Elevated Plasma microRNA-206 Levels Predict Cognitive Decline and Progression to Dementia from Mild Cognitive Impairment

 ,
,  ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Collection
2.3. Neuropsychological Assessment
2.4. RNA Extraction and OpenArray Profiling
2.5. Individual RT-qPCR
2.6. MiRNA Electrochemical Detection
2.7. Statistical Analysis
3. Results
3.1. MicroRNA Profiling in Patient Plasma
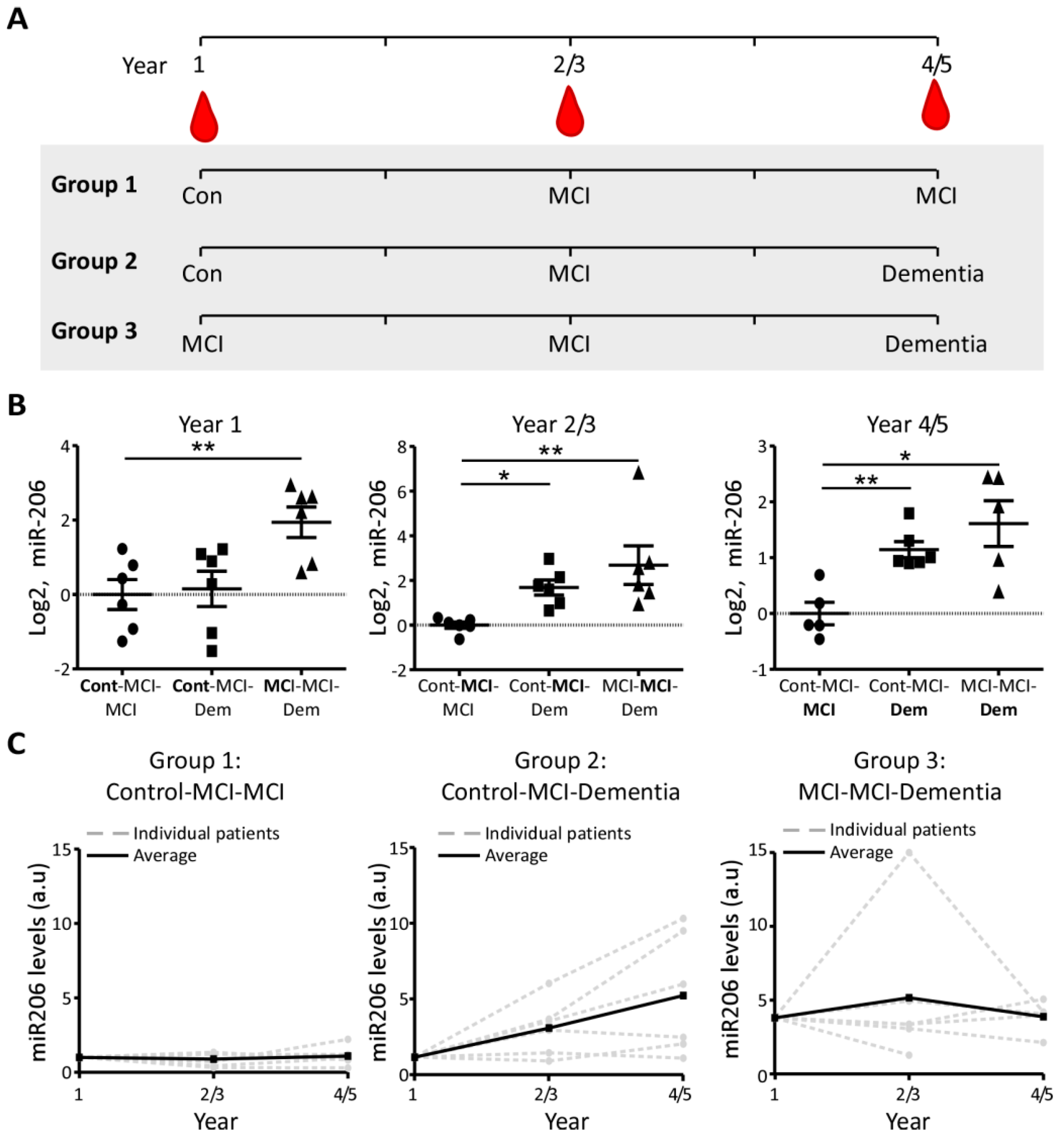
3.2. Increased miR-206 Plasma Levels Predict Cognitive Decline during MCI
3.3. MiR-206 Plasma Concentration in Longitudinal Sampling
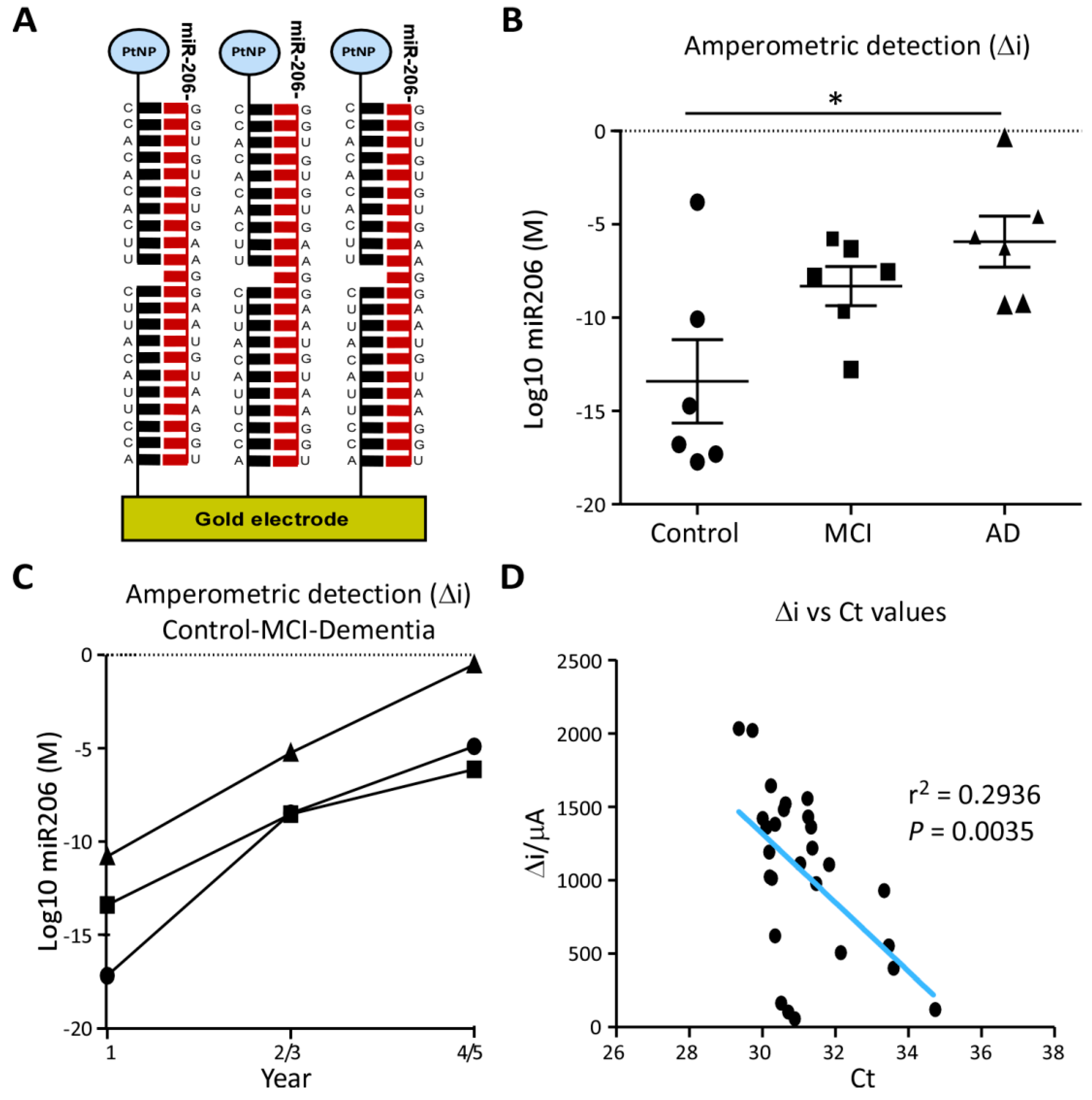
3.4. Prototype Clinical Assay for AD Risk
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Mehta, D.; Jackson, R.; Paul, G.; Shi, J.; Sabbagh, M. Why do trials for Alzheimer’s disease drugs keep failing? A discontinued drug perspective for 2010-2015. Expert Opin. Investig. Drugs 2017, 26, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Salloway, S.; Sperling, R.; Fox, N.C.; Blennow, K.; Klunk, W.; Raskind, M.; Sabbagh, M.; Honig, L.S.; Porsteinsson, A.P.; Ferris, S.; et al. Two Phase 3 Trials of Bapineuzumab in Mild-to-Moderate Alzheimer’s Disease. N. Engl. J. Med. 2014, 370, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Honig, L.S.; Vellas, B.; Woodward, M.; Boada, M.; Bullock, R.; Borrie, M.; Hager, K.; Andreasen, N.; Scarpini, E.; Liu-Seifert, H.; et al. Trial of Solanezumab for Mild Dementia Due to Alzheimer’s Disease. N. Engl. J. Med. 2018, 378, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Sutphen, C.L.; Jasielec, M.S.; Shah, A.R.; Macy, E.M.; Xiong, C.; Vlassenko, A.G.; Benzinger, T.L.S.; Stoops, E.E.J.; Vanderstichele, H.M.J.; Brix, B.; et al. Longitudinal Cerebrospinal Fluid Biomarker Changes in Preclinical Alzheimer Disease During Middle AgeCerebrospinal Fluid Biomarker Changes in Preclinical Alzheimer DiseaseCerebrospinal Fluid Biomarker Changes in Preclinical Alzheimer Disease. JAMA Neurol. 2015, 72, 1029–1042. [Google Scholar] [CrossRef]
- Dubois, B.; Hampel, H.; Feldman, H.H.; Scheltens, P.; Aisen, P.; Andrieu, S.; Bakardjian, H.; Benali, H.; Bertram, L.; Blennow, K.; et al. Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement. 2016, 12, 292–323. [Google Scholar] [CrossRef]
