
Racial/Ethnic Health Disparity in the U.S.: A Decomposition Analysis



Abstract
1. Introduction
2. Data
3. Methods
4. Results
4.1. Coefficient Estimates
4.2. Decomposition Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Descriptive Statistics



{kind=link}
{kind=link}
| Variable | Race/Ethnicity | ||||||
|---|---|---|---|---|---|---|---|
| N | All | White | Black | Hispanic | Asian | AIAN | |
| Reported age in years | 1,212,890 | 45.07 | 46.81 | 42.23 | 39.14 | 38.82 | 42.51 |
| Gender (male = 1) | 1,212,890 | 0.494 | 0.495 | 0.448 | 0.507 | 0.547 | 0.534 |
| Marital status | 1,212,889 | 0.591 | 0.626 | 0.391 | 0.552 | 0.610 | 0.506 |
| Education: | 1,212,890 | ||||||
| Grade 8 or less | 0.041 | 0.020 | 0.035 | 0.169 | 0.010 | 0.048 | |
| Grades 9–11 (Some high school) | 0.076 | 0.060 | 0.110 | 0.145 | 0.031 | 0.128 | |
| Grade 12 or GED (High school graduate) | 0.307 | 0.308 | 0.361 | 0.298 | 0.162 | 0.349 | |
| College 1 year to 3 years | 0.274 | 0.282 | 0.289 | 0.227 | 0.221 | 0.297 | |
| College 4 years or more | 0.302 | 0.331 | 0.205 | 0.162 | 0.576 | 0.178 | |
| Employment: * | 1,211,418 | ||||||
| Employed for wages | 0.551 | 0.543 | 0.578 | 0.569 | 0.601 | 0.519 | |
| Self-employed | 0.085 | 0.091 | 0.057 | 0.074 | 0.076 | 0.093 | |
| Out of work for more than 1 year | 0.016 | 0.013 | 0.032 | 0.023 | 0.022 | 0.028 | |
| Out of work for less than 1 year | 0.031 | 0.024 | 0.054 | 0.047 | 0.039 | 0.044 | |
| A homemaker | 0.074 | 0.073 | 0.033 | 0.115 | 0.063 | 0.060 | |
| A student | 0.044 | 0.038 | 0.053 | 0.053 | 0.115 | 0.044 | |
| Retired | 0.159 | 0.184 | 0.124 | 0.071 | 0.069 | 0.118 | |
| Unable to work | 0.039 | 0.033 | 0.071 | 0.047 | 0.015 | 0.096 | |
| Annual Household Income ($1000) * | 1,068,122 | 52.88 | 57.53 | 39.41 | 35.41 | 62.57 | 40.80 |
| Have health plan | 1,212,890 | 0.859 | 0.894 | 0.808 | 0.701 | 0.869 | 0.765 |
| Smoking | 1,212,890 | 0.223 | 0.229 | 0.225 | 0.186 | 0.142 | 0.373 |
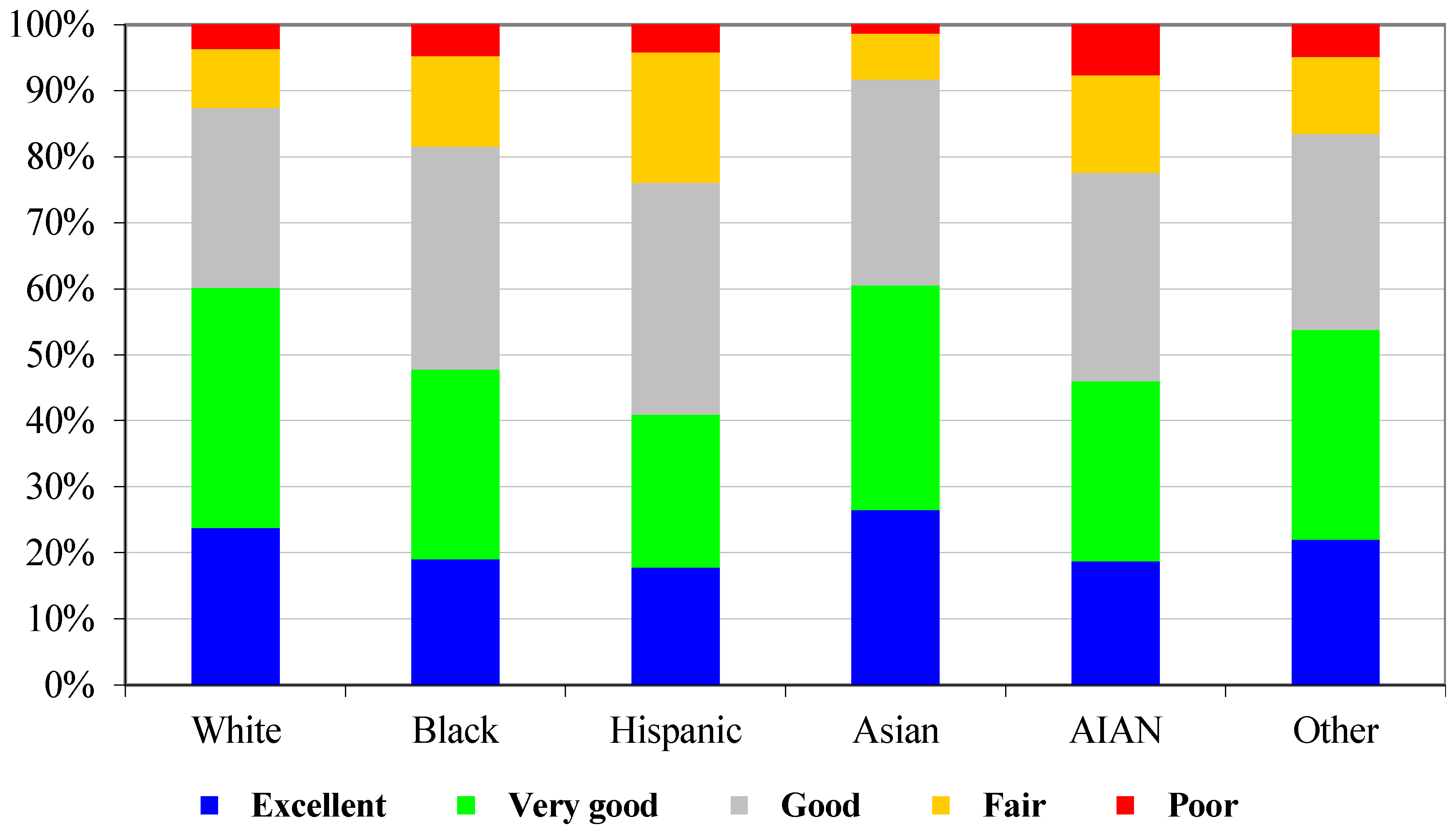
| Self-assessed health status: | 1,212,890 | ||||||
| Excellent | 0.226 | 0.238 | 0.191 | 0.178 | 0.265 | 0.188 | |
| Very good | 0.338 | 0.364 | 0.287 | 0.232 | 0.340 | 0.272 | |
| Good | 0.291 | 0.273 | 0.338 | 0.351 | 0.312 | 0.316 | |
| Fair | 0.108 | 0.089 | 0.137 | 0.198 | 0.069 | 0.148 | |
| Poor | 0.038 | 0.037 | 0.048 | 0.042 | 0.014 | 0.077 | |
| (a): Coefficient estimates of the scale function to control for heteroskedasticity | |||||||
| Variable | Coefficient Estimate | Standard Error | p-value | ||||
| Gender (male = 1) | 0.1804 | 0.0076 | 0.0000 | ||||
