Ethnomedicinal Knowledge of Traditional Healers in Roi Et, Thailand

 and
and 
Abstract
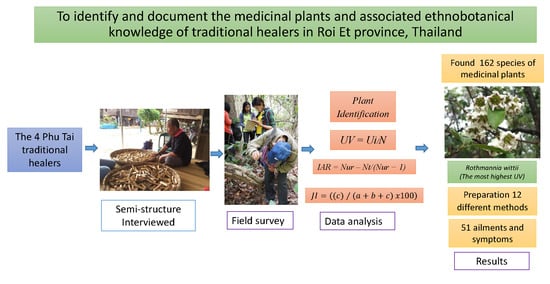
1. Introduction
2. Results
2.1. The Traditional Healers
2.2. Diversity of Medicinal Plants
2.3. Similarities of the Medicinal Plants Used by Healers
2.4. Life Forms of the Plants Used
2.5. Plant Parts Used
2.6. Preparation of Medicine
2.7. Use Value Index (UV) and Symptoms and Ailments Treated by the Phu Tai Traditional Healers
2.8. Informant Agreement Ratio (IAR) among Healers
2.9. Habitats and Status of Medicinal Plants
3. Discussions
3.1. The Traditional Healers
3.2. Diversity of Medicinal Plants
3.3. Similarities of Plants Used by the Healers
3.4. Life Forms of Medicinal Plants
3.5. Plant Parts Used for Medicine
3.6. Preparation and Administration
3.7. Use Value Index (UV) and Symptoms and Ailments Treated
3.8. Informant Agreement Ratio (IAR)
3.9. Habitats and Status of Medicinal Plants
4. Materials and Methods
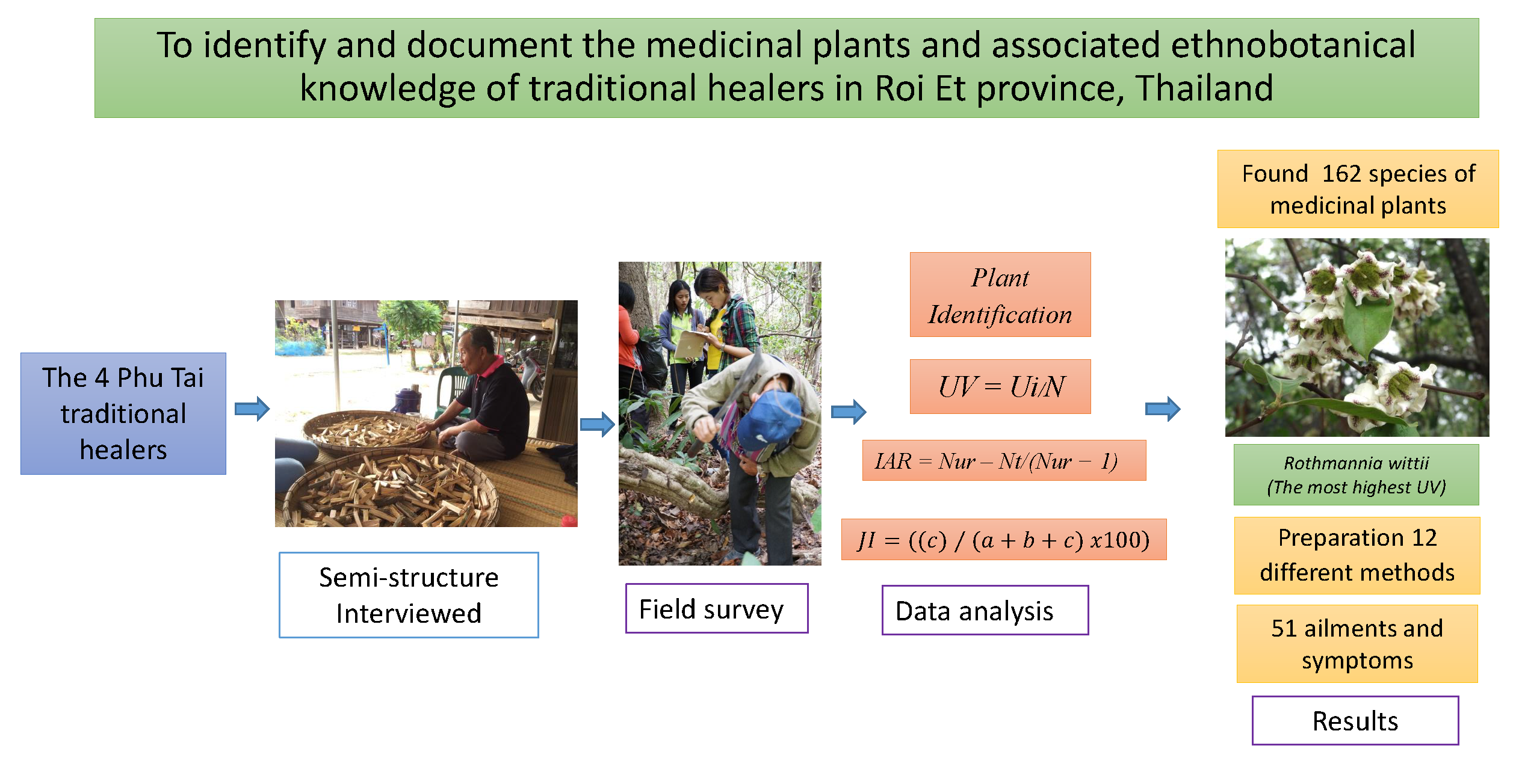
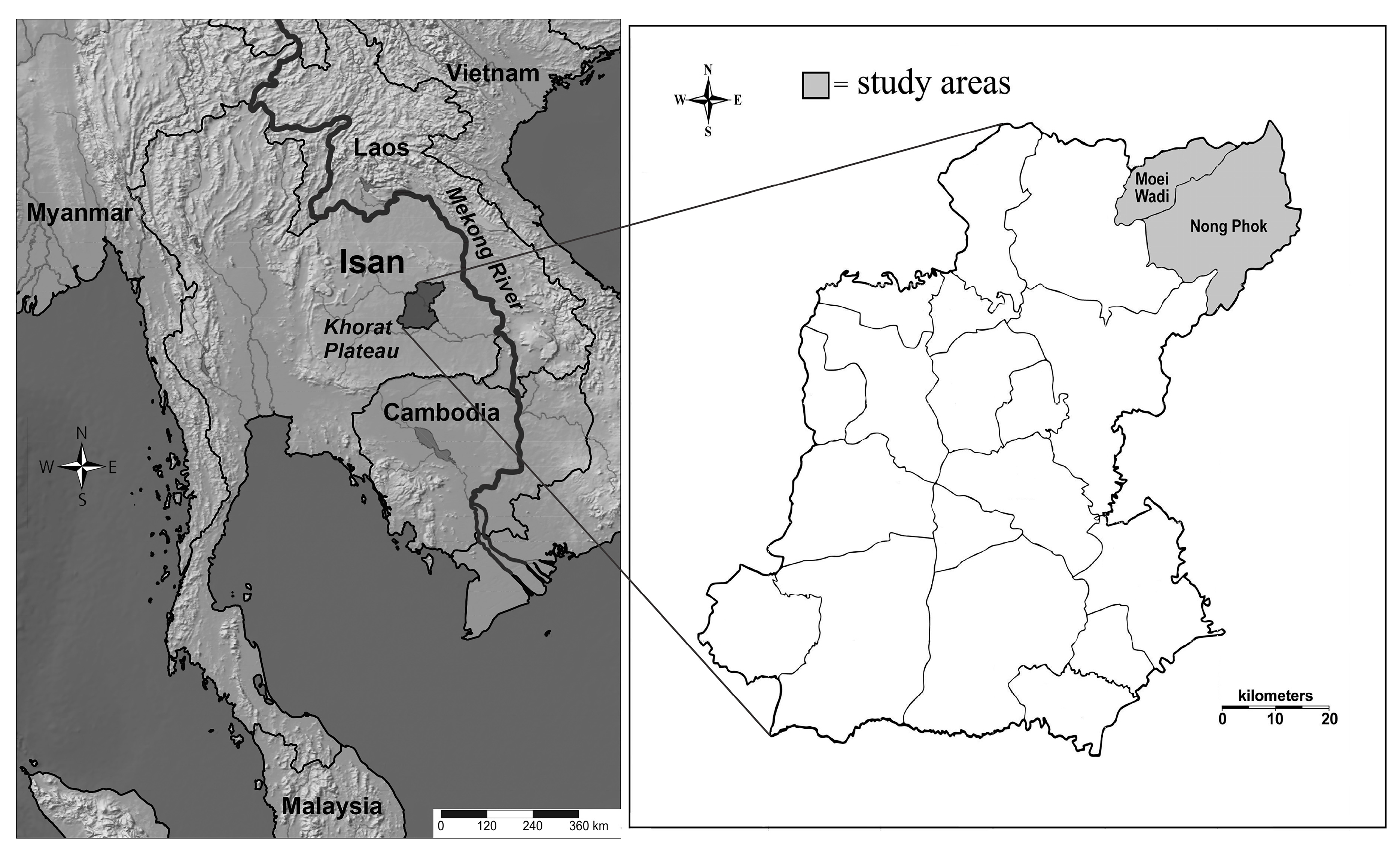
4.1. Study Area
4.2. Informants
4.3. Data Collection
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahmed, H.M. Ethnopharmaco botanical study on the medicinal plants used by herbalists in Sulaymaniyah Province, Kurdistan, Iraq. J. Ethnobiol. Ethnomed. 2016, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Boudjelal, A.; Henchiri, C.; Sari, M.; Sarri, D.; Hendel, N.; Benkhaled, A.; Ruberto, G. Herbalists and wild medicinal plants in M’Sila (North Algeria): An ethnopharmacology survey. J. Ethnopharmacol. 2013, 148, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.M.; Rastogi, S.; Rawat, A.K.S. Indian Traditional Ayurvedic System of Medicine and Nutritional Supplementation. Evid. Based Complement. Altern. Med. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ergil, K.; Kramer, E.J.; Ng, A.T. Chinese herbal medicines. West J. Med. 2002, 176, 275–279. [Google Scholar] [PubMed]
- World Health Organization. Traditional Medicine: Growing Needs and Potential. 2002. Available online: https://apps.who.int/iris/handle/10665/67294 (accessed on 17 June 2019).
- World Health Organization. WHO Traditional Medicine Strategy: 2014–2023. 2013. Available online: https://apps.who.int/iris/handle/10665/92455 (accessed on 4 January 2019).
