Prognostic Value of a Novel and Established High-Sensitivity Troponin I Assay in Patients Presenting with Suspected Myocardial Infarction

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.1.1. Biomarkers in Acute Cardiac Care Study Population
2.1.2. StenoCardia Study Population
2.2. Standard Diagnostic Approach and Adjudication of the Final Diagnosis
2.3. Patient Follow-Up
2.4. Troponin I Measurements
2.5. Singulex Clarity cTnI
2.6. Abbott ARCHITECT STAT hs-TnI
2.7. Statistical Analyses
3. Results
3.1. Baseline Characteristics
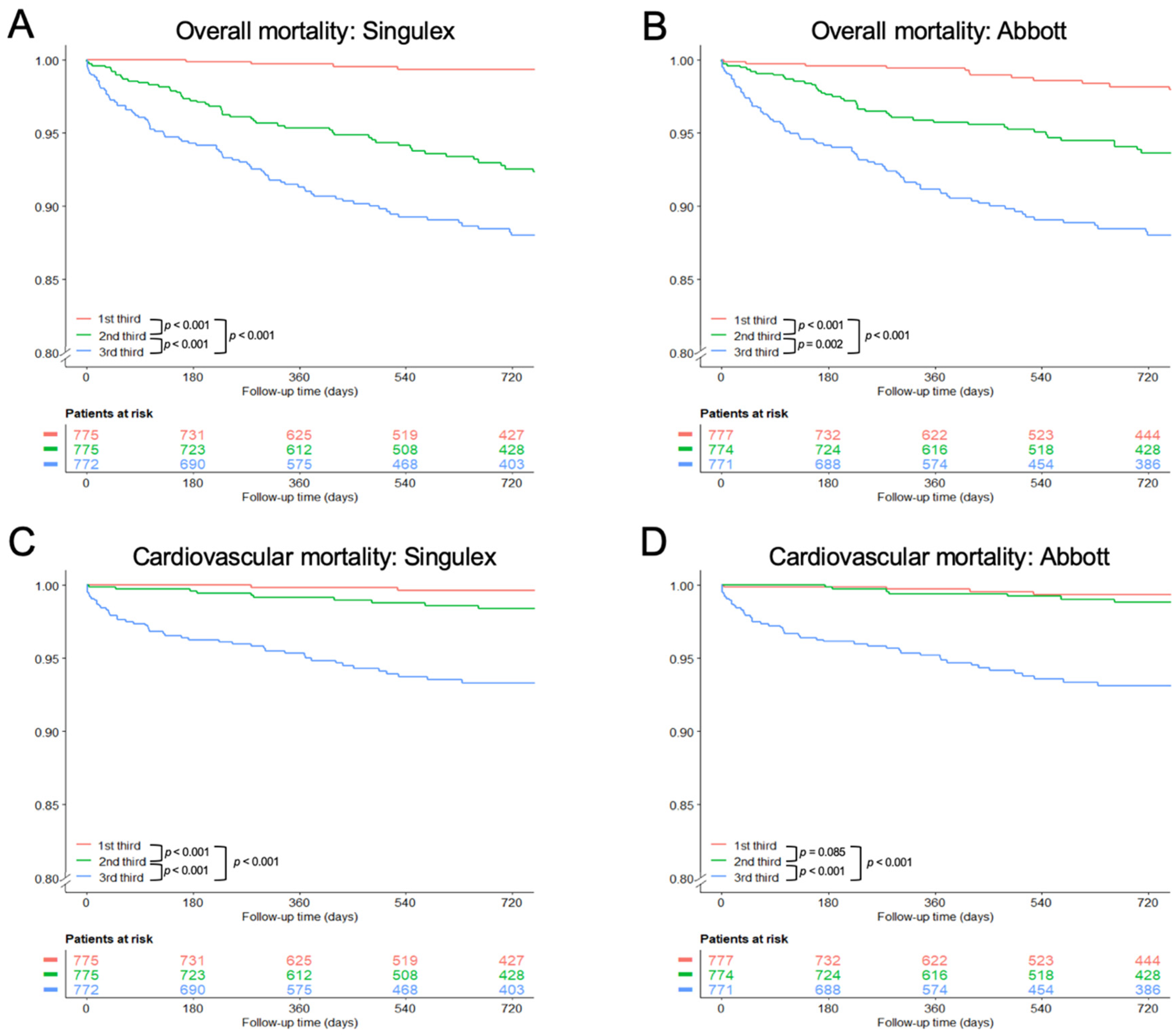
3.2. Survival Analysis According to Troponin Thirds
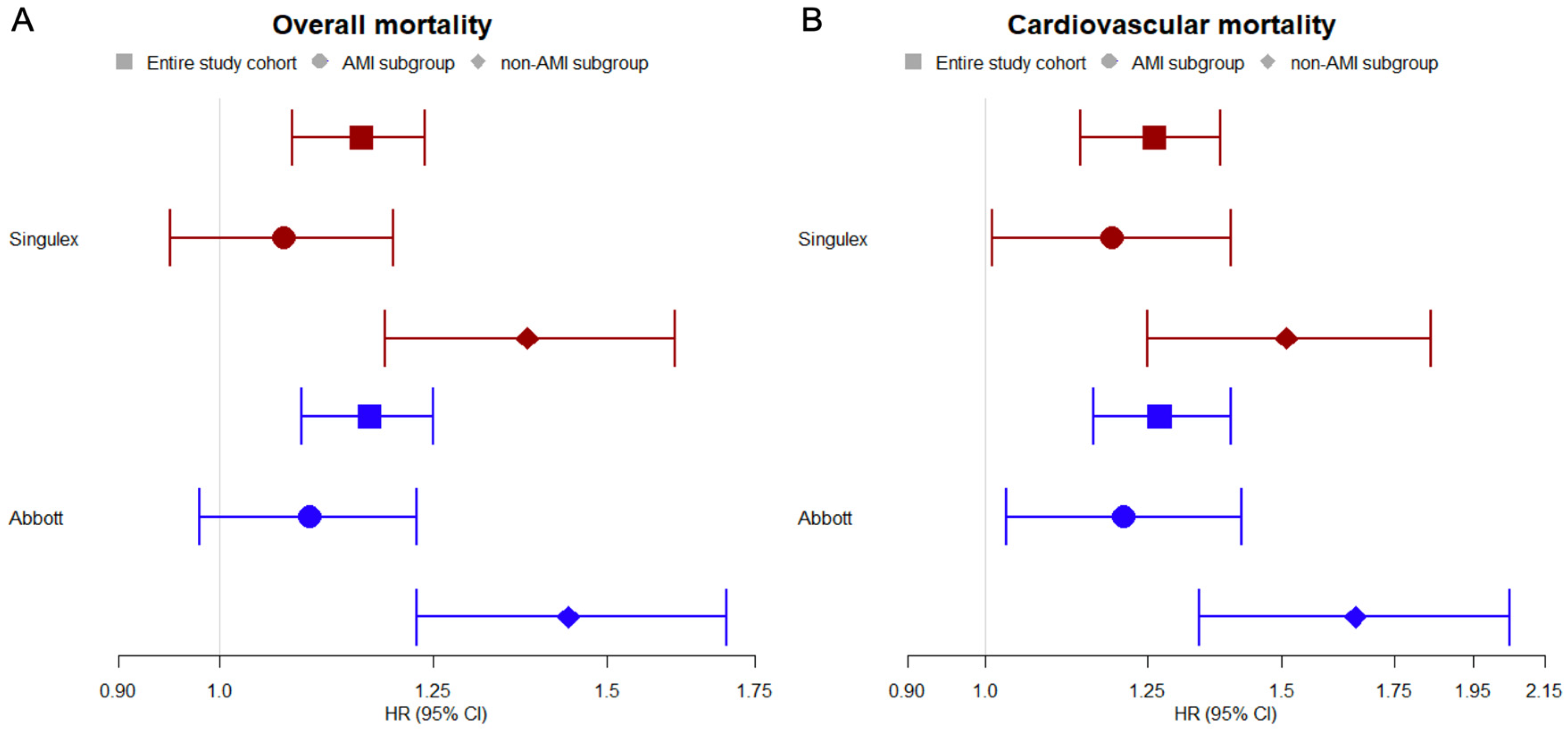
3.3. Prognostic Value of hs-TnI
4. Prediction of Adverse Outcome
5. Discussion
6. Conclusions
7. Disclosures
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Apple, F.S.; Collinson, P.O. Analytical characteristics of high-sensitivity cardiac troponin assays. Clin. Chem. 2012, 58, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Westermann, D.; Neumann, J.T.; Sörensen, N.A.; Blankenberg, S. High-sensitivity assays for troponin in patients with cardiac disease. Nat. Rev. Cardiol. 2017, 14, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Reichlin, T.; Schindler, C.; Drexler, B.; Twerenbold, R.; Reiter, M.; Zellweger, C.; Moehring, B.; Ziller, R.; Hoeller, R.; Rubini Gimenez, M.; et al. One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch. Intern. Med. 2012, 172, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Rubini Gimenez, M.; Twerenbold, R.; Jaeger, C.; Schindler, C.; Puelacher, C.; Wildi, K.; Reichlin, T.; Haaf, P.; Merk, S.; Honegger, U.; et al. One-hour Rule-in and Rule-out of Acute Myocardial Infarction Using High-sensitivity Cardiac Troponin I. Am. J. Med. 2015, 128, 861–870. [Google Scholar] [CrossRef]