| Age 18–24 | −0.0376 | 0.0189 | 0.0473 | ||||
| Age 25–29 | −0.0767 | 0.0198 | 0.0001 | ||||
| Age 30–34 | −0.0882 | 0.0193 | 0.0000 | ||||
| Age 35–39 | −0.0792 | 0.0182 | 0.0000 | ||||
| Age 40–44 | −0.0873 | 0.0180 | 0.0000 | ||||
| Age 45–49 | −0.0466 | 0.0181 | 0.0102 | ||||
| Age 55–59 | 0.1123 | 0.0176 | 0.0000 | ||||
| Age 60–64 | 0.1879 | 0.0178 | 0.0000 | ||||
| Age 65–69 | 0.1937 | 0.0194 | 0.0000 | ||||
| Age 70–74 | 0.2423 | 0.0185 | 0.0000 | ||||
| Age 75–79 | 0.3340 | 0.0188 | 0.0000 | ||||
| Age 80–84 | 0.4545 | 0.0216 | 0.0000 | ||||
| Age ≥ 85 | 0.6140 | 0.0267 | 0.0000 | ||||
| Black | 0.3515 | 0.0121 | 0.0000 | ||||
| Hispanic | 0.4024 | 0.0120 | 0.0000 | ||||
| Asian | 0.3715 | 0.0237 | 0.0000 | ||||
| AIAN | 0.4308 | 0.0247 | 0.0000 | ||||
| Annual Household Income ($1000) | −0.0031 | 0.0002 | 0.0000 | ||||
| Having health plan | −0.1716 | 0.0126 | 0.0000 | ||||
| Education higher than high school | −0.1647 | 0.0086 | 0.0000 | ||||
| Black | Hispanic | AIAN | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Component | Endowment | Coef. | Total | Endowment | Coef. | Total | Endowment | Coef. | Total | |
| Intercept | % | 30.1 | 30.1 | 39.7 | 39.7 | −27.7 | −27.7 | |||
| Age 25–29 | % | 0.6 | −1.6 | −1.0 | 1.0 | −0.4 | 0.6 | 0.4 | 0.3 | 0.7 |
| Age 30–34 | % | 0.7 | −1.4 | −0.7 | 1.3 | 0.1 | 1.4 | 0.2 | 1.8 | 1.9 |
| Age 35–39 | % | 0.5 | −1.1 | −0.6 | 1.2 | 0.8 | 2.0 | 0.2 | 4.2 | 4.4 |
| Age 40–44 | % | 0.2 | 2.1 | 2.3 | −0.3 | 0.9 | 0.6 | 0.4 | 4.5 | 4.9 |
| Age 45–49 | % | 0.2 | 4.5 | 4.7 | −1.1 | 1.5 | 0.4 | −0.3 | 5.2 | 5.0 |
| Age 50–54 | % | −1.2 | 5.1 | 3.9 | −2.6 | 0.9 | −1.7 | −1.1 | 3.3 | 2.2 |
| Age 55–59 | % | −1.8 | 4.3 | 2.5 | −3.2 | 0.8 | −2.4 | −0.3 | 3.2 | 2.8 |
| Age 60–64 | % | −1.3 | 3.6 | 2.4 | −2.9 | 0.3 | −2.7 | −0.3 | 2.2 | 1.9 |
| Age 65–69 | % | −1.6 | 2.5 | 0.9 | −3.6 | −0.3 | −3.9 | −1.2 | 1.2 | 0.1 |
| Age 70–74 | % | −4.0 | 0.4 | −3.5 | −4.3 | −0.2 | −4.6 | −3.7 | −0.1 | −3.8 |
| Age 75–79 | % | −5.5 | 0.0 | −5.4 | −4.9 | −0.4 | −5.3 | −4.7 | −0.8 | −5.5 |
| Age 80–84 | % | −3.6 | −0.3 | −3.8 | −3.4 | −0.2 | −3.6 | −2.5 | −0.4 | −2.9 |
| Age ≥ 85 | −1.8 | 0.0 | −1.8 | −1.9 | −0.1 | −1.9 | −1.0 | 0.0 | −1.0 | |
| Gender (male=1) | % | −1.2 | −26.1 | −27.3 | 0.3 | −14.2 | −13.9 | 0.4 | −16.7 | −16.3 |
| Smoking | % | 0.2 | −6.9 | −6.7 | −2.2 | −5.0 | −7.1 | 8.0 | −8.5 | −0.5 |
| Marital status | % | 2.8 | −0.2 | 2.6 | 0.5 | 3.7 | 4.2 | 1.1 | −1.8 | −0.7 |
| Grades 9–11 (Some high school) | % | −2.0 | −1.4 | −3.4 | −2.8 | −2.8 | −5.6 | −2.0 | 1.3 | −0.8 |