- Cicero, A.F.G.; DeRosa, G.; Gaddi, A. What do herbalists suggest to diabetic patients in order to improve glycemic control? Evaluation of scientific evidence and potential risks. Acta Diabetol. 2004, 41, 91–98. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.S.; Soliman, A.; Annan, K.; Lartey, R.N.; Awuah, B.; Merajver, S.D. Traditional herbalists and cancer management in Kumasi, Ghana. J. Cancer Educ. 2012, 27, 573–579. [Google Scholar] [CrossRef]
- Benarba, B.; Belabid, L.; Righi, K.; Bekkar, A.A.; Elouissi, M.; Khaldi, A.; Hamimed, A. Ethnobotanical study of medicinal plants used by traditional healers in Mascara (North West of Algeria). J. Ethnopharmacol. 2015, 175, 626–637. [Google Scholar] [CrossRef]
- D’Avigdor, E.; Wohlmuth, H.; Asfaw, Z.; Awas, T. The current status of knowledge of herbal medicine and medicinal plants in Fiche, Ethiopia. J. Ethnobiol. Ethnomed. 2014, 10, 38. [Google Scholar] [CrossRef]
- Amiri, M.S.; Joharchi, M.R. Ethnobotanical investigation of traditional medicinal plants commercialized in the markets of Mashhad, Iran. Avicenna J. Phytomed. 2013, 3, 254–271. [Google Scholar]
- Al-Douri, N.A.; Al-Essa, L.Y. A survey of plants used in Iraqi traditional medicine. Jordan J. Pharm. Sci. 2010, 3, 100–108. [Google Scholar]
- Ghasemi, P.A.; Momeni, M.; Bahmani, M. Ethnobotanical Study of Medicinal Plants Used by Kurd Tribe in Dehloran and Abdanan Districts, Ilam Province, Iran. Afr. J. Tradit. Complement. Altern. Med. 2012, 10, 368–385. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Marwat, S.K.; Gohar, F.; Khan, A.; Bhatti, K.H.; Amin, M.; Ud, N.D.; Ahmad, M.; Zafar, M. Ethnobotanical Study of Medicinal Plants of Semi-Tribal Area of Makerwal & Gulla Khel (Lying between Khyber Pakhtunkhwa and Punjab Provinces). Am. J. Plant Sci. 2013, 4, 98–116. [Google Scholar]
- Rajaei, P.; Mohamadi, N. Ethnobotanical Study of Medicinal Plants of Hezar Mountain Allocated in South East of Iran. Iran. J. Pharm. Res. 2012, 11, 1153–1167. [Google Scholar] [PubMed]
- Regulatory Situation of Herbal Medicines a Worldwide Review. Available online: http://apps.who.int/medicinedocs/pdf/whozip57e/whozip57e.pdf (accessed on 14 June 2019).
- Promdee, S.; Jantapo, A.; Siltragool, W. Thai Traditional Medicine: Applying Local Wisdom Knowledge for Health Treatment of Cancer Patients in Aphinyana Arokhayasala Foundation. Asian Cult. Hist. 2014, 6, 126. [Google Scholar] [CrossRef]
