
Improving the Spatial Accessibility of Community-Level Healthcare Service toward the ‘15-Minute City’ Goal in China

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
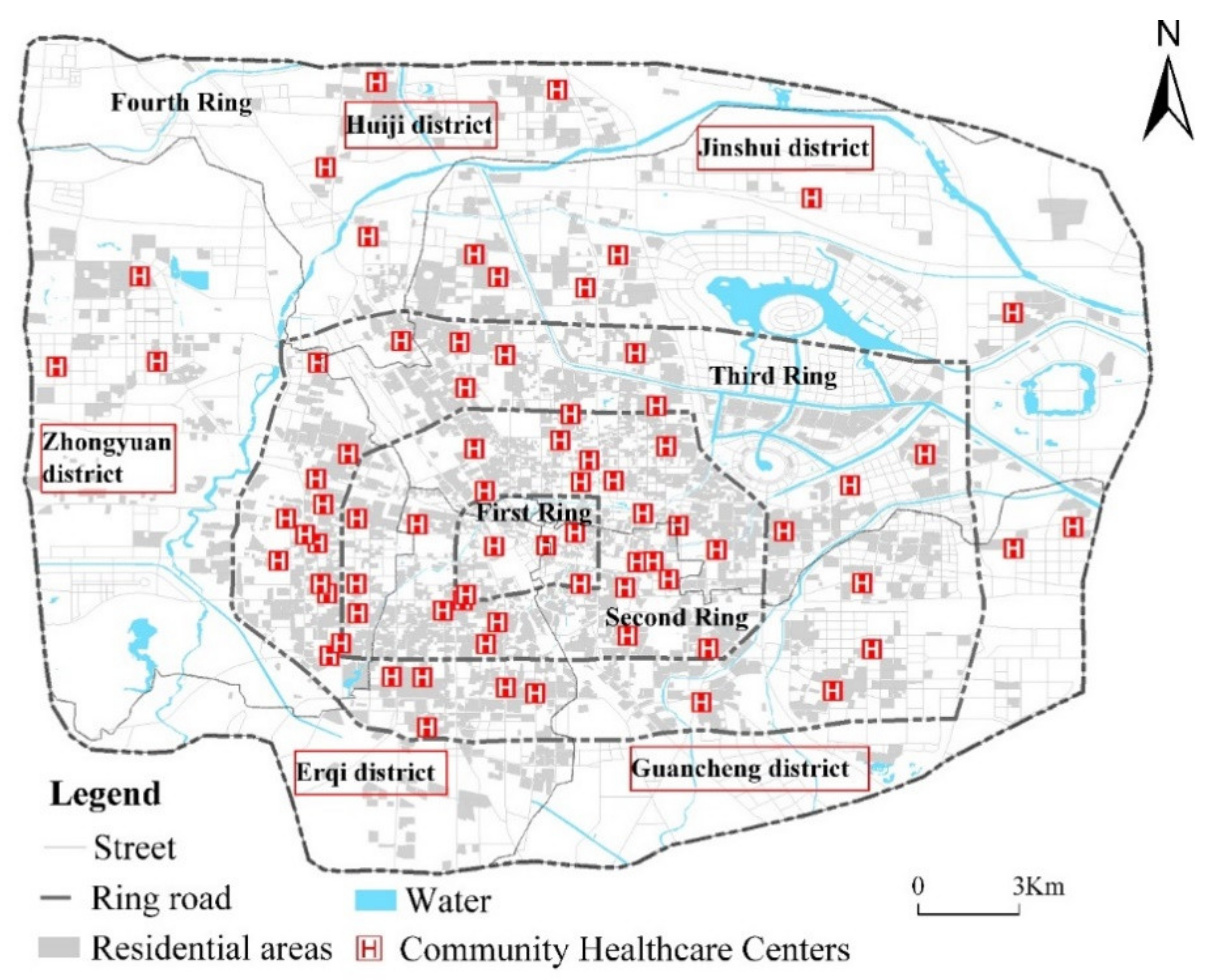
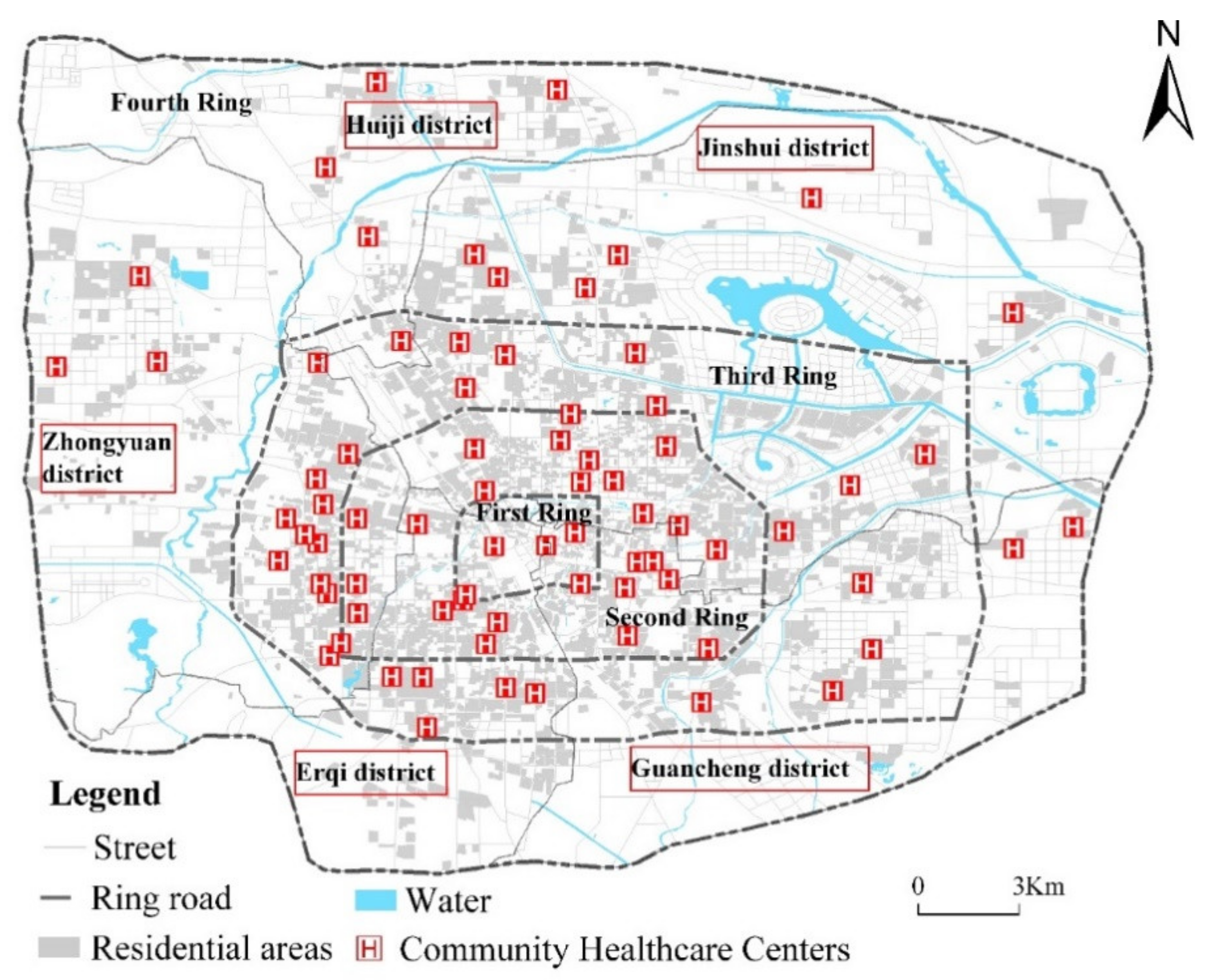
2.1. Study Area
2.2. Data Sources
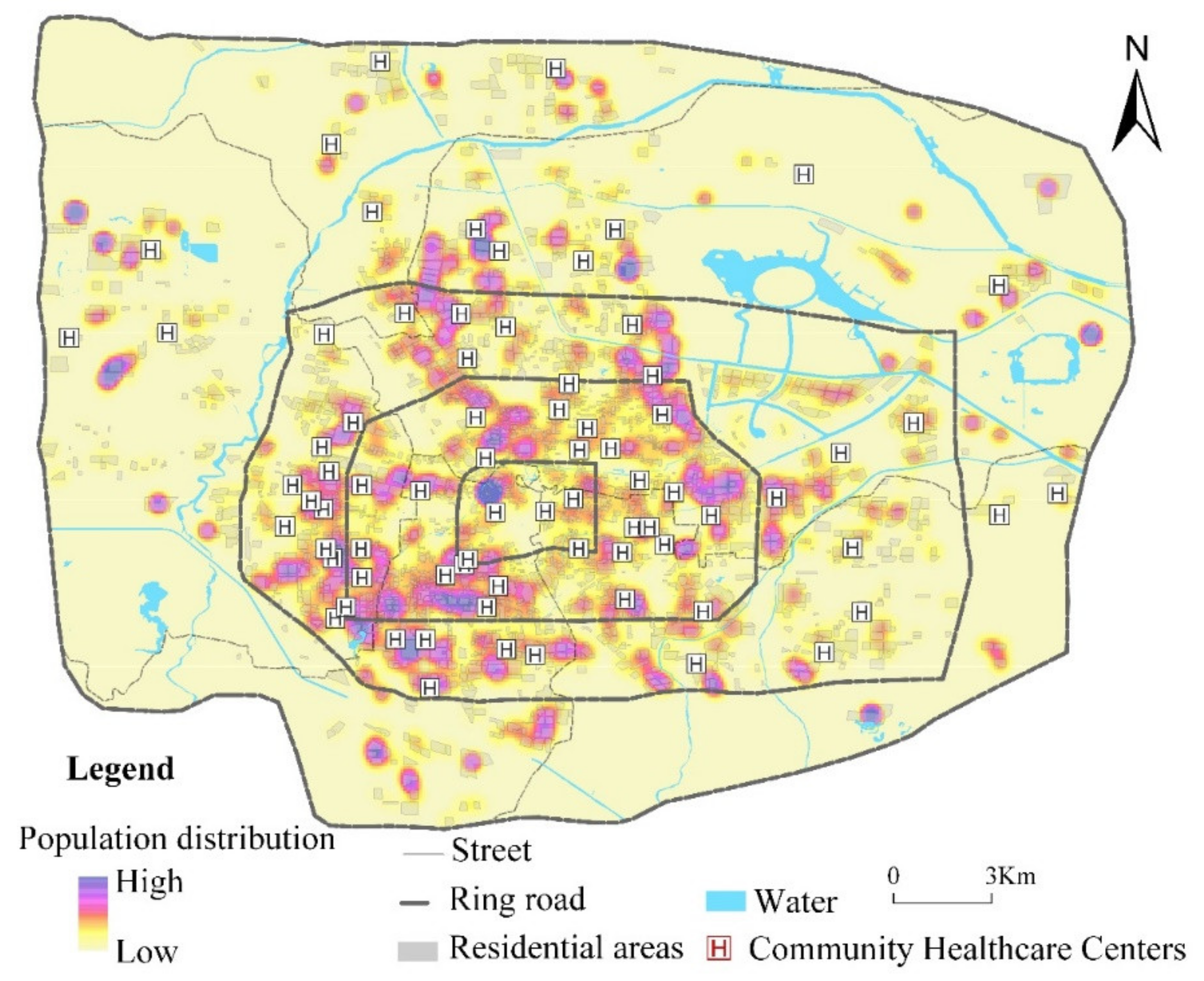
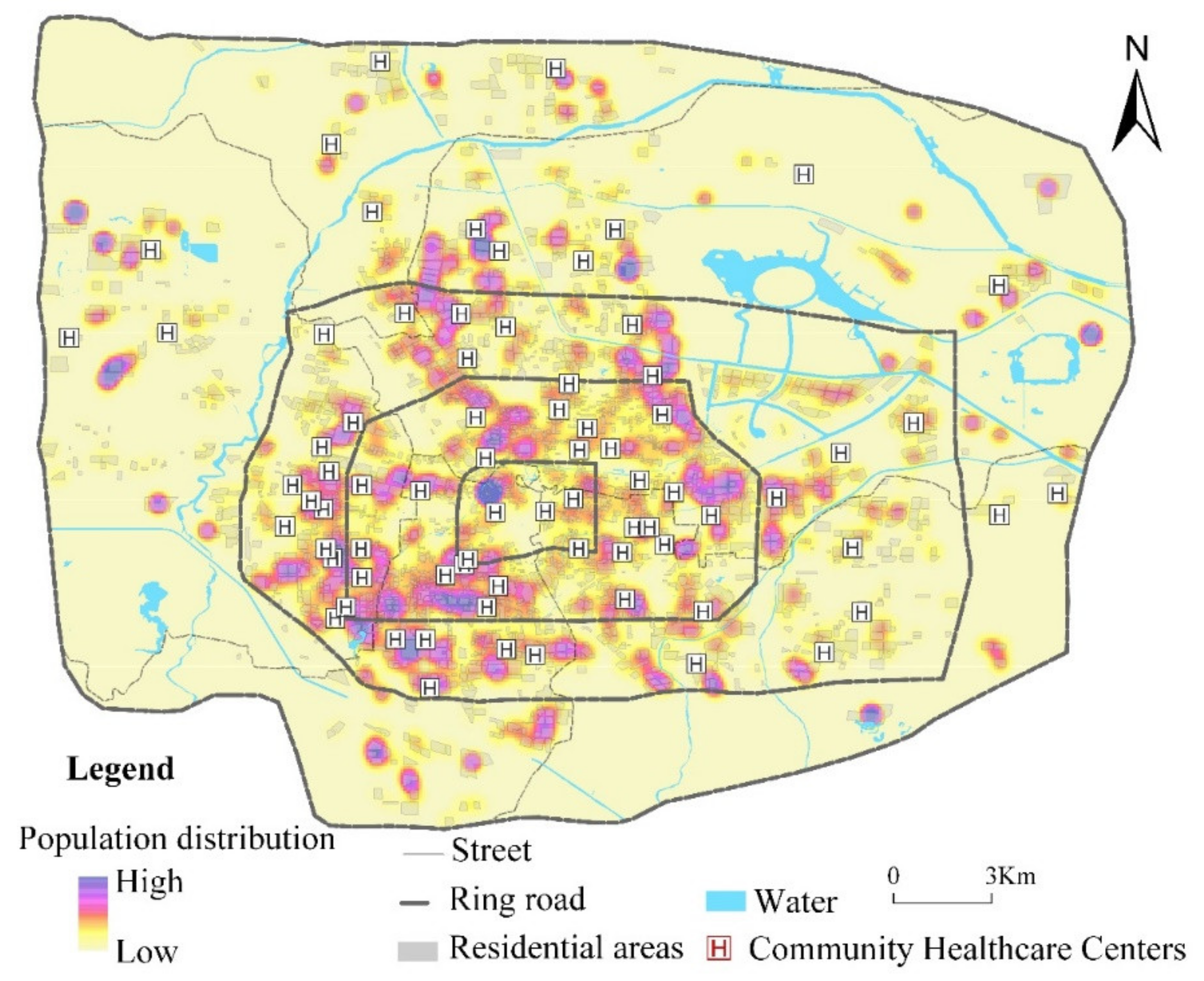
2.2.1. Residential Population
2.2.2. Community-Level Healthcare Service Centers
2.2.3. Travel Time
2.3. Methods
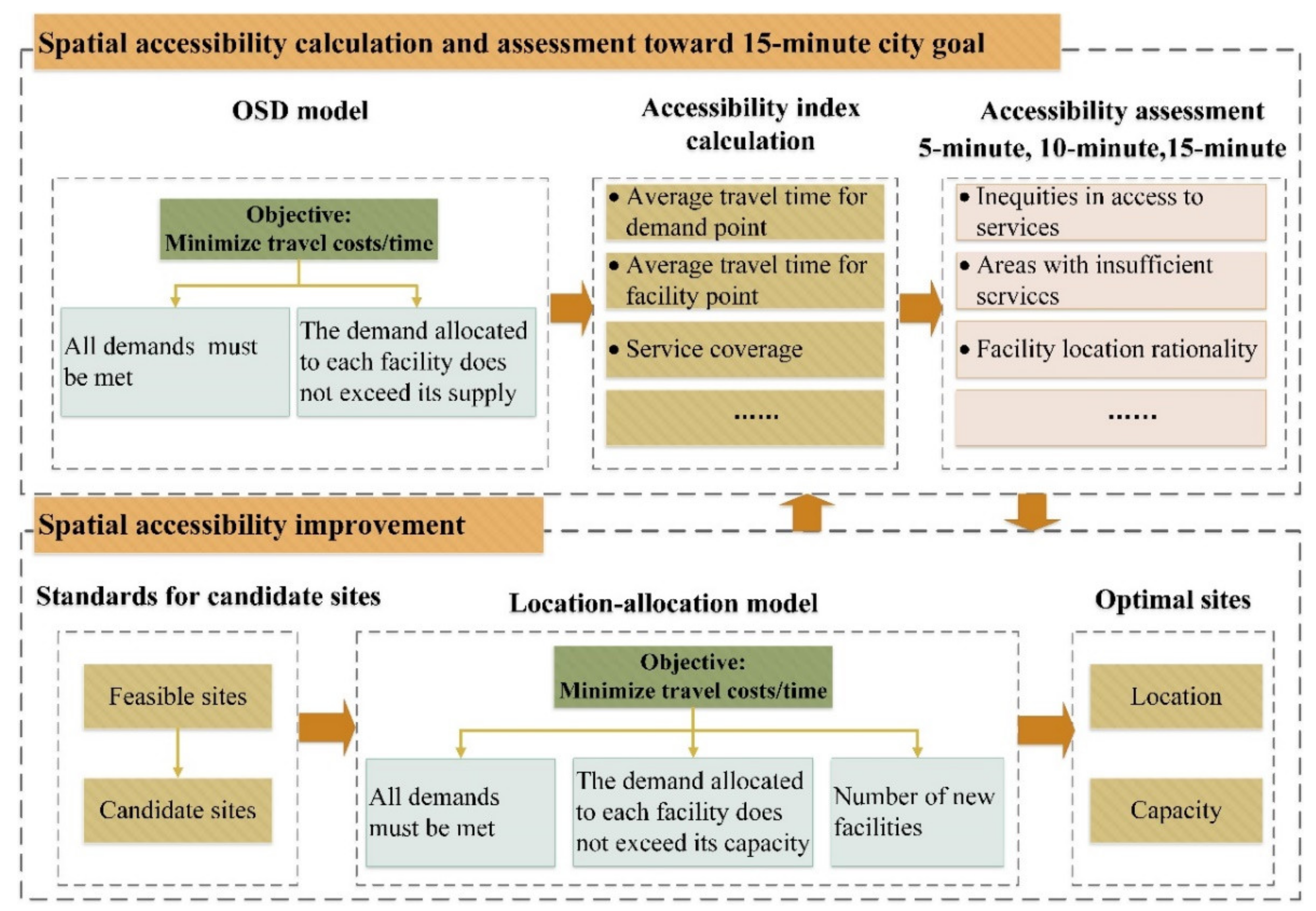
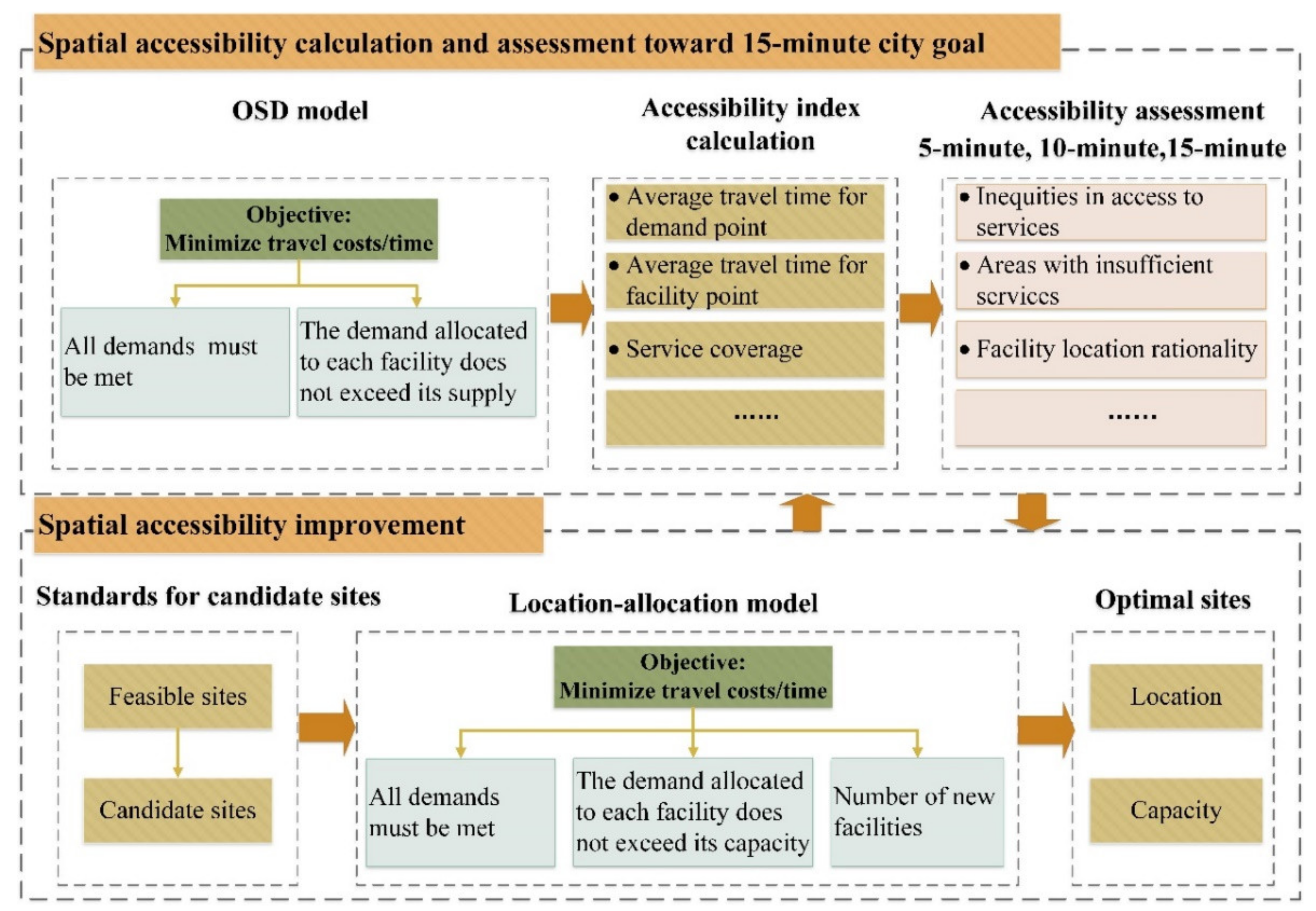
2.3.1. Analytical Framework
2.3.2. Optimal Supply–Demand Allocation
2.3.3. Capacitated p-Median Problem (CPMP) Model
2.3.4. Patients and Public Involvement