| Grade 12 or GED (High school graduate) | % | −7.8 | 8.6 | 0.7 | −1.3 | −3.7 | −5.0 | −5.2 | 7.0 | 1.8 |
| College 1 year to 3 years | % | −3.0 | 11.7 | 8.7 | 6.3 | −4.5 | 1.9 | −2.6 | 10.9 | 8.3 |
| College 4 years or more (College graduate) | % | 32.5 | 14.0 | 46.6 | 32.5 | −1.7 | 30.8 | 27.2 | 9.9 | 37.1 |
| Self-employed | % | 1.5 | 1.2 | 2.6 | 0.6 | 0.0 | 0.6 | −0.2 | 1.1 | 0.9 |
| Out of work | % | 3.5 | −1.7 | 1.8 | 1.9 | −2.2 | −0.3 | 1.5 | −2.1 | −0.6 |
| Homemaker | % | 0.0 | 0.8 | 0.8 | 0.0 | 1.3 | 1.3 | 0.0 | 0.8 | 0.8 |
| Student | % | −0.3 | 0.8 | 0.5 | −0.1 | 0.0 | −0.2 | −0.2 | 1.2 | 1.0 |
| Retired | % | −2.8 | 4.3 | 1.5 | −4.3 | 0.5 | −3.9 | −2.2 | 5.4 | 3.2 |
| Unable to work | % | 19.3 | −10.6 | 8.7 | 3.7 | −4.0 | −0.3 | 21.9 | −4.6 | 17.3 |
| Having health plan | % | 0.8 | −11.5 | −10.7 | 1.5 | −17.6 | −16.0 | 1.0 | 1.3 | 2.2 |
| Income pc $10k–$15k | % | −2.9 | 2.0 | −0.9 | −2.5 | −2.0 | −4.5 | −2.1 | 1.2 | −0.9 |
| Income pc $15k–$20k | % | −2.6 | 4.0 | 1.4 | −0.6 | −1.2 | −1.8 | −1.8 | 1.6 | −0.3 |
| Income pc $20k–$25k | % | −0.1 | 4.1 | 4.0 | 2.3 | −1.9 | 0.4 | −0.6 | −1.4 | −1.9 |
| Income pc $25k–$35k | % | 6.4 | 6.4 | 12.8 | 7.5 | −1.6 | 5.9 | 4.8 | 0.8 | 5.6 |
| Income pc $35k–$50k | % | 7.7 | 3.3 | 11.0 | 8.3 | −1.0 | 7.3 | 4.7 | −1.7 | 3.1 |
| Income pc $50k–$75k | % | 16.6 | 4.5 | 21.1 | 13.1 | −1.1 | 12.0 | 12.8 | −0.1 | 12.6 |
| Income pc ≥ $75k | % | 15.4 | 1.6 | 17.0 | 11.7 | −0.7 | 11.0 | 10.6 | −0.9 | 9.8 |
| County median household income | % | 2.8 | −11.4 | −8.6 | 1.0 | 22.1 | 23.1 | 2.1 | 37.7 | 39.9 |
| County income inequality | % | 0.8 | 13.1 | 13.9 | 1.0 | 24.8 | 25.8 | 0.4 | 0.2 | 0.5 |
| County percent Black | % | 1.5 | −16.7 | −15.2 | 0.0 | −3.1 | −3.1 | 0.0 | −1.1 | −1.1 |
| County percent Hispanic | % | −0.6 | 0.3 | −0.4 | −4.6 | 15.3 | 10.7 | −0.4 | 0.8 | 0.4 |
| County of metro areas of 1 million or more population | % | 1.8 | −14.0 | −12.2 | 1.3 | 7.0 | 8.3 | −0.7 | −3.9 | −4.6 |
| Total | 71.8 | 28.3 | 100.0 | 50.3 | 49.6 | 99.9 | 64.5 | 35.5 | 100.0 | |
| 1 | The terms “disparity” and “inequality” are used interchangeably in this paper. |
| 2 | We found that between 40% and 50% of the total health inequality in our sample is due to income-related health inequality—an estimate that is much higher than 25% reported by Wagstaff and van Doorslaer (2004) for Canada. |
| 3 | See, for instance, Williams and Collins (1995), Ayanian et al. (1999), and Shishehbor et al. (2006). |
| 4 | Van Doorslaer and Jones (2003) have shown that this heteroskedastic model accommodates possible individual-specific heterogeneity in the subjective thresholds. |
