Balmanivimab/Etesevimab | Balmanivimab 700 mg, etesevimab 1.4 g, IV single dose | No dose adjustment recommended |
| 10 | Baricitinib | CrCl ≥ 60 mL/min: 4 mg, once daily, oral, for 14 days | CrCl 30 to <60 mL/min: 2 mg, once daily, orally. CrCl 15 to <30 mL/min: 1 mg, once daily, orally. CrCl < 15 mL/min or Hemodialysis: not recommended |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karattuthodi, M.S.; Thorakkattil, S.A.; Abdulsalim, S.; Sridhar, S.B.; Parakkal, S.A.; Arain, S.; Madathil, H.; Karumbaru Kuzhiyil, A.; Mohammed Ahmed Ageeli, M.; Unnikrishnan, M.K. The Pharmacist’s Role in Managing COVID-19 in Chronic Kidney Disease Patients: A Review of Existing Strategies and Future Implications. Pharmacy 2022, 10, 94. https://doi.org/10.3390/pharmacy10040094
Karattuthodi MS, Thorakkattil SA, Abdulsalim S, Sridhar SB, Parakkal SA, Arain S, Madathil H, Karumbaru Kuzhiyil A, Mohammed Ahmed Ageeli M, Unnikrishnan MK. The Pharmacist’s Role in Managing COVID-19 in Chronic Kidney Disease Patients: A Review of Existing Strategies and Future Implications. Pharmacy. 2022; 10(4):94. https://doi.org/10.3390/pharmacy10040094
Chicago/Turabian StyleKarattuthodi, Mohammed Salim, Shabeer Ali Thorakkattil, Suhaj Abdulsalim, Sathvik Belagodu Sridhar, Sainul Abideen Parakkal, Savera Arain, Hafees Madathil, Ajmal Karumbaru Kuzhiyil, Mamdouh Mohammed Ahmed Ageeli, and Mazhuvanchery Kesavan Unnikrishnan. 2022. "The Pharmacist’s Role in Managing COVID-19 in Chronic Kidney Disease Patients: A Review of Existing Strategies and Future Implications" Pharmacy 10, no. 4: 94. https://doi.org/10.3390/pharmacy10040094
APA StyleKarattuthodi, M. S., Thorakkattil, S. A., Abdulsalim, S., Sridhar, S. B., Parakkal, S. A., Arain, S., Madathil, H., Karumbaru Kuzhiyil, A., Mohammed Ahmed Ageeli, M., & Unnikrishnan, M. K. (2022). The Pharmacist’s Role in Managing COVID-19 in Chronic Kidney Disease Patients: A Review of Existing Strategies and Future Implications. Pharmacy, 10(4), 94. https://doi.org/10.3390/pharmacy10040094