- Phumthum, M.; Srithi, K.; Inta, A.; Junsongduang, A.; Tangjitman, K.; Pongamornkul, W.; Trisonthi, C.; Balslev, H. Ethnomedicinal plant diversity in Thailand. J. Ethnopharmacol. 2018, 214, 90–98. [Google Scholar] [CrossRef]
- National Health Commission Office. National Health Act, B.E. 2550: The Kingdom of Thailand. Available online: http://www.ilo.org/dyn/natlex/natlex4.detail?p_lang=en&p_isn=82872&p_country=THA&p_count=441 (accessed on 2 January 2019).
- The Promotion and Development of Traditional Medicine: Report of a WHO Meeting. Available online: https://apps.who.int/iris/handle/10665/40995 (accessed on 6 February 2019).
- Suwankhong, D.; Liamputtong, P.; Rumbold, B. Existing Roles of Traditional Healers (mor baan) in Southern Thailand. J. Community Health 2011, 36, 438–445. [Google Scholar] [CrossRef]
- Sermsri, S. Utilization of traditional and modern health care services in Thailand. In The Triumph of Practicality: Tradition and Modernity in Health Care Utilization in Selected Asian Countries; Quah, S.R., Ed.; Institute of Southeast Asian Studies: Singapore, 1989; pp. 160–179. [Google Scholar]
- Sawatsing, C. Provision and Utilization of Traditional Health Services in Rural Thailand. Master’s Thesis, Mahidol University, Bangkok, Thailand, 3 September 2003. [Google Scholar]
- Ruff, A.M. A boost for old remedies. Far East. Econ. Rev. 2000, 163, 100–101. [Google Scholar]
- Adthasit, R.; Kulsomboon, S.; Chantraket, R.; Suntananukan, S.; Jirasatienpong, P. The situation of knowledge management and research in the area of local wisdom in health care. In The Report Situations of Thai Traditional Medicine, Indigenous Medicine and Alternative Medicine 2005–2007; Petrakard, P., Chantraket, R., Eds.; Mnat Films: Nonthaburi, Thailand, 2007; pp. 16–22. [Google Scholar]
- Chokevivat, V.; Chuthaputti, A.; Chuthaputti, P. The use of traditional medicine in the Thai health care system. In Proceedings of the Regional Consultation on Development of Traditional Medicine in the South East Asia Region, Pyongyang, DPR Korea, 22–24 June 2005. [Google Scholar]
- Maneenoon, K.; Khuniad, C.; Teanuan, Y.; Saedan, N.; Prom-In, S.; Rukleng, N.; Kongpool, W.; Pinsook, P.; Wongwiwat, W. Ethnomedicinal plants used by traditional healers in Phatthalung Province, Peninsular Thailand. J. Ethnobiol. Ethnomed. 2015, 11, 43. [Google Scholar] [CrossRef]
- Amoah, S.K.; Sandjo, L.P.; Bazzo, M.L.; Leite, S.N.; Biavatti, M.W. Herbalists, traditional healers and pharmacists: A view of the tuberculosis in Ghana. Rev. Bras. Farm. 2014, 24, 89–95. [Google Scholar] [CrossRef]