3. Results
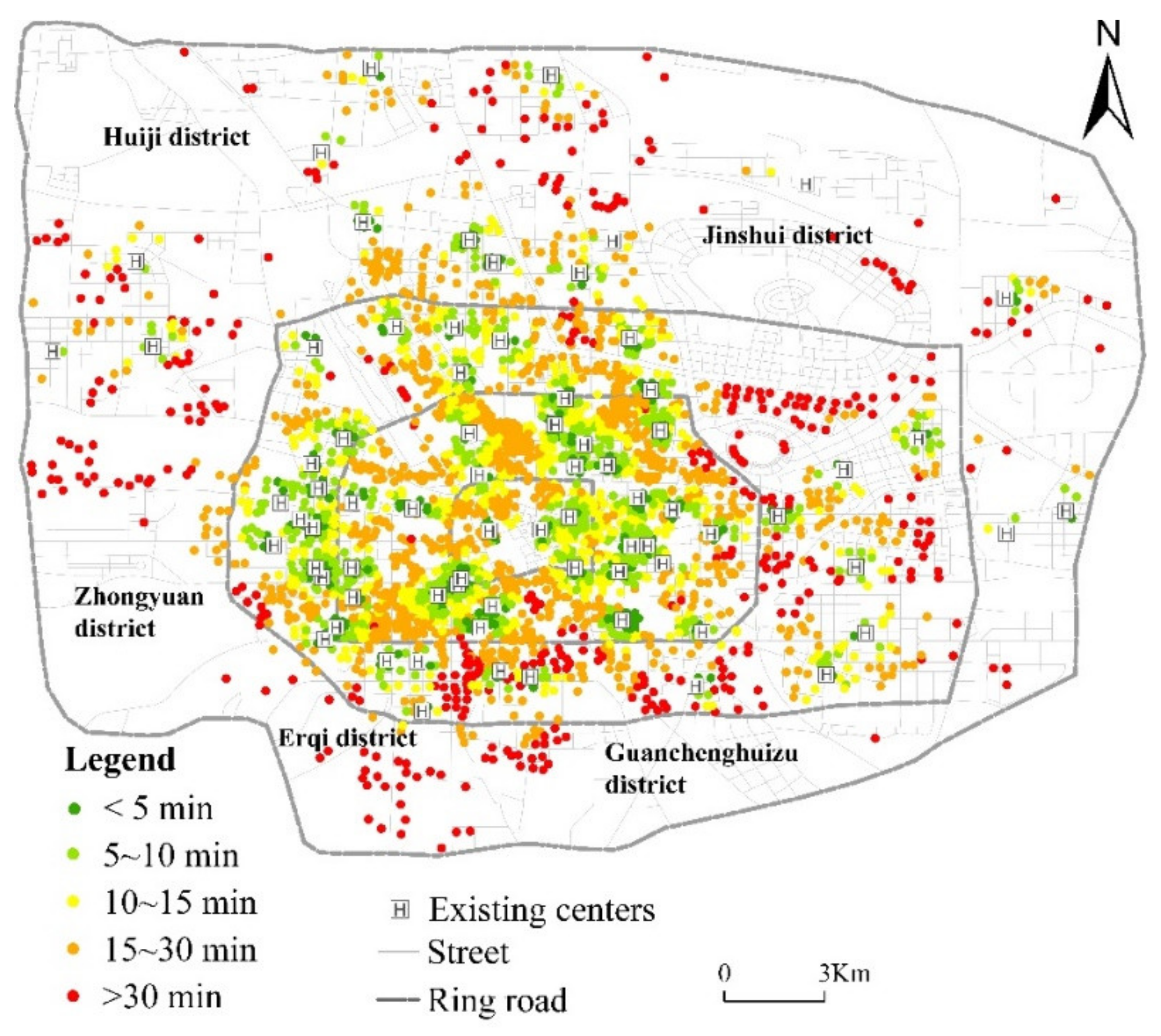
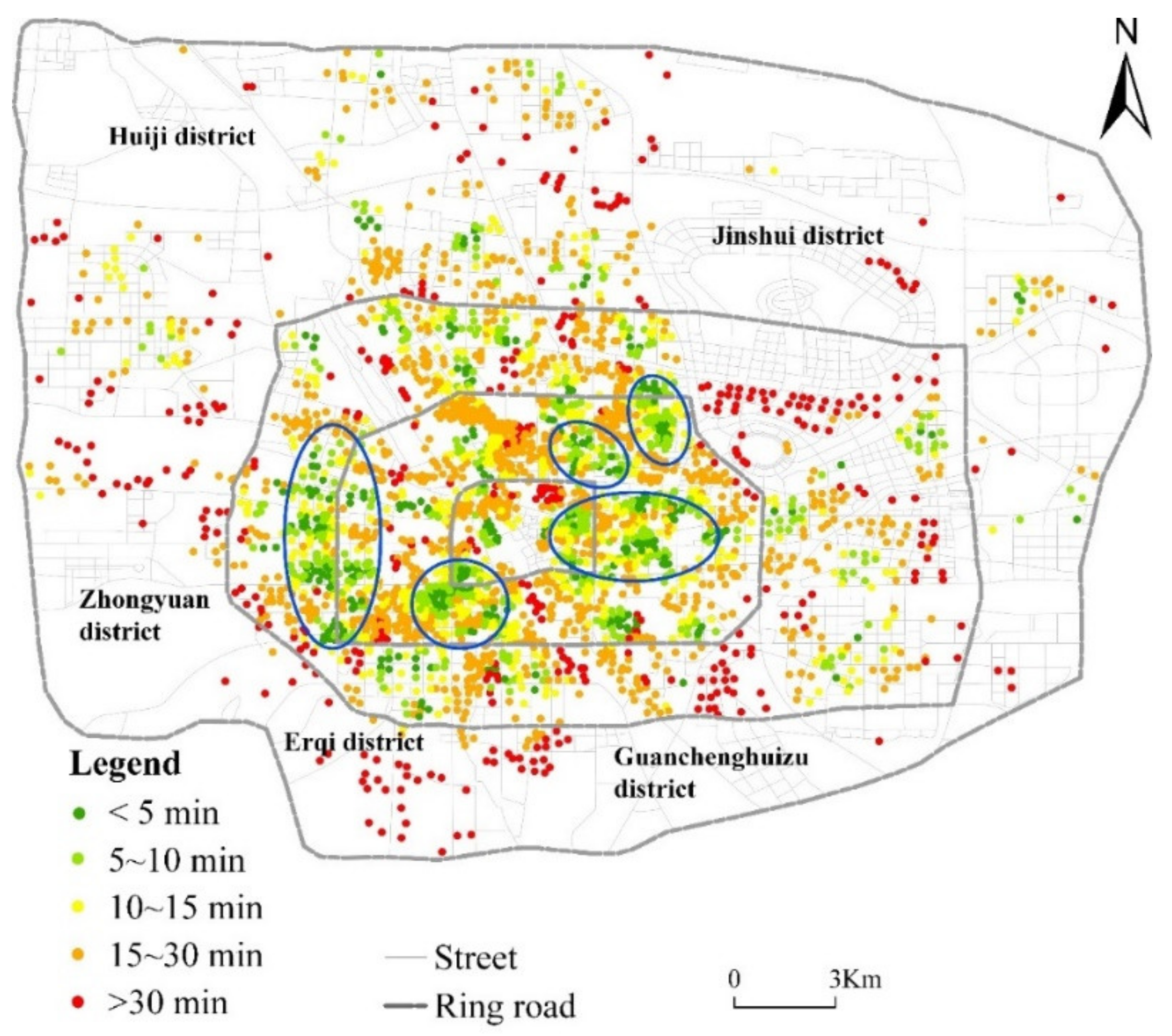
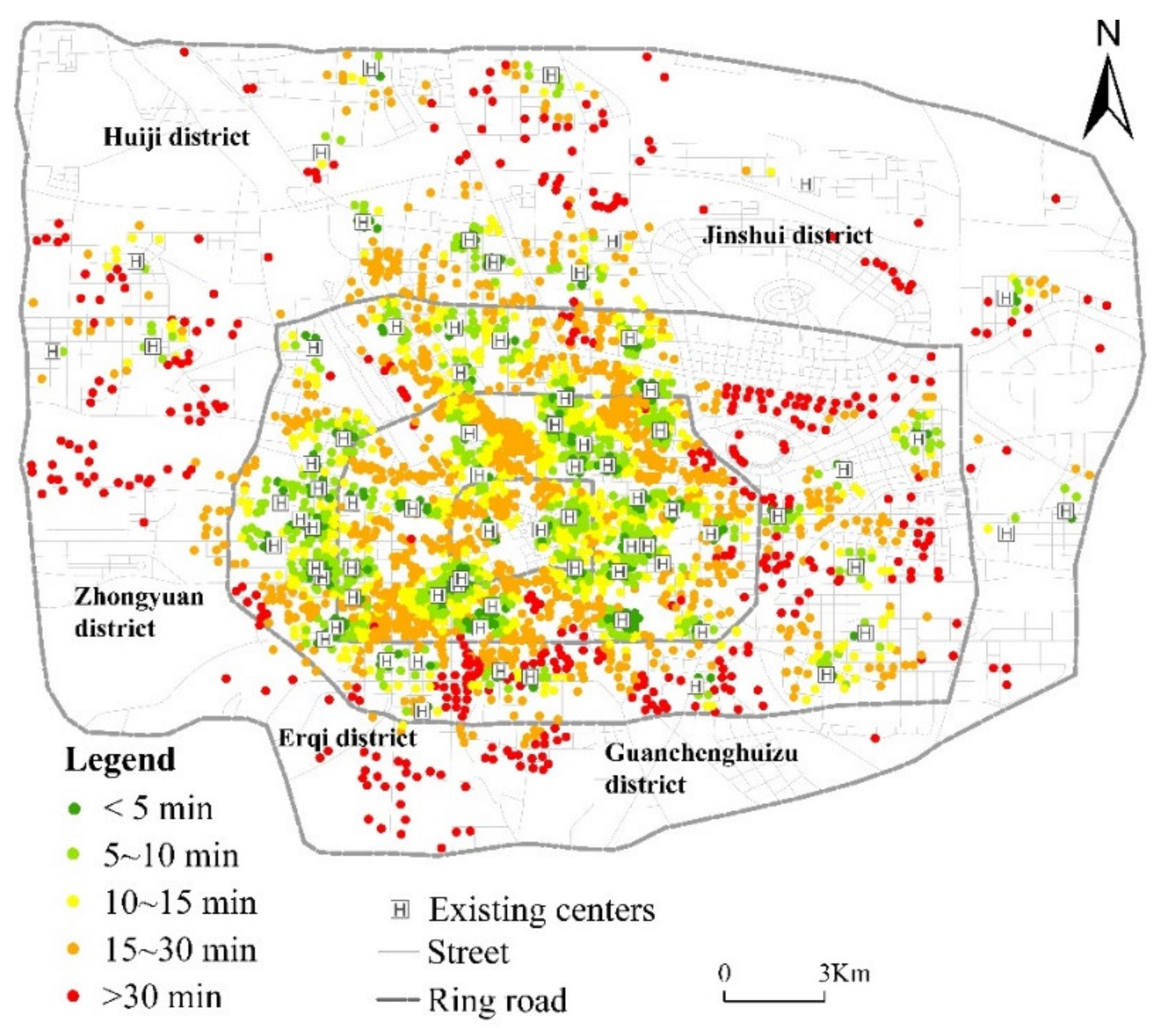
3.1. Current Status of Healthcare Services
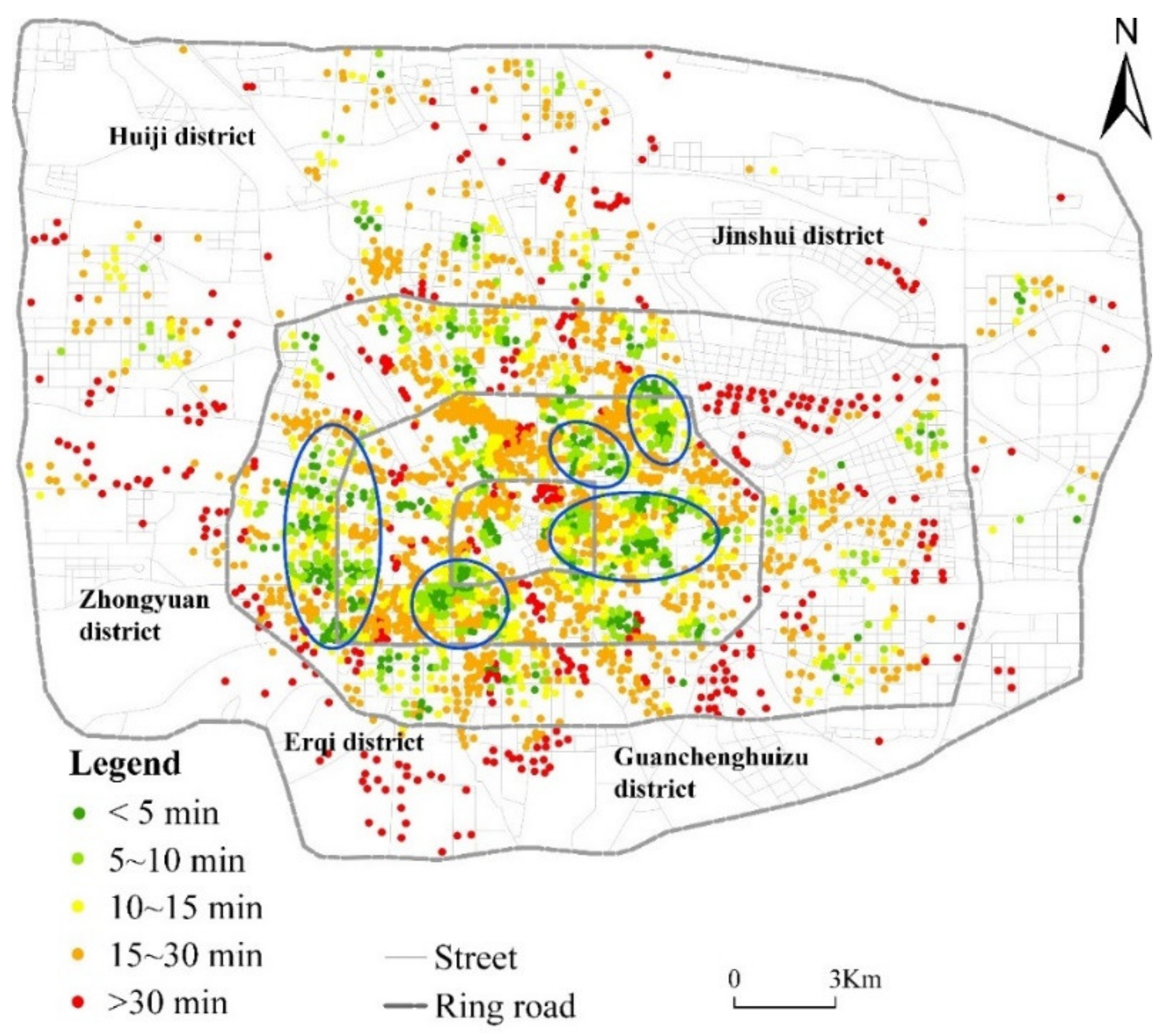
3.2. Potential Spatial Accessibility of Healthcare Services
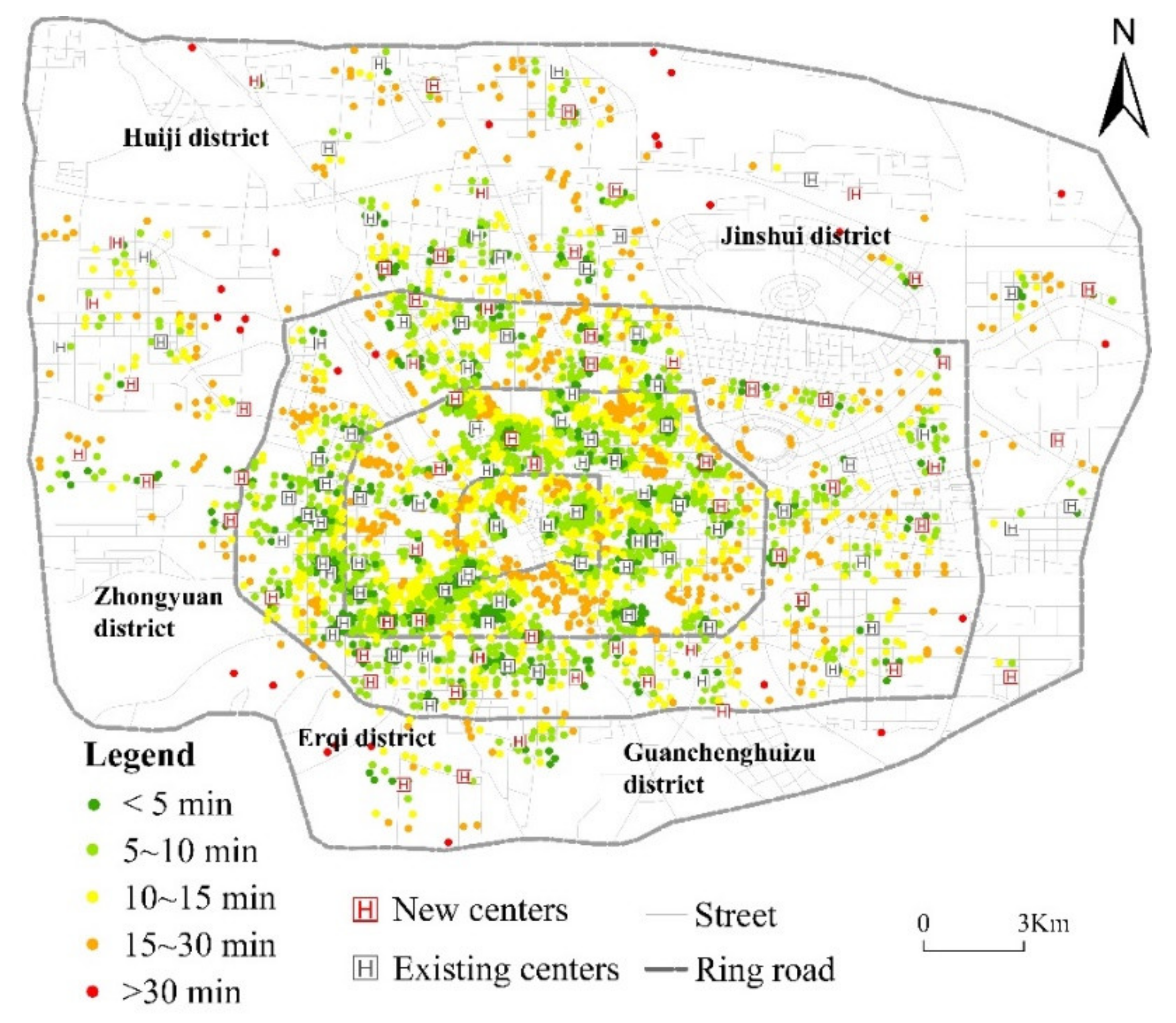
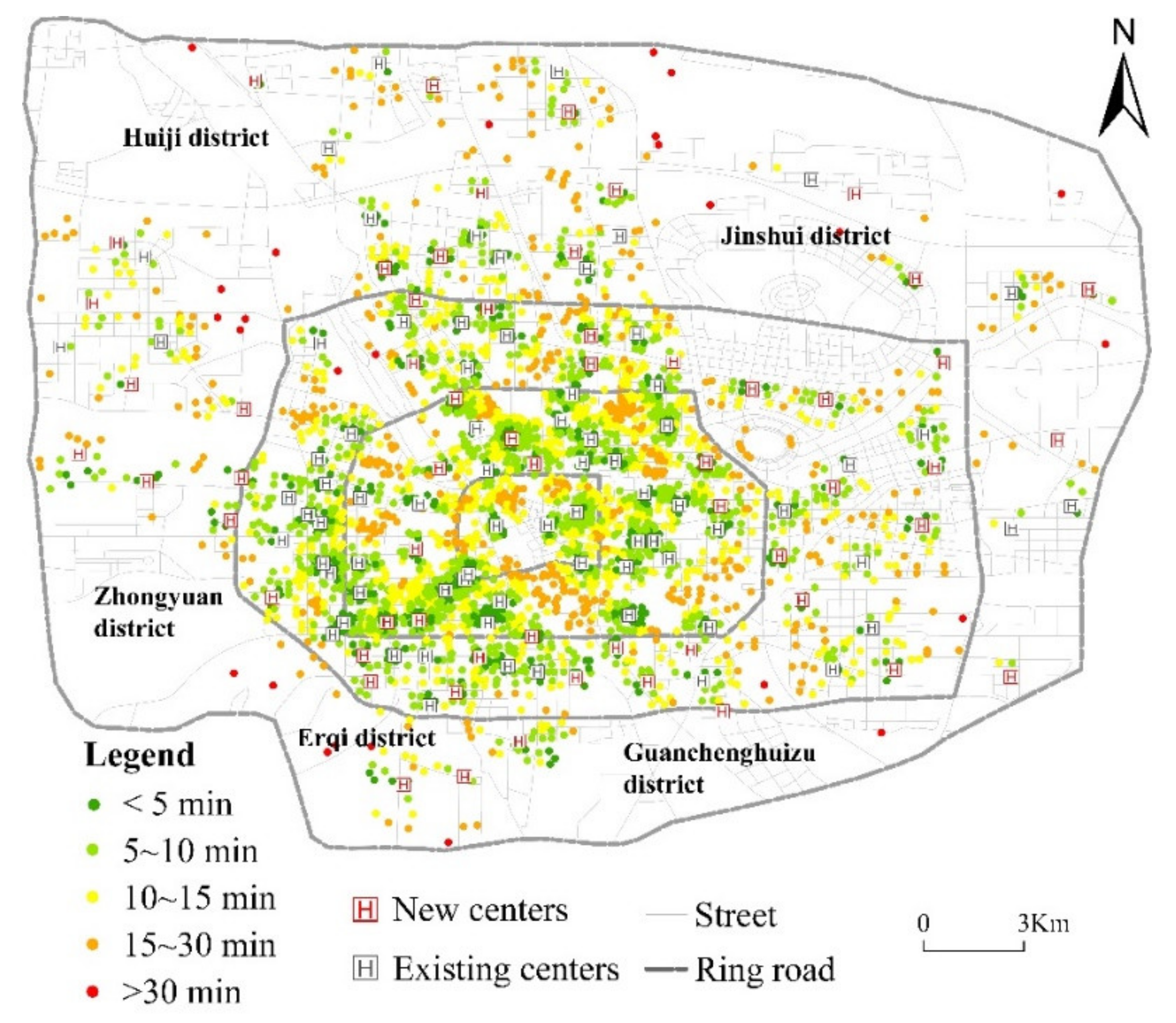
3.3. Improving the Spatial Accessibility of Healthcare Services
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shifa:, M.; David, A.; Leibbrandt, M. Spatial inequality through the prism of a pandemic: COVID-19 in South Africa. Sci. Rep. 2021, 13, e00949. [Google Scholar] [CrossRef] [PubMed]