| 5 | One should be cautious about interpreting the contribution of each dummy coefficient in Table A2 since it is sensitive to the reference point selected in defining the dummy. However, the total contribution of a group of coefficients is not sensitive to the reference point. For example, the contribution of the coefficient of dummy for “unable to work” with “employed” as the reference point will be different from its contribution with “out of work” as the reference. |
References
- Adams, Peter, Michael Hurd, Daniel McFadden, Angela Merrill, and Tiago Ribeiro. 2003. Healthy, wealthy, and wise? Tests for direct causal between health and socioeconomic status. Journal of Econometrics 112: 3–56. [Google Scholar] [CrossRef]
- Adler, Nancy E., and Katherine Newman. 2002. Socioeconomic health disparities: Pathways and policies. Health Affairs 21: 60–76. [Google Scholar] [CrossRef]
- Adler, Nancy E., and Joan M. Ostrove. 1999. SES and health: What we know and what we do not. Annals of the New York Academy of Sciences 896: 3–5. [Google Scholar] [CrossRef] [PubMed]
- Ayanian, John Z., Joel S. Weissman, Scotte Chasan-Taber, and Arnold M. Epstein. 1999. Quality of care by race and gender for congestive heart failure and pneumonia. Medical Care 37: 1260–69. [Google Scholar] [CrossRef]
- Blinder, Alan. 1973. Wage Discrimination: Reduced Form and Structural Estimates. Journal of Human Resources 7: 436–55. [Google Scholar] [CrossRef]
- Bommier, Antoine, and Guy Stecklov. 2002. Defining health inequality: Why Rawls succeeds where social welfare theory fails. Journal of Health Economics 21: 497–513. [Google Scholar] [CrossRef]
- Bruner, Deborah W., Michele Jones, David Buchanan, and Jose Russo. 2006. Reducing cancer disparities for minorities: A multidisciplinary research agenda to improve patient access to health systems, clinical trials, and effective cancer therapy. Journal of Clinical Oncology 24: 2209–15. [Google Scholar] [CrossRef]
- Case, Anne, and Angus Deaton. 2020. Deaths of Despair and the Future of Capitalism. Princeton: Princeton University Press. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). 1999–2014. Behavioral Risk Factor Surveillance System Survey Questionnaire; Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
- Centers for Disease Control and Prevention (CDC). 2013. Health Disparities and Inequalities Report (CHDIR)—United States. MMWR 62 Suppl. 3. Available online: https://www.cdc.gov/minorityhealth/chdir/index.html (accessed on 28 April 2021).