- Neumann, J.T.; Sörensen, N.A.; Schwemer, T.; Ojeda, F.; Bourry, R.; Sciacca, V.; Schaefer, S.; Waldeyer, C.; Sinning, C.; Renné, T.; et al. Diagnosis of Myocardial Infarction Using a High-Sensitivity Troponin I 1-Hour Algorithm. JAMA Cardiol. 2016, 306, 2684–2693. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2015, 37, 267–315. [Google Scholar] [CrossRef] [PubMed]
- de Lemos, J.A.; Drazner, M.H.; Omland, T.; Ayers, C.R.; Khera, A.; Rohatgi, A.; Hashim, I.; Berry, J.D.; Das, S.R.; Morrow, D.A.; et al. Association of Troponin T Detected with a Highly Sensitive Assay and Cardiac Structure and Mortality Risk in the General Population. JAMA 2010, 304, 2503. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.T.; Havulinna, A.S.; Zeller, T.; Appelbaum, S.; Kunnas, T.; Nikkari, S.; Jousilahti, P.; Blankenberg, S.; Sydow, K.; Salomaa, V. Comparison of Three Troponins as Predictors of Future Cardiovascular Events—Prospective Results from the FINRISK and BiomaCaRE Studies. PLoS ONE 2014, 9, e90063. [Google Scholar] [CrossRef]
- Blankenberg, S.; Salomaa, V.; Makarova, N.; Ojeda, F.; Wild, P.; Lackner, K.J.; Jørgensen, T.; Thorand, B.; Peters, A.; Nauck, M.; et al. Troponin I and cardiovascular risk prediction in the general population: The BiomarCaRE consortium. Eur. Heart J. 2016, 37, 2428–2437. [Google Scholar] [CrossRef]
- Wang, T.J.; Wollert, K.C.; Larson, M.G.; Coglianese, E.; McCabe, E.L.; Cheng, S.; Ho, J.E.; Fradley, M.G.; Ghorbani, A.; Xanthakis, V.; et al. Prognostic utility of novel biomarkers of cardiovascular stress: The framingham heart study. Circulation 2012, 126, 1596–1604. [Google Scholar] [CrossRef]
- Chapman, A.R.; Lee, K.K.; McAllister, D.A.; Cullen, L.; Greenslade, J.H.; Parsonage, W.; Worster, A.; Kavsak, P.A.; Blankenberg, S.; Neumann, J.; et al. Association of High-Sensitivity Cardiac Troponin I Concentration with Cardiac Outcomes in Patients with Suspected Acute Coronary Syndrome. JAMA 2017, 318, 1913–1924. [Google Scholar] [CrossRef] [PubMed]