- Alemdar, K.D.; Kaya, Ö.; Çodur, M.Y.; Campisi, T.; Tesoriere, G. Accessibility of vaccination centers in COVID-19 outbreak control: A GIS-Based multi-criteria decision making approach. ISPRS Int. J. Geo-Inf. 2021, 10, 708. [Google Scholar] [CrossRef]
- Kang, J.Y.; Michels, A.; Lyu, F.; Wang, S.; Agbodo, N.; Freeman, V.L.; Wang, S. Rapidly measuring spatial accessibility of COVID-19 healthcare resources: A case study of Illinois, USA. Int. J. Health Geogr. 2020, 19, 36. [Google Scholar] [CrossRef] [PubMed]
- Earle, L. Urban crises and the new urban agenda. Environ. Urban 2016, 28, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Klopp, J.M.; Petretta, D.L. The urban sustainable development goal: Indicators, complexity and the politics of measuring cities. Cities 2017, 63, 92–97. [Google Scholar] [CrossRef]
- Moreno, C.; Allam, Z.; Chabaud, D.; Gall, C.; Pratlong, F. Introducing the ‘15-minute city’: Sustainability, resilience and place identity in future post-pandemic cities. Smart Cities 2021, 4, 93–111. [Google Scholar] [CrossRef]
- Weng, M.; Ding, N.; Li, J.; Jin, X.; Xiao, H.; He, Z.; Su, S. The 15-minute walkable neighborhoods: Measurement, social inequalities and implications for building healthy communities in urban China. J. Transp. Health 2019, 13, 259–273. [Google Scholar] [CrossRef]
- Pozoukidou, G.; Chatziyiannaki, Z. 15-Minute City: Decomposing the new urban planning eutopia. Sustainability 2021, 13, 928. [Google Scholar] [CrossRef]