- Charasse-Pouélé, Cecile, and Martin Fournier. 2006. Health disparities between racial groups in South Africa: A decomposition analysis. Social Science & Medicine 62: 2897–914. [Google Scholar]
- Cutler, David M., and Adriana Lleras-Muney. 2006. Education and Health: Evaluating Theories and evidence. In National Bureau of Economic Research Working Paper 12352. Cambridge: National Bureau of Economic Research. [Google Scholar]
- Cutler, David M., and Elizabeth Richardson. 1997. Measuring the health of the U.S. population. Brooking Papers on Economic Activity. Microeconomics 1997: 217–71. [Google Scholar] [CrossRef]
- Cutler, David M., and Elizabeth Richardson. 1998. The value of health: 1970–1990. American Economic Review 88: 97–100. [Google Scholar]
- Cutler, David M., Angus Deaton, and Adriana Lleras-Muney. 2006. The determinants of mortality. Journal of Economic Perspectives 20: 97–120. [Google Scholar] [CrossRef]
- Deaton, Angus. 2006. Global pattern of income and health: Facts, interpretation, and policies. In National Bureau of Economic Research Working Paper 12735. Cambridge: National Bureau of Economic Research. [Google Scholar]
- Deaton, Angus, and Darren Lubotsky. 2003. Mortality, inequality, and race in American cities and states. Social Science & Medicine 56: 1139–53. [Google Scholar]
- Diez-Roux, Ana. V., F. Javier Nieto, Laura Caulfield, Hermonn A. Tyroler, Robert L. Watson, and Moyses Szklo. 1999. Neighborhood differences in diet: The Atherosclerosis Risk in Communities (ARIC) study. Journal of Epidemiology and Community Health 53: 55–63. [Google Scholar] [CrossRef]
- Ecob, Russell, and Sally MacIntyre. 2000. Small area variations in health-related behaviors: Do these depend on the behavior itself, its measurement, or on personal characteristics? Health & Place 6: 261–74. [Google Scholar]
- Fairlie, R. W. 1999. The absence of the African-American owned business: An analysis of the dynamics of self-employment. Journal of Labor Economics 17: 80–108. [Google Scholar] [CrossRef]
- Fairlie, Robert W. 2005. An Extension of the Blinder-Oaxaca decomposition technique to Logit and Probit models. Journal of Economic and Social Measurement 30: 305–16. [Google Scholar] [CrossRef]
- Fiscella, Kevin, Peter Franks, Mark P. Doescher, and Barry G. Saver. 2002. Disparity in health care by race, ethnicity, and language among the insured: Findings from a national sample. Medical Care 40: 52–9. [Google Scholar] [CrossRef] [PubMed]
- Gomulka, Joanna, and Nicholas Stern. 1990. The employment of married woman in the United Kingdom 1970–1983. Economica 57: 171–99. [Google Scholar] [CrossRef]
- Groot, Wim. 2000. Adaptation and scale of reference bias in self-assessments of quality of life. Journal of Health Economics 19: 403–20. [Google Scholar] [CrossRef]
- Health Resources and Services Administration. 2009. Area Resource File; (ARF 2008 release). Washington, DC: U.S. Department of Health and Human Services.