- Epelbaum, S.; Genthon, R.; Cavedo, E.; Habert, M.O.; Lamari, F.; Gagliardi, G.; Lista, S.; Teichmann, M.; Bakardjian, H.; Hampel, H.; et al. Preclinical Alzheimer’s disease: A systematic review of the cohorts underlying the concept. Alzheimers Dement. 2017, 13, 454–467. [Google Scholar] [CrossRef]
- Cummings, J.L.; Morstorf, T.; Zhong, K. Alzheimer’s disease drug-development pipeline: Few candidates, frequent failures. Alzheimers Res. 2014, 6, 37. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Dekosky, S.T.; Barberger-Gateau, P.; Cummings, J.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G.; et al. Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef]
- Okello, A.; Koivunen, J.; Edison, P.; Archer, H.A.; Turkheimer, F.E.; Någren, K.; Bullock, R.; Walker, Z.; Kennedy, A.; Fox, N.C.; et al. Conversion of amyloid positive and negative MCI to AD over 3 years: An 11C-PIB PET study. Neurology 2009, 73, 754–760. [Google Scholar] [CrossRef]
- Dai, Z.; Yan, C.; Wang, Z.; Wang, J.; Xia, M.; Li, K.; He, Y. Discriminative analysis of early Alzheimer’s disease using multi-modal imaging and multi-level characterization with multi-classifier (M3). Neuroimage 2012, 59, 2187–2195. [Google Scholar] [CrossRef]
- Tarawneh, R.; Head, D.; Allison, S.; Buckles, V.; Fagan, A.M.; Ladenson, J.H.; Morris, J.C.; Holtzman, D.M. Cerebrospinal Fluid Markers of Neurodegeneration and Rates of Brain Atrophy in Early Alzheimer DiseaseCSF Markers of Neurodegeneration and Brain Atrophy in ADCSF Markers of Neurodegeneration and Brain Atrophy in AD. JAMA Neurol. 2015, 72, 656–665. [Google Scholar] [CrossRef] [PubMed]
- McMahon, P.M.; Araki, S.S.; Neumann, P.J.; Harris, G.J.; Gazelle, G.S. Cost-effectiveness of functional imaging tests in the diagnosis of Alzheimer disease. Radiology 2000, 217, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Fuh, J.L.; Lirng, J.F.; Chen, S.P.; Hseu, S.S.; Wu, J.C.; Wang, S.J. Cerebrospinal fluid leakage and headache after lumbar puncture: A prospective non-invasive imaging study. Brain 2015, 138, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Bhalala, O.G.; Srikanth, M.; Kessler, J.A. The emerging roles of microRNAs in CNS injuries. Nat. Rev. Neurol. 2013, 9, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, J.P.; Ward, J.; Taylor, I.A.; Waters, M.; Shi, Y.; Cannon, B.; Kelnar, K.; Kemppainen, J.; Brown, D.; Chen, C.; et al. Identification of miRNA changes in Alzheimer’s disease brain and CSF yields putative biomarkers and insights into disease pathways. J. Alzheimers Dis. 2008, 14, 27–41. [Google Scholar] [CrossRef]