- Shapi, M.; Matengu, K.; Mu Ashekele, H. Indigenous Knowledge System Pilot Study—Oshikoto Region; Multidisciplinary Research Centre, University of Namibia: Windhoek, Namibia, 2009. [Google Scholar]
- Sumungkaset, A.; Nantasri, C. Knowledge and wisdom of folk healers in Namon district, Kalasin Province (in Thai). TLC Res. J. 2016, 9, 87–105. [Google Scholar]
- Cheikhyoussef, N.; Shapi, M.; Matengu, K.K.; Ashekele, H.M. Ethnobotanical study of indigenous knowledge on medicinal plant use by traditional healers in Oshikoto region, Namibia. J. Ethnobiol. Ethnomed. 2011, 7, 10. [Google Scholar] [CrossRef]
- Srithi, K.; Balslev, H.; Wangpakapattanawong, P.; Srisanga, P.; Trisonthi, C. Medicinal plant knowledge and its erosion among the Mien (Yao) in northern Thailand. J. Ethnopharmacol. 2009, 123, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Burn, V. Traditional Thai Medicine. In Medicine across Cultures: History and Practice of Medicine in Non-Western Cultures; Selin, H., Ed.; Kluwer Academic Publishers: London, UK, 2003; pp. 112–132. [Google Scholar]
- Pholhiamhan, R.; Saeunsouk, S.; Saeunsouk, P. Ethnobotany of Phu Thai ethnic group in Nakhon Phanom province, Thailand. Walailak J. Sci. Tech. 2018, 15, 679–699. [Google Scholar]
- Phumthum, M.; Balslev, H. Thai Ethnomedicinal Plants Used for Diabetes Treatment. OBM Integr. Complement. Med. 2018, 3, 1–25. [Google Scholar] [CrossRef]
- Neamsuvan, O.; Madeebing, N.; Mah, L.; Lateh, W. A survey of medicinal plants for diabetes treating from Chana and Nathawee district, Songkhla province, Thailand. J. Ethnopharmacol. 2015, 174, 82–90. [Google Scholar] [CrossRef]
- Chantarapon, P.; Tantien, S.; Neamsuvan, O. Diversity of medicinal plant for fever healing from Khao Panom Benja National Park Krabi province. KKU Sci. J. 2014, 42, 313–326. [Google Scholar]
- Badami, S.; Moorkoth, S.; Suresh, B. Caesalpinia sappan—A medicinal and dye yielding plant. Nat. Prod. Radiance. 2004, 3, 75–82. [Google Scholar]
- Vidal, J. La thérapeutique par les plantes au Laos. J. Agric. Trop. Bot. Appl. 1958, 5, 601–616. [Google Scholar] [CrossRef]
- Dubost, J.M.; Phakeovilay, C.; Her, C.; Bochaton, A.; Elliott, E.; Deharo, E.; Xayvue, M.; Bouamanivong, S.; Bourdy, G. Hmong herbal medicine and herbalists in Lao PDR: Pharmacopeia and knowledge transmission. J. Ethnobiol. Ethnomed. 2019, 15, 27. [Google Scholar] [CrossRef]
