This section discusses the research challenges that the MEDIWARN communication system poses and the design choices made to address the system requirements.
4.1. Requirements
The wireless network involved in the MEDIWARN system must satisfy several application requirements, which pose the following design challenges.
High data rate. The monitors may need to transmit a significant amount of data within short intervals (e.g., waveforms). For this reason, a wireless technology that support high data rates is required.
Local communications. The patients’ data have to be transferred over a private network that is locally managed within the hospital. This design choice was driven by the explicit request of the medical staff involved in the MEDIWARN project to avoid transmitting sensitive data to remote servers. This choice is beneficial to privacy and it also makes the data availability independent of any network provider.
Reliability and fault-tolerance. The MEDIWARN communication system needs to provide high reliability and availability, as the monitoring must work and the patient’s vital parameters must be delivered to the MEDIWARN Virtual Biosensor even in the case of faults. Consequently, negative conditions, such as interference or faults in one or multiple nodes, shall not make the communication network fail. For these reasons, suitable mechanisms, such as retransmissions and node/path redundancy, are needed. In addition, the host running the MEDIWARN Virtual Biosensor must be fault tolerant, thus hardware and software redundancy have to be introduced.
Mobility. The MEDIWARN system involves handheld devices, i.e., mobile nodes. As a consequence, mechanisms to support node mobility are required.
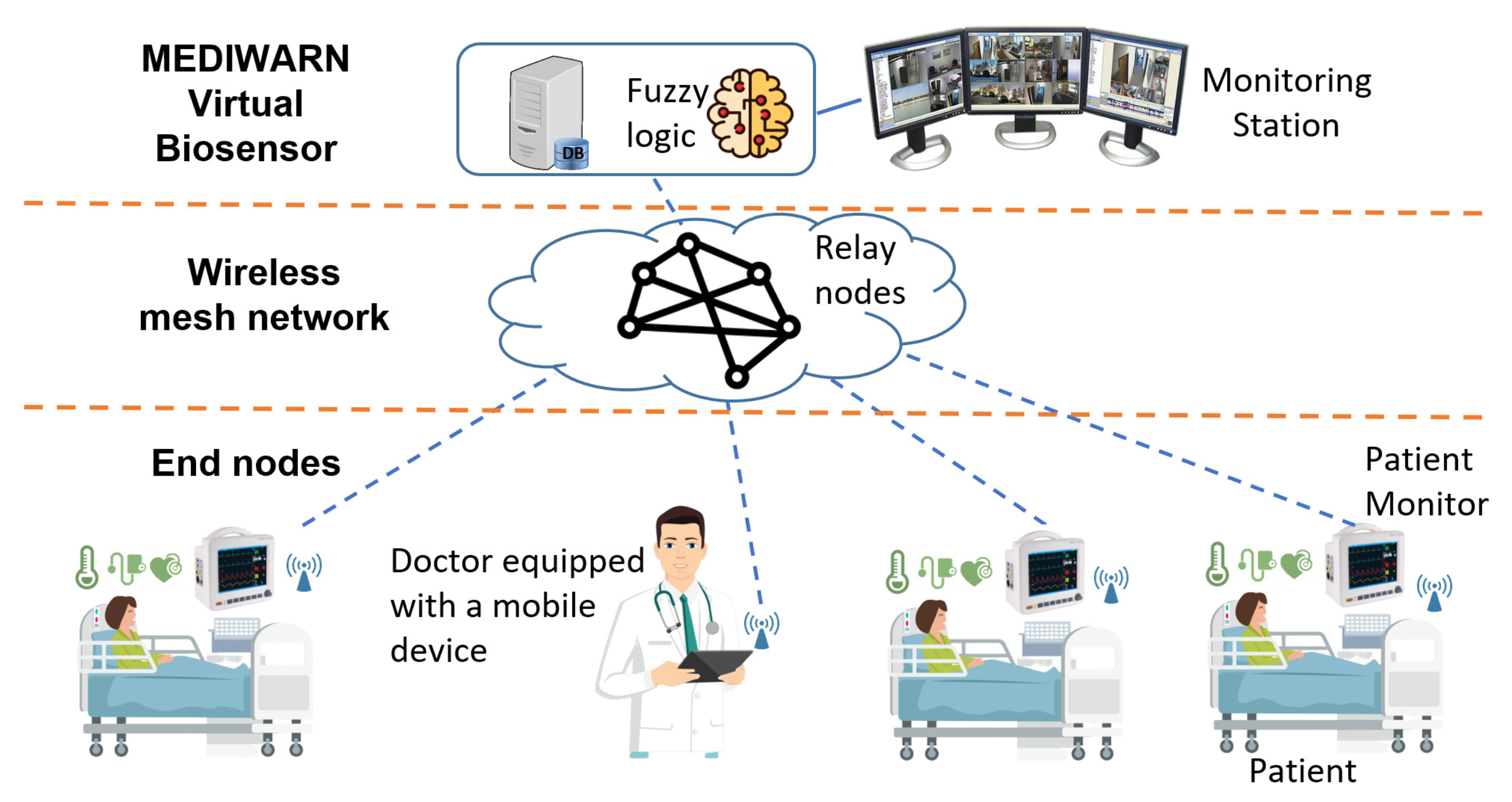
Multi-hop communication. The target application may demand for large-scale communication network deployments, and therefore the monitors can be multiple hops away from the MEDIWARN Virtual Biosensor. This requires the adoption of a number of relay nodes, i.e., intermediate nodes that receive the messages intended for other nodes and forward them up to their final destination. The number and placement of such relay nodes must be accurately evaluated according to some metrics, such as the coverage range of each node and the number of senders in a specific area. Moreover, a trade-off between the number of relay nodes and the network reliability (node/path redundancy) has to be found. In fact, while a higher number of relay nodes provides multiple paths for each message transmission from a source to the intended destination, and therefore alternative ways to reach the destination even in case of faults (e.g., a node failure), it entails higher costs in terms of network devices and energy consumption.
Routing. In the MEDIWARN network architecture, routing, i.e., the process of selecting one or multiple paths for message forwarding, is a critical issue. In fact, the routing protocol should not introduce a significant overhead, in terms of network workload, to not impair the communication network performance in terms of end-to-end delay. This turned out to be a research question, as explained in the following subsection. The solution here proposed is presented in