- Geekiyanage, H.; Jicha, G.A.; Nelson, P.T.; Chan, C. Blood serum miRNA: Non-invasive biomarkers for Alzheimer’s disease. Exp. Neurol. 2012, 235, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, S.; Kenny, A.; Medina, M.; Engel, T.; Jimenez-Mateos, E.M. MicroRNAs in Neurodegenerative Diseases. Int. Rev. Cell. Mol. Biol. 2017, 334, 309–343. [Google Scholar]
- Joilin, G.; Guévremont, D.; Ryan, B.; Claudianos, C.; Cristino, A.S.; Abraham, W.C.; Williams, J.M. Rapid regulation of microRNA following induction of long-term potentiation in vivo. Front. Mol. Neurosci. 2014, 7. [Google Scholar] [CrossRef]
- Glinge, C.; Clauss, S.; Boddum, K.; Jabbari, R.; Jabbari, J.; Risgaard, B.; Tomsits, P.; Hildebrand, B.; Kääb, S.; Wakili, R.; et al. Stability of Circulating Blood-Based MicroRNAs - Pre-Analytic Methodological Considerations. PLoS ONE 2017, 12, e0167969. [Google Scholar] [CrossRef]
- Olazaran, J.; Valenti, M.; Frades, B.; Zea-Sevilla, M.A.; Avila-Villanueva, M.; Fernandez-Blazquez, M.A.; Calero, M.; Dobato, J.L.; Hernandez-Tamames, J.A.; Leon-Salas, B.; et al. The Vallecas Project: A Cohort to Identify Early Markers and Mechanisms of Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7, 181. [Google Scholar] [CrossRef]
- Martinez-Martin, P.; Avila, J.; Investigators, A.D.R.U. Alzheimer Center Reina Sofia Foundation: Fighting the disease and providing overall solutions. J. Alzheimers Dis. 2010, 21, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Avila-Villanueva, M.; Fernandez-Blazquez, M.A. Subjective Cognitive Decline as a Preclinical Marker for Alzheimer’s Disease: The Challenge of Stability Over Time. Front. Aging Neurosci. 2017, 9, 377. [Google Scholar] [CrossRef] [PubMed]
- Pena-Casanova, J.; Gramunt-Fombuena, N.; Quinones-Ubeda, S.; Sanchez-Benavides, G.; Aguilar, M.; Badenes, D.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Payno, M.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for the Rey-Osterrieth complex figure (copy and memory), and free and cued selective reminding test. Arch. Clin. Neuropsychol. 2009, 24, 371–393. [Google Scholar] [CrossRef] [PubMed]