- Chen, I.-N.; Chang, C.-C.; Ng, C.-C.; Wang, C.-Y.; Shyu, Y.-T.; Chang, T.-L. Antioxidant and Antimicrobial Activity of Zingiberaceae Plants in Taiwan. Plant Foods Hum. Nutr. 2007, 63, 15–20. [Google Scholar] [CrossRef]
- Ilavarasan, R.; Mallika, M.; Venkataraman, S. Anti-inflammatory and free radical scavenging activity of Ricinus communis root extract. J. Ethnopharmacol. 2006, 103, 478–480. [Google Scholar] [CrossRef] [PubMed]
- Agyare, C.; Boakye, Y.D.; Bekoe, E.O.; Hensel, A.; Dapaah, S.O.; Appiah, T. Review: African medicinal plants with wound healing properties. J. Ethnopharmacol. 2016, 177, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Birru, E.M.; Asrie, A.B.; Adinew, G.M.; Tsegaw, A. Antidiarrheal activity of crude methanolic root extract of Idigofera spicata Forssk. (Fabaceae). BMC Complement. Altern. Med. 2016, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- El Haouari, M.; Rosado, J.A. Medicinal Plants with Antiplatelet Activity. Phytotherapy Res. 2016, 30, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Ndam, L.M.; Mih, A.M.; Tening, A.S.; Fongod, A.G.N.; Temenu, N.A.; Fujii, Y. Phytochemical analysis, antimicrobial and antioxidant activities of Euphorbia golondrina L.C. Wheeler (Euphorbiaceae Juss.): An unexplored medicinal herb reported from Cameroon. SpringerPlus 2016, 5, 264. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Neamsuvan, O.; Ruangrit, T. A survey of herbal weeds that are used to treat gastrointestinal disorders from southern Thailand: Krabi and Songkhla provinces. J. Ethnopharmacol. 2017, 196, 84–93. [Google Scholar] [CrossRef]
- Sutjaritjai, N.; Wangpakapattanawong, P.; Balslev, H.; Inta, A. Traditional Uses of Leguminosae among the Karen in Thailand. Plants 2019, 8, 600. [Google Scholar] [CrossRef]
- Singh, D.; Baghel, U.S.; Gautam, A.; Baghel, D.S.; Yadav, D.; Malik, J.; Yadav, R. The genus Anogeissus: A review on ethnopharmacology, phytochemistry and pharmacology. J. Ethnopharmacol. 2016, 194, 30–56. [Google Scholar] [CrossRef]
- Ashraf, M.U.; Muhammad, G.; Hussain, M.A.; Bukhari, S.N.A. Cydonia oblonga M. a medicinal plant rich in phytonutrients for pharmaceuticals. Front. Pharmacol. 2016, 7, 163. [Google Scholar] [CrossRef]