- Sörensen, N.A.; Neumann, J.T.; Ojeda, F.; Schwemer, T.; Renné, T.; Schnabel, R.B.; Zeller, T.; Karakas, M.; Blankenberg, S.; Westermann, D. Challenging the 99th percentile: A lower troponin cutoff leads to low mortality of chest pain patients. Int. J. Cardiol. 2017, 232, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.; Twerenbold, R.; Ojeda, F.; Sörensen, N.; Chapman, A.; Shah, A.; Anand, A.; Boeddinghaus, J.; Nestelberger, T.; Badertscher, P.; et al. Application of High-Sensitivity Troponin in Suspected Myocardial Infarction. N. Engl. J. Med. 2019, 380, 2529–2540. [Google Scholar] [CrossRef] [PubMed]
- Biener, M.; Giannitsis, E.; Kuhner, M.; Zelniker, T.; Mueller-Hennessen, M.; Vafaie, M.; Stoyanov, K.M.; Neumann, F.-J.; Katus, H.A.; Hochholzer, W.; et al. Risk prediction in stable cardiovascular disease using a high-sensitivity cardiac troponin T single biomarker strategy compared to the ESC-SCORE. Open Hear. 2018, 5, e000710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochholzer, W.; Reichlin, T.; Twerenbold, R.; Stelzig, C.; Hochholzer, K.; Meissner, J.; Haaf, P.; Schaub, N.; Steuer, S.; Bassetti, S.; et al. Incremental value of high-sensitivity cardiac troponin T for risk prediction in patients with suspected acute myocardial infarction. Clin. Chem. 2011, 57, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Lan, N.S.R.; Bell, D.A.; McCaul, K.A.; Vasikaran, S.D.; Yeap, B.B.; Norman, P.E.; Almeida, O.P.; Golledge, J.; Hankey, G.J.; Flicker, L. High-Sensitivity Cardiac Troponin I Improves Cardiovascular Risk Prediction in Older Men: HIMS (The Health in Men Study). J. Am. Heart Assoc. 2019, 8, e011818. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.T.; Sörensen, N.A.; Rübsamen, N.; Ojeda, F.; Schock, A.; Seddighizadeh, P.; Zeller, T.; Westermann, D.; Blankenberg, S. Evaluation of a new ultra-sensitivity troponin I assay in patients with suspected myocardial infarction. Int. J. Cardiol. 2018, 283, 35–40. [Google Scholar] [CrossRef]