- Caselli, B.; Carra, M.; Rossetti, S.; Zazzi, M. Exploring the 15-minute neighbourhoods. An evaluation based on the walkability performance to public facilities. Procedia Comput. Sci. 2022, 60, 346–353. [Google Scholar] [CrossRef]
- Balletto, G.; Ladu, M.; Milesi, A.; Campisi, T.; Borruso, G. Walkability and city users. Critical analysis of opportunities and risks. In Proceedings of the 1st Conference on Future Challenges in Sustainable Urban Planning & Territorial Management, Sciforum Platform, 17–19 January 2022. [Google Scholar] [CrossRef]
- GB50180-2018; Urban Residential Area Planning and Design Standards. Ministry of Housing and Urban-Rural Development of the People’s Republic of China: Beijing, China, 2018.
- Wu, H.; Wang, L.; Zhang, Z.; Gao, J. Analysis and optimization of 15-minute community life circle based on supply and demand matching: A case study of Shanghai. PLoS ONE 2021, 16, e0256904. [Google Scholar] [CrossRef]
- Allam, Z.; Nieuwenhuijsen, M.; Chabaud, D.; Moreno, C. The 15-minute city offers a new framework for sustainability, liveability, and health. Lancet Planet. Health 2022, 6, 181–183. [Google Scholar] [CrossRef]
- Montgomery, M.R. World Development Report 2009: Reshaping Economic Geography; The World Bank: Washington, DC, USA, 2009; Available online: http://hdl.handle.net/10986/5991 (accessed on 10 June 2021).