- Hodgson, David C., Charles S. Fuchs, and John Z. Ayanian. 2001. Impact of patient and provider characteristics on the treatment and outcomes of colorectal cancer. Journal of the National Cancer Institute 93: 501–15. [Google Scholar] [CrossRef] [PubMed]
- Humphries, Karin H., and Eddy van Doorslaer. 2000. Income-related health inequality in Canada. Social Science Medicine 50: 663–71. [Google Scholar] [CrossRef]
- Idler, Ellen L., and Yael Benyamini. 1997. Self-rated health and mortality: A review of twenty-seven community studies. Journal of Health and Social Behavior 38: 21–37. [Google Scholar] [CrossRef]
- Institute of Medicine. 2002. Unequal Treatment: Controlling Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press. [Google Scholar]
- Kennedy, Bruce P., Ichiro Kawachi, Roberto Glass, and Deborah Prothrow-Stith. 1998. Income distribution, socioeconomic status, and self-rated health in the United States: Multilevel analysis. BMJ 317: 917–21. [Google Scholar] [CrossRef]
- Lahiri, Kajal, and Jijye Kim. 2021. American HALE at Midlife: An Analysis Based on HRS, under submission for publication.
- Lahiri, Kajal, and Zulkarnain Pulungan. 2007. Income Related Health Disparity and Its Determinants in New York State: Racial/Ethnic and Geographical Comparisons. In Toward Equity in Health: A New Global Approach to Inequities in Health. Edited by Barbara Wallace. Berlin/Heidelberg: Springer, pp. 97–127. [Google Scholar]
- Lahiri, Kajal, Denton R. Vaughan, and Bernard Wixon. 1995. Modeling SSA’s sequential disability determination process using matched SIPP data. Social Security Bulletin 58: 1–41. [Google Scholar]
- Lee, A. James, Lee Analytics, Colin S. Baker, Stephen Gehlbach, David Hosmer, and Monika Reti. 1998. Do black elderly Medicare patients receive fewer services? An analysis of the procedure used for selected patient conditions. Medical Care Research and Review 55: 314–33. [Google Scholar] [CrossRef]
- Manor, Orly, Shirley Matthews, and Chris Power. 2001. Self-rated health and limiting longstanding illness: Inter-relationships with morbidity in early adulthood. International Journal of Epidemiology 30: 600–7. [Google Scholar] [CrossRef]
- McKelvey, Richard, and William Zavoina. 1975. A statistical model for the analysis of ordinal level-dependent variables. Journal of Mathematical Sociology 4: 103–20. [Google Scholar] [CrossRef]
- Oaxaca, Ronald. 1973. Male-Female Wage Differentials in Urban Labor Market. International Economic Review 14: 693–709. [Google Scholar] [CrossRef]
- Rawls, John. 1971. A Theory of Justice. Cambridge: Harvard University Press. [Google Scholar]
- Rubin, Donald B. 1987. Multiple Imputation for Nonresponse in Surveys. New York: John Wiley. [Google Scholar]
- Safaei, Jahl. 2007. Income and health inequality across Canadian provinces. Health & Place 13: 629–38. [Google Scholar]
- Schafer, Joseph L. 1997. Analysis of Incomplete Multivariate Data. New York: Chapman and Hall. [Google Scholar]
- Shishehbor, Mehdi H., David Litaker, Claire E. Pothier, and Michael S. Lauer. 2006. Association of socioeconomic status with functional capacity, heart rate recovery, and all-cause mortality. Journal of American Medical Association 295: 784–92. [Google Scholar] [CrossRef]
- Sickles, Robin C., and Paul Taubman. 1997. Mortality and morbidity among adults and elderly. In Handbook of Population and Family Economics. Edited by Mark R. Rosenzweig and Oded Stark. Amsterdam: North-Holland, pp. 559–643. [Google Scholar]
- Soobader, Mah-J., and Felicia B. LeClere. 1999. Aggregation and the measurement of income inequality: Effects on morbidity. Social Science & Medicine 48: 733–44. [Google Scholar]
- Subramanian, Sabu V., and Ichiro Kawachi. 2003. The association between state income inequality and worse health is not confounded by race. International Journal of Epidemiology 32: 1022–28. [Google Scholar] [CrossRef]
- Subramanian, Sabu V., and Ichiro Kawachi. 2004. Income inequality and health: What have we learned so far? Epidemiologic Reviews 26: 78–91. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, Sabu V., and Ichiro Kawachi. 2006. Whose health is affected by income inequality? A multilevel interaction analysis of contemporaneous and lagged effects of state income inequality on individual self-rated health in the United States. Health & Place 12: 141–56. [Google Scholar]
- U.S. Department of Health and Human Services (US-DHHS). 2020. Healthy People 2020; Washington, DC: US-DHHS. Available online: https://www.cdc.gov/nchs/healthy_people/hp2020.htm (accessed on 3 April 2021).