- Garcia-Osuna, A.; Gaze, D.; Grau-Agramunt, M.; Morris, T.; Telha, C.; Bartolome, A.; Bishop, J.J.; Monsalve, L.; Livingston, R.; Estis, J.; et al. Ultrasensitive quantification of cardiac troponin I by a Single Molecule Counting method: Analytical validation and biological features. Clin. Chim. Acta 2018, 486, 224–231. [Google Scholar] [CrossRef]
- Apple, F.S.; Ler, R.; Murakami, M.M. Determination of 19 Cardiac Troponin I and T Assay 99th Percentile Values from a Common Presumably Healthy Population. Clin. Chem. 2012, 58, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Keller, T.; Zeller, T.; Ojeda, F.; Tzikas, S.; Lillpopp, L.; Sinning, C.; Wild, P.; Genth-Zotz, S.; Warnholtz, A.; Giannitsis, E.; et al. Serial changes in highly sensitive troponin I assay and early diagnosis of myocardial infarction. JAMA 2011, 306, 2684–2693. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Katus, H.A.; Apple, F.S.; Lindahl, B.; Morrow, D.A.; et al. Third universal definition of myocardial infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeller, T.; Ojeda, F.; Brunner, F.J.; Peitsmeyer, P.; Münzel, T.; Binder, H.; Pfeiffer, N.; Michal, M.; Wild, P.S.; Blankenberg, S.; et al. High-sensitivity cardiac troponin I in the general population–defining reference populations for the determination of the 99th percentile in the Gutenberg Health Study. Clin. Chem. Lab. Med. 2015, 53, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Antolini, L.; Nam, B.H.; D’Agostino, R.B. Inference on correlated discrimination measures in survival analysis: A nonparametric approach. Commun. Stat. Theory Methods 2004, 33, 2117–2135. [Google Scholar] [CrossRef]
- R Development Team Core. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org (accessed on 9 September 2019).