- Pansiri, J.; Mmereki, R.N. Using the SERVQUAL model to evaluate the impact of public service reforms in the provision of primary health care in Botswana. J. Afr. Bus. 2010, 11, 219–234. [Google Scholar] [CrossRef]
- Ding, H.; Xu, Y.; Zheng, K.F. Establishment of performance evaluation indicator system for community health service. Chin. Health Qual. Manag. 2016, 23, 113–115. [Google Scholar] [CrossRef]
- Chen, Y.T.; Liu, Y. Research on performance optimization of government purchasing community health services based on tripartite game. J. Xiangtan Univ. 2020, 44, 39–45. [Google Scholar] [CrossRef]
- Qiu, C.L.; Xu, X.; Wang, H.R. Status of resource allocation of community health center in main labor distribution regions of Shenzhen. Chin. Gen. Pract. 2013, 16, 33–36. [Google Scholar] [CrossRef]
- Tang, L.J.; Wang, C.Q.; Qian, D.F. Study on resource allocation and service provision of community health institutions under the background of aging: A case study of Jiangsu province. Chin. J. Health Policy 2020, 13, 33–39. [Google Scholar] [CrossRef]
- Griffin, P.M.; Scherrer, C.R.; Swann, J.L. Optimization of community health center locations and service offerings with statistical need estimation. IIE Trans. 2008, 40, 880–892. [Google Scholar] [CrossRef]
- Shariff, S.; Moin, N.H.; Omar, M. Location allocation modeling for healthcarefacility planning in Malaysia. Comput. Ind. Eng. 2012, 62, 1000–1010. [Google Scholar] [CrossRef]
- Zhao, L.Z.; Gao, S.Q. Research on optimization of community health service facilities layout based on population density: Taking Central Urban area of Beijing for an example. Urban Dev. Stud. 2020, 27, 26–32. [Google Scholar]
- Ahmadi-Javid, A.; Seyedi, P.; Syam, S.S. A survey of healthcare facility location. Comput. Oper. Res. 2017, 79, 223–263. [Google Scholar] [CrossRef]
- Revelle, C.; Marks, D.; Liebman, J.C. An analysis of private and public sector location models. Manag. Sci. 1970, 16, 692–707. [Google Scholar] [CrossRef]
- Toregas, C.; Swain, R.; ReVelle, C.; Bergman, L. The location of emergency service facilities. Oper. Res. 1971, 19, 1363–1373. [Google Scholar] [CrossRef]
- Church, R.; ReVelle, C. The Maximal Covering Location Problem. In Papers of the Regional Science Association; Springer: Berlin/Heidelberg, Germany, 1974; Volume 32, pp. 101–118. [Google Scholar] [CrossRef]
- Daskin, M.S.; Hesse, S.M.; Revelle, C.S. α-Reliable p-minimax regret: A new model for strategic facility location modeling. Locat. Sci. 1997, 5, 227–246. [Google Scholar] [CrossRef]
- Widener, M.J.; Horner, M.W. A hierarchical approach to modeling hurricane disaster relief goods distribution. J. Transp. Geogr. 2011, 19, 821–828. [Google Scholar] [CrossRef]
- Yaghini, M.; Karimi, M.; Rahbar, M. A hybrid metaheuristic approach for the capacitated p-median problem. Appl. Soft Comput. 2013, 13, 3922–3930. [Google Scholar] [CrossRef]
- Xu, J.; Yin, X.; Chen, D.; An, J.; Nie, G. Multi-criteria location model of earthquake evacuation shelters to aid in urban planning. Int. J. Disaster Risk Reduct. 2016, 20, 51–62. [Google Scholar] [CrossRef]
- Kocatepe, A.; Ozguven, E.E.; Horner, M.; Ozel, H. Pet- and special needs-friendly shelter planning in south florida: A spatial capacitated p-median-based approach. Int. J. Disaster Risk Reduct. 2018, 31, 1207–1222. [Google Scholar] [CrossRef]
- Gu, X.; Tao, S.; Dai, B. Spatial accessibility of country parks in Shanghai, China. Urban For. Urban Green. 2017, 27, 373–382. [Google Scholar] [CrossRef]
- Shin, K.; Lee, T. Improving the measurement of the Korean emergency medical System’s spatial accessibility. Appl. Geogr. 2018, 100, 30–38. [Google Scholar] [CrossRef]
- Wang, X.; Yang, H.; Duan, Z.; Pan, J. Spatial accessibility of primary healthcare in China: A case study in Sichuan Province. Soc. Sci. Med. 2018, 209, 14–24. [Google Scholar] [CrossRef]
- Yiannakoulias, N.; Bland, W.; Svenson, L.W. Estimating the effect of turn penalties and traffic congestion on measuring spatial accessibility to primary healthcare. Appl. Geogr. 2013, 39, 172–182. [Google Scholar] [CrossRef]
- Järv, O.; Tenkanen, H.; Salonen, M.; Ahas, R.; Toivonen, T. Dynamic cities: Location-based accessibility modelling as a function of time. Appl. Geogr. 2018, 95, 101–110. [Google Scholar] [CrossRef]
- Kwan, M.-P.; Murray, A.T.; O’Kelly, M.E.; Tiefelsdorf, M. Recent advances in accessibility research: Representation, methodology and applications. J. Geogr. Syst. 2003, 5, 129–138. [Google Scholar] [CrossRef]
- Zhang, Q.; Northridge, M.E.; Jin, Z.; Metcalf, S.S. Modeling accessibility of screening and treatment facilities for older adults using transportation networks. Appl. Geogr. 2018, 93, 64–75. [Google Scholar] [CrossRef]
- Joseph, A.E.; Bantock, P.R. Measuring potential physical accessibility to general practitioners in rural areas: A method and case study. Soc. Sci. Med. 1982, 16, 85–90. [Google Scholar] [CrossRef]
- Onega, T.; Duell, E.J.; Shi, X. Geographic access to cancer care in the US. Cancer 2008, 112, 909–918. [Google Scholar] [CrossRef]
- Schuurman, N.; Berube, M.; Crooks, V.A. Measuring potential spatial access to primary healthcare physicians using a modified gravity model. Cancer Geogr. 2010, 54, 29–45. [Google Scholar] [CrossRef]
- Xia, N.; Cheng, L.; Chen, S.; Wei, X.; Zong, W.; Li, M. Accessibility based on gravity-radiation model and google maps API: A case study in Australia. J. Transp. Geogr. 2018, 72, 178–190. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of spatial accessibility to healthcare in a GIS environment: Synthesis and a case study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Whippo, T. Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health Place 2012, 18, 789–795. [Google Scholar] [CrossRef]
- Reshadat, S.; Zangeneh, A.; Saeidi, S.; Teimouri, R.; Yigitcanlar, T. Measures of spatial accessibility to health centers: Investigating urban and rural disparities in Kermanshah, Iran. J. Public Health 2019, 27, 519–529. [Google Scholar] [CrossRef]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Spencer, J.; Angeles, G. Kernel density estimation as a technique for assessing availability of health services in Nicaragua. Health Serv. Outcomes Res. Methodol. 2007, 7, 145–157. [Google Scholar] [CrossRef]
- Ghorbanzadeh, M.; Kim, K.; Erman Ozguven, E.; Horner, M.W. Spatial accessibility assessment of COVID-19 patients to healthcare facilities: A case study of Florida. Travel Behav. Soc. 2021, 24, 95–101. [Google Scholar] [CrossRef]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary care in rural areas: Improving the effectiveness of the two-step floating catchment area method. Appl. Geogr. 2009, 29, 533–541. [Google Scholar] [CrossRef]
- Wang, F. Measurement, optimization, and impact of healthcare accessibility: A methodological review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary healthcare services: Utilising dynamic catchment sizes. Appl. Geogr. 2014, 54, 182–188. [Google Scholar] [CrossRef]
- Pu, Q.; Yoo, E.-H.; Rothstein, D.H.; Cairo, S.; Malemo, L. Improving the spatial accessibility of healthcare in North Kivu, Democratic Republic of Congo. Appl. Geogr. 2020, 121, 102262. [Google Scholar] [CrossRef]
- Cetin, M. Using GIS analysis to assess urban green space in terms of accessibility: Case study in Kutahya. Int. J. Sustain. Dev. World Ecol. 2015, 22, 420–424. [Google Scholar] [CrossRef]
- Liu, D.; Kwan, M.-P.; Kan, Z. Analysis of urban green space accessibility and distribution inequity in the City of Chicago. Urban For. Urban Green. 2021, 59, 127029. [Google Scholar] [CrossRef]
- Li, M.T.; Yang, L.B.; Wei, Y. Improved Gaussian based 2-step floating catchment area method: A case study of green space accessibility in Shanghai. Prog. Geogr. 2016, 35, 990–996. Available online: http://www.progressingeography.com/CN/10.18306/dlkxjz.2016.08.008 (accessed on 15 June 2021).