- Van Doorslaer, Eddy, and Andrew M. Jones. 2003. Inequalities in self-reported health: Validation of a new approach to measurement. Journal of Health Economics 22: 61–87. [Google Scholar] [CrossRef]
- Van Ourti, Tom, Eddy van Doorslaer, and Xander Koolman. 2006. The Effect of Growth and Inequality in Incomes on Health Inequality: Theory and Empirical Evidence from the European Panel. Tinbergen Institute Discussion Paper, TI 2006-108/3. Rotterdam: Erasmus University. [Google Scholar]
- Wagstaff, Adam, and Eddy van Doorslaer. 2004. Overall versus socioeconomic health inequality: A measurement framework and two empirical illustrations. Health Economics 13: 297–301. [Google Scholar] [CrossRef]
- Wenzlow, Audra T., John Mullahy, and Barbara L. Wolfe. 2004. Understanding Racial Disparity in Health: The Income-Wealth Paradox. Discussion Paper No. 1283-04. Madison: Institute on Research on Poverty, University of Wisconsin. [Google Scholar]
- Wilkinson, Richard G. 1992. Income distribution and life expectancy. British Medical Journal 304: 165–68. [Google Scholar] [CrossRef]
- Wilkinson, Richard G., and Kate E. Pickett. 2006. Income inequality and population health: A review and explanation of the evidence. Social Science & Medicine 62: 1768–84. [Google Scholar]
- Williams, David R., and Chiquita Collins. 1995. US socioeconomic and racial differences in health: Patterns and explanations. Annual Review of Sociology 21: 349–86. [Google Scholar] [CrossRef]
| Coefficient Estimate | |||||
|---|---|---|---|---|---|
| Variable | White | Black | Hispanic | Asian | AIAN |
| Intercept | 2.767 | 2.633 | 2.502 | 3.509 | 2.943 |
| Age 25–29 | −0.105 | −0.038 | −0.087 | −0.066 | −0.121 |
| Age 30–34 | −0.182 | −0.126 | −0.188 | −0.143 | −0.292 |
| Age 35–39 | −0.252 | −0.207 | −0.290 | −0.208 | −0.501 |
| Age 40–44 | −0.354 | −0.433 | −0.408 | −0.334 | −0.594 |
| Age 45–49 | −0.507 | −0.701 | −0.618 | −0.462 | −0.845 |
| Age 50–54 | −0.647 | −0.913 | −0.738 | −0.548 | −0.904 |
| Age 55–59 | −0.728 | −1.029 | −0.847 | −0.703 | −1.007 |
| Age 60–64 | −0.733 | −1.063 | −0.788 | −0.792 | −0.994 |
| Age 65–69 | −0.858 | −1.115 | −0.761 | −0.708 | −1.039 |
| Age 70–74 | −1.040 | −1.108 | −0.964 | −0.780 | −1.017 |
| Age 75–79 | −1.245 | −1.253 | −1.032 | −0.846 | −0.932 |
| Age 80–84 | −1.328 | −1.214 | −1.115 | −1.118 | −1.115 |
| Age ≥ 85 | −1.347 | −1.342 | −1.099 | −1.099 | −1.342 |
| Gender (male = 1) | −0.090 | 0.175 | 0.093 | 0.042 | 0.112 |
| Smoking | −0.385 | −0.250 | −0.210 | −0.278 | −0.235 |
| Marital status | 0.055 | 0.057 | 0.010 n | 0.037 | 0.078 |
| Grades 9–11 (Some high school) | 0.190 | 0.255 | 0.319 | 0.010 n | 0.122 n |
| Grade 12 or GED (High school graduate) | 0.552 | 0.439 | 0.636 | 0.179 | 0.420 |
| College 1 year to 3 years | 0.704 | 0.534 | 0.836 | 0.323 | 0.481 |
| College 4 years or more (College graduate) | 1.007 | 0.733 | 1.080 | 0.540 | 0.692 |
| Self-employed | 0.213 | 0.125 | 0.214 | 0.225 | 0.138 |
| Out of work | −0.367 | −0.273 | −0.161 | −0.128 | −0.159 |