- Newton-Cheh, C.; Tofler, G.H.; Robins, S.J.; Selhub, J.; Larson, M.G.; Levy, D.; D’Agostino, R.B.; Rifai, N.; Wang, T.J.; Vasan, R.S.; et al. Multiple Biomarkers for the Prediction of First Major Cardiovascular Events and Death. N. Engl. J. Med. 2006, 355, 2631–2639. [Google Scholar] [Green Version]
- Zeller, T.; Peetz, D.; Tiret, L.; Jachmann, N.; Nicaud, V.; Wild, P.S.; Bickel, C.; Baldus, S.; Roth, A.; Sinning, C.R.; et al. Sensitive Troponin I Assay in Early Diagnosis of Acute Myocardial Infarction. N. Engl. J. Med. 2009, 361, 868–877. [Google Scholar]
- Kaess, B.M.; de las Heras Gala, T.; Zierer, A.; Meisinger, C.; Wahl, S.; Peters, A.; Todd, J.; Herder, C.; Huth, C.; Thorand, B.; et al. Ultra-sensitive troponin I is an independent predictor of incident coronary heart disease in the general population. Eur. J. Epidemiol. 2017, 32, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Welsh, P.; Evans, J.D.W.; Tschiderer, L.; Boachie, C.; Jukema, J.W.; Ford, I.; Trompet, S.; Stott, D.J.; Kearney, P.M.; et al. High-Sensitivity Cardiac Troponin Concentration and Risk of First-Ever Cardiovascular Outcomes in 154,052 Participants. J. Am. Coll. Cardiol. 2017, 70, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Hammarsten, O.; Fu, M.L.X.; Sigurjonsdottir, R.; Petzold, M.; Said, L.; Landin-Wilhelmsen, K.; Widgren, B.; Larsson, M.; Johanson, P. Troponin T percentiles from a random population sample, emergency room patients and patients with myocardial infarction. Clin. Chem. 2012, 58, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Apple, F.S.; Diercks, D.; Peacock, W.F.; Wu, A.H.B.; De Marco, T.; Wynne, J.; Fonarow, G.C. Cardiac Troponin and Outcome in Acute Heart Failure. N. Engl. J. Med. 2008, 358, 2117–2126. [Google Scholar]
- Ahmed, A.N.; Blonde, K.; Hackam, D.; Iansavichene, A.; Mrkobrada, M. Prognostic significance of elevated troponin in non-cardiac hospitalized patients: A systematic review and meta-analysis. Ann. Med. 2014, 46, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Roos, A.; Bandstein, N.; Lundbäck, M.; Hammarsten, O.; Ljung, R.; Holzmann, M.J. Stable High-Sensitivity Cardiac Troponin T Levels and Outcomes in Patients with Chest Pain. J. Am. Coll. Cardiol. 2017, 70, 2226–2236. [Google Scholar] [CrossRef] [PubMed]
- Roos, A.; Hellgren, A.; Rafatnia, F.; Hammarsten, O.; Ljung, R.; Carlsson, A.C.; Holzmann, M.J. Investigations, findings, and follow-up in patients with chest pain and elevated high-sensitivity cardiac troponin T levels but no myocardial infarction. Int. J. Cardiol. 2017, 232, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Antman, E.M.; Tanasijevic, M.J.; Thompson, B.; Schactman, M.; McCabe, C.H.; Cannon, C.P.; Fischer, G.A.; Fung, A.Y.; Thompson, C.; Wybenga, D.; et al. Cardiac-Specific Troponin I Levels to Predict the Risk of Mortality in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 1996, 335, 1342–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 70, 1082. [Google Scholar]
- Eggers, K.M.; Lagerqvist, B.; Venge, P.; Wallentin, L.; Lindahl, B. Persistent cardiac troponin I elevation in stabilized patients after an episode of acute coronary syndrome predicts long-term mortality. Circulation 2007, 116, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Chia, S.; Senatore, F.; Raffel, O.C.; Lee, H.; Wackers, F.J.T.; Jang, I.K. Utility of Cardiac Biomarkers in Predicting Infarct Size, Left Ventricular Function, and Clinical Outcome After Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2008, 1, 415–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All (n = 2332) | AMI (n = 518) | non-AMI (n = 1814) | p-Value | |