- Grober, E.; Sanders, A.E.; Hall, C.; Lipton, R.B. Free and cued selective reminding identifies very mild dementia in primary care. Alzheimer Dis. Assoc. Disord. 2010, 24, 284–290. [Google Scholar] [CrossRef]
- Grande, G.; Vanacore, N.; Vetrano, D.L.; Cova, I.; Rizzuto, D.; Mayer, F.; Maggiore, L.; Ghiretti, R.; Cucumo, V.; Mariani, C.; et al. Free and cued selective reminding test predicts progression to Alzheimer’s disease in people with mild cognitive impairment. Neurol. Sci. 2018, 39, 1867–1875. [Google Scholar] [CrossRef]
- Jimenez-Mateos, E.M.; Arribas-Blazquez, M.; Sanz-Rodriguez, A.; Concannon, C.; Olivos-Ore, L.A.; Reschke, C.R.; Mooney, C.M.; Mooney, C.; Lugara, E.; Morgan, J.; et al. microRNA targeting of the P2 × 7 purinoceptor opposes a contralateral epileptogenic focus in the hippocampus. Sci. Rep. 2015, 5, 17486. [Google Scholar] [CrossRef]
- Kenny, A.; Jimenez-Mateos, E.M.; Calero, M.; Medina, M.; Engel, T. Detecting Circulating MicroRNAs as Biomarkers in Alzheimer’s Disease. Methods Mol. Biol. 2018, 1779, 471–484. [Google Scholar]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- McArdle, H.; Jimenez-Mateos, E.M.; Raoof, R.; Carthy, E.; Boyle, D.; ElNaggar, H.; Delanty, N.; Hamer, H.; Dogan, M.; Huchtemann, T.; et al. “TORNADO”—Theranostic One-Step RNA Detector; microfluidic disc for the direct detection of microRNA-134 in plasma and cerebrospinal fluid. Sci. Rep. 2017, 7, 1750. [Google Scholar] [CrossRef]
- Liu, C.G.; Wang, J.L.; Li, L.; Xue, L.X.; Zhang, Y.Q.; Wang, P.C. MicroRNA-135a and -200b, potential Biomarkers for Alzheimers disease, regulate beta secretase and amyloid precursor protein. Brain Res. 2014, 1583, 55–64. [Google Scholar] [CrossRef]
- Denk, J.; Boelmans, K.; Siegismund, C.; Lassner, D.; Arlt, S.; Jahn, H. MicroRNA Profiling of CSF Reveals Potential Biomarkers to Detect Alzheimer‘s Disease. PLoS ONE 2015, 10, e0126423. [Google Scholar] [CrossRef] [PubMed]
- Derkow, K.; Rössling, R.; Schipke, C.; Krüger, C.; Bauer, J.; Fähling, M.; Stroux, A.; Schott, E.; Ruprecht, K.; Peters, O.; et al. Distinct expression of the neurotoxic microRNA family let-7 in the cerebrospinal fluid of patients with Alzheimer’s disease. PLoS ONE 2018, 13, e0200602. [Google Scholar] [CrossRef] [PubMed]