| A homemaker | 0.002 n | −0.113 | −0.086 | −0.091 | −0.089 |
| A student | 0.128 | 0.048 | 0.130 | 0.034 n | −0.037 n |
| Retired | −0.266 | −0.424 | −0.319 | −0.198 | −0.568 |
| Unable to work | −2.384 | −1.684 | −1.741 | −1.615 | −2.058 |
| Having health plan | 0.045 | 0.107 | 0.219 | 0.134 | 0.034 n |
| Income pc 10–15 | 0.176 | 0.121 | 0.248 | 0.063 | 0.129 |
| Income pc 15–20 | 0.340 | 0.214 | 0.409 | 0.212 | 0.270 |
| Income pc 20–25 | 0.450 | 0.298 | 0.605 | 0.244 | 0.519 |
| Income pc 25–35 | 0.576 | 0.370 | 0.683 | 0.335 | 0.538 |
| Income pc 35–50 | 0.680 | 0.508 | 0.810 | 0.480 | 0.796 |
| Income pc 50–75 | 0.865 | 0.630 | 0.972 | 0.659 | 0.873 |
| Income pc ≥ 75 | 0.939 | 0.745 | 1.105 | 0.723 | 1.079 |
| County median household income | 0.035 | 0.047 | 0.002 n | −0.037 | −0.021 n |
| County income inequality | −0.217 | −0.365 n | −0.622 | −1.173 | −0.220 n |
| County percent Black | −0.045 | 0.241 | 0.140 | 0.187 | 0.021 n |
| County percent Hispanic | 0.167 | 0.157 | −0.182 | 0.276 | 0.123 n |
| County of metro areas of 1 million pop. or more | −0.051 | 0.036 | −0.115 | 0.020 n | 0.002 n |
| McKelvey-Zavoina R2 = 0.46 | |||||
| White-Black | White-Hispanic | White-AIAN | |||||
|---|---|---|---|---|---|---|---|
| Component | Endow. | Coef. | Endow | Coef. | Endow | Coef. | |
| Age | (%) | −18.5 | 18.1 | −24.7 | 3.6 | −13.9 | 24.7 |
| Sex (male = 1) | (%) | −1.2 | −26.1 | 0.3 | −14.2 | 0.4 | −16.7 |
| Smoking | (%) | 0.2 | −6.9 | −2.2 | −5.0 | 8.0 | −8.5 |
| Marital status | (%) | 2.8 | −0.2 | 0.5 | 3.7 | 1.1 | −1.8 |
| Education | (%) | 19.7 | 32.9 | 34.7 | −12.7 | 17.3 | 29.0 |
| Employment | (%) | 21.2 | −5.2 | 1.6 | −4.4 | 20.8 | 1.8 |
| Health plan | (%) | 0.8 | −11.5 | 1.5 | −17.6 | 1.0 | 1.3 |
| Household income | (%) | 40.4 | 25.8 | 39.8 | −9.6 | 28.4 | −0.4 |
| County median household income | (%) | 2.8 | −11.4 | 1.0 | 22.1 | 2.1 | 37.7 |
| County income inequality | (%) | 0.8 | 13.1 | 1.0 | 24.8 | 0.4 | 0.2 |
| County percent Blacks | (%) | 1.5 | −16.7 | 0.0 | −3.1 | 0.0 | −1.1 |
| County percent Hispanics | (%) | −0.6 | 0.3 | −4.6 | 15.3 | −0.4 | 0.8 |
| Metro area | (%) | 1.8 | −14.0 | 1.3 | 7.0 | −0.7 | −3.9 |
| Total | (%) | 71.8 | 28.3 | 50.3 | 49.6 | 64.5 | 35.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahiri, K.; Pulungan, Z. Racial/Ethnic Health Disparity in the U.S.: A Decomposition Analysis. Econometrics 2021, 9, 22. https://doi.org/10.3390/econometrics9020022
Lahiri K, Pulungan Z. Racial/Ethnic Health Disparity in the U.S.: A Decomposition Analysis. Econometrics. 2021; 9(2):22. https://doi.org/10.3390/econometrics9020022
Chicago/Turabian StyleLahiri, Kajal, and Zulkarnain Pulungan. 2021. "Racial/Ethnic Health Disparity in the U.S.: A Decomposition Analysis" Econometrics 9, no. 2: 22. https://doi.org/10.3390/econometrics9020022
APA StyleLahiri, K., & Pulungan, Z. (2021). Racial/Ethnic Health Disparity in the U.S.: A Decomposition Analysis. Econometrics, 9(2), 22. https://doi.org/10.3390/econometrics9020022