- Panyaphu, K.; Van On, T.; Sirisa-Ard, P.; Srisa-Nga, P.; Chansakaow, S.; Nathakarnkitkul, S. Medicinal plants of the Mien (Yao) in Northern Thailand and their potential value in the primary healthcare of postpartum women. J. Ethnopharmacol. 2011, 135, 226–237. [Google Scholar] [CrossRef]
- Tugume, P.; Kakudidi, E.K.; Buyinza, M.; Namaalwa, J.; Kamatenesi, M.; Mucunguzi, P.; Kalema, J. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomed. 2016, 12, 5. [Google Scholar] [CrossRef]
- Sivasankari, B.; Anandharaj, M.; Gunasekaran, P. An ethnobotanical study of indigenous knowledge on medicinal plants used by the village peoples of Thoppampatti, Dindigul district, Tamilnadu, India. J. Ethnopharmacol. 2014, 153, 408–423. [Google Scholar] [CrossRef] [PubMed]
- Junsongduang, A.; Balslev, H.; Inta, A.; Jampeetong, A.; Wangpakapattanawong, P. Karen and Lawa medicinal plant use: Uniformity or ethnic divergence? J. Ethnopharmacol. 2014, 151, 517–527. [Google Scholar] [CrossRef]
- Mowobi, G.G.; Abubakar, S.; Osuji, C.; Etim, V.N.; Ogechi, N.; Egya, J.J. Ethnobotanical survey of medicinal plants used for the treatment of skin disease in Keffi, Nigeria. Am. J. Phytomed. Clin. Ther. 2016, 4, 73–90. [Google Scholar]
- Lamxay, V.; De Boer, H.; Björk, L. Traditions and plant use during pregnancy, childbirth and postpartum recovery by the Kry ethnic group in Lao PDR. J. Ethnobiol. Ethnomed. 2011, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Inta, A.; Shengji, P.; Balslev, H.; Wangpakapattanawong, P.; Trisonthi, C. A comparative study on medicinal plants used in Akha’s traditional medicine in China and Thailand, cultural coherence or ecological divergence? J. Ethnopharmacol. 2008, 116, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Chuakul, W.; Saralamp, P.; Prathanturarug, S. Siam Pi Saj Cha Ya Pruek, 3rd ed.; Amarin Printing: Bangkok, Thailand, 2000. [Google Scholar]
- Yamasaki, K.; Kanchanapoom, T.; Klai-On, S.; Kasai, R.; Otsuka, H. A New Tricyclic Iridoid Glucoside from the Thai Medicinal Plant, Rothmannia wittii. Heterocycles 2002, 57, 2409. [Google Scholar] [CrossRef]
- Thomas, A.; Rajesh, E.K.; Kumar, D.S. The significance of Tinospora crispa in treatment of diabetes mellitus. Phytother. Res. 2016, 30, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Khuankaew, S.; Srithi, K.; Tiansawat, P.; Jampeetong, A.; Inta, A.; Wangpakapattanawong, P. Ethnobotanical study of medicinal plants used by Tai Yai in Northern Thailand. J. Ethnopharmacol. 2014, 151, 829–838. [Google Scholar] [CrossRef]