Section 5.
Real-time. The MEDIWARN system continuously collects and processes data in order to promptly alert the medical staff. Consequently, bounded delivery times must be guaranteed to the messages carrying such data. In particular, the Virtual Biosensor considers the monitor transmission period as a soft deadline on the message delivery time, which can be occasionally exceeded without compromising the proper system operation. However, any data delivered to the receiver with a delay longer than the transmission period are not useful for real-time monitoring, and therefore they are not forwarded to the virtual biosensor. This aspect, combined with the requirements on routing previously mentioned, also poses a research challenge. In the following, the design choices corresponding to the above-mentioned requirements are described in detail.
4.2. Design Solutions
Communication technology. The IEEE 802.11 (WiFi) technology offers high bandwidth and high quality of service [
35,
36]. Compared to other high-bandwidth wireless technologies, such as cellular networks, WiFi is locally managed and its availability does not depend on any network provider. For these reasons, WiFi is the technology chosen for the MEDIWARN system. In addition, the use of IEEE 802.11-based networks allows to maintain sensitive data within the hospital intranet (instead of sending them through the Internet), thus meeting one of the previously discussed MEDIWARN system requirements.
The IEEE 802.11 standard supports both the infrastructure operating mode and the ad-hoc one, but the requirements of the MEDIWARN systems lead to the use of WiFi in ad-hoc mode, as it offers higher flexibility and higher fault tolerance. Such a choice meets both the high data rate and local communication requirements. In fact, the ad-hoc mode allows each end node to communicate directly with the other end nodes within the same coverage area and supports link redundancy. This way, mesh topologies are supported and the same message can be transmitted over multiple paths. However, WiFi in ad-hoc mode increases the network management complexity.
Redundancy mechanisms. In order to guarantee the message delivery even in case of faults (e.g., intermediate node failures) or corrupted transmissions due to interference or noise, both spatial redundancy and retransmission mechanisms were adopted in the MEDIWARN system. This way the reliability and fault-tolerance requirements are met. Spatial redundancy, allowing for transmissions on multiple paths, increases the probability that the messages will be received correctly. The retransmission mechanism is based on end-to-end acknowledgements (ack), and therefore a missing ack after a message transmission will indicate that something went wrong and will cause the retransmission of the unconfirmed message.