- Leidinger, P.; Backes, C.; Deutscher, S.; Schmitt, K.; Mueller, S.C.; Frese, K.; Haas, J.; Ruprecht, K.; Paul, F.; Stähler, C.; et al. A blood based 12-miRNA signature of Alzheimer disease patients. Genome. Biol. 2013, 14, R78. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Liu, Z.; Jiang, L.; Liu, W.; Song, M.; Zhang, Q.; Zhang, R.; Cui, D.; Wang, X.; Xu, S. Increased Serum miR-206 Level Predicts Conversion from Amnestic Mild Cognitive Impairment to Alzheimer’s Disease: A 5-Year Follow-up Study. J. Alzheimers Dis. 2017, 55, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Schindler, S.E.; McCue, L.M.; Moulder, K.L.; Benzinger, T.L.S.; Cruchaga, C.; Fagan, A.M.; Grant, E.; Gordon, B.A.; Holtzman, D.M.; et al. Assessment of Racial Disparities in Biomarkers for Alzheimer Disease. JAMA Neurol. 2019, 76, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.D.; Sagare, A.P.; Zlokovic, B.V. Blood-brain barrier breakdown in Alzheimer disease and other neurodegenerative disorders. Nat. Rev. Neurol. 2018, 14, 133–150. [Google Scholar] [CrossRef]
- Montagne, A.; Barnes, S.R.; Sweeney, M.D.; Halliday, M.R.; Sagare, A.P.; Zhao, Z.; Toga, A.W.; Jacobs, R.E.; Liu, C.Y.; Amezcua, L.; et al. Blood-brain barrier breakdown in the aging human hippocampus. Neuron 2015, 85, 296–302. [Google Scholar] [CrossRef]
- Lee, S.T.; Chu, K.; Jung, K.H.; Kim, J.H.; Huh, J.Y.; Yoon, H.; Park, D.K.; Lim, J.Y.; Kim, J.M.; Jeon, D.; et al. miR-206 regulates brain-derived neurotrophic factor in Alzheimer disease model. Ann. Neurol. 2012, 72, 269–277. [Google Scholar] [CrossRef]
- Moon, J.; Lee, S.-T.; Kong, I.G.; Byun, J.-I.; Sunwoo, J.-S.; Shin, J.-W.; Shim, J.-Y.; Park, J.-H.; Jeon, D.; Jung, K.-H.; et al. Early diagnosis of Alzheimer’s disease from elevated olfactory mucosal miR-206 level. Sci. Rep. 2016, 6, 20364. [Google Scholar] [CrossRef]
- Jellinger, K.A. Clinicopathological analysis of dementia disorders in the elderly--An update. J. Alzheimers Dis. 2006, 9, 61–70. [Google Scholar] [CrossRef]
- Grasso, M.; Piscopo, P.; Talarico, G.; Ricci, L.; Crestini, A.; Tosto, G.; Gasparini, M.; Bruno, G.; Denti, M.A.; Confaloni, A. Plasma microRNA profiling distinguishes patients with frontotemporal dementia from healthy subjects. Neurobiol. Aging 2019. In Press. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Ratcliff, G.; Belle, S.H.; Cauley, J.A.; DeKosky, S.T.; Ganguli, M. Patterns of Cognitive Decline in Presymptomatic Alzheimer Disease: A Prospective Community Study. JAMA Psychiatry 2001, 58, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Hensel, A.; Luck, T.; Luppa, M.; Glaesmer, H.; Angermeyer, M.C.; Riedel-Heller, S.G. Does a reliable decline in Mini Mental State Examination total score predict dementia? Diagnostic accuracy of two reliable change indices. Dement. Geriatr. Cogn. Disord. 2009, 27, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Leurgans, S.E.; Boyle, P.A.; Bennett, D.A. Cognitive Decline in Prodromal Alzheimer Disease and Mild Cognitive ImpairmentCognitive Decline in Prodromal AD and MCI. Arch. Neurol. 2011, 68, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Small, B.J.; Bäckman, L.; Fratiglioni, L. Stability of the preclinical episodic memory deficit in Alzheimer’s disease. Brain 2001, 124, 96–102. [Google Scholar]
- Williams, A.H.; Valdez, G.; Moresi, V.; Qi, X.; McAnally, J.; Elliott, J.L.; Bassel-Duby, R.; Sanes, J.R.; Olson, E.N. MicroRNA-206 delays ALS progression and promotes regeneration of neuromuscular synapses in mice. Science 2009, 326, 1549–1554. [Google Scholar] [CrossRef]
- Guida, N.; Valsecchi, V.; Laudati, G.; Serani, A.; Mascolo, L.; Molinaro, P.; Montuori, P.; Di Renzo, G.; Canzoniero, L.M.; Formisano, L. The miR206-JunD Circuit Mediates the Neurotoxic Effect of Methylmercury in Cortical Neurons. Toxicol. Sci. 2018, 163, 569–578. [Google Scholar] [CrossRef]
- Panja, D.; Bramham, C.R. BDNF mechanisms in late LTP formation: A synthesis and breakdown. Neuropharmacology 2014, 76 Pt C, 664–676. [Google Scholar] [CrossRef]
- Edelmann, E.; Lessmann, V.; Brigadski, T. Pre- and postsynaptic twists in BDNF secretion and action in synaptic plasticity. Neuropharmacology 2014, 76 Pt C, 610–627. [Google Scholar] [CrossRef]
- Holsinger, R.M.; Schnarr, J.; Henry, P.; Castelo, V.T.; Fahnestock, M. Quantitation of BDNF mRNA in human parietal cortex by competitive reverse transcription-polymerase chain reaction: Decreased levels in Alzheimer’s disease. Brain Res. Mol. Brain Res. 2000, 76, 347–354. [Google Scholar] [CrossRef]
- Peng, S.; Wuu, J.; Mufson, E.J.; Fahnestock, M. Precursor form of brain-derived neurotrophic factor and mature brain-derived neurotrophic factor are decreased in the pre-clinical stages of Alzheimer’s disease. J. Neurochem. 2005, 93, 1412–1421. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discovery Cohort | Control (n = 31, CDR = 0) | MCI (n = 30, CDR = 0.5) | AD (n = 25, CDR ≥1) | p Value |