- Ogoina, D. Fever, fever patterns and diseases called ‘fever’—A review. J. Infect Public Health 2011, 4, 108–124. [Google Scholar] [CrossRef]
- Jirapaet, K. Thai healthy newborns have a higher risk. J. Med. Assoc. Thail. 2005, 88, 1314–1318. [Google Scholar]
- Phasanasophon, P. Active ingredients in herbs. J. Phrapokklao Nurs. Coll. 2016, 27, 120–131. [Google Scholar]
- Gazzaneo, L.R.S.; De Lucena, R.F.P.; Albuquerque, U.P. Knowledge and use of medicinal plants by local specialists in an region of Atlantic Forest in the state of Pernambuco (Northeastern Brazil). J. Ethnobiol. Ethnomed. 2005, 1, 9. [Google Scholar] [CrossRef]
- Maroyi, A. Garden Plants in Zimbabwe: Their ethnomedicinal uses and reported toxicity. Ethnobot. Res. Appl. 2012, 10, 45–57. [Google Scholar] [CrossRef]
- Office of Agricultural Economics. Agricultural statistics of Thailand 2004; Center for Agricultural Information; Office of Agricultural Economics, Ministry of Agriculture & Co-operatives: Bangkok, Thailand, 2004. [Google Scholar]
- Grabowsky, V. The Isan up to its integration into the Siamese state. In Regions and National Integration in Thailand 1982–1992; Harrossowitz, W., Ed.; Harrassowitz Verlag: Wiesbaden, Germany, 1995; p. 296. [Google Scholar]
- Keyes, C.F. Thailand, Buddhist Kingdom as Modern Nation-State; Routledge: New York, NY, USA, 2019; p. 252. [Google Scholar]
- Keyes, C.F. Isan: Regionalism in Northeastern Thailand; Cornell University: Ithaca, NY, USA, 1967; p. 220. [Google Scholar]
- Pitipat, S. The Religious and Believing of Taidam People in Sipsongjutai; Thammasart University: Bangkok, Thailand, 2003; p. 124. [Google Scholar]
- Bernard, H.R. Social Research Methods: Qualitative and Quantitative Approaches, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2013; p. 766. [Google Scholar]
- Pooma, R.; Suddee, S. Tem Smitinand’s Thai Plant Names; Department of National Parks, Wildlife and Plant Conservation, The Office of the Forest Herbarium: Bangkok, Thailand, 2014. [Google Scholar]
- Phillips, O.L.; Gentry, A.; Reynel, C.; Wilkin, P.; Gálvez-Durand, B.C. Quantitative Ethnobotany and Amazonian Conservation. Conserv. Biol. 1994, 8, 225–248. [Google Scholar] [CrossRef]
- Trotter, R.T.; Logan, M.H. Informant census: A new approach for identifying potentially effective medicinal plants. In Plants in Indigenous Medicine and Diet; Etkin, L.N., Ed.; Bedford Hill: New York, NY, USA, 1986; pp. 91–112. [Google Scholar]