Mesh topology with mobility support. According to the hospital organization, the MEDIWARN system may require a large-scale deployment that includes mobile nodes. As a result, the wireless network needs to manage a dynamic topology [
37] and multi-hop communications. For this reason, a mesh topology with a proper number of relay nodes is needed to guarantee a total coverage of the hospital units included in the MEDIWARN system. The number of relay nodes needed in a specific application scenario depends on multiple parameters. Among them, the area to be covered, the devices used and their transmission power, the presence of obstacles, interference and signal attenuation and the reliability level required by the application.
This strategy provides the nodes with mobility support, as the handheld devices can freely move within the area without losing the local wireless connection. The wireless nodes, therefore, dynamically establish all the possible connections between each other to create a mesh topology and support multiple transmission paths for messages from the source to the intended destination.
Routing protocol. The MEDIWARN system includes mobile nodes, i.e., the handheld devices of the medical staff on the move within the hospital unit and the patients’ monitors, which can be relocated according to the hospital unit needs. Consequently, a dynamic routing protocol is considered the best option for MEDIWARN. This way, message forwarding is based on the current network conditions and the routing protocol is able to route around faults, such as node failures or loss of connection between nodes.
Several routing protocols were standardized for ad-hoc wireless networks [
38]. Among them, the Ad-hoc On-demand Distance Vector (AODV) and the Dynamic Source Routing (DSR) are reactive protocols that, on demand, select a path from the source to the destination. As discussed in ref. [
38], although these approaches entail a low overhead in terms of the workload introduced by the routing message exchange, they increase the network latency.
Since MEDIWARN requires low latency communications, the above mentioned protocols are not suitable solutions, whereas proactive or hybrid routing protocols could be considered. However, both the Destination-Sequenced Distance-Vector Routing (DSDV) and the Temporally Ordered Routing Algorithm (TORA), as discussed in ref. [
38], would significantly increase the network workload in the MEDIWARN system.
Another option could be the hybrid routing protocol for wireless mesh routing that is defined in the IEEE amendment 802.11s [
39,
40]. However, the IEEE 802.11s requires specific hardware/software features that may not be supported by a number of COTS devices.
Due to the limitations in this respect of the state-of-the-art solutions previously mentioned, here, a custom routing protocol is proposed for the MEDIWARN system. The protocol, called the MultiPath Routing Protocol for MEDIWARN (MP-RPM), is described in
Section 5 and aims to support reliable transmissions on a dynamic network, while limiting the network overhead due to the control messages. Being totally hardware independent, MP-RPM can be used on any COTS device without any hardware/software modifications (unlike the IEEE 802.11s standard).
Soft real-time communications support. Soft real-time messages have deadlines that are taken into account when routing and forwarding messages, but without strict guarantees, so an occasional deadline miss may happen and it is tolerated. However, the messages carrying, for example, a patient’s physiological parameters, if not delivered on time, will not be used for real-time monitoring and will not be displayed on the screen that shows the patient’s current conditions.
To minimize the number of deadline misses, here, we propose an IEEE 802.11-based mesh network that includes on the relay nodes suitable mechanisms to improve the soft real-time performance of the MEDIWARN system. Each relay node implements a priority queue of outbound messages. When a node receives a message to forward, the message is inserted in the queue. Message priority is assigned according to a configurable criterion, for example, the hop count, i.e., the number of hops that the message has traversed so far. This way, the messages that traverse more links to reach the destination would be favored to compensate for the longest path.
In addition, the custom routing protocol (i.e., the MP-RPM) here proposed allows choosing the best next hop for each message to be forwarded based on a route selection algorithm. In particular, every time a message needs to be forwarded by a relay node, the latter searches its routing table for all the possible routes to the destination. The routes are sorted from best to worst according to a configurable metrics, e.g., the hop distance, so the relay node selects the first path to forward the message. This way, each message follows the best path between the sender and the receiver based on a specific metrics. Note that, as discussed in
Section 5.2, the MP-RPM implements multipath routing, and therefore each message can be sent over multiple paths to provide redundancy and increase the protocol reliability. Consequently, each relay node selects the first
paths thanks to the route selection algorithm.
Summarizing, the MEDIWARN system needs a simple, lightweight and configurable routing protocol able to both take the message priority into account to reduce the delay of soft real-time messages and provide path redundancy and mobility support without significantly increasing the network workload and latency. The solution here proposed is described in detail in the following Section.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}