| Age, mean (SD) [range] | 75.0 (4.7) [69–86] | 76.8 (4.0) [69–84] | 84.6 (3.5) [77–90] | <0.0001 *** |
| Male sex, No. (%) | 17 (54.8) | 13 (43.3) | 4 (16) | 0.02 * |
| Educational level mean (SD) | 11.8 (5.6) | 7.0 (4.3) | 3.8 (1.1) | <0.0001 *** |
| 1 or 2 APOE4 alleles | 4.0 | 9.0 | 10.0 | 0.05 |
| Diabetes Mellitus, % | 12.9 | 26.7 | 15.8 | 0.37 |
| Hypertension, % | 48.4 | 53.3 | 57.9 | 0.86 |
| Physical Exercise frequency, mean (SD) [range] | 0.6 (0.4) [0–1] | 0.4 (0.4) [0–1] | NA | 0.0568 |
| Never/Rarely (0) | 7.0 | 15.0 | NA | |
| Sometimes (0.5) | 10.0 | 9.0 | NA | |
| Frequently/Always (1) | 14.0 | 6.0 | NA | |
| Annual visits completed, (SD) [range] | 3.8 (1.1) [2–5] | 3.8 (1.4) [2–5] | NA | 0.83 |
| MMSE mean (SD) | 28.7 (1.5) | 26.6 (2) | NA | <0.0001 *** |
| Longitudinal Cohort | Group 1: Control-MCI-MCI (n = 6) | Group 2: Control-MCI-Dementia (n = 6) | Group 3: MCI-MCI-Dementia (n = 6) | p Value |
| Age, mean (SD) [range] | 74.0 (3.2) [69.6–76.9] | 77.3 (3.8) [70.7–81.8] | 75.8 (3.6) [72.3-82.3] | 0.338 |
| Male sex, No. (%) | 2 (33.3) | 1 (16.6) | 4 (66.6) | 0.213 |
| Hypertension, % | 32.2 | 50 | 32.2 | 0.802 |
| Physical Exercise frequency, mean (SD) [range] | 0.5 (0.4) [0–1] | 0.6 (0.5) [0–1] | 0.4 (0.4) [0–1] | 0.79 |
| Never/Rarely (0) | 2 | 2 | 2 | |
| Sometimes (0.5) | 2 | 1 | 3 | |
| Frequently/Always (1) | 2 | 3 | 1 | |
| Annual visits completed, (SD) [range] | 5.2 (1) [4–6] | 5 (0) [5–5] | 4 (0.6) [3–5] | 0.0291 * |
| Visit 1 MMSE, mean (SD) | 27.3 (1.9) | 26.8 (3.3) | 22 (1.8) | 0.1609 |
| Age Adjusted FCSRT MCI Cut-Off Groups | MCI Above Cut-Off (n = 12) | MCI Below Cut-Off (n = 5) | p Value |
| Free Cued Selective Recall Test, mean (SD) | |||
| Free Score at first sampling | 14.3 (5.6) | 8.4 (3.2) | 0.0445 * |
| Free score annual change | 1.4 (5.0) | −0.1 (5.2) | 0.33 |
| Free Score at final sampling | 18.5 (7.1) | 8 (3.2) | 0.0059 ** |
| Total score at first sampling | 29.5 (6.9) | 24.4 (6.6) | 0.186 |
| Total score annual change | 2.2 (6.5) | −0.1 (6.8) | 0.26 |
| Total Score at final sampling | 36.0 (6.2) | 24.2 (7.2) | 0.0037 ** |
| Digit Symbol test, mean (SD) | |||
| Score at first sampling | 13.1 (5.8) | 16.2 (4.8) | 0.293 |
| Annual change | −0.8 (2.9) | −1.2 (2.9) | 0.39 |
| Score at final sampling | 10.73(6.0) | 12.6 (4.7) | 0.376 |