- Höft, M.; Barik, S.K.; Lykke, A.M. Quantitative Ethnobotany. In Applications of Multivariate and Statistical Analysis in Ethnobotany; People Plant Working Paper, Place de Fontenoy; NESCO: Paris, France, 1999; p. 45. [Google Scholar]


{kind=link}
{kind=link}
| District | Name (Age) | Years Practicing Herbal Medicine | Number of Known Medicinal Plant (spp.) | Type of Training |
|---|---|---|---|---|
| Nong Phok | Healer 1 (78 years) | 64 | 89 | Family members |
| Healer 2 (82 years) | 60 | 37 | Formal Training | |
| Muei Wadi | Healer 3 (76 years) | 45 | 95 | Formal Training |
| Healer 4 (77 years) | 60 | 53 | Family members | |
| Average | 78 | 57 | 68 |
| Healer | Healer 2 Species (%) | Healer 3 Species (%) | Healer 4 Species (%) |
|---|---|---|---|
| Healer 1 | 11 (6.5) | 14 (8.0) | 11 (8.5) |
| Healer 2 | - | 9 (7.8) | 3 (4.4) |
| Healer 3 | - | - | 8 (7.9) |
| Methods | Number of Species | % |
|---|---|---|
| Decoction | 124 | 76 |
| Crush or grind and apply to skin | 23 | 14 |
| Grind with water and drink | 10 | 6 |
| Soaked and bath | 6 | 3 |
| Eat as food | 4 | 2 |
| Soaked and drink | 4 | 2 |
| Eat as fresh | 3 | 1 |
| Boil and bath | 2 | 1 |
| Steamed | 2 | 1 |
| Chewed | 1 | <1 |
| Grind with water and wash hair | 1 | <1 |
| Grind with lemon juice and drink | 1 | <1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Junsongduang, A.; Kasemwan, W.; Lumjoomjung, S.; Sabprachai, W.; Tanming, W.; Balslev, H. Ethnomedicinal Knowledge of Traditional Healers in Roi Et, Thailand. Plants 2020, 9, 1177. https://doi.org/10.3390/plants9091177
Junsongduang A, Kasemwan W, Lumjoomjung S, Sabprachai W, Tanming W, Balslev H. Ethnomedicinal Knowledge of Traditional Healers in Roi Et, Thailand. Plants. 2020; 9(9):1177. https://doi.org/10.3390/plants9091177
Chicago/Turabian StyleJunsongduang, Auemporn, Wanpen Kasemwan, Sukanya Lumjoomjung, Wichuda Sabprachai, Wattana Tanming, and Henrik Balslev. 2020. "Ethnomedicinal Knowledge of Traditional Healers in Roi Et, Thailand" Plants 9, no. 9: 1177. https://doi.org/10.3390/plants9091177
APA StyleJunsongduang, A., Kasemwan, W., Lumjoomjung, S., Sabprachai, W., Tanming, W., & Balslev, H. (2020). Ethnomedicinal Knowledge of Traditional Healers in Roi Et, Thailand. Plants, 9(9), 1177. https://doi.org/10.3390/plants9091177