- Xu, Y.; Song, W.X.; Liu, C.H. Social-spatial accessibility to urban educational resources under the school district system: A case study of public primary schools in Nanjing, China. Sustainability 2018, 10, 2305. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Chen, Y.; Wu, J.; Xu, T.; Gao, L.; Zhao, X. Mapping spatial accessibility of public transportation network in an urban area—A case study of Shanghai Hongqiao transportation Hub. Transp. Res. D Transp. Environ. 2018, 59, 478–495. [Google Scholar] [CrossRef]
- Chen, X.; Jia, P. A comparative analysis of accessibility measures by the two-step floating catchment area (2SFCA) method. Int. J. Geogr. Inf. Sci. 2019, 33, 1739–1758. [Google Scholar] [CrossRef]
- Zhai, S.; He, X.; Kong, Y.; Luo, J.; Song, G. Measuring spatial accessibility of public service by optimal supply-demand allocation. Acta Geogr. Sin. 2022, 77, 1028–1038. [Google Scholar] [CrossRef]
- Rong, P.; Zheng, Z.; Kwan, M.P.; Qin, Y. Evaluation of the spatial equity of medical facilities based on improved potential model and map service API: A case study in Zhengzhou, China. Appl. Geogr. 2020, 119, 102192. [Google Scholar] [CrossRef]
- Zhengzhou, S.B.O. Zhengzhou Statistical Yearbook 2020; China Statistics Press: Beijing, China, 2021; Available online: https://navi.cnki.net/knavi/yearbooks/YZZTJ/detail (accessed on 1 October 2021).
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Zhao, P.; Li, S.; Liu, D. Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef]
- Chai, Y.; Li, C. Urban life cycle planning: From research to practice. City Plan. Rev. 2019, 43, 9–16, +60. [Google Scholar]
- Sun, D.; Chai, Y.; Zhang, y. The definition and measurement of community life circle: A case study of Qinghe Area in Beijing. Urban Dev. Stud. 2016, 23, 1–9. [Google Scholar]
- Cheng, R. Planning and Practice of a 15-Minute Community Living Circle in Shanghai Guided by Promoting Implementation. Shanghai Urban Plan. Rev. 2018, 2, 84–88. [Google Scholar]
- Du, G.; Sun, C. Location planning problem of service centers for sustainable home healthcare: Evidence from the empirical analysis of Shanghai. Sustainability 2015, 7, 15812–15832. [Google Scholar] [CrossRef] [Green Version]
- Gu, W.; Wang, X.; McGregor, S.E. Optimization of preventive healthcare facility locations. Int. J. Health Geogr. 2010, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Tian, L.; Luo, L.; Yi, H.; Wang, F. Two-Step optimization for spatial accessibility improvement: A case study of healthcare planning in rural China. Biomed. Res. Int. 2017, 2017, 2094654. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Hou, C.; Zhao, L.; Wang, S. Evaluation Of 15-minute public service level. Planners 2018, 34, 106–110. [Google Scholar]
- Liu, Q.; Qian, Z.; Huang, D.; Zhou, X. The characteristics of spatial pattern evolution and the trend of the 15-minute life circle. Urban Plan. Forum 2020, 6, 94–101. [Google Scholar]
- Thoughts, methodology, and practice: Symposium on the planning of 15-minute community-life circles. Urban Plan. Forum 2020, 1, 1–8.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ring Road | Number of Communities (%) | Population Size (%) | Number of Centers (%) |
|---|---|---|---|
| First ring | 279 (8.40) | 215,375 (4.44) | 5 (6.67) |
| Second ring | 1528 (46.01) | 1,436,335 (29.63) | 25 (33.33) |
| Third ring | 1072 (32.28) | 1,876,302 (38.71) | 30 (40.00) |
| Fourth ring | 442 (13.31) | 1,319,526 (27.22) | 15 (20.00) |
| <5 min (%) | <10 min (%) | <15 min (%) | <30 min (%) | >30 min (%) | Average Time (min) | |
|---|---|---|---|---|---|---|
| All | 8.28 | 23.08 | 39.57 | 78.93 | 21.07 | 18.25 |
| First ring | 7.29 | 22.83 | 39.82 | 89.8 | 10.2 | 16 |
| Second ring | 10.67 | 28.76 | 53.11 | 95.48 | 4.51 | 15.04 |
| Third ring | 10.68 | 27.37 | 43.41 | 79.44 | 20.57 | 18.69 |
| Fourth ring | 2.42 | 10.84 | 19.32 | 58.42 | 41.58 | 33.53 |
| <5 min (%) | <10 min (%) | <15 min (%) | <30 min (%) | >30 min (%) | Average Time (min) | |
|---|---|---|---|---|---|---|
| All | 9.63 | 29.18 | 48.11 | 81.64 | 18.35 | 16.48 |
| First ring | 8.36 | 47.57 | 78.78 | 100 | 0 | 10.45 |
| Second ring | 14.16 | 38.09 | 65.04 | 98.34 | 1.67 | 12.75 |
| Third ring | 11.13 | 32.36 | 51.24 | 84.72 | 15.28 | 16.71 |
| Fourth ring | 2.78 | 11.97 | 20.23 | 56.11 | 43.88 | 32.28 |
| Center Numbers | <5 min (%) | <10 min (%) | <15 min (%) | <30 min (%) | >30 min (%) | Average Time (min) |
|---|---|---|---|---|---|---|
| 75 | 8.28 | 23.08 | 39.57 | 78.93 | 21.07 | 18.25 |
| 85 | 11.41 | 35.38 | 59.81 | 93.02 | 6.98 | 13.35 |
| 95 | 12.76 | 39.54 | 65.88 | 96.13 | 3.87 | 12.25 |
| 105 | 14.63 | 44.31 | 70.61 | 96.64 | 3.36 | 11.41 |
| 115 | 16.79 | 48.54 | 74.53 | 96.86 | 3.14 | 10.8 |
| 125 | 17.92 | 52.35 | 78.46 | 97.14 | 2.86 | 10.35 |
| 135 | 19.05 | 54.5 | 80.11 | 97.87 | 2.13 | 10 |
| <5 min (%) | 5~10 min (%) | 10~15 min (%) | 15~30 min (%) | >30 min (%) | Average Time (min) | |
|---|---|---|---|---|---|---|
| All | 19.05 | 35.45 | 25.61 | 17.76 | 2.13 | 10.00 |
| First ring | 8.36 | 39.81 | 32.96 | 18.87 | 0.00 | 10.24 |
| Second ring | 19.88 | 38.49 | 28.82 | 12.80 | 0.00 | 9.34 |
| Third ring | 23.34 | 38.87 | 24.75 | 12.50 | 0.54 | 9.43 |
| Fourth ring | 13.78 | 26.57 | 22.13 | 30.47 | 7.05 | 13.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, G.; He, X.; Kong, Y.; Li, K.; Song, H.; Zhai, S.; Luo, J. Improving the Spatial Accessibility of Community-Level Healthcare Service toward the ‘15-Minute City’ Goal in China. ISPRS Int. J. Geo-Inf. 2022, 11, 436. https://doi.org/10.3390/ijgi11080436
Song G, He X, Kong Y, Li K, Song H, Zhai S, Luo J. Improving the Spatial Accessibility of Community-Level Healthcare Service toward the ‘15-Minute City’ Goal in China. ISPRS International Journal of Geo-Information. 2022; 11(8):436. https://doi.org/10.3390/ijgi11080436
Chicago/Turabian StyleSong, Genxin, Xinxin He, Yunfeng Kong, Ke Li, Hongquan Song, Shiyan Zhai, and Jingjing Luo. 2022. "Improving the Spatial Accessibility of Community-Level Healthcare Service toward the ‘15-Minute City’ Goal in China" ISPRS International Journal of Geo-Information 11, no. 8: 436. https://doi.org/10.3390/ijgi11080436
APA StyleSong, G., He, X., Kong, Y., Li, K., Song, H., Zhai, S., & Luo, J. (2022). Improving the Spatial Accessibility of Community-Level Healthcare Service toward the ‘15-Minute City’ Goal in China. ISPRS International Journal of Geo-Information, 11(8), 436. https://doi.org/10.3390/ijgi11080436