| MicroRNA relative expression, mean (SD) | |||
| miR-206 | 0.9 (0.7) | 2.9 (1.9) | 0.0174 * |
| Let-7b | 2.1 (1.1) | 2.5 (0.9) | 0.68 |
| miR-135a | 1.2(1.3) | 1.9 (1.6) | 0.078 |
| MMSE Grouping | MCI Stable (n = 9) | MCI Decliners (n = 8) | p Value |
| Mini-Mental-State-Exam, mean (SD) | |||
| Score at first sampling | 27.6 (0.5) | 26.0 (1.5) | 0.0059 ** |
| Annual change | −0.3 (2.4) | −1.3 (2.6) | 0.16 |
| Score at final sampling | 26.6 (1.1) | 22.0 (2.0) | < 0.0001 *** |
| Functional activities questionnaire, mean (SD) | |||
| Score at first sampling | 3.1 (1.4) | 2 (1.4) | 0.12 |
| Annual change | −0.3 (2.0) | 0.9 (2.8) | 0.13 |
| Score at final sampling | 2.8 (1.8) | 4.8 (6.0) | 0.56 |
| MicroRNA relative expression, mean (SD) | |||
| miR-206 | 0.9 (1.0) | 2.4 (1.5) | 0.0055 ** |
| Let-7b | 2.4 (1.2) | 3.1 (2.9) | 0.72 |
| miR-135a | 1.2 (1.2) | 1.6 (1.6) | 0.9551 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kenny, A.; McArdle, H.; Calero, M.; Rabano, A.; Madden, S.F.; Adamson, K.; Forster, R.; Spain, E.; Prehn, J.H.M.; Henshall, D.C.; et al. Elevated Plasma microRNA-206 Levels Predict Cognitive Decline and Progression to Dementia from Mild Cognitive Impairment. Biomolecules 2019, 9, 734. https://doi.org/10.3390/biom9110734
Kenny A, McArdle H, Calero M, Rabano A, Madden SF, Adamson K, Forster R, Spain E, Prehn JHM, Henshall DC, et al. Elevated Plasma microRNA-206 Levels Predict Cognitive Decline and Progression to Dementia from Mild Cognitive Impairment. Biomolecules. 2019; 9(11):734. https://doi.org/10.3390/biom9110734
Chicago/Turabian StyleKenny, Aidan, Hazel McArdle, Miguel Calero, Alberto Rabano, Stephen F. Madden, Kellie Adamson, Robert Forster, Elaine Spain, Jochen H.M. Prehn, David C. Henshall, and et al. 2019. "Elevated Plasma microRNA-206 Levels Predict Cognitive Decline and Progression to Dementia from Mild Cognitive Impairment" Biomolecules 9, no. 11: 734. https://doi.org/10.3390/biom9110734
APA StyleKenny, A., McArdle, H., Calero, M., Rabano, A., Madden, S. F., Adamson, K., Forster, R., Spain, E., Prehn, J. H. M., Henshall, D. C., Medina, M., Jimenez-Mateos, E. M., & Engel, T. (2019). Elevated Plasma microRNA-206 Levels Predict Cognitive Decline and Progression to Dementia from Mild Cognitive Impairment. Biomolecules, 9(11), 734. https://doi.org/10.3390/biom9110734