|---|---|---|---|---|
| Age (years) | 64.0 (52.0, 74.0) | 68.0 (58.0, 75.0) | 62.0 (50.0, 73.0) | <0.001 |
| Sex (male) No. (%) | 1508 (64.7) | 368 (71.0) | 1140 (62.8) | <0.001 |
| Current smoker No. (%) | 567 (24.5) | 161 (31.2) | 406 (22.5) | <0.001 |
| Diabetes No. (%) | 334 (14.5) | 95 (18.5) | 239 (13.3) | 0.0041 |
| Body mass index (kg/m²) | 26.5 (24.0, 30.0) | 26.7 (24.1, 29.8) | 26.4 (23.9, 30.1) | 0.71 |
| Hypertension No. (%) | 1610 (69.2) | 397 (76.8) | 1213 (67.0) | <0.001 |
| Dyslipoproteinemia No. (%) | 1129 (48.4) | 287 (55.4) | 842 (46.4) | <0.001 |
| History of AMI No. (%) | 412 (17.8) | 112 (21.7) | 300 (16.6) | 0.0093 |
| History of coronary artery disease No. (%) | 791 (34.1) | 200 (38.6) | 591 (32.8) | 0.015 |
| Family history of coronary artery disease No. (%) | 521 (23.0) | 110 (22.0) | 411 (23.3) | 0.59 |
| Atrial fibrillation No. (%) | 382 (16.5) | 81 (15.7) | 301 (16.7) | 0.65 |
| Heart failure No. (%) | 217 (9.4) | 64 (12.4) | 153 (8.5) | 0.0088 |
| eGFR (mL/min for 1.73 m²) | 77.6 (61.4, 91.8) | 70.1 (54.9, 85.5) | 80.3 (64.0, 92.9) | <0.001 |
| GRACE Score > 140 No. (%) | 245 (10.9) | 96 (19.3) | 149 (8.5) | <0.001 |
| hs-TnI 0h Singulex (ng/L) | 2.3 (1.0, 10.4) | 88.3 (13.8, 616.9) | 1.6 (0.8, 3.8) | <0.001 |
| hs-TnI 0h Abbott (ng/L) | 6.8 (3.1, 25.3) | 182.8 (26.7, 1404.6) | 5.0 (2.6, 10.6) | <0.001 |
| Prediction Models | C-Index | |
|---|---|---|
| Overall mortality | Age, sex, CVRFs | 0.761 (0.709, 0.813) |
| Age, sex, CVRFs + TnI (Singulex) | 0.771 (0.719, 0.824) | |
| C-index difference; p-value | 0.01; 0.08 | |
| Age, sex, CVRFs | 0.761 (0.709, 0.813) | |
| Age, sex, CVRFs + TnI (Abbott) | 0.773 (0.720, 0.825) | |
| C-index difference; p-value | 0.012; 0.074 | |
| Cardiovascular mortality | Age, sex, CVRFs | 0.783 (0.706, 0.860) |
| Age, sex, CVRFs + TnI (Singulex) | 0.821 (0.744, 0.898) | |
| C-index difference; p-value | 0.038; 0.001 | |
| Age, sex, CVRFs | 0.783 (0.706, 0.860) | |
| Age, sex, CVRFs + TnI (Abbott) | 0.825 (0.748, 0.902) | |
| C-index difference; p-value | 0.042; <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sörensen, N.A.; Ludwig, S.; Makarova, N.; Neumann, J.T.; Lehmacher, J.; Hartikainen, T.S.; Haller, P.M.; Keller, T.; Blankenberg, S.; Westermann, D.; et al. Prognostic Value of a Novel and Established High-Sensitivity Troponin I Assay in Patients Presenting with Suspected Myocardial Infarction. Biomolecules 2019, 9, 469. https://doi.org/10.3390/biom9090469
Sörensen NA, Ludwig S, Makarova N, Neumann JT, Lehmacher J, Hartikainen TS, Haller PM, Keller T, Blankenberg S, Westermann D, et al. Prognostic Value of a Novel and Established High-Sensitivity Troponin I Assay in Patients Presenting with Suspected Myocardial Infarction. Biomolecules. 2019; 9(9):469. https://doi.org/10.3390/biom9090469
Chicago/Turabian StyleSörensen, Nils A., Sebastian Ludwig, Nataliya Makarova, Johannes T. Neumann, Jonas Lehmacher, Tau S. Hartikainen, Paul M. Haller, Till Keller, Stefan Blankenberg, Dirk Westermann, and et al. 2019. "Prognostic Value of a Novel and Established High-Sensitivity Troponin I Assay in Patients Presenting with Suspected Myocardial Infarction" Biomolecules 9, no. 9: 469. https://doi.org/10.3390/biom9090469
APA StyleSörensen, N. A., Ludwig, S., Makarova, N., Neumann, J. T., Lehmacher, J., Hartikainen, T. S., Haller, P. M., Keller, T., Blankenberg, S., Westermann, D., Zeller, T., & Schofer, N. (2019). Prognostic Value of a Novel and Established High-Sensitivity Troponin I Assay in Patients Presenting with Suspected Myocardial Infarction. Biomolecules, 9(9), 469. https://doi.org/10.3390